Effect of Tooth Types on the Accuracy of Dental 3D Scanners: An In Vitro Study



Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Medina-Sotomayor, P.; Pascual-Moscardo, A.; Camps, I. Accuracy of 4 digital scanning systems on prepared teeth digitally isolated from a complete dental arch. J. Prosthet. Dent. 2019, 121, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Michelinakis, G.; Apostolakis, D.; Tsagarakis, A.; Kourakis, G.; Pavlakis, E. A comparison of accuracy of 3 intraoral scanners: A single-blinded in vitro study. J. Prosthet. Dent. 2019. [Google Scholar] [CrossRef] [PubMed]
- Nedelcu, R.; Olsson, P.; Nyström, I.; Thor, A. Finish line distinctness and accuracy in 7 intraoral scanners versus conventional impression: An in vitro descriptive comparison. BMC Oral Health 2018, 18, 27. [Google Scholar] [CrossRef] [PubMed]
- Nedelcu, R.G.; Persson, A.S. Scanning accuracy and precision in 4 intraoral scanners: An in vitro comparison based on 3-dimensional analysis. J. Prosthet. Dent. 2014, 112, 1461–1471. [Google Scholar] [CrossRef]
- Park, G.-H.; Son, K.; Lee, K.-b. Feasibility of using an intraoral scanner for a complete-arch digital scan. J. Prosthet. Dent. 2019, 121, 803–810. [Google Scholar] [CrossRef]
- Abdel-Azim, T.; Rogers, K.; Elathamna, E.; Zandinejad, A.; Metz, M.; Morton, D. Comparison of the marginal fit of lithium disilicate crowns fabricated with CAD/CAM technology by using conventional impressions and two intraoral digital scanners. J. Prosthet. Dent. 2015, 114, 554–559. [Google Scholar] [CrossRef]
- Arezoobakhsh, A.; Shayegh, S.S.; Ghomi, A.J.; Hakimaneh, S.M.R. Comparison of marginal and internal fit of 3-unit zirconia frameworks fabricated with CAD-CAM technology using direct and indirect digital scans. J. Prosthet. Dent. 2020, 123, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Braian, M.; Wennerberg, A. Trueness and precision of 5 intraoral scanners for scanning edentulous and dentate complete-arch mandibular casts: A comparative in vitro study. J. Prosthet. Dent. 2019, 122, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-H. Fabricating a crown under an existing removable partial denture with impression scanning and CAD-CAM technology. J. Prosthet. Dent. 2019. [Google Scholar] [CrossRef]
- Wulfman, C.; Naveau, A.; Rignon-Bret, C. Digital scanning for complete-arch implant-supported restorations: A systematic review. J. Prosthet. Dent. 2019. [Google Scholar] [CrossRef]
