
Clinical Performance of CAD/CAM All-Ceramic Tooth-Supported Fixed Dental Prostheses: A Systematic Review and Meta-Analysis

 ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
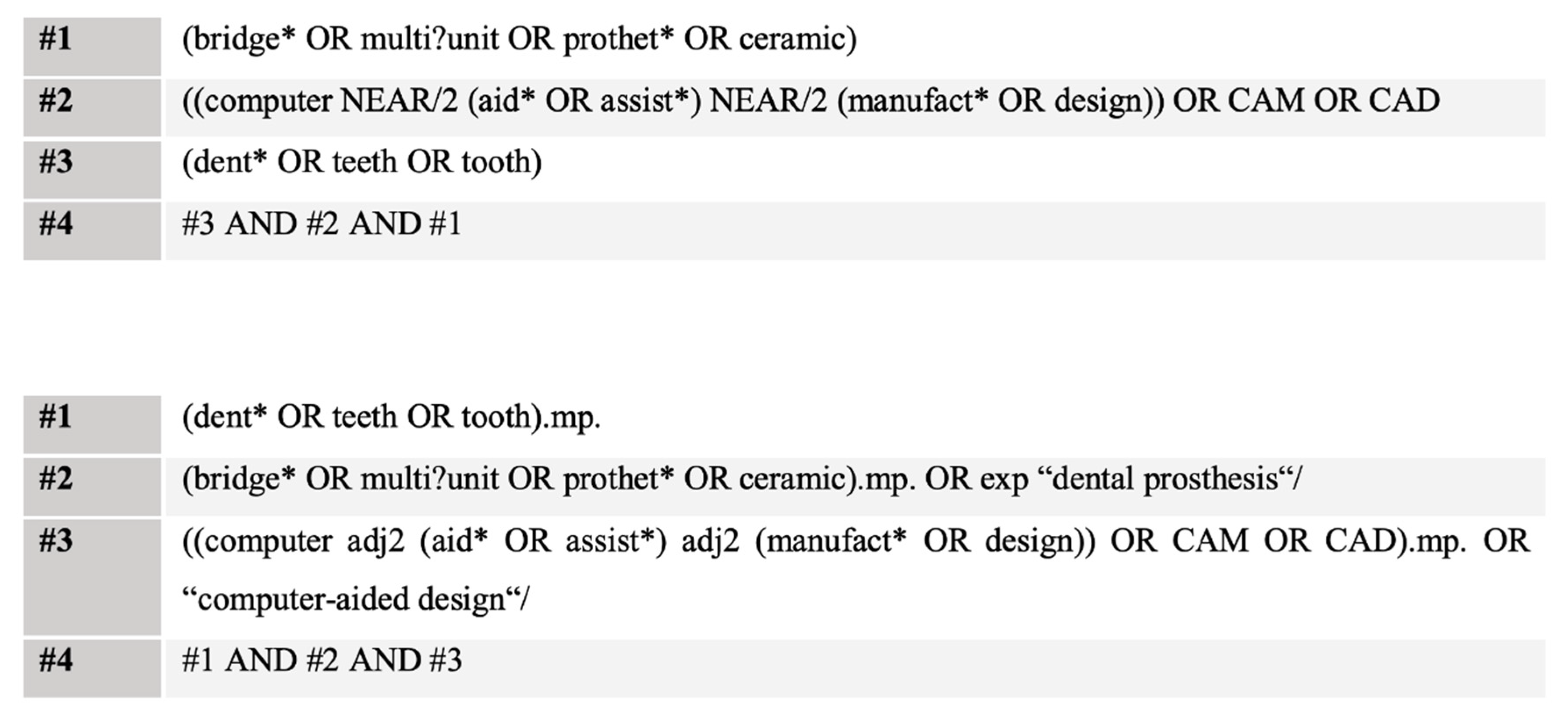
2.1. Data Collection
- Metal and metal-ceramic restorations as an intervention.
- Implant-borne prostheses as an intervention.
- Hybrid bridges as an intervention.
- Cantilever bridges as an intervention.
- Crowns.
- Animal studies.
- In vitro studies.
- Retrospective studies.
- Case studies.
- Languages other than German or English.
2.2. Assessment of the Risk of Bias
2.3. Statistics
3. Results
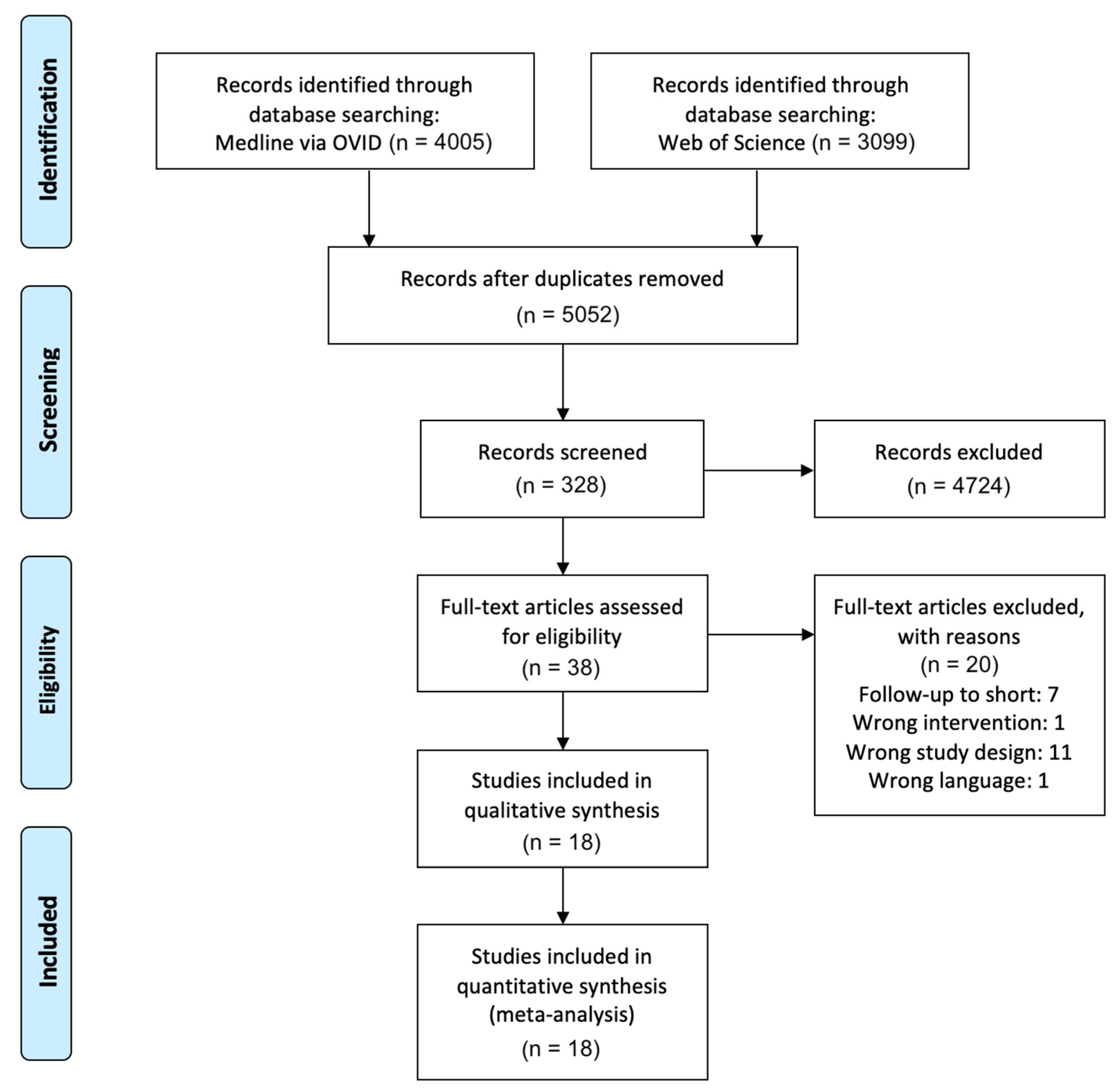
3.1. Study Selection and Study Characteristics
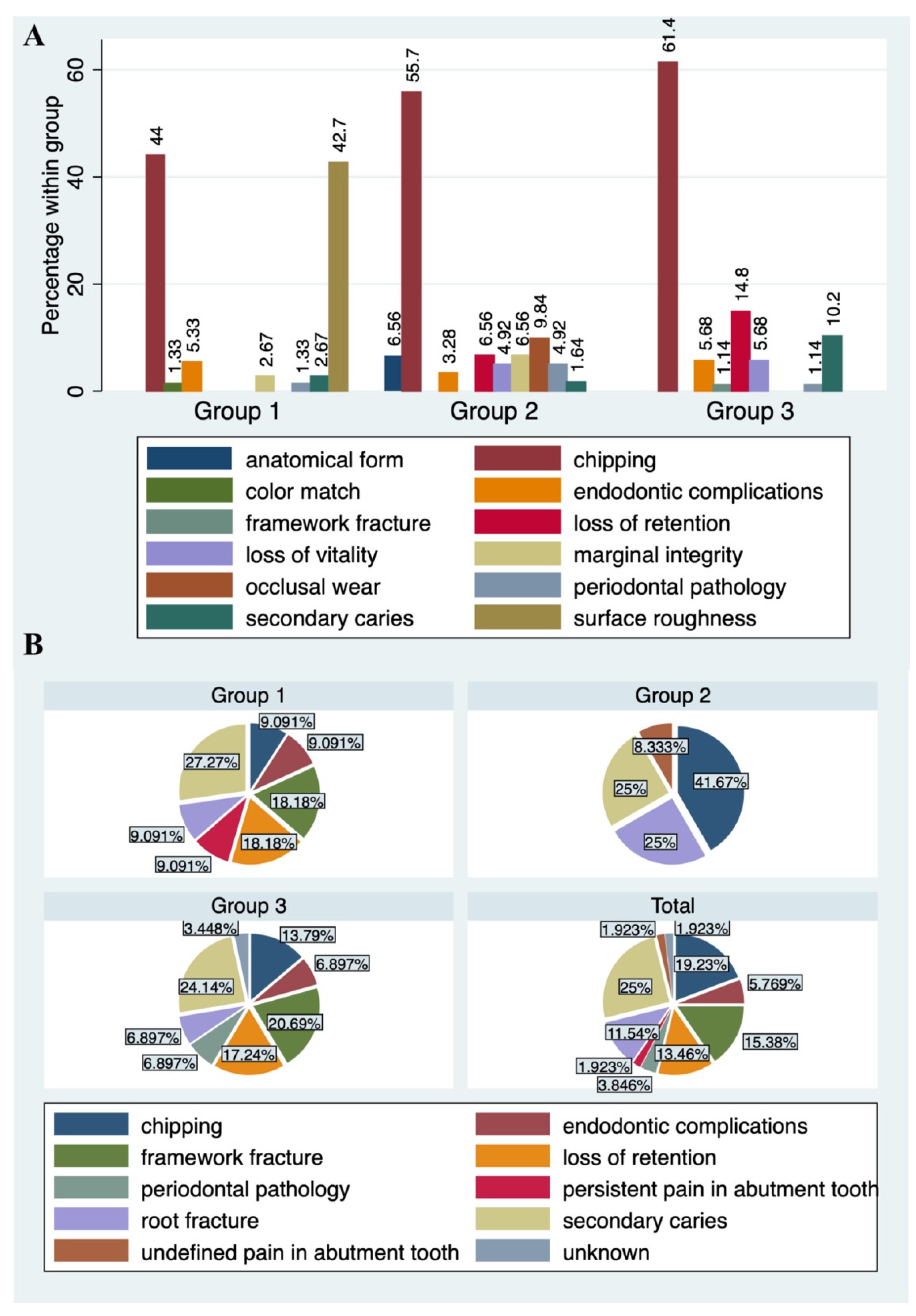
3.2. Qualitative Synthesis of Results
3.2.1. Group 1
3.2.2. Group 2
3.2.3. Group 3
3.3. Quantitative Synthesis of Results
3.3.1. Group 1
3.3.2. Group 2
3.3.3. Group 3
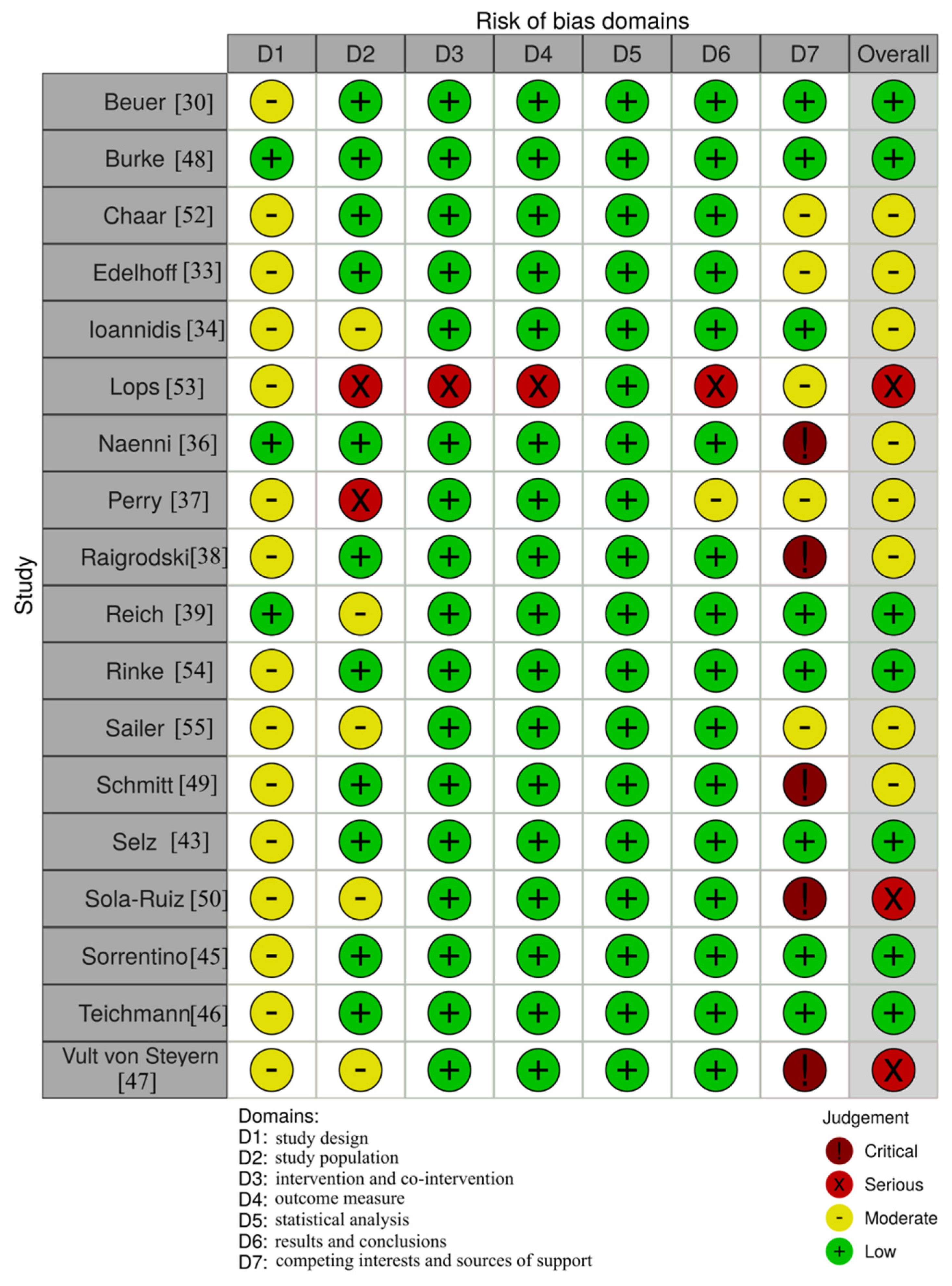
3.4. Assessment of the Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pjetursson, B.E.; Valente, N.A.; Strasding, M.; Zwahlen, M.; Liu, S.; Sailer, I. A Systematic Review of the Survival and Complication Rates of Zirconia-Ceramic and Metal-Ceramic Single Crowns. Clin. Oral Implants Res. 2018, 29 (Suppl. 16), 199–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heintze, S.D.; Rousson, V. Survival of Zirconia- and Metal-Supported Fixed Dental Prostheses: A Systematic Review. Int. J. Prosthodont 2010, 23, 493–502. [Google Scholar] [PubMed]
- Aziz, A.; El-Mowafy, O.; Paredes, S. Clinical Outcomes of Lithium Disilicate Glass-Ceramic Crowns Fabricated with CAD/CAM Technology: A Systematic Review. Dent. Med. Probl. 2020, 57, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Al-Haj Husain, N.; Özcan, M.; Molinero-Mourelle, P.; Joda, T. Clinical Performance of Partial and Full-Coverage Fixed Dental Restorations Fabricated from Hybrid Polymer and Ceramic CAD/CAM Materials: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2107. [Google Scholar] [CrossRef]
- Malament, K.A.; Natto, Z.S.; Thompson, V.; Rekow, D.; Eckert, S.; Weber, H.-P. Ten-Year Survival of Pressed, Acid-Etched e.Max Lithium Disilicate Monolithic and Bilayered Complete-Coverage Restorations: Performance and Outcomes as a Function of Tooth Position and Age. J. Pros. Dent. 2019, 121, 782–790. [Google Scholar] [CrossRef] [Green Version]
- Gautam, C.; Joyner, J.; Gautam, A.; Rao, J.; Vajtai, R. Zirconia Based Dental Ceramics: Structure, Mechanical Properties, Biocompatibility and Applications. Dalt. Trans. 2016, 45, 19194–19215. [Google Scholar] [CrossRef]
- Kern, M.; Kern, M. So Hält Keramischer Stahl. Dent. Mag. 2008, 1, 28–34. [Google Scholar]
- Strub, J.R.; Kern, M.; Türp, J.C.; Witkowski, S.; Heydecke, G.; Wolfahrt, S. Currciulum Prothetik, 4th ed.; Quintessenz Verlags-GmbH: Berlin, Germany, 2011; Volume 2. [Google Scholar]
- Pospiech, P. Chipping–Systemimmanente Oder Verarbeitungsbedingte Probleme. Quintessenz 2010, 61, 173–181. [Google Scholar]
- Abboud, M. Stark H Vollkeramische Restaurationen Im Front-Und Seitenzahnbereich. Quintessenz 2003, 54, 1295–1302. [Google Scholar]
- Kern, M.; Kohal, R.J.; Mehl, A.; Pospiech, P.; Frankenberger, R.; Reiss, B.; Wiedhahn, K.; Kunzelmann, K.H. Vollkeramik Auf Einen Blick: Leitfaden Zur Indikation, Werkstoffauswahl, Vorbereitung Und Eingliederung von Vollkeramischen Restaurationen; Arbeitsgemeinschaft für Keramik in der Zahnheilkunde: Malsch, Germany, 2010; ISBN 3-00-017195-9. [Google Scholar]
