
Comparative Evaluation of Mineral Trioxide Aggregate Obturation Using Four Different Techniques—A Laboratory Study



Abstract
:1. Introduction
2. Materials and Methods
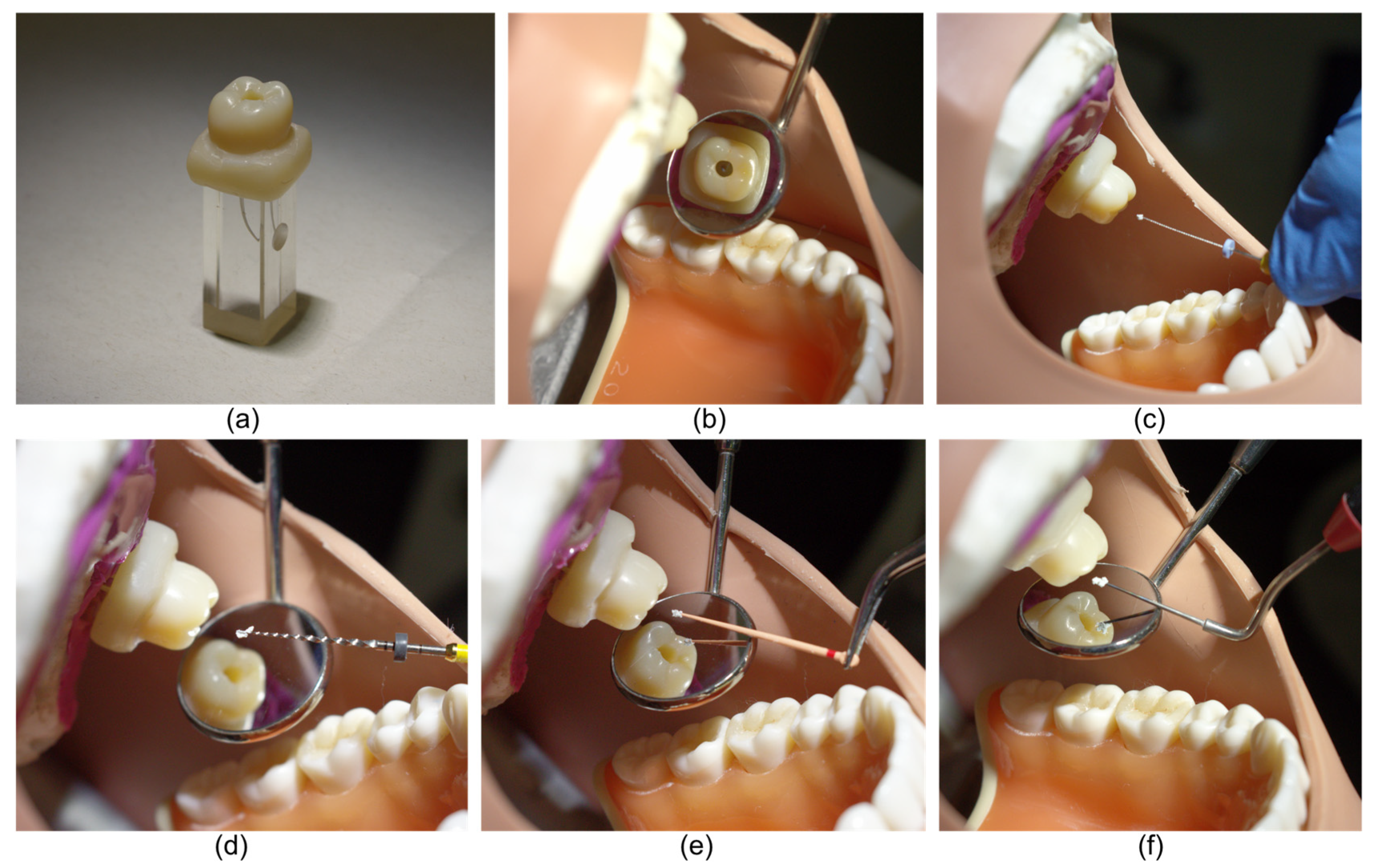
2.1. Preparation of Samples
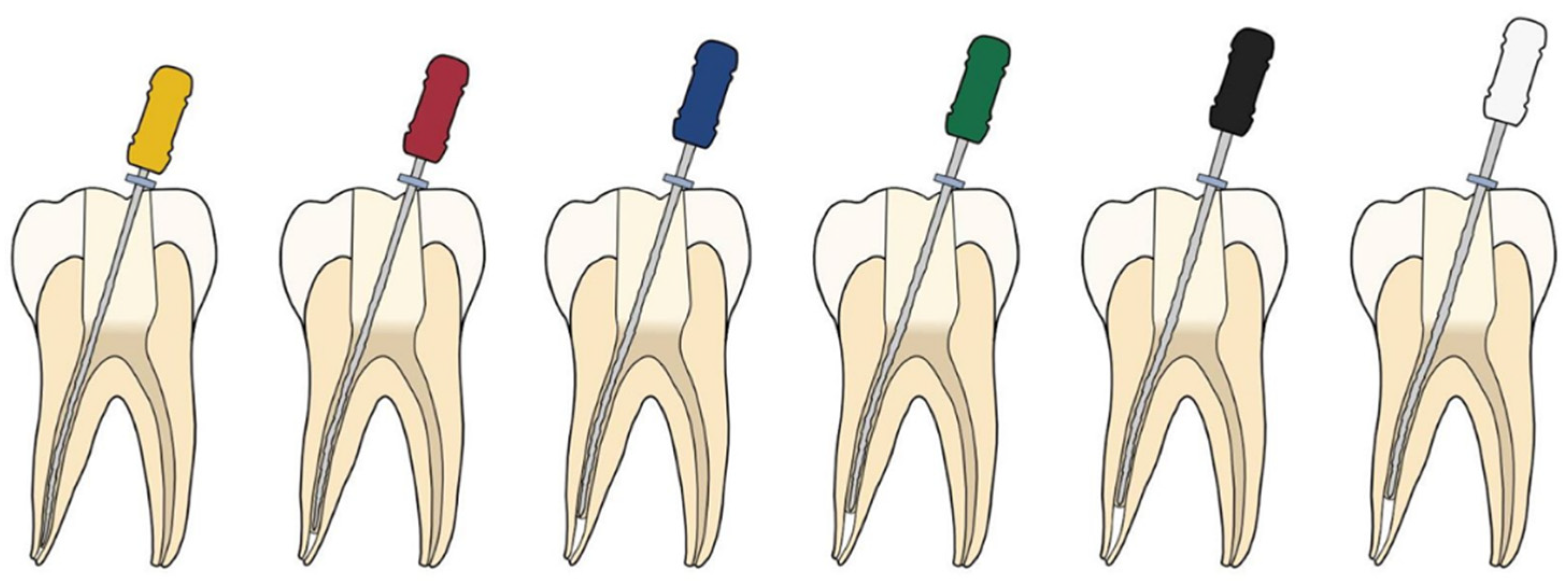
2.2. Experimental Groups
2.2.1. Lawaty Group
2.2.2. Auger Group
2.2.3. GP Group
2.2.4. Plugger Group
2.3. Obturation of Canals
2.4. Obturation Time
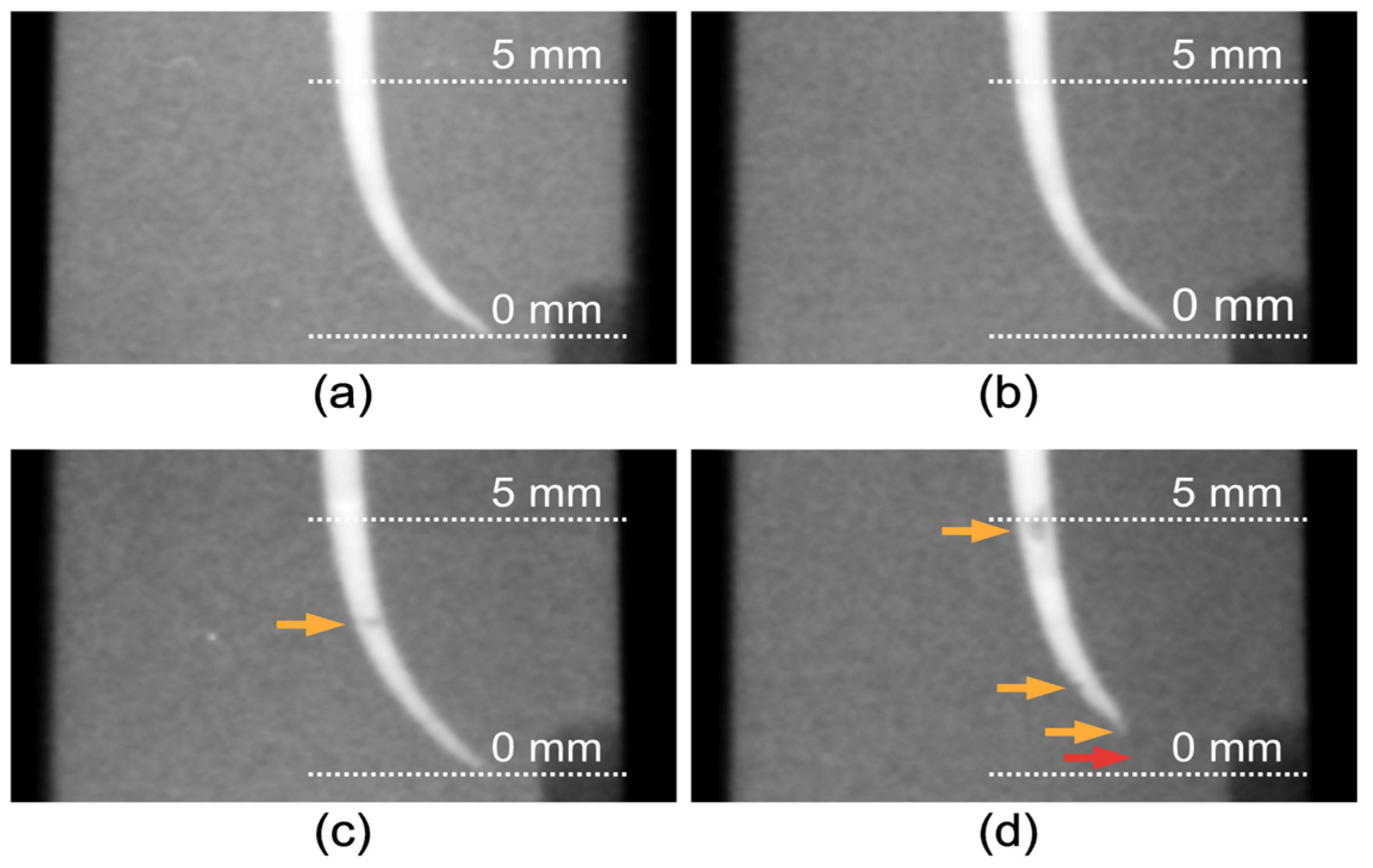
2.5. Evaluation of Canal Fillings
3. Results
3.1. Obturation Mass
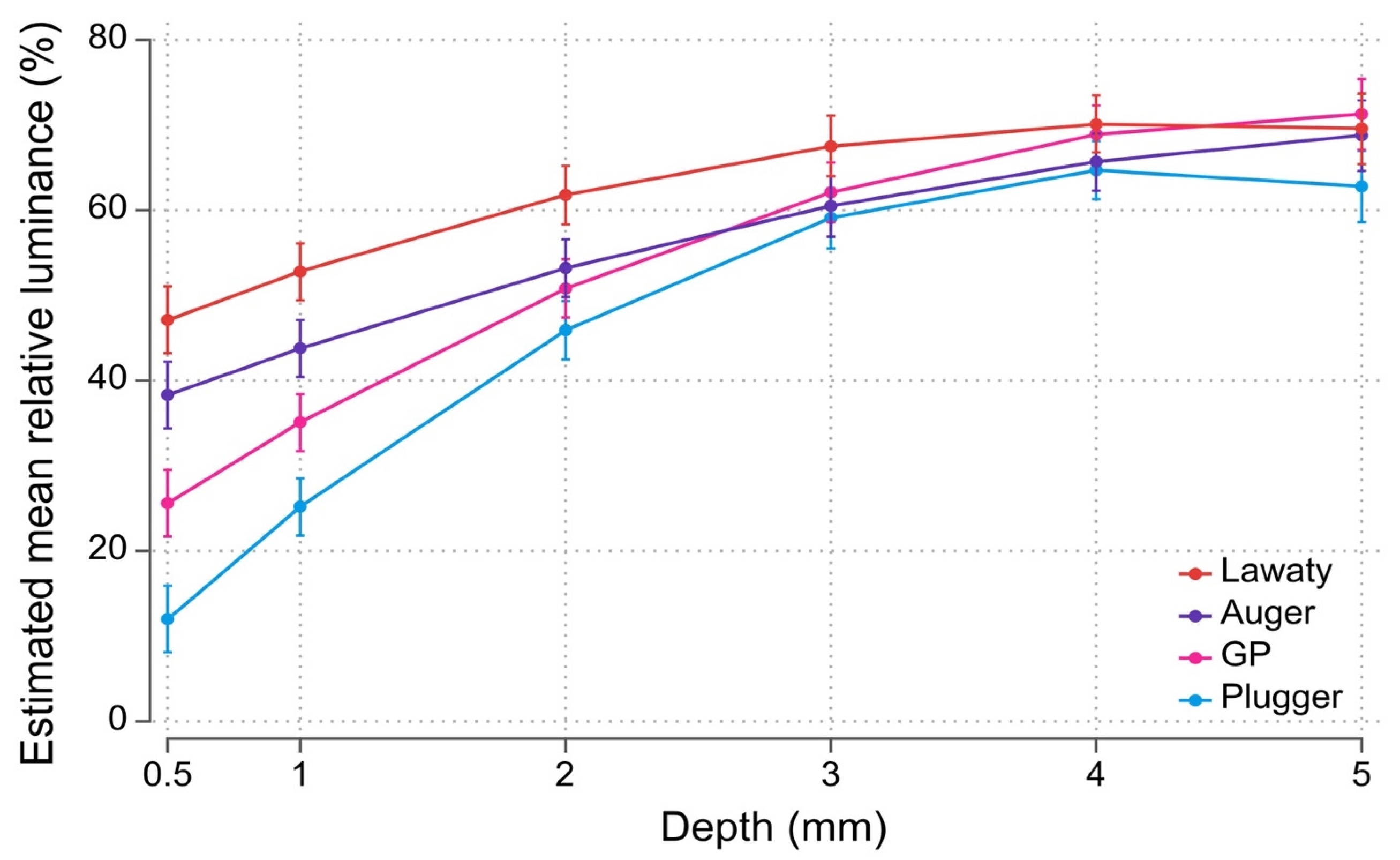
3.2. Radiopacity (Relative Luminance)
3.3. Obturation Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parirokh, M.; Torabinejad, M. Mineral trioxide aggregate: A comprehensive literature review—Part III: Clinical applications, drawbacks, and mechanism of action. J. Endod. 2010, 36, 400–413. [Google Scholar] [CrossRef]
- Parirokh, M.; Torabinejad, M. Mineral trioxide aggregate: A comprehensive literature review—Part I: Chemical, physical, and antibacterial properties. J. Endod. 2010, 36, 16–27. [Google Scholar] [CrossRef]
- Bogen, G.; Kuttler, S. Mineral trioxide aggregate obturation: A review and case series. J. Endod. 2009, 35, 777–790. [Google Scholar] [CrossRef]
- Bogen, G.; Lawaty, I.; Chandler, N. MTA root canal obturation. In Mineral Trioxide Aggregate: Properties and Clinical Applications; Torabinejad, M., Ed.; Wiley-Blackwell: Oxford, UK, 2014; pp. 207–249. [Google Scholar] [CrossRef]
- Sarkar, N.K.; Caicedo, R.; Ritwik, P.; Moiseyeva, R.; Kawashima, I. Physicochemical basis of the biologic properties of mineral trioxide aggregate. J. Endod. 2005, 31, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Al-Hezaimi, K.; Naghshbandi, J.; Oglesby, S.; Simon, J.H.; Rotstein, I. Human saliva penetration of root canals obturated with two types of mineral trioxide aggregate cements. J. Endod. 2005, 31, 453–456. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Shimizu, A.; Ebisu, S. MTA for obturation of mandibular central incisors with open apices: Case report. J. Endod. 2004, 30, 120–122. [Google Scholar] [CrossRef]
