
Progress and Current Limitations of Materials for Artificial Bile Duct Engineering

 , and
, and
Abstract
:1. Introduction
2. Materials Choice for Artificial Bile Ducts
2.1. Non-Degradable Materials
2.2. Degradable Natural Materials
2.3. Degradable Synthetic Materials
2.4. Nanomaterials
3. Cell-Seeded Scaffolds
3.1. Stem Cells
3.2. Stem Cell-Derived Bile Duct Cells and 3D Organoids
4. Biologically Active Factor-Functionalized Scaffolds
5. Current Limitations and Reasons for Poor Clinical Translation
5.1. Limitations of Scaffold Materials
5.2. Limitations of Cell-Seeding Techniques
5.3. Limitations of Biologically Active Factor-Functionalized Scaffolds
6. Future Research Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schreuder, A.M.; Busch, O.R.; Besselink, M.G.; Ignatavicius, P.; Gulbinas, A.; Barauskas, G.; Gouma, D.J.; van Gulik, T.M. Long-Term Impact of Iatrogenic Bile Duct Injury. Dig. Surg. 2019, 37, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Sicklick, J.K.; Camp, M.S.; Lillemoe, K.D.; Melton, G.B.; Yeo, C.J.; Campbell, K.A.; Talamini, M.A.; Pitt, H.A.; Coleman, J.A.; Sauter, P.A.; et al. Surgical management of bile duct injuries sustained during laparoscopic cholecystectomy. Ann. Surg. 2005, 241, 786–795. [Google Scholar] [CrossRef]
- Pekolj, J.; Alvarez, F.A.; Palavecino, M.; Sánchez Clariá, R.; Mazza, O.; de Santibañes, E. Intraoperative Management and Repair of Bile Duct Injuries Sustained during 10,123 Laparoscopic Cholecystectomies in a High-Volume Referral Center. J. Am. Coll. Surg. 2013, 216, 894–901. [Google Scholar] [CrossRef]
- Ng, J.J.; Kow, A.W. Pedicled omental patch as a bridging procedure for iatrogenic bile duct injury. World J. Gastroenterol. 2017, 23, 6741–6746. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Zou, H.; Liu, Y.-X.; Zhang, X.-W. Effects of Paclitaxel-conjugated N-Succinyl-Hydroxyethyl Chitosan Film for Proliferative Cholangitis in Rabbit Biliary Stricture Model. Chin. Med. J. 2018, 131, 696–703. [Google Scholar] [CrossRef]
- Parra-membrives, P.; Martínez-baena, D.; Sánchez-sánchez, F. Late Biliary Complications after Pancreaticoduodenectomy. Am. Surg. 2016, 82, 456–461. [Google Scholar] [CrossRef]
- Settmacher, U.; Steinmuller, T.H.; Schmidt, S.C.; Heise, M.; Pascher, A.; Theruvath, T.; Hintze, R.; Neuhaus, P. Technique of bile duct reconstruction and management of biliary complications in right lobe living donor liver transplantation. Clin. Transplant. 2003, 17, 37–42. [Google Scholar] [CrossRef]
- Barrett, M.; Asbun, H.J.; Chien, H.-L.; Brunt, L.M.; Telem, D.A. Bile duct injury and morbidity following cholecystectomy: A need for improvement. Surg. Endosc. 2017, 32, 1683–1688. [Google Scholar] [CrossRef]
- Zeng, J.; Wang, J.; Dong, J.; Huang, X.; Xia, H.; Xiang, X. The application of vascularized stomach flap to repair postoperative biliary stricture. Medicine 2018, 97, e11344. [Google Scholar] [CrossRef]
- Ramos-Gonzalez, G.; Kim, H.B. Autologous intestinal reconstruction surgery. Semin. Pediatric Surg. 2018, 27, 261–266. [Google Scholar] [CrossRef]
- Yoon, S.-H.; Yeo, M.-K.; Kim, S.-H.; Song, I.-S.; Jeon, G.-S.; Han, S.-J. Feasibility of using the homologous parietal peritoneum as a vascular substitute for venous reconstruction during abdominal surgery: An animal model. Surgery 2021, 170, 1268–1276. [Google Scholar] [CrossRef]
- Du, Y.; Guo, J.L.; Wang, J.; Mikos, A.G.; Zhang, S. Hierarchically designed bone scaffolds: From internal cues to external stimuli. Biomaterials 2019, 218, 119334. [Google Scholar] [CrossRef] [PubMed]
- Schanaider, A.; Pannain, V.L.; Müller, L.C.; Maya, M.C. Expanded polytetrafluoroethylene in canine bile duct injury: A critical analysis. Acta Cir. Bras. 2011, 26, 247–252. [Google Scholar] [CrossRef] [Green Version]
- Ren, W.; Shi, D. Experimental study on repair of bile duct defects with expanded polytetrafluoroethylene. Chin. J. Reparative Reconstr. Surg. 2001, 15, 305–307. [Google Scholar]