- Kunzelmann, K.-H.; Pospiech, P.; Kern, M. Hat Sich Vollkeramik Bewährt. Eine Positionsp. Kons Prothetik. Dentalfresh 2007, 2, 16–19. [Google Scholar]
- Poticny, D.J.; Klim, J. CAD/CAM in-Office Technology: Innovations after 25 Years for Predictable, Esthetic Outcomes. J. Am. Dent. Assoc. 2010, 141 (Suppl. 2), 5S–9S. [Google Scholar] [CrossRef]
- Beuer, F.; Schweiger, J.; Edelhoff, D. Digital Dentistry: An Overview of Recent Developments for CAD/CAM Generated Restorations. Br. Dent. J. 2008, 204, 505–511. [Google Scholar] [CrossRef]
- Strietzel, R.; Lahl, C. CAD/CAM-Systeme in Labor Und Praxis; Verlag Neuer Merkur GmbH: Planegg, Germany, 2007; ISBN 3-937346-41-4. [Google Scholar]
- Harsono, M.; Simon, J.F.; Stein, J.M.; Kugel, G. Evolution of Chairside CAD/CAM Dentistry. Tex Dent. J. 2013, 130, 238–244. [Google Scholar] [PubMed]
- Kattadiyil, M.T.; Jekki, R.; Goodacre, C.J.; Baba, N.Z. Comparison of Treatment Outcomes in Digital and Conventional Complete Removable Dental Prosthesis Fabrications in a Predoctoral Setting. J. Pros. Dent. 2015, 114, 818–825. [Google Scholar] [CrossRef] [PubMed]
- Goodacre, B.J.; Goodacre, C.J.; Baba, N.Z.; Kattadiyil, M.T. Comparison of Denture Base Adaptation between CAD-CAM and Conventional Fabrication Techniques. J. Pros. Dent. 2016, 116, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Janeva, N.M.; Kovacevska, G.; Elencevski, S.; Panchevska, S.; Mijoska, A.; Lazarevska, B. Advantages of CAD/CAM versus Conventional Complete Dentures-A Review. Open Access Maced. J. Med. Sci. 2018, 6, 1498–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cattoni, F.; Teté, G.; Calloni, A.M.; Manazza, F.; Gastaldi, G.; Capparè, P. Milled versus Moulded Mock-Ups Based on the Superimposition of 3D Meshes from Digital Oral Impressions: A Comparative in Vitro Study in the Aesthetic Area. BMC Oral Health 2019, 19, 230. [Google Scholar] [CrossRef]
- Goodacre, B.J.; Goodacre, C.J.; Baba, N.Z.; Kattadiyil, M.T. Comparison of Denture Tooth Movement between CAD-CAM and Conventional Fabrication Techniques. J. Pros. Dent. 2018, 119, 108–115. [Google Scholar] [CrossRef]
- Saponaro, P.C.; Yilmaz, B.; Johnston, W.; Heshmati, R.H.; McGlumphy, E.A. Evaluation of Patient Experience and Satisfaction with CAD-CAM-Fabricated Complete Dentures: A Retrospective Survey Study. J. Pros. Dent. 2016, 116, 524–528. [Google Scholar] [CrossRef]
- PRISMA-P Group; Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Moga, C. Development of a Quality Appraisal Tool for Case Series Studies Using a Modified Delphi Technique: Methodology Paper; Institute of Health Economics: Edmonton, AB, Canada, 2012; ISBN 978-1-926929-04-0. Available online: https://www.semanticscholar.org/paper/Development-of-a-quality-appraisal-tool-for-case-a-Moga-Guo/fd47b9a8e1b91168b3adcb6f3009a59e9078f181 (accessed on 11 April 2021).
- Sinclair, A.; Peprah, K.; Quay, T.; McInnis, M.; Lang, E.; Severn, M.; Mulla, S.; Weeks, L.; Tsoi, B.; Herrington, E.; et al. Optimal Strategies for the Diagnosis of Acute Pulmonary Embolism: A Health Technology Assessment; CADTH Optimal Use Reports; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2018. [Google Scholar]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (Robvis): An R Package and Shiny Web App for Visualizing Risk-of-bias Assessments. Res. Syn. Meth 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Cvar, J.F.; Ryge, G. Reprint of Criteria for the Clinical Evaluation of Dental Restorative Materials. Clin. Oral Investig. 2005, 9, 215–232. [Google Scholar] [CrossRef]