- Fukazawa, S.; Odaira, C.; Kondo, H. Investigation of accuracy and reproducibility of abutment position by intraoral scanners. J. Prosthodont. Res. 2017, 61, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Latham, J.; Ludlow, M.; Mennito, A.; Kelly, A.; Evans, Z.; Renne, W. Effect of scan pattern on complete-arch scans with 4 digital scanners. J. Prosthet. Dent. 2020, 123, 89–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isola, G.; Perillo, L.; Migliorati, M.; Matarese, M.; Dalessandri, D.; Grassia, V.; Alibrandi, A.; Matarese, G. The impact of temporomandibular joint arthritis on functional disability and global health in patients with juvenile idiopathic arthritis. Eur. J. Orthod. 2019, 41, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, R.; Muraglie, S.; Lo Giudice, A.; Aboulazm, K.S.; Nucera, R. Evaluation of mandibular symmetry and morphology in adult patients with unilateral posterior crossbite: A CBCT study using a surface-to-surface matching technique. Eur. J. Orthod. 2020, 29, 106. [Google Scholar] [CrossRef] [PubMed]
- Son, K.; Lee, S.; Kang, S.H.; Park, J.; Lee, K.-b.; Jeon, M.; Yun, B.J. A Comparison Study of Marginal and Internal Fit Assessment Methods for Fixed Dental Prostheses. J. Clin. Med. 2019, 8, 785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cappare, P.; Sannino, G.; Minoli, M.; Montemezzi, P.; Ferrini, F. Conventional versus digital impressions for full arch screw-retained maxillary rehabilitations: A randomized clinical trial. Int. J. Environ. Res. Public Health 2019, 16, 829. [Google Scholar] [CrossRef] [Green Version]
- Ferrini, F.; Capparé, P.; Vinci, R.; Gherlone, E.F.; Sannino, G. Digital versus traditional workflow for posterior maxillary rehabilitations supported by one straight and one tilted implant: A 3-year prospective comparative study. Biomed. Res. Int. 2018, 2018, 4149107. [Google Scholar] [CrossRef]
- Gherlone, E.; Mandelli, F.; Capparè, P.; Pantaleo, G.; Traini, T.; Ferrini, F. A 3 years retrospective study of survival for zirconia-based single crowns fabricated from intraoral digital impressions. J. Dent. 2014, 42, 1151–1155. [Google Scholar] [CrossRef]
- Ender, A.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J. Prosthet. Dent. 2016, 115, 313–320. [Google Scholar] [CrossRef] [Green Version]
- Jeong, I.-D.; Lee, J.-J.; Jeon, J.-H.; Kim, J.-H.; Kim, H.-Y.; Kim, W.-C. Accuracy of complete-arch model using an intraoral video scanner: An in vitro study. J. Prosthet. Dent. 2016, 115, 755–759. [Google Scholar] [CrossRef]