- D’Arcangelo, C.; D’Amario, M. Use of MTA for orthograde obturation of nonvital teeth with open apices: Report of two cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 104, e98–e101. [Google Scholar] [CrossRef]
- Aslan, T.; Esim, E.; Üstün, Y.; Özkan, H.D. Evaluation of stress distributions in mandibular molar teeth with different iatrogenic root perforations repaired with Biodentine or MTA: A finite element analysis study. J. Endod. 2021, 47, 631–640. [Google Scholar] [CrossRef]
- Tsai, Y.-L.; Ian, W.-H.; Jeng, J.-H. Treatment of pulp floor and stripping perforation by mineral trioxide aggregate. J. Formos. Med. Assoc. 2006, 105, 522–526. [Google Scholar] [CrossRef] [Green Version]
- Keleş, A.; Torabinejad, M.; Keskin, C.; Sah, D.; Uzun, İ.; Alçin, H. Micro-CT evaluation of voids using two root filling techniques in the placement of MTA in mesial root canals of Vertucci type II configuration. Clin. Oral Investig. 2017, 22, 1907–1913. [Google Scholar] [CrossRef] [PubMed]
- Woelber, J.P.; Bruder, M.; Tennert, C.; Wrbas, K.-T. Assessment of endodontic treatment of c-shaped root canals. Swiss Dent. J. 2014, 124, 11–15. [Google Scholar] [PubMed]
- Teixidó, M.; Abella, F.; Duran-Sindreu, F.; Moscoso, S.; Roig, M. The use of cone-beam computed tomography in the preservation of pulp vitality in a maxillary canine with type 3 dens invaginatus and an associated periradicular lesion. J. Endod. 2014, 40, 1501–1504. [Google Scholar] [CrossRef] [PubMed]
- Kfir, A.; Telishevsky-Strauss, Y.; Leitner, A.; Metzger, Z. The diagnosis and conservative treatment of a complex type 3 dens invaginatus using cone beam computed tomography (CBCT) and 3D plastic models. Int. Endod. J. 2012, 46, 275–288. [Google Scholar] [CrossRef] [PubMed]