- Wilson, M.A.; Cowan, A.J.; Randall, R.C.; Crisp, R.J.; Wilson, N.H.F. A Practice-Based, Randomized, Controlled Clinical Trial of a New Resin Composite Restorative: One-Year Results. Oper. Dent. 2002, 27, 423–429. [Google Scholar]
- Beuer, F.; Edelhoff, D.; Gernet, W.; Sorensen, J.A. Three-Year Clinical Prospective Evaluation of Zirconia-Based Posterior Fixed Dental Prostheses (FDPs). Clin. Oral Invest. 2009, 13, 445–451. [Google Scholar] [CrossRef]
- Burke, F.J.T.; Crisp, R.J.; Cowan, A.J.; Lamb, J.; Thompson, O.; Tulloch, N. Five-Year Clinical Evaluation of Zirconia-Based Bridges in Patients in UK General Dental Practices. J. Dent. 2013, 41, 992–999. [Google Scholar] [CrossRef]
- Chaar, M.S.; Passia, N.; Kern, M. Ten-Year Clinical Outcome of Three-Unit Posterior FDPs Made from a Glass-Infiltrated Zirconia Reinforced Alumina Ceramic (In-Ceram Zirconia). J. Dent. 2015, 43, 512–517. [Google Scholar] [CrossRef]
- Edelhoff, D.; Florian, B.; Florian, W.; Johnen, C. HIP Zirconia Fixed Partial Dentures--Clinical Results after 3 Years of Clinical Service. Quint. Int. 2008, 39, 459–471. [Google Scholar]
- Ioannidis, A.; Bindl, A. Clinical Prospective Evaluation of Zirconia-Based Three-Unit Posterior Fixed Dental Prostheses: Up-to Ten-Year Results. J. Dent. 2016, 47, 80–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lops, D.; Mosca, D.; Casentini, P.; Ghisolfi, M.; Romeo, E. Prognosis of Zirconia Ceramic Fixed Partial Dentures: A 7-Year Prospective Study. Int. J. Prosthodont. 2012, 25, 21–23. [Google Scholar]
- Naenni, N.; Bindl, A.; Sax, C.; Hämmerle, C.; Sailer, I. A Randomized Controlled Clinical Trial of 3-Unit Posterior Zirconia-Ceramic Fixed Dental Prostheses (FDP) with Layered or Pressed Veneering Ceramics: 3-Year Results. J. Dent. 2015, 43, 1365–1370. [Google Scholar] [CrossRef] [Green Version]
- Perry, R.D.; Kugel, G.; Sharma, S.; Ferreira, S.; Magnuson, B. Two-Year Evaluation Indicates Zirconia Bridges Acceptable Alternative to PFMs. Compend. Contin. Educ. Dent. 2012, 33, e1–e5. [Google Scholar]
- Raigrodski, A.J.; Yu, A.; Chiche, G.J.; Hochstedler, J.L.; Mancl, L.A.; Mohamed, S.E. Clinical Efficacy of Veneered Zirconium Dioxide-Based Posterior Partial Fixed Dental Prostheses: Five-Year Results. J. Prosthet Dent. 2012, 108, 214–222. [Google Scholar] [CrossRef]
- Reich, S.; Endres, L.; Weber, C.; Wiedhahn, K.; Neumann, P.; Schneider, O.; Rafai, N.; Wolfart, S. Three-Unit CAD/CAM-Generated Lithium Disilicate FDPs after a Mean Observation Time of 46 Months. Clin. Oral Invest. 2014, 18, 2171–2178. [Google Scholar] [CrossRef]
- Rinke, S.; Wehle, J.; Schulz, X.; Bürgers, R.; Rödiger, M. Prospective Evaluation of Posterior Fixed Zirconia Dental Prostheses: 10-Year Clinical Results. Int. J. Pros. 2018, 31, 35–42. [Google Scholar] [CrossRef]
- Sailer, I.; Fehér, A.; Filser, F.; Lüthy, H.; Gauckler, L.J.; Schärer, P.; Franz Hämmerle, C.H. Prospective Clinical Study of Zirconia Posterior Fixed Partial Dentures: 3-Year Follow-Up. Quint. Int. 2006, 37, 685–693. [Google Scholar]