- Lim, J.-H.; Park, J.-M.; Kim, M.; Heo, S.-J.; Myung, J.-Y. Comparison of digital intraoral scanner reproducibility and image trueness considering repetitive experience. J. Prosthet. Dent. 2018, 119, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.; Ender, A.; Joda, T.; Katsoulis, J. Impact of digital intraoral scan strategies on the impression accuracy using the TRIOS Pod scanner. Quintessence Int. 2016, 47, 343–349. [Google Scholar] [PubMed]
- Son, K.; Huang, M.-Y.; Lee, K.-b. A method to evaluate the accuracy of dental implant placement without postoperative radiography after computer-guided implant surgery: A dental technique. J. Prosthet. Dent. 2019. [Google Scholar] [CrossRef] [PubMed]
- Cattoni, F.; Teté, G.; Calloni, A.M.; Manazza, F.; Gastaldi, G.; Capparè, P. Milled versus moulded mock-ups based on the superimposition of 3D meshes from digital oral impressions: A comparative in vitro study in the aesthetic area. BMC Oral Health 2019, 19, 230. [Google Scholar] [CrossRef]
- Yeung, M.; Abdulmajeed, A.; Carrico, C.K.; Deeb, G.R.; Bencharit, S. Accuracy and precision of 3D-printed implant surgical guides with different implant systems: An in vitro study. J. Prosthet. Dent. 2019. [Google Scholar] [CrossRef]
- Koulivand, S.; Ghodsi, S.; Siadat, H.; Alikhasi, M. A clinical comparison of digital and conventional impression techniques regarding finish line locations and impression time. J. Esthet. Restor. Dent. 2020, 32, 236–243. [Google Scholar] [CrossRef]
- Revilla-León, M.; Jiang, P.; Sadeghpour, M.; Piedra-Cascón, W.; Zandinejad, A.; Özcan, M.; Krishnamurthy, V.R. Intraoral digital scans-Part 1: Influence of ambient scanning light conditions on the accuracy (trueness and precision) of different intraoral scanners. J. Prosthet. Dent. 2019. [Google Scholar] [CrossRef]
- Lee, H.; Kim, H.-S.; Noh, K.; Paek, J.; Pae, A. A simplified method for evaluating the 3-dimensional cement space of dental prostheses by using a digital scanner. J. Prosthet. Dent. 2017, 118, 584–586. [Google Scholar] [CrossRef]
- Marghalani, A.; Weber, H.-P.; Finkelman, M.; Kudara, Y.; El Rafie, K.; Papaspyridakos, P. Digital versus conventional implant impressions for partially edentulous arches: An evaluation of accuracy. J. Prosthet. Dent. 2018, 119, 574–579. [Google Scholar] [CrossRef]
- Pathak, V.K.; Singh, A.K. Investigating Alignment Effect on Inspection Accuracy of AM Part Using 3D Scanner. J. Adv. Manuf. Syst. 2017, 16, 157–169. [Google Scholar] [CrossRef]