- Habibi, M.; Ghoddusi, J.; Habibi, A.; Mohtasham, N. Healing process following application of set or fresh mineral trioxide aggregate as a root-end filling material. Eur. J. Dent. 2011, 5, 19–23. [Google Scholar] [CrossRef] [Green Version]
- Saunders, W.P.; Saunders, E.M. Coronal leakage as a cause of failure in root-canal therapy: A review. Endod. Dent. Traumatol. 1994, 10, 105–108. [Google Scholar] [CrossRef]
- Yoo, J.S.; Chang, S.-W.; Oh, S.R.; Perinpanayagam, H.; Lim, S.-M.; Yoo, Y.-J.; Oh, Y.-R.; Woo, S.-B.; Han, S.-H.; Zhu, Q.; et al. Bacterial entombment by intratubular mineralization following orthograde mineral trioxide aggregate obturation: A scanning electron microscopy study. Int. J. Oral Sci. 2014, 6, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Alsalleeh, F.; Chung, N.; Stephenson, L. Antifungal activity of Endosequence root repair material and mineral trioxide aggregate. J. Endod. 2014, 40, 1815–1819. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Noula, G.; Lambrianidis, T. Ex vivo study of the efficiency of two techniques for the removal of mineral trioxide aggregate used as a root canal filling material. J. Endod. 2008, 34, 1239–1242. [Google Scholar] [CrossRef]
- El-Ma’aita, A.M.; Qualtrough, A.J.E.; Watts, D.C. A micro-computed tomography evaluation of mineral trioxide aggregate root canal fillings. J. Endod. 2012, 38, 670–672. [Google Scholar] [CrossRef]
- Jho, W.; Park, J.W.; Kim, E.; Song, M.; Seo, D.G.; Yang, D.K.; Shin, S.J. Comparison of root canal filling quality by mineral trioxide aggregate and gutta percha cones/AH plus sealer. Dent. Mater. J. 2016, 35, 644–650. [Google Scholar] [CrossRef] [Green Version]
- Alsulaimani, R.S. Single-visit endodontic treatment of mature teeth with chronic apical abscesses using mineral trioxide aggregate cement: A randomized clinical trial. BMC Oral Health 2016, 16, 78. [Google Scholar] [CrossRef] [Green Version]