- Schmitt, J.; Holst, S.; Wichmann, M.; Reich, S.; Gollner, M.; Hamel, J. Zirconia Posterior Fixed Partial Dentures: A Prospective Clinical 3-Year Follow-Up. Int. J. Prosthod. 2009, 22, 597–603. [Google Scholar]
- Selz, C.F.; Bogler, J.; Vach, K.; Strub, J.R.; Guess, P.C. Veneered Anatomically Designed Zirconia FDPs Resulting from Digital Intraoral Scans: Preliminary Results of a Prospective Clinical Study. J. Dent. 2015, 43, 1428–1435. [Google Scholar] [CrossRef]
- Solá-Ruíz, M.F.; Agustin-Panadero, R.; Fons-Font, A.; Labaig-Rueda, C. A Prospective Evaluation of Zirconia Anterior Partial Fixed Dental Prostheses: Clinical Results after Seven Years. J. Pros. Dent. 2015, 113, 578–584. [Google Scholar] [CrossRef]
- Sorrentino, R.; De Simone, G.; Tetè, S.; Russo, S.; Zarone, F. Five-Year Prospective Clinical Study of Posterior Three-Unit Zirconia-Based Fixed Dental Prostheses. Clin. Oral Invest. 2012, 16, 977–985. [Google Scholar] [CrossRef]
- Teichmann, M.; Wienert, A.L.; Rückbeil, M.; Weber, V.; Wolfart, S.; Edelhoff, D. Ten-Year Survival and Chipping Rates and Clinical Quality Grading of Zirconia-Based Fixed Dental Prostheses. Clin. Oral Investig. 2018, 22, 2905–2915. [Google Scholar] [CrossRef]
- Vult von Steyern, P.; Carlson, P.; Nilner, K. All-Ceramic Fixed Partial Dentures Designed According to the DC-Zirkon Technique. A 2-Year Clinical Study. J. Oral Rehabil. 2005, 32, 180–187. [Google Scholar] [CrossRef]
- Sailer, I.; Makarov, N.A.; Thoma, D.S.; Zwahlen, M.; Pjetursson, B.E. All-Ceramic or Metal-Ceramic Tooth-Supported Fixed Dental Prostheses (FDPs)? A Systematic Review of the Survival and Complication Rates. Part I: Single Crowns (SCs). Dent. Mater. 2015, 31, 603–623. [Google Scholar] [CrossRef] [Green Version]
- Pjetursson, B.E.; Sailer, I.; Makarov, N.A.; Zwahlen, M.; Thoma, D.S. All-Ceramic or Metal-Ceramic Tooth-Supported Fixed Dental Prostheses (FDPs)? A Systematic Review of the Survival and Complication Rates. Part II: Multiple-Unit FDPs. Dent. Mater. 2015, 31, 624–639. [Google Scholar] [CrossRef] [Green Version]
- Rinke, S.; Gersdorff, N.; Lange, K.; Roediger, M. Prospective Evaluation of Zirconia Posterior Fixed Partial Dentures: 7-Year Clinical Results. Int. J. Pros. 2013, 26, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Sailer, I.; Gottnerb, J.; Kanelb, S.; Hammerle, C.H.F. Randomized Controlled Clinical Trial of Zirconia-Ceramic and Metal-Ceramic Posterior Fixed Dental Prostheses: A 3-Year Follow-Up. Int. J. Pros. 2009, 22, 553–560. [Google Scholar]
- Guess, P.C.; Zavanelli, R.A.; Silva, N.R.F.A.; Bonfante, E.A.; Coelho, P.G.; Thompson, V.P. Monolithic CAD/CAM Lithium Disilicate versus Veneered Y-TZP Crowns: Comparison of Failure Modes and Reliability after Fatigue. Int. J. Prosthodont. 2010, 23, 434–442. [Google Scholar]
- Sulaiman, T.A.; Abdulmajeed, A.A.; Delgado, A.; Donovan, T.E. Fracture Rate of 188695 Lithium Disilicate and Zirconia Ceramic Restorations after up to 7.5 Years of Clinical Service: A Dental Laboratory Survey. J. Pros. Dent. 2020, 123, 807–810. [Google Scholar] [CrossRef]
- Belli, R.; Petschelt, A.; Hofner, B.; Hajtó, J.; Scherrer, S.S.; Lohbauer, U. Fracture Rates and Lifetime Estimations of CAD/CAM All-Ceramic Restorations. J. Dent. Res. 2016, 95, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Tinschert, J.; Schulze, K.A.; Natt, G.; Latzke, P.; Heussen, N.; Spiekermann, H. Clinical Behavior of Zirconia-Based Fixed Partial Dentures Made of DC-Zirkon: 3-Year Results. Int. J. Prosthodont. 2008, 21, 217–222. [Google Scholar]