- Li, H.; Yin, Y.; Xiang, Y.; Liu, H.; Guo, R. A novel 3D printing PCL/GelMA scaffold containing USPIO for MRI-guided bile duct repair. Biomed. Mater. 2020, 15, 045004. [Google Scholar] [CrossRef]
- Aikawa, M.; Miyazawa, M.; Okamoto, K.; Toshimitsu, Y.; Torii, T.; Okada, K.; Akimoto, N.; Ohtani, Y.; Koyama, I.; Yoshito, I. A novel treatment for bile duct injury with a tissue-engineered bioabsorbable polymer patch. Surgery 2010, 147, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Struecker, B.; Hillebrandt, K.-H.; Raschzok, N.; Jöhrens, K.; Butter, A.; Tang, P.; Andreou, A.; Napierala, H.; Reutzel-Selke, A.; Denecke, T.; et al. Implantation of a Tissue-Engineered Neo-Bile Duct in Domestic Pigs. Eur. Surg. Res. 2015, 56, 61–75. [Google Scholar] [CrossRef]
- Li, Q.; Tao, L.; Chen, B.; Ren, H.; Hou, X.; Zhou, S.; Zhou, J.; Sun, X.; Dai, J.; Ding, Y. Extrahepatic bile duct regeneration in pigs using collagen Scaffolds loaded with human collagen-binding bFGF. Biomaterials 2012, 33, 4298–4308. [Google Scholar] [CrossRef]
- Pérez Alonso, A.J.; Del Olmo Rivas, C.; Romero, I.M.; Cañizares Garcia, F.J.; Poyatos, P.T. Tissue-engineering repair of extrahepatic bile ducts. J. Surg. Res. 2013, 179, 18–21. [Google Scholar] [CrossRef]
- Nakashima, S.; Nakamura, T.; Miyagawa, K.; Yoshikawa, T.; Kin, S.; Kuriu, Y.; Nakase, Y.; Sakakura, C.; Otsuji, E.; Hagiwara, A.; et al. In situ tissue engineering of the bile duct using polypropylene mesh-collagen tubes. Int. J. Artif. Organs 2007, 30, 75–85. [Google Scholar] [CrossRef]
- Gilbert, T.W.; Sellaro, T.L.; Badylak, S.F. Decellularization of tissues and organs. Biomaterials 2006, 27, 3675–3683. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.L.; Griffiths, L.G. Immunogenicity in xenogeneic SCAFFOLD generation: Antigen removal Vs. decellularization. Acta Biomater. 2014, 10, 1806–1816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassanein, W.; Uluer, M.C.; Langford, J.; Woodall, J.D.; Cimeno, A.; Dhru, U.; Werdesheim, A.; Harrison, J.; Rivera-Pratt, C.; Klepfer, S.; et al. Recellularization via the bile duct supports functional allogenic and xenogenic cell growth on a decellularized rat liver scaffold. Organogenesis 2016, 13, 16–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Y.; Xiong, X.-Z.; Zhou, R.-X.; Deng, Y.-L.; Jin, Y.-W.; Lu, J.; Li, F.-Y.; Cheng, N.-S. Repair of a common bile duct defect with a decellularized ureteral graft. World J. Gastroenterol. 2016, 22, 10575. [Google Scholar] [CrossRef]
- Zhu, M.; Li, W.; Dong, X.; Yuan, X.; Midgley, A.C.; Chang, H.; Wang, Y.; Wang, H.; Wang, K.; Ma, P.X.; et al. In vivo engineered extracellular matrix scaffolds with instructive niches for oriented tissue regeneration. Nat. Commun. 2019, 10, 4620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Holzwarth, J.M.; Ma, P.X. Functionalized synthetic biodegradable polymer scaffolds for tissue engineering. Macromol. Biosci. 2012, 12, 911–919. [Google Scholar] [CrossRef] [Green Version]
- Asghari, F.; Samiei, M.; Adibkia, K.; Akbarzadeh, A.; Davaran, S. Biodegradable and biocompatible polymers for tissue engineering application: A review. Artif. Cells Nanomed. Biotechnol. 2016, 45, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Barralet, J.E.; Wallace, L.L.; Strain, A.J. Tissue engineering of human biliary epithelial cells on polyglycolic acid/polycaprolactone scaffolds maintains long-term phenotypic stability. Tissue Eng. 2003, 9, 1037–1045. [Google Scholar] [CrossRef] [PubMed]
- Zong, C.; Wang, M.; Yang, F.; Chen, G.; Chen, J.; Tang, Z.; Liu, Q.; Gao, C.; Ma, L.; Wang, J. A novel therapy strategy for bile duct repair using tissue engineering technique: PCL/PLGA bilayered scaffold with hMSCs. J. Tissue Eng. Regen. Med. 2015, 11, 966–976. [Google Scholar] [CrossRef] [PubMed]