- Vizgirda, P.J.; Liewehr, F.R.; Patton, W.R.; McPherson, J.C.; Buxton, T.B. A comparison of laterally condensed gutta-percha, thermoplasticized gutta-percha, and mineral trioxide aggregate as root canal filling materials. J. Endod. 2004, 30, 103–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giovarruscio, M.; Uccioli, U.; Malentacca, A.; Koller, G.; Foschi, F.; Mannocci, F. A technique for placement of apical MTA plugs using modified Thermafil carriers for the filling of canals with wide apices. Int. Endod. J. 2013, 46, 88–97. [Google Scholar] [CrossRef]
- Aminoshariae, A.; Hartwell, G.R.; Moon, P.C. Placement of mineral trioxide aggregate using two different techniques. J. Endod. 2003, 29, 679–682. [Google Scholar] [CrossRef] [PubMed]
- Yeung, P.; Liewehr, F.R.; Moon, P.C. A quantitative comparison of the fill density of MTA produced by two placement techniques. J. Endod. 2006, 32, 456–459. [Google Scholar] [CrossRef] [PubMed]
- Krell, K.; Madison, S. The use of the messing gun in placing calcium hydroxide powder. J. Endod. 1985, 11, 233–234. [Google Scholar] [CrossRef]
- Chang, S.W.; Oh, T.S.; Lee, W.; Cheung, G.S.; Kim, H.C. Long-term observation of the mineral trioxide aggregate extrusion into the periapical lesion: A case series. Int. J. Oral Sci. 2013, 5, 54–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, W.N.; Nicholson, T.; Kahler, B.; Walsh, L.J. Mineral trioxide aggregate-A review of properties and testing methodologies. Materials 2017, 10, 1261. [Google Scholar] [CrossRef] [Green Version]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, M.K.; R’oris, A.; Barkis, D.; Wesselink, P.R. Prevalence and extent of long oval canals in the apical third. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 89, 739–743. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, H.M.A.; Rossi-Fedele, G. Preferred reporting items for root and canal anatomy in the human dentition (PROUD 2020)-A systematic review and a proposal for a standardized protocol. Eur. Endod. J. 2020, 5, 159–176. [Google Scholar] [CrossRef]