- Gulati, V. Implementation of Micro CT in CAD/CAM Dentistry for Image Processing and Soft Computing: A Review. J. Phys. Conf. Ser. 2020, 1432, 012079. [Google Scholar] [CrossRef]
- Sberna, M.T.; Rizzo, G.; Zacchi, E.; Capparè, P.; Rubinacci, A. A Preliminary Study of the Use of Peripheral Quantitative Computed Tomography for Investigating Root Canal Anatomy. Int. Endod. J. 2009, 42, 66–75. [Google Scholar] [CrossRef]
- Gherlone, E.F.; Capparé, P.; Tecco, S.; Polizzi, E.; Pantaleo, G.; Gastaldi, G.; Grusovin, M.G. A Prospective Longitudinal Study on Implant Prosthetic Rehabilitation in Controlled HIV-Positive Patients with 1-Year Follow-Up: The Role of CD4+ Level, Smoking Habits, and Oral Hygiene. Clin. Implant Dent. Relat. Res. 2016, 18, 955–964. [Google Scholar] [CrossRef]
- Saravi, B.E.; Putz, M.; Patzelt, S.; Alkalak, A.; Uelkuemen, S.; Boeker, M. Marginal Bone Loss around Oral Implants Supporting Fixed versus Removable Prostheses: A Systematic Review. Int. J. Implant Dent. 2020, 6, 20. [Google Scholar] [CrossRef]
- Saravi, B.; Lang, G.; Ülkümen, S.; Burchard, T.; Weihrauch, V.; Patzelt, S.; Boeker, M.; Li, Z.; Woelber, J.P. The Tissue Renin-Angiotensin System (TRAS) and the Impact of Its Inhibition on Inflammation and Bone Loss in the Periodontal Tissue. Eur. Cell Mater. 2020, 40, 203–226. [Google Scholar] [CrossRef]
- Saravi, B.; Vollmer, A.; Lang, G.; Adolphs, N.; Li, Z.; Giers, V.; Stoll, P. Impact of Renin-Angiotensin System Inhibitors and Beta-Blockers on Dental Implant Stability. Int. J. Implant Dent. 2021, 7, 31. [Google Scholar] [CrossRef]
- Tartuk, B.K.; Ayna, E.; Başaran, E. Comparison of The Load-Bearing Capacities of Monolithic PEEK, Zirconia and Hybrid Ceramic Molar Crowns. Meandros Med Dent J. 2018, 20, 45–50. [Google Scholar] [CrossRef]
- Stawarczyk, B.; Beuer, F.; Wimmer, T.; Jahn, D.; Sener, B.; Roos, M.; Schmidlin, P.R. Polyetheretherketone-a Suitable Material for Fixed Dental Prostheses? J. Biomed. Mater. Res. B Appl. Biomater. 2013, 101, 1209–1216. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study and Year of Publication | No. of Patients | No. of FDPs | No. of FDP Units | Region (Percentage) | Mean Age/ Range | CAD/CAM | Cement | Drop-Out (%) |
|---|---|---|---|---|---|---|---|---|
| Beuer et al. 2009 [30] | 19 | 21 | 3 | posterior | 50.9 (27–71) | InLab Sirona | Glass ionomer cement | 0 |
| Burke et al. 2013 [31] | 36 | 41 | 3–4 | anterior (33%)/ posterior (67%) | NR | Lava System | RelyX | 20 |
| Chaar et al. 2015 [32] | 58 | 65 | 3 | posterior | 46.8 | InLab Sirona | Glass ionomer cement | 9.2 |
| Edelhoff et al. 2008 [33] | 18 | 22 | 3–6 | Anterior (19.1%)/ posterior (80.9%) | 19–70 | DigiDent | Glass ionomer cement | 5.6 |
| Ioannidis et al. 2016 [34] | 55 | 59 | 3 | posterior | 52.6 | InLab Sirona | Panavia | 3.6 |
| Lops et al. 2012 [35] | 28 | 28 | NR | anterior/ posterior (NR) | NR | NR | NR | 14.3 |
| Naenni et al. 2015 [36] | 40 | 40 | 3 | posterior | 52.3 | Cerec Sirona/InLab milling unit | Panavia | 10 |
| Perry et al. 2012 [37] | 15 | 16 | 3–4 | NR | NR | Lava System | RelyX | 0 |
| Raigrodski et al. 2012 [38] | 16 | 20 | 3 | posterior | 48 (36–60) | Lava System | RelyX | 6.3 |