- Miyazawa, M.; Torii, T.; Toshimitsu, Y.; Okada, K.; Koyama, I.; Ikada, Y. A tissue-engineered artificial bile duct grown to resemble the native bile duct. Am. J. Transplant. 2005, 5, 1541–1547. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Wang, Y.; Ferracci, G.; Zheng, J.; Cho, N.; Lee, B.H. Gelatin methacryloyl and its hydrogels with an exceptional degree of controllability and batch-to-batch consistency. Sci. Rep. 2019, 9, 6863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moazeni, N.; Semnani, D.; Rafeinia, M.; Hasani, H.; Naeimi, M.; Sadrjahani, M. The effect of electrospinning parameters on the compliance behavior of electrospun polyurethane tube for artificial common bile duct. Polym. Sci. Ser. A 2017, 59, 67–75. [Google Scholar] [CrossRef]
- Griffith, L.G. Tissue Engineering--Current Challenges and Expanding Opportunities. Science 2002, 295, 1009–1014. [Google Scholar] [CrossRef] [PubMed]
- Funfak, A.; Bouzhir, L.; Gontran, E.; Minier, N.; Dupuis-Williams, P.; Gobaa, S. Biophysical Control of Bile Duct Epithelial Morphogenesis in Natural and Synthetic Scaffolds. Prime Arch. Biotechnol. 2020, 7, 417. [Google Scholar]
- Tanimizu, N.; Miyajima, A.; Mostov, K.E. Liver progenitor cells develop cholangiocyte-type epithelial polarity in three-dimensional culture. Mol. Biol. Cell 2007, 18, 1472–1479. [Google Scholar] [CrossRef] [Green Version]
- Crosby, H.A.; Kelly, D.A.; Strain, A.J. Human hepatic stem-like cells isolated using c-kit or CD34 can differentiate into biliary epithelium. Gastroenterology 2001, 120, 534–544. [Google Scholar] [CrossRef]
- Lewis, P.L.; Su, J.; Yan, M.; Meng, F.; Glaser, S.S.; Alpini, G.D.; Green, R.M.; Sosa-Pineda, B.; Shah, R.N. Complex bile duct network formation within liver decellularized extracellular matrix hydrogels. Sci. Rep. 2018, 8, 12220. [Google Scholar] [CrossRef]
- Liu, X.; Yan, J.; Liu, J.; Wang, Y.; Yin, J.; Fu, J. Fabrication of a dual-layer cell-laden tubular scaffold for nerve regeneration and bile duct reconstruction. Biofabrication 2021, 13, 035038. [Google Scholar] [CrossRef]
- Lin, Y.; Yan, L.; Cheng, N. Application of bone marrow cells: A novel therapy for bile leak? Med. Hypotheses 2009, 73, 374–376. [Google Scholar] [CrossRef]
- Takahashi, K.; Yamanaka, S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell 2006, 126, 663–676. [Google Scholar] [CrossRef] [Green Version]
- Cervantes-Alvarez, E.; Wang, Y.; Collin de l’Hortet, A.; Guzman-Lepe, J.; Zhu, J.; Takeishi, K. Current strategies to generate mature human induced pluripotent stem cells derived cholangiocytes and future applications. Organogenesis 2017, 13, 1–15. [Google Scholar] [CrossRef]
- Matsui, S.; Ochiai, M.; Yasuda, K.; Mae, S.-i.; Kotaka, M.; Toyoda, T.; Yamamoto, T.; Osafune, K. Differentiation and isolation of iPSC-derived Remodeling Ductal plate-like cells by use of an AQP1-GFP Reporter human iPSC line. Stem Cell Res. 2019, 35, 101400. [Google Scholar] [CrossRef]
- Sampaziotis, F.; de Brito, M.C.; Geti, I.; Bertero, A.; Hannan, N.R.F.; Vallier, L. Directed differentiation of human induced pluripotent stem cells into functional cholangiocyte-like cells. Nat. Protoc. 2017, 12, 814–827. [Google Scholar] [CrossRef]
- De Assuncao, T.M.; Sun, Y.; Jalan-Sakrikar, N.; Drinane, M.C.; Huang, B.Q.; Li, Y.; Davila, J.I.; Wang, R.; O’Hara, S.P.; Lomberk, G.A.; et al. Development and characterization of human-induced pluripotent stem cell-derived cholangiocytes. Lab. Investig. 2015, 95, 684–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dianat, N.; Dubois-Pot-Schneider, H.; Steichen, C.; Desterke, C.; Leclerc, P.; Raveux, A.; Combettes, L.; Weber, A.; Corlu, A.; Dubart-Kupperschmitt, A. Generation of functional cholangiocyte-like cells from human pluripotent stem cells and HepaRG cells. Hepatology 2014, 60, 700–714. [Google Scholar] [CrossRef] [Green Version]