- Uhm, S.-H.; Kim, J.-H.; Jiang, H.B.; Woo, C.-W.; Chang, M.; Kim, K.-N.; Bae, J.-M.; Oh, S. Evaluation of the accuracy and precision of four intraoral scanners with 70% reduced inlay and four-unit bridge models of international standard. Dent. Mater. J. 2017, 36, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flügge, T.V.; Schlager, S.; Nelson, K.; Nahles, S.; Metzger, M.C. Precision of intraoral digital dental impressions with iTero and extraoral digitization with the iTero and a model scanner. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Son, K.; Lee, W.S.; Lee, K.-b. Displacement of Customized Abutments Designed on a Working Cast and in the Oral Cavity: A Comparative In Vivo Study. J. Prosthodont. 2020, 29, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Jiang, P.; Sadeghpour, M.; Piedra-Cascón, W.; Zandinejad, A.; Özcan, M.; Krishnamurthy, V.R. Intraoral digital scans: Part 2-influence of ambient scanning light conditions on the mesh quality of different intraoral scanners. J. Prosthet. Dent. 2019. [Google Scholar] [CrossRef]
- Lee, J.-J.; Jeong, I.-D.; Park, J.-Y.; Jeon, J.-H.; Kim, J.-H.; Kim, W.-C. Accuracy of single-abutment digital cast obtained using intraoral and cast scanners. J. Prosthet. Dent. 2017, 117, 253–259. [Google Scholar] [CrossRef]
- May, L.G.; Kelly, J.R.; Bottino, M.A.; Hill, T. Influence of the resin cement thickness on the fatigue failure loads of CAD/CAM feldspathic crowns. Dent. Mater. 2015, 31, 895–900. [Google Scholar] [CrossRef] [Green Version]
- Anh, J.-W.; Park, J.-M.; Chun, Y.-S.; Kim, M.; Kim, M. A comparison of the precision of three-dimensional images acquired by 2 digital intraoral scanners: Effects of tooth irregularity and scanning direction. Korean J. Orthod. 2016, 46, 3–12. [Google Scholar] [CrossRef] [Green Version]
- ALShami, A.; ALHarthi, S.; Binshabaib, M.; Wahi, M. Tooth Morphology Overview. In Basics of Dental Morphology and Anatomy; IntechOpen: London, UK, 2019. [Google Scholar] [CrossRef] [Green Version]
- International Organization for Standardization. ISO 12836:2015. Dentistry—Digitizing Devices for CAD/CAM Systems for Indirect Dental Restorations-Test Methods for Assessing Accuracy; International Organization for Standardization: Geneva, Switzerland, 2015; Available online: https://www.iso.org/standard/68414.html (accessed on 8 April 2020).
- Son, K.; Lee, K.-b. Prediction of learning curves of 2 dental CAD software programs, part 2: Differences in learning effects by type of dental personnel. J. Prosthet. Dent. 2019. [Google Scholar] [CrossRef]
- Son, K.; Lee, W.S.; Lee, K.-b. Prediction of the learning curves of 2 dental CAD software programs. J. Prosthet. Dent. 2019, 121, 95–100. [Google Scholar] [CrossRef]