| Reich et al. 2014 [39] | 33 | 38 | 3 | anterior/ posterior (NR) | 54.8 (31.2–86.4) | InLab System/MC XL milling unit (Sirona) | Multilink Automix | 3 |
| Rinke et al. 2018 [40] | 75 | 99 | 3–4 | posterior | 49.4 (26–76) | Cercon (DeguDent) | Zinc phosphate cement | 24.2 |
| Sailer et al. 2006 [31] | 45 | 57 | 3–5 | posterior | NR | NR | Variolink/Panavia | 20 |
| Schmitt et al. 2009 [42] | 30 | 30 | 3–4 | posterior | 52.2 (27–75) | NR | Glass ionomer cement | 10 |
| Selz et al. 2015 [43] | 24 | 24 | 3 | Anterior (8.3%)/ posterior (91.7%) | 48.5 (30–65) | iTero System/ 3 + 1 axes milling unit | Multilink Automix | 8.3 |
| Solá-Ruiz et al. 2015 [44] | 27 | 27 | 3–6 | anterior | 30–65 | Lava System | Multilink Automix | 0 |
| Sorrentino et al. 2012 [45] | 37 | 48 | 3 | posterior | 45.3 | Procera System/Procera Center | RelyX | 0 |
| Teichmann et al. 2018 [46] | 17 | 22 | 3–6 | Anterior (15%)/ posterior (85%) | 40.1 | DigiDent | Glass ionomer cement | 9.1 |
| Vult von Steyern et al. 2005 [47] | 18 | 20 | 3–5 | Anterior (25%)/ posterior (75%) | NR | DCS Dentform Software/Precimill machining center | Zinc phosphate cement | 0 |
| Group 1 | ||||||
|---|---|---|---|---|---|---|
| Study and Year of Publication | No. of FDPs after Drop-Outs | Follow-Up in Months (Years) | Type of Material | No. of Failure (Distribution of Failures) | No. of Complications (Distribution of Complications) * | Reported Survival Rate (%) |
| Edelhoff et al. 2008 [33] | 21 | 39.1 (3.3) | Zirconia with veneering ceramics | 0 | 4 (chipping: 3 periapical pathology: 1) | 100 |
| Beuer et al. 2009 [30] | 21 | 40 (3.3) | Zirconia with veneering ceramics | 2 (framework fracture:1 loss of retention: 1 | 1 (endodontic complications: 1) | 90.5 |
| Vult von Steyern et al. 2005 [47] | 20 | 24 (2) | Zirconia with veneering ceramics | 0 | 3 (chipping: 3) | 100 |
| Perry et al. 2012 [37] | 16 | 24 (2) | Zirconia with veneering ceramics | 0 | 3 (chipping: 2) | 100 |
| Selz et al. 2015 [43] | 22 | 18 (1.5) | Zirconia with veneering ceramics | 0 | 19 (chipping: 2 marginal integrity: 2 color match: 1 surface roughness: 14) | 100 |
| Sailer et al. 2006 [41] | 46 | 36 (3) | Zirconia with veneering ceramics | 7 (secondary caries: 3 loss of retention: 1 chipping: 1 endodontic complications: 1 root fracture: 1) | 8 (chipping: 6 secondary caries: 2) | 84.8 |
| Naenni et al. 2015 [36] | 36 | 36 (3) | Zirconia with veneering ceramics | 0 | 30 (chipping: 12 surface roughness: 18) | 100 |
| Schmitt et al. 2009 [42] | 27 | 34.2 (2.9) | Zirconia with veneering ceramics | 0 | 3 (chipping: 3) | 100 |
| Reich et al. 2014 [39] | 32 | 46 (3.8) | Lithium disilicate ceramics | 2 (framework fracture: 1 persistent pain in abutment tooth: 1) | 5 (chipping: 2 endodontic complications: 3) | 93 |
| Group 2 | ||||||
| Study and Year of Publication | No. of FDPs after Drop-Outs | Follow-Up in Months (Years) | Type of Material | No. of Failure (Distribution of Failures) | No. of Complications (Distribution of Complications) * | Reported Survival Rate (%) |
| Lops et al. 2012 [35] | 24 | 78 (6.5) | Zirconia with veneering ceramics | 2 (framework fracture: 1 undefined pain in abutment tooth: 1) | 3 (chipping: 1 loss of retention: 2) | 88.9 |
| Raigrodski et al. 2012 [38] | 19 | 60 (5) | Zirconia with veneering ceramics | 3 (chipping: 2 root fracture: 1) | 4 (chipping: 2 marginal integrity: 1 endodontic complications: 1) | 90 |