- Noto, F.K.; Duncan, S.A. Generation of hepatocyte-like cells from human pluripotent stem cells. In Stem Cells Handbook; Humana Press: New York, NY, USA, 2013; pp. 139–147. [Google Scholar]
- Lancaster, M.A.; Knoblich, J.A. Organogenesis in a dish: Modeling development and disease using organoid technologies. Science 2014, 345, 1247125. [Google Scholar] [CrossRef]
- Sampaziotis, F.; Justin, A.W.; Tysoe, O.C.; Sawiak, S.; Godfrey, E.M.; Upponi, S.S.; Gieseck, R.L.; de Brito, M.C.; Berntsen, N.L.; Gómez-Vázquez, M.J.; et al. Reconstruction of the mouse extrahepatic biliary tree using primary human extrahepatic cholangiocyte organoids. Nat. Med. 2017, 23, 954–963. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Khandekar, G.; Llewellyn, J.; Polacheck, W.; Chen, C.S.; Wells, R.G. A bile duct-on-a-chip with organ-level functions. Hepatology 2019, 71, 1350–1363. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, S.P.; Mark Saltzman, W. Materials for protein delivery in tissue engineering. Adv. Drug Deliv. Rev. 1998, 33, 71–86. [Google Scholar] [CrossRef]
- Zong, Y.; Stanger, B.Z. Molecular mechanisms of bile duct development. Wiley Interdiscip. Rev. Dev. Biol. 2012, 1, 643–655. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Li, P.; Jin, X.; Su, F.; Shen, J.; Yuan, J. Poly(ε-caprolactone)/keratin/heparin/VEGF bio-composite mats for vascular tissue engineering. J. Biomed. Mater. Res. Part A 2019, 108, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Vasanthan, K.S.; Subramanian, A.; Krishnan, U.M.; Sethuraman, S. Development of porous hydrogel scaffolds with multiple cues for liver tissue engineering. Regen. Eng. Transl. Med. 2017, 3, 176–191. [Google Scholar] [CrossRef]
- Strazzabosco, M.; Fabris, L. Functional anatomy of normal bile ducts. Anat. Rec. Adv. Integr. Anat. Evol. Biol. 2008, 291, 653–660. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, K.; Nakamura, T. Hepatocyte growth factor: Renotropic role and potential therapeutics for renal diseases. Kidney Int. 2001, 59, 2023–2038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrara, N.; Gerber, H.-P.; LeCouter, J. The biology of VEGF and its receptors. Nat. Med. 2003, 9, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Huajiang, D.; Huipeng, M.; Tao, J.; Yanlin, H.; Wangcheng, R.; Jian, X.; Yanlong, Z.; Shuwang, Y. The Combination of N-methyl-D-aspartate Receptor Antagonists and MSCs Therapy may have a Multiplier Effect in Spinal Cord Injury. Turk. Neurosurg. 2021, 31, 479–480. [Google Scholar] [CrossRef]
- Makino, T.; Jinnin, M.; Muchemwa, F.C.; Fukushima, S.; Kogushi-Nishi, H.; Moriya, C.; Igata, T.; Fujisawa, A.; Johno, T.; Ihn, H. Basic fibroblast growth factor stimulates the proliferation of human dermal fi-broblasts via the ERK1/2 and JNK pathways. Br. J. Dermatol. 2009, 162, 717–723. [Google Scholar] [CrossRef]
- Mihara, M.; Hashizume, M.; Yoshida, H.; Suzuki, M.; Shiina, M. IL-6/IL-6 receptor system and its role in physiological and pathological conditions. Clin. Sci. 2011, 122, 143–159. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Sakamoto, T.; Yokomuro, S.; Ezure, T.; Subbotin, V.; Murase, N.; Contrucci, S.; Demetris, A.J. Acute obstructive cholangiopathy in interleukin-6 deficient mice: Compensation by leukemia inhibitory factor (LIF) suggests importance of gp-130 signaling in the ductular reaction. Liver 2000, 20, 114–124. [Google Scholar] [CrossRef]
- Postlethwaite, A.E.; Keski-Oja, J.; Moses, H.L.; Kang, A.H. Stimulation of the chemotactic migration of human fibroblasts by transforming growth factor beta. J. Exp. Med. 1987, 165, 251–256. [Google Scholar] [CrossRef] [Green Version]