- Duarte, M.A.H.; de Oliveira El Kadre, G.D.; Vivan, R.R.; Guerreiro-Tanomaru, J.M.; Filho, M.T.; de Moraes, I.G. Radiopacity of Portland cement associated with different radiopacifying agents. J. Endod. 2009, 35, 737–740. [Google Scholar] [CrossRef]
- Hartmann, R.C.; Fensterseifer, M.; Peters, O.A.; De Figueiredo, J.A.P.; Gomes, M.S.; Rossi-Fedele, G. Methods for measurement of root canal curvature: A systematic and critical review. Int. Endod. J. 2019, 52, 169–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loizides, A.; Eliopoulos, D.; Kontakiotis, E. Root canal transportation with a Ni-Ti rotary file system and stainless steel hand files in simulated root canals. Quintessence Int. 2006, 37, 369–374. [Google Scholar]
- Alodeh, M.H.; Doller, R.; Dummer, P.M. Shaping of simulated root canals in resin blocks using the step-back technique with K-files manupulated in a simple in/out filling motion. Int. Endod. J. 1989, 22, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Fanibunda, K.B. A method of measuring the volume of human dental pulp cavities. Int. Endod. J. 1986, 19, 194–197. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 2. Influence of clinical factors. Int. Endod. J. 2007, 41, 6–31. [Google Scholar] [CrossRef]
- Al-Kahtani, A.; Shostad, S.; Schifferle, R.; Bhambhani, S. In-vitro evaluation of microleakage of an orthograde apical plug of mineral trioxide aggregate in permanent teeth with simulated immature apices. J. Endod. 2005, 31, 117–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Placement Technique | Difference in Mean Obturation Mass (mg) | Standard Error | (95% Confidence Interval) | p-Value | |
|---|---|---|---|---|---|
| Lawaty | 5.96 | 0.81 | 4.31 | 7.60 | <0.01 * |
| Auger | 6.67 | 0.81 | 5.03 | 8.31 | <0.01 * |
| GP | 5.90 | 0.81 | 4.26 | 7.54 | <0.01 * |
| Position from Apical End (mm) | Placement Technique | Difference in Mean Relative Luminance (%) | Standard Error | (95% Confidence Interval) | p-Value | |