- Son, K.; Yu, B.-y.; Yoon, T.H.; Lee, K.-b. Comparative Study of the Trueness of the Inner Surface of Crowns Fabricated from Three Types of Lithium Disilicate Blocks. Appl. Sci. 2019, 9, 1798. [Google Scholar] [CrossRef] [Green Version]
- Ferrini, F.; Sannino, G.; Chiola, C.; Capparé, P.; Gastaldi, G.; Gherlone, E.F. Influence of Intra-Oral Scanner (IOS) on The Marginal Accuracy of CAD/CAM Single Crowns. Int. J. Environ. Res. Public Health 2019, 16, 544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gherlone, E.; Capparé, P.; Vinci, R.; Ferrini, F.; Gastaldi, G.; Crespi, R. Conventional Versus Digital Impressions for “All-on-Four” Restorations. Int. J. Oral Maxillofac. Implants 2016, 31, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Mandelli, F.; Gherlone, E.; Gastaldi, G.; Ferrari, M. Evaluation of the accuracy of extraoral laboratory scanners with a single-tooth abutment model: A 3D analysis. J. Prosthodont. Res. 2017, 61, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Son, K.; Lee, K.-b. Effects of Trueness and Surface Microhardness on the Fitness of Ceramic Crowns. Appl. Sci. 2020, 10, 1858. [Google Scholar] [CrossRef] [Green Version]
- Kang, B.H.; Son, K.; Lee, K.-b. Accuracy of Five Intraoral Scanners and Two Laboratory Scanners for a Complete Arch: A Comparative In Vitro Study. Appl. Sci. 2020, 10, 74. [Google Scholar] [CrossRef] [Green Version]
- Park, J.M.; Kim, R.J.Y.; Lee, K.W. Comparative reproducibility analysis of 6 intraoral scanners used on complex intracoronal preparations. J. Prosthet. Dent. 2020, 123, 113–120. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Displacement Type | Desktop Scanner | Intraoral Scanner | P | |||||
|---|---|---|---|---|---|---|---|---|
| 3Shape E1 | DOF | CS3500 | CS3600 | Trios2 | Trios3 | i500 | ||
| RMS (Mean ± SD, μm) | ||||||||
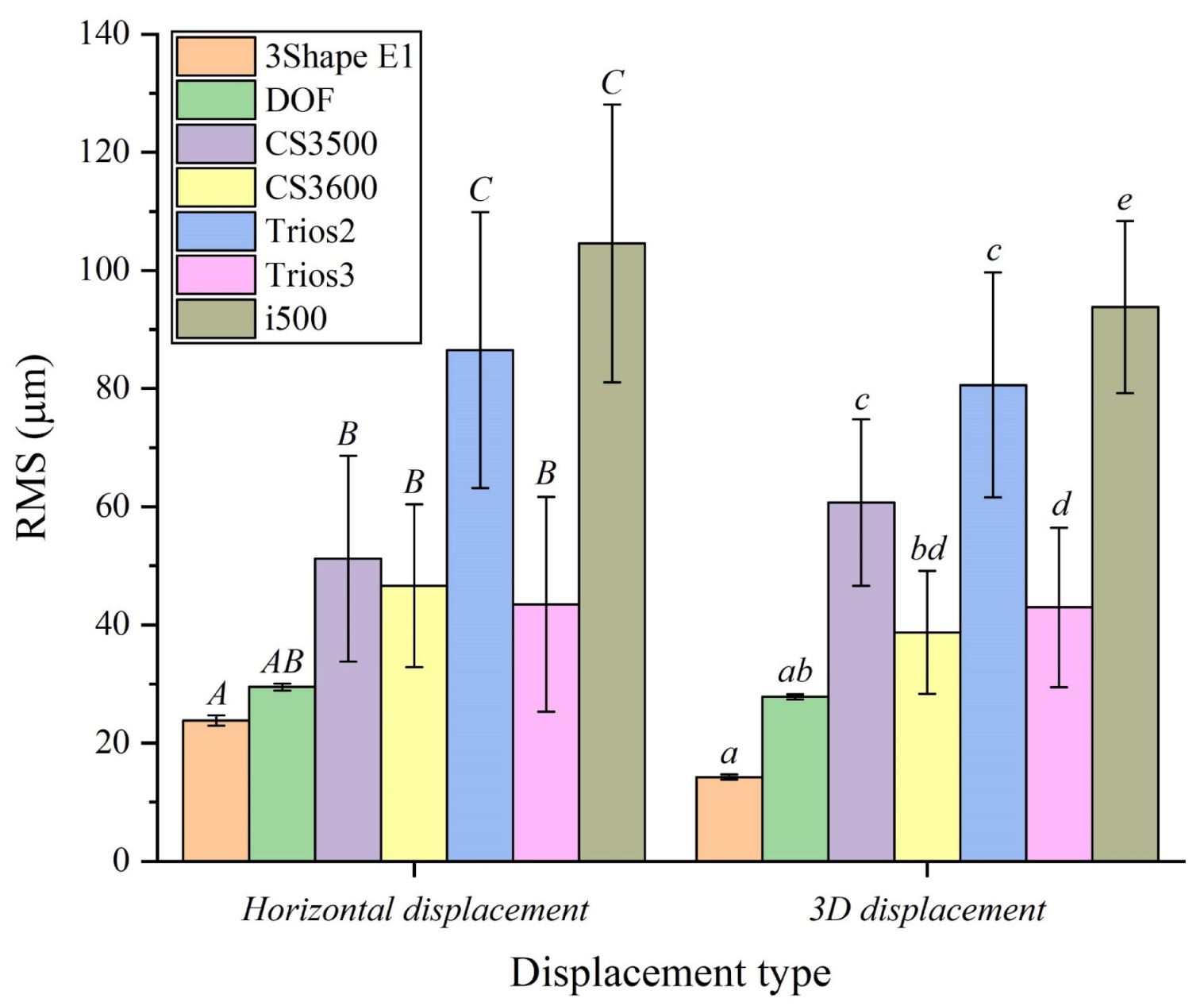
| Horizontal displacement | 23.8 ± 0.8A | 29.4 ± 0.5AB | 51.2 ± 17.4B | 46.6 ± 13.7B | 86.5 ± 23.3C | 43.4 ± 18.1B | 104.6 ± 23.5C | <0.001 * |
| 3D displacement | 14.2 ± 0.4A | 27.8 ± 0.4AB | 60.7 ± 14C | 38.7 ± 10.3BD | 80.6 ± 19C | 42.9 ± 13.4D | 93.8 ± 14.5E | <0.001 * |
| Tooth Type | Desktop Scanner | Intraoral Scanner | P | |||||
|---|---|---|---|---|---|---|---|---|
| 3Shape E1 | DOF | CS3500 | CS3600 | Trios2 | Trios3 | i500 | ||
| RMS (Mean ± SD, μm) | ||||||||
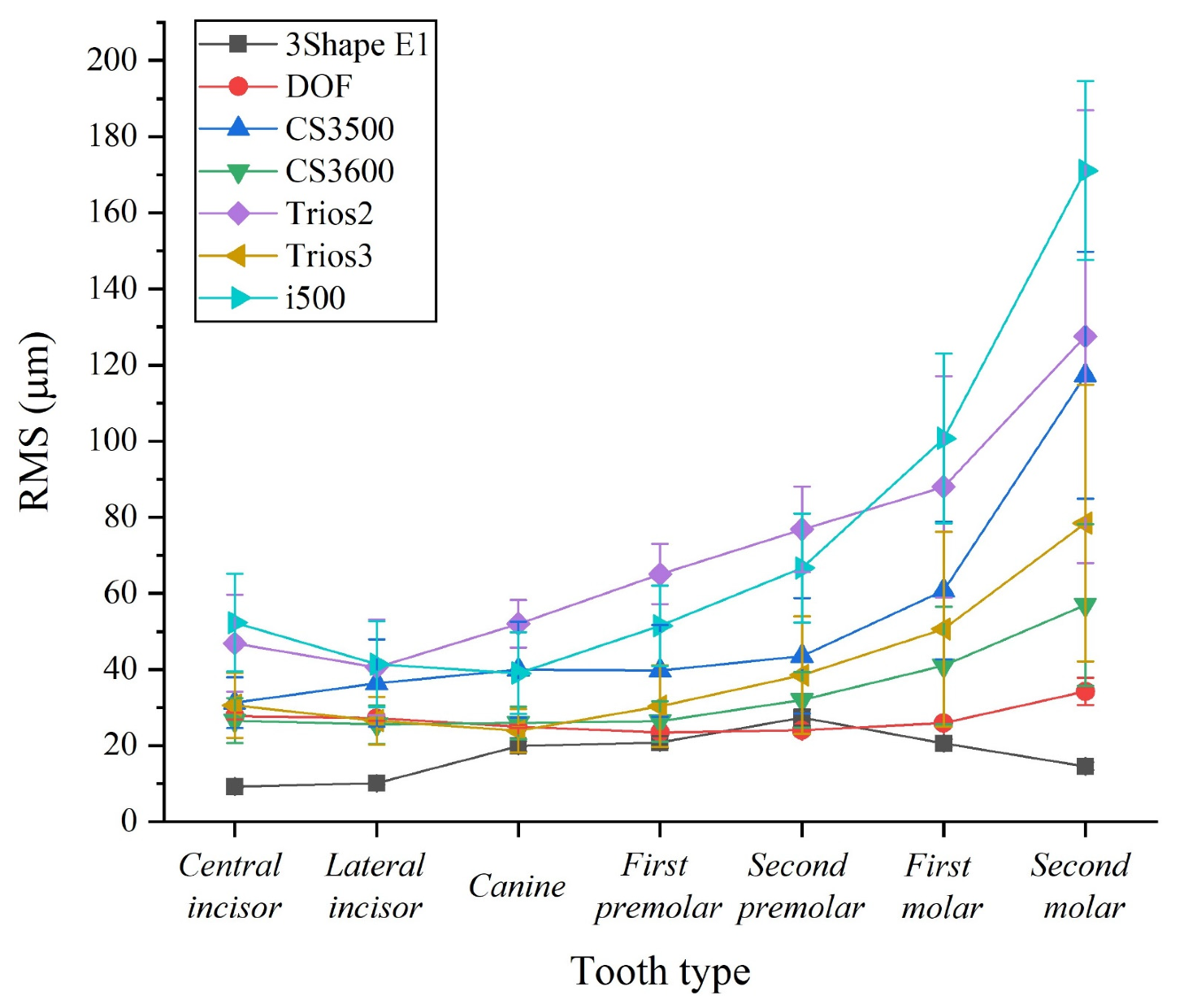
| Central incisor | 9.1 ± 0.3Aa | 27.7 ± 0.8Ba | 31.2 ± 6.6Ba | 26.5 ± 5.9Ba | 46.9 ± 12.7Ca | 30.6 ± 8.5Ba | 52.2 ± 12.8Cab | <0.001 * |
| Lateral incisor | 10.1 ± 0.4Aa | 27.2 ± 0.6Bab | 36.4 ± 11