- Antoniou, A.; Raynaud, P.; Cordi, S.; Zong, Y.; Tronche, F.; Stanger, B.Z.; Jacquemin, P.; Pierreux, C.E.; Clotman, F.; Lemaigre, F.P. Intrahepatic bile ducts develop according to a new mode of tubulogenesis regulated by the transcription factor SOX9. Gastroenterology 2009, 136, 2325–2333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Jochems, P.G.; Salz, L.; Schneeberger, K.; Penning, L.C.; van de Graaf, S.F.; Beuers, U.; Clevers, H.; Geijsen, N.; Masereeuw, R.; et al. Bioengineered bile ducts recapitulate key cholangiocyte functions. Biofabrication 2018, 10, 034103. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, M.; Ogawa, S.; Bear, C.E.; Ahmadi, S.; Chin, S.; Li, B.; Grompe, M.; Keller, G.; Kamath, B.M.; Ghanekar, A. Directed differentiation of cholangiocytes from human pluripotent stem cells. Nat. Biotechnol. 2015, 33, 853–861. [Google Scholar] [CrossRef]
- Sampaziotis, F.; Cardoso de Brito, M.; Madrigal, P.; Bertero, A.; Saeb-Parsy, K.; Soares, F.A.; Schrumpf, E.; Melum, E.; Karlsen, T.H.; Bradley, J.A.; et al. Cholangiocytes derived from human induced pluripotent stem cells for disease modeling and drug validation. Nat. Biotechnol. 2015, 33, 845–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterling, J.A.; Lowenburg, H. Observations of infants with hepatic duct atresia and use of artificial duct prosthesis. Pediatric Clin. N. Am. 1962, 9, 485–504. [Google Scholar] [CrossRef]
- Uller, W.; Müller-Wille, R.; Loss, M.; Hammer, S.; Schleder, S.; Goessmann, H.; Wiggermann, P.; Stroszczynski, C.; Wohlgemuth, W. Percutaneous management of postoperative bile leaks with an ethylene vinyl alcohol copolymer (Onyx). RöFo-Fortschr. Auf Dem Geb. Der Röntgenstrahlen Und Der Bildgeb. Verfahr. 2013, 185, 1182–1187. [Google Scholar] [CrossRef] [Green Version]
- Chan, G.; Mooney, D.J. New materials for tissue engineering: Towards greater control over the biological response. Trends Biotechnol. 2008, 26, 382–392. [Google Scholar] [CrossRef]
- Singhi, A.D.; Slivka, A. Evaluation of indeterminate biliary strictures: Is it time to FISH or cut bait? Gastrointest. Endosc. 2016, 83, 1236–1238. [Google Scholar] [CrossRef] [Green Version]
- Hogan, W.; Geenen, J.; Dodds, W. Dysmotility disturbances of the biliary tract: Classification, diagnosis, and treatment. Semin. Liver Dis. 1987, 7, 302–310. [Google Scholar] [CrossRef]
- Taylor, D. Welcome to the journal of the mechanical behavior of biomedical materials. J. Mech. Behav. Biomed. Mater. 2008, 1, 1. [Google Scholar] [CrossRef]
- Duch, B.U.; Andersen, H.; Gregersen, H. Mechanical properties of the porcine bile duct wall. Biomed. Eng. Online 2004, 3, 23. [Google Scholar] [CrossRef] [Green Version]
- Li, W.C.; Zhang, H.M.; Li, J.; Dong, R.K.; Yao, B.C.; He, X.J.; Wang, H.Q.; Song, J. Comparison of biomechanical properties of bile duct between pigs and humans for liver xenotransplant. Transplant. Proc. 2013, 45, 741–747. [Google Scholar] [CrossRef]
- Park, S.-H.; Kang, B.-K.; Lee, J.E.; Chun, S.W.; Jang, K.; Kim, Y.H.; Jeong, M.A.; Kim, Y.; Kang, K.; Lee, N.K.; et al. Design and fabrication of A Thin-Walled Free-Form scaffold on the basis of medical image data and a 3d Printed Template: Its potential use in bile duct regeneration. ACS Appl. Mater. Interfaces 2017, 9, 12290–12298. [Google Scholar] [CrossRef]
- Tao, L.; Li, Q.; Ren, H.; Chen, B.; Hou, X.; Mou, L.; Zhou, S.; Zhou, J.; Sun, X.; Dai, J.; et al. Repair of extrahepatic bile duct defect using a collagen patch in a Swine model. Artif. Organs 2015, 39, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Nau, P.; Liu, J.; Ellison, E.C.; Hazey, J.W.; Henn, M.; Muscarella, P.; Narula, V.K.; Melvin, W.S. Novel reconstruction of the extrahepatic biliary tree with a biosynthetic absorbable graft. HPB 2011, 13, 573–578. [Google Scholar] [CrossRef] [Green Version]
- Rosen, M.; Ponsky, J.; Petras, R.; Fanning, A.; Brody, F.; Duperier, F. Small intestinal submucosa as a bioscaffold for biliary tract regeneration. Surgery. 2002, 132, 480. [Google Scholar] [CrossRef] [PubMed]
- Shiojiri, N.; Sugiyama, Y. Immunolocalization of extracellular matrix components and integrins during mouse liver development. Hepatology 2004, 40, 346–355. [Google Scholar] [CrossRef]