| Sorrentino et al. 2012 [45] | 48 | 60 (5) | Zirconia with veneering ceramics | 0 | 16 (chipping: 3 occlusal wear: 6 marginal integrity: 3 anatomical form: 4) | 100 |
| Burke et al. 2013 [31] | 33 | 60 (5) | Zirconia with veneering ceramics | 1 (chipping: 1) | 7 (chipping: 7) | 97 |
| Solá-Ruiz et al. 2015 [44] | 27 | 84 (7) | Zirconia with veneering ceramics | 3 (secondary caries: 2 chipping: 1) | 8 (chipping: 5 loss of retention: 2 periapical pathology: 1) | 88.9 |
| Ioannidis et al. 2016 [34] | 57 | 75.6 (6.3) | Zirconia with veneering ceramics | 3 (root fracture: 2 Secondary caries: 1) | 23 (chipping: 16 loss of vitality: 3 periodontal pathology: 2 secondary caries: 1 endodontic complications: 1) | 85 |
| Group 3 | ||||||
| Study and Year of Publication | No. of FDPs after Drop-Outs | Follow-Up in Months (Years) | Type of Material | No. of Failure (Distribution of Failures) | No. of Complications (Distribution of Complications) * | Reported Survival Rate (%) |
| Rinke et al. 2018 [40] | 75 | 119 (9.9) | Zirconia with veneering ceramics | 24 (framework fracture: 4 chipping: 4 loss of retention: 5 secondary caries: 6 periodontal pathology: 2 root fracture: 2 unknown: 1) | 50 (chipping: 31 framework fracture: 1 loss of retention: 7 secondary caries: 6 loss of vitality: 5) | 75 |
| Teichmann et al. 2018 [46] | 20 | 120 (10) | Zirconia with veneering ceramics | 1 (endodontic complications: 1) | 9 (chipping: 8 periodontal pathology: 1) | 95 |
| Chaar et al. 2015 [32] | 59 | 116.4 (9.7) | Zirconia with veneering ceramics | 4 (framework fracture: 2 secondary caries: 2 | 29 (chipping: 15 loss of retention: 6 endodontic complications: 5 secondary caries: 3) | 93.6 |
| Study and Year of Publication | Total FDP Exposure Time | Total No of Failures | Estimated Failure Rate Per 100 FDP Years (95% CI) | Estimated 3 Year Survival Rate (%) | Estimated 5 Year Survival Rate (%) | Estimated 10 Year Survival Rate (%) | Total No. of Complications * | Estimated Complication Rate (Per 100 FDP Years) | Estimated 3 Year Success Rate | Estimated 5 Year Success Rate | Estimated 10 Year Success Rate |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Edelhoff et al. 2008 [33] | 66.46 | 0 | - | 100.00 | 100.00 | 100.00 | 4 | 6.02 (2.259–16.037) | 81.94 | 69.91 | 81.94 |
| Beuer et al. 2009 [30] | 68.99 | 2 | 2.89 (0.725–11.589) | 91.30 | 85.51 | 71.01 | 1 | 1.45 (0.204–10.289) | 95.65 | 92.75 | 95.65 |
| Vult Von Steyern et al. 2005 [47] | 40.00 | 0 | - | 100.00 | 100.00 | 100.00 | 3 | 7.50 (2.419–23.254) | 77.50 | 62.50 | 77.50 |
| Perry et al. 2012 [37] | 32.00 | 0 | - | 100.00 | 100.00 | 100.00 | 2 | 6.25 (1.563–24.990) | 81.25 | 68.75 | 81.25 |
| Selz et al. 2015 [43] | 36.00 | 0 | - | 100.00 | 100.00 | 100.00 | 19 | 13.89 (5.781–33.368) | 58.33 | 30.56 | 58.33 |
| Sailer et al. 2006 [31] | 138.60 | 7 | 5.05 (2.408–10.594) | 84.85 | 74.75 | 49.49 | 8 | 5.77 (2.887–11.542) | 82.68 | 71.14 | 82.68 |
| Naenni et al. 2015 [36] | 116.00 | 0 | - | 100.00 | 100.00 | 100.00 | 30 | 10.34 (5.875–18.216) | 68.97 | 48.28 | 68.97 |
| Schmitt et al. 2009 [42] | 77.00 | 0 | - | 100.00 | 100.00 | 100.00 | 3 | 3.90 (1.257–12.080) | 88.31 | 80.52 | 88.31 |
| Reich et al. 2014 [39] § | 138.87 | 2 | 1.44 (0.36–5.759) | 95.68 | 92.80 | 85.60 | 5 | 3.60 (1.499–8.650) | 89.20 | 82.00 | 89.20 |
| Total | 713.91 | 11 | 75 | ||||||||