|---|---|---|---|---|---|---|
| 0.5 | Lawaty Auger GP | 35.10 26.26 13.56 | 2.83 2.83 2.83 | 29.55 20.71 8.01 | 40.64 31.80 19.10 | <0.001 * <0.001 * <0.001 * |
| 1 | Lawaty Auger GP | 27.60 18.57 9.91 | 2.43 2.43 2.43 | 22.83 13.80 5.14 | 32.37 23.34 14.68 | <0.001 * <0.001 * <0.001 * |
| 2 | Lawaty Auger GP | 15.86 7.27 4.93 | 2.47 2.47 2.47 | 11.02 2.44 0.09 | 20.70 12.11 9.77 | <0.001 * 0.003 * 0.046 * |
| 3 | Lawaty Auger GP | 8.47 1.41 3.03 | 2.55 2.55 2.55 | 3.48 −3.60 −1.97 | 13.47 6.41 8.03 | 0.001 * 0.581 0.235 |
| 4 | Lawaty Auger GP | 5.45 0.97 4.21 | 2.43 2.43 2.43 | 0.69 −3.79 −0.55 | 10.20 5.73 8.96 | 0.025 * 0.690 0.083 |
| 5 | Lawaty Auger GP | 6.78 5.96 8.47 | 3.01 3.01 3.01 | 0.87 0.06 2.56 | 12.67 11.86 14.37 | 0.025 * 0.048 0.005 |
| Placement Technique | Difference in Mean Obturation Times (mins) | Standard Error | (95% Confidence Interval) | p-Value | |
|---|---|---|---|---|---|
| Lawaty | 3.84 | 0.15 | 3.54 | 4.15 | <0.0001 * |
| Auger | 0.03 | 0.09 | −0.16 | 0.22 | 0.7835 * |
| GP | 0.03 | 0.06 | −0.10 | 0.16 | 0.6551 * |
| Author (Year) | Tooth Model | Benchtop * vs. Clinical Simulation | Technique Used | Method of Measurement | Finding |
|---|---|---|---|---|---|
| Keleş et al. [11] | Moderately curved (15–20 degrees) mesial roots from mandibular molars with a Vertucci type II canal configuration prepared with Reciproc R25 (size 25, variable taper) | Benchtop | Plugger, ultrasonically activated plugger | Micro-CT—percentage of voids | No significant difference between techniques at apical 3 mm; no significant difference between the two techniques at the coronal half of the isthmus |
| El-Ma’aita et al. [20] | Minimally curved single canal; anterior human teeth with crowns removed prepared with Protaper F5 (size 50, variable taper) | Benchtop | Plugger ultrasonic activated plugger | Micro-CT—percentage of voids | Ultrasonic compaction produced significantly less-dense root fillings |