- Raynaud, P.; Carpentier, R.; Antoniou, A.; Lemaigre, F.P. Biliary differentiation and bile duct morphogenesis in development and disease. Int. J. Biochem. Cell Biol. 2011, 43, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Michalopoulos, G.K.; Barua, L.; Bowen, W.C. Transdifferentiation of rat hepatocytes into biliary cells after bile duct ligation and toxic biliary injury. Hepatology 2005, 41, 535–544. [Google Scholar] [CrossRef]
- Tysoe, O.C.; Justin, A.W.; Brevini, T.; Chen, S.E.; Mahbubani, K.T.; Frank, A.K.; Zedira, H.; Melum, E.; Saeb-Parsy, K.; Markaki, A.E.; et al. Isolation and propagation of primary human cholangiocyte organoids for the generation of bioengineered biliary tissue. Nat. Protoc. 2019, 14, 1884–1925. [Google Scholar] [CrossRef]
- Pawlowski, K.J. Endothelial cell seeding of polymeric vascular grafts. Front. Biosci. 2004, 9, 1412. [Google Scholar] [CrossRef] [Green Version]
- Kitagawa, T.; Yamaoka, T.; Iwase, R.; Murakami, A. Three-dimensional cell seeding and growth in radial-flow perfusion bioreactor for in vitro tissue reconstruction. Biotechnol. Bioeng. 2006, 93, 947–954. [Google Scholar] [CrossRef]
- Roh, J.D.; Nelson, G.N.; Udelsman, B.V.; Brennan, M.P.; Lockhart, B.; Fong, P.M.; Lopez-Soler, R.I.; Saltzman, W.M.; Breuer, C.K. Centrifugal seeding increases seeding efficiency and cellular distribution of bone mar-row stromal cells in porous biodegradable scaffolds. Tissue Eng. 2007, 13, 2743–2749. [Google Scholar] [CrossRef] [PubMed]
- Haykal, S.; Zhou, Y.; Marcus, P.; Salna, M.; Machuca, T.; Hofer, S.O.P.; Waddell, T.K. The effect of de-cellularization of tracheal allografts on leukocyte infiltration and of re-cellularization on regulatory T cell recruitment. Biomaterials 2013, 34, 5821–5832. [Google Scholar] [CrossRef] [PubMed]
- Duan, Z.-X.; Xie, L.-Q. Role of the Vascular Endothelial Growth Factor Pathway in Tumor Growth and Angiogenesis. World Chin. J. Dig. 2010, 18, 2894. [Google Scholar] [CrossRef]
- Cao, R.; Bjorndahl Meit, A.; Gallego, M.I.; Chen, S.; Religa, P.; Hansen, A.J.; Cao, Y. Hepatocyte growth factor is a lymphangiogenic factor with an indirect mechanism of action. Blood 2006, 107, 3531–3536. [Google Scholar] [CrossRef] [Green Version]
- Han, U.; Park, H.H.; Kim, Y.J.; Park, T.H.; Park, J.H.; Hong, J. Efficient Encapsulation and Sustained Release of Basic Fibroblast Growth Factor in Nanofilm: Extension of the Feeding Cycle of Human Induced Pluripotent Stem Cell Culture. ACS Appl. Mater. Interfaces 2017, 9, 25087–25097. [Google Scholar] [CrossRef]
- Lazaridis, K.N.; Strazzabosco, M.; LaRusso, N.F. The cholangiopathies: Disorders of biliary epithelia. Gastroenterology 2004, 127, 1565–1577. [Google Scholar] [CrossRef]
- Chilvery, S.; Bansod, S.; Saifi, M.A.; Godugu, C. Piperlongumine attenuates bile duct ligation-induced liver fibrosis in mice via inhibition of TGF-β1/Smad and EMT pathways. Int. Immunopharmacol. 2020, 88, 106909. [Google Scholar] [CrossRef]
- Oh, M.Y.; Kim, H.; Choi, Y.J.; Byun, Y.; Han, Y.; Kang, J.S.; Sohn, H.; Lee, J.M.; Kwon, W.; Jang, J.Y. Conversion surgery for initially unresectable extrahepatic biliary tract cancer. Ann. Hepato-Biliary-Pancreat. Surg. 2021, 25, 349–357. [Google Scholar] [CrossRef]
- Washington, K.; Rocha, F. Approach to Resectable Biliary Cancers. Curr. Treat. Options Oncol. 2021, 22, 97. [Google Scholar] [CrossRef]
- Patel, M.; Uboha, N.V. Treatment Approach to Adenocarcinoma of the Ampulla of Vater. Curr. Treat. Options Oncol. 2021, 22, 103. [Google Scholar] [CrossRef]
- Baiguera, S.; Arkhipva, S.; Yin, D.; Holterman, M.; Macchiarini, P. Rat bile duct decellularization. BioNanoScience 2016, 6, 578–584. [Google Scholar] [CrossRef]
- Schmidt, J.B.; Tranquillo, R.T. Tissue-engineered heart valves. In Heart Valves; Springer: Boston, MA, USA, 2013; pp. 261–280. [Google Scholar]