| Summary Estimate (95% Ci) # | 1.78 (1.435–2.216) | 94.66 | 91.10 | 82.20 | 1.24 (0.932–1.661) | 96.27 | 93.78 | 87.56 | |||
| Study and Year of Publication | Total FDP Exposure Time | Total No of Failures | Estimated Failure Rate Per 100 FDP Years (95% CI) | Estimated 3 Year Survival Rate | Estimated 5 Year Survival Rate | Estimated 10 Year Survival Rate | Total No. of Complications | Estimated Complication Rate (Per 100 FDP Years) | Estimated 3 Year Success Rate | Estimated 5 Year Success Rate | Estimated 10 Year Success Rate |
| Lops et al. 2012 [35] | 156.00 | 2 | 1.28 (0.321–5.126) | 96.15 | 93.59 | 87.18 | 3 | 1.92 (0.620–5.963) | 94.23 | 90.38 | 94.23 |
| Raigrodski et al. 2012 [38] | 94.00 | 3 | 3.19 (1.029–9.895) | 90.43 | 84.04 | 68.09 | 4 | 4.26 (1.597–11.338) | 87.23 | 78.72 | 87.23 |
| Sorrentino et al. 2012 [45] | 240.00 | 0 | - | 100.00 | 100.00 | 100.00 | 16 | 6.67 (4.084–10.882) | 80.00 | 66.67 | 80.00 |
| Burke et al. 2013 | 176.00 | 1 | 0.57 (0.08–4.034) | 98.30 | 97.16 | 94.32 | 7 | 3.98 (1.896–8.343) | 88.07 | 80.11 | 88.07 |
| Solá-Ruiz et al. 2015 [44] | 177.00 | 3 | 1.69 (0.547–5.255) | 94.92 | 91.53 | 83.05 | 8 | 4.52 (2.260–9.038) | 86.44 | 77.40 | 86.44 |
| Ioannidis et al. 2016 [34] | 365.10 | 3 | 0.82 (0.265–2.548) | 97.53 | 95.89 | 91.78 | 23 | 6.30 (4.186–9.480) | 81.10 | 68.50 | 81.10 |
| Total | 1208.10 | 12 | 61 | ||||||||
| Summary Estimate (95% Ci) # | 2.07 (1.555–2.746) | 93.80 | 89.67 | 79.33 | 1.08 (0.759–1.523) | 96.77 | 94.62 | 89.25 | |||
| Study and Year of Publication | Total FDP Exposure time | Total No of Failures | Estimated Failure Rate Per 100 FDP Years (95% CI) | Estimated 3 Year Survival Rate | Estimated 5 Year Survival Rate | Estimated 10 Year Survival Rate | Total No. of Complications | Estimated Complication Rate (Per 100 FDP Years) | Estimated 3 Year Success Rate | Estimated 5 Year Success Rate | Estimated 10 Year Success Rate |
| Rinke et al. 2018 [40] | 695.27 | 24 | 3.45 (2.314–5.15) | 89.64 | 82.74 | 65.48 | 50 | 7.19 (5.451–9.488) | 78.43 | 64.04 | 78.43 |
| Teichmann et al. 2018 [46] | 213.50 | 1 | 0.47 (0.066–3.325) | 98.59 | 97.66 | 95.32 | 9 | 4.22 (2.193–8.102) | 87.35 | 78.92 | 87.35 |
| Chaar et al. 2015 [32] | 561.88 | 4 | 0.72 (0.267–1.897) | 97.86 | 96.44 | 92.88 | 29 | 5.16 (3.587–7.427) | 84.52 | 74.19 | 84.52 |
| Total | 1470.65 | 29 | 88 | ||||||||
| Summary Estimate (95% Ci) # | 1.82 (1.716–1.935) | 94.53 | 90.89 | 81.78 | 1.82 (1.479–2.244) | 94.53 | 90.89 | 81.78 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saravi, B.; Vollmer, A.; Hartmann, M.; Lang, G.; Kohal, R.-J.; Boeker, M.; Patzelt, S.B.M. Clinical Performance of CAD/CAM All-Ceramic Tooth-Supported Fixed Dental Prostheses: A Systematic Review and Meta-Analysis. Materials 2021, 14, 2672. https://doi.org/10.3390/ma14102672
Saravi B, Vollmer A, Hartmann M, Lang G, Kohal R-J, Boeker M, Patzelt SBM. Clinical Performance of CAD/CAM All-Ceramic Tooth-Supported Fixed Dental Prostheses: A Systematic Review and Meta-Analysis. Materials. 2021; 14(10):2672. https://doi.org/10.3390/ma14102672
Chicago/Turabian StyleSaravi, Babak, Andreas Vollmer, Maja Hartmann, Gernot Lang, Ralf-Joachim Kohal, Martin Boeker, and Sebastian B. M. Patzelt. 2021. "Clinical Performance of CAD/CAM All-Ceramic Tooth-Supported Fixed Dental Prostheses: A Systematic Review and Meta-Analysis" Materials 14, no. 10: 2672. https://doi.org/10.3390/ma14102672