| Yeung et al. [26] | Acrylic blocks with 30-degree curved canals and straight canals prepared with K3 (size 45, 6% taper) | Benchtop | Plugger ultrasonic activated plugger | Fill density using difference in mass | Pluggers with US activation resulted in an MTA fill that was statistically significantly heavier |
| Aminoshariae et al. [25] | Polypropylene tubes with an inner diameter of 0.7 mm at the apical tip | Benchtop | Plugger direct ultrasonic placement | Void scores using radiographs and light microscope | Pluggers resulted in better adaptation to the tube walls and fewer voids |
| Present study | Acrylic blocks with 30-degree curved canals prepared to F2 (size 25, variable taper); blocks have resin crowns and are mounted in a phantom head | Clinical simulation | Lawaty auger GP plugger | Fill density using difference in mass relative luminance (radiopacity); obturation time | The Lawaty technique has the highest relative luminance and mass but also consumes the most time; the plugger technique has the lowest relative luminance and mass |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathew, A.I.; Lee, S.C.; Rossi-Fedele, G.; Bogen, G.; Nagendrababu, V.; Ha, W.N. Comparative Evaluation of Mineral Trioxide Aggregate Obturation Using Four Different Techniques—A Laboratory Study. Materials 2021, 14, 3126. https://doi.org/10.3390/ma14113126
Mathew AI, Lee SC, Rossi-Fedele G, Bogen G, Nagendrababu V, Ha WN. Comparative Evaluation of Mineral Trioxide Aggregate Obturation Using Four Different Techniques—A Laboratory Study. Materials. 2021; 14(11):3126. https://doi.org/10.3390/ma14113126
Chicago/Turabian StyleMathew, Abhishek Isaac, Silvia Chamin Lee, Giampiero Rossi-Fedele, George Bogen, Venkateshbabu Nagendrababu, and William Nguyen Ha. 2021. "Comparative Evaluation of Mineral Trioxide Aggregate Obturation Using Four Different Techniques—A Laboratory Study" Materials 14, no. 11: 3126. https://doi.org/10.3390/ma14113126