- Wang, F.; Maeda, Y.; Zachar, V.; Ansari, T.; Emmersen, J. Regeneration of the oesophageal muscle layer from oesophagus acellular matrix scaffold using adipose-derived stem cells. Biochem. Biophys. Res. Commun. 2018, 503, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Thurner, M.; Deutsch, M.; Janke, K.; Messner, F.; Kreutzer, C.; Beyl, S.; Couillard-Després, S.; Hering, S.; Troppmair, J.; Marksteiner, R. Generation of myogenic progenitor cell-derived smooth muscle cells for sphincter regeneration. Stem Cell Res. Ther. 2020, 11, 233. [Google Scholar] [CrossRef] [PubMed]
- Carpino, G.; Cardinale, V.; Onori, P.; Franchitto, A.; Berloco, P.B.; Rossi, M.; Wang, Y.; Semeraro, R.; Anceschi, M.; Brunelli, R.; et al. Biliary tree stem/progenitor cells in glands of extrahepatic and intraheptic bile ducts: An anatomical in situ study yielding evidence of maturational lineages. J. Anat. 2011, 220, 186–199. [Google Scholar] [CrossRef] [Green Version]
- Attisano, L.; Wrana, J.L. Signal integration in TGF-β, WNT, and Hippo pathways. F1000Prime Rep. 2013, 5, 17. [Google Scholar] [CrossRef]
- Gordillo, M.; Evans, T.; Gouon-Evans, V. Orchestrating liver development. Development 2015, 142, 2094–2108. [Google Scholar] [CrossRef] [Green Version]
- Valizadeh, A.; Majidinia, M.; Samadi-Kafil, H.; Yousefi, M.; Yousefi, B. The roles of signaling pathways in liver repair and regeneration. J. Cell. Physiol. 2019, 234, 14966–14974. [Google Scholar] [CrossRef]
- Lemaigre, F.P. Development of the Intrahepatic and Extrahepatic Biliary Tract: A Framework for Understanding Congenital Diseases. Annu. Rev. Pathol. Mech. Dis. 2020, 15, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Lozier, J.; McCright, B.; Gridley, T. Notch signaling regulates bile duct morphogenesis in mice. PLoS ONE 2008, 3, e1851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nijjar, S.S.; Wallace, L.; Crosby, H.A.; Hubscher, S.G.; Strain, A.J. Altered notch ligand expression in human liver disease. Am. J. Pathol. 2002, 160, 1695–1703. [Google Scholar] [CrossRef]
- Andersson, E.R.; Chivukula, I.V.; Hankeova, S.; Sjöqvist, M.; Tsoi, Y.L.; Ramsköld, D.; Masek, J.; Elmansuri, A.; Hoogendoorn, A.; Vazquez, E.; et al. Mouse Model of Alagille Syndrome and Mechanisms of Jagged1 Missense Mutations. Gastroenterology 2018, 154, 1080–1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, J.O.; Ko, S.; Monga, S.P.; Shin, D. Notch Inhibition Promotes Differentiation of Liver Progenitor Cells into Hepatocytes via sox9b Repression in Zebrafish. Stem Cells Int. 2019, 2019, 8451282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Si-Tayeb, K.; Lemaigre, F.P.; Duncan, S.A. Organogenesis and development of the liver. Dev. Cell 2010, 18, 175–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clotman, F.; Clotman, V.J.; Reber, M.; Cereghini, S.; Cassiman, D.; Jacquemin, P.; Roskams, T.; Rousseau, G.G.; Lemaigre, F.P. The onecut transcription factor HNF6 is required for normal development of the biliary tract. Development 2002, 129, 1819–1828. [Google Scholar] [CrossRef]
- Zohorsky, K.; Mequanint, K. Designing Biomaterials to Modulate Notch Signaling in Tissue Engineering and Regenerative Medicine. Tissue Eng. Part B Rev. 2020, 27, 383–410. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Zhou, Y.; Hu, T.; Zhang, H.; Shen, M.; Cheng, P.; Dai, W.; Wang, F.; Chen, K.; Zhang, Y.; et al. Notch Signaling Coordinates Progenitor Cell-Mediated Biliary Regeneration Following Partial Hepatectomy. Sci. Rep. 2016, 6, 22754. [Google Scholar] [CrossRef] [Green Version]
- L’Heureux, N.; McAllister, T.N.; de la Fuente, L.M. Human tissue-engineered blood vessels for adult arterial revascularization. N. Engl. J. Med. 2007, 357, 1451–1453. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author, Year, Country | BDI Model | Materials | Limitations |
|---|---|---|---|
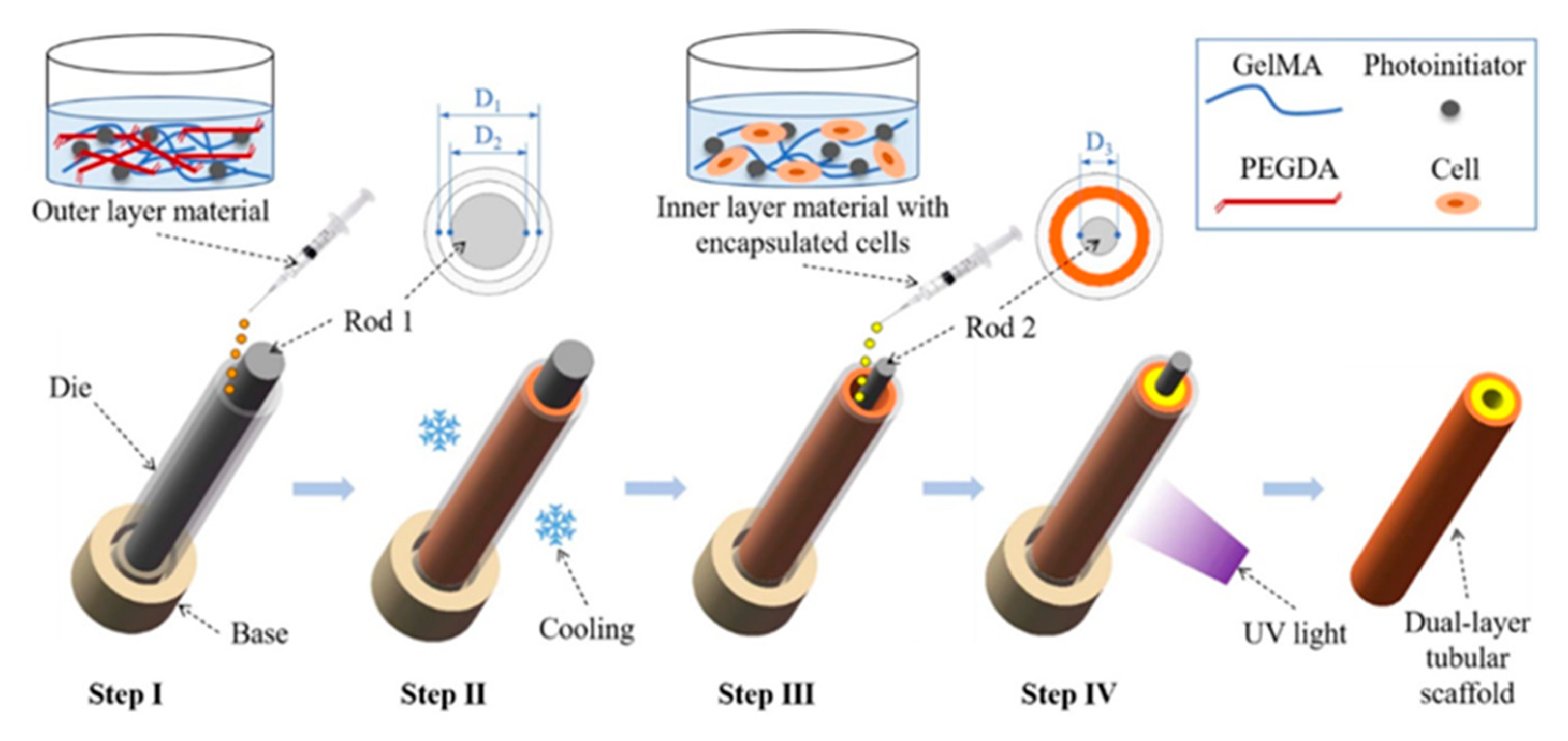
| Liu, X. et al., 2021, China [38] | None | BMSC-laden inner GelMA layer and GelMA/PEGDA outer layer | In vitro only, interface adhesion between the two layers is not perfect |
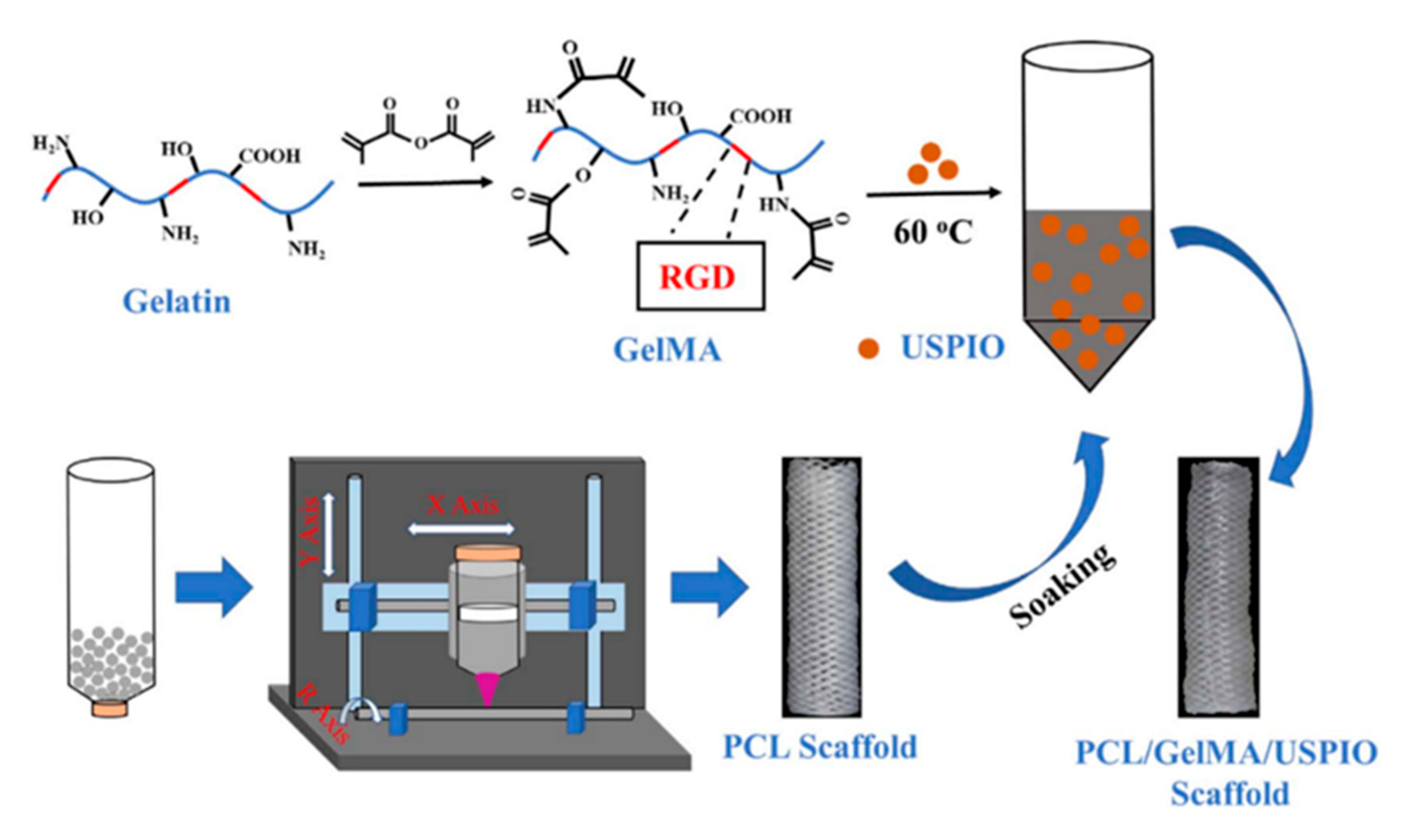
| Li, H. et al., 2020, China [15] | None | USPIO nanoparticle-loaded and GelMA-coated 3D-printed PCL tubular scaffolds | In vitro only, USPIO inhibited BMSC proliferation, mechanisms of BMSC growth on GelMA not investigated |
| Park, S.H. et al., 2017, S. Korea [74] | Rabbit common bile duct replacement | 3D-printed PVA bile duct replica dip-coated in PCL before PVA removal | Mechanical inadequacies, anastomotic stenosis, mild dilatation of intrahepatic bile duct |
| Sampaziotis, F. et al., 2017, UK [48] | Mouse extrahepatic BDI | 3D cholangiocytic-like cell organoid-seeded collagen tubes | Complex five-step method, unclear impact of long-term in vitro culture on phenotype |
| Zong, C. et al., 2017, China [29] | Pig extrahepatic BDI | Compact PCL inner layer and multiparous PLGA outer layer | Implants had initial impact on liver function, inflammation, and fibrous hyperplasia after long-term transplant |
| Struecker, B. et al., 2016, Germany [17] | Pig extrahepatic BDI | Decellularized aorta abdominal aorta, recellularization with bile duct cells | Short experimental duration (14 days), biochemical parameters deviation from normal range, partial implant stenosis |
| Cheng, Y. et al., 2016, China [24] | Pig extrahepatic BDI | Decellularized ureteral graft | Bile duct stenosis, intrahepatic and extrahepatic bile duct dilatation, stents or T-tubes required |
| Tao, L. et al., 2014, China [75] | Pig extrahepatic BDI | Freeze-dried collagen membranes | Limited to mesh, fast degradation increased risk of bile leakage and collapse, morphological issues, risk of stenosis. |
| Pérez Alonso, A.J. et al., 2013, Spain [19] | Guinea pig extrahepatic BDI | Three-dimensional collagen tubes coated with 2% agarose hydrogel | Bile duct marker expression decreased, scaffold not absorbed and granuloma formation at anastomosis site |
| Li, Q. et al., 2012, China [18] | Pig extrahepatic BDI | CBD-bFGF loading collagen membranes | Limited to mesh, fast degradation increased risk of bile leakage and collapse, morphological issues, risk of stenosis |
| Nau, P. et al., 2011, USA [76] | Dog extrahepatic BDI | Co-polymer of PGA and trimethylene carbonate | Bile leakage, obstruction, cholangitis |
| Aikawa, M. et al., 2010, Japan [16] | Pig extrahepatic BDI | Bioabsorbable copolymer patch of PLA/PCL reinforced with PGA fibers | Adhesion, anastomosis deformation, slow cell infiltration |
| Nakashima, S. et al., 2007, Japan [20] | Dog extrahepatic BDI | Collagen sponge reinforced with polypropylene mesh | Non-biodegradable stents required surgical removal after 2 weeks, prone to stenosis |
| Barralet, J.E. et al., 2003, UK [28] | None | PGA fiber dip-coated with three layers of PCL | In vitro only |
| Rosen, M. et al., 2002, USA [77] | Dog extrahepatic BDI | Decellularised small intestine submucosa | Lacked mechanical strength, observed collapse, anastomotic stenosis, and fibrosis, zoonotic risk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, Q.; Shen, Z.; Liang, X.; He, Y.; Kong, D.; Midgley, A.C.; Wang, K. Progress and Current Limitations of Materials for Artificial Bile Duct Engineering. Materials 2021, 14, 7468. https://doi.org/10.3390/ma14237468
Sun Q, Shen Z, Liang X, He Y, Kong D, Midgley AC, Wang K. Progress and Current Limitations of Materials for Artificial Bile Duct Engineering. Materials. 2021; 14(23):7468. https://doi.org/10.3390/ma14237468
Chicago/Turabian StyleSun, Qiqi, Zefeng Shen, Xiao Liang, Yingxu He, Deling Kong, Adam C. Midgley, and Kai Wang. 2021. "Progress and Current Limitations of Materials for Artificial Bile Duct Engineering" Materials 14, no. 23: 7468. https://doi.org/10.3390/ma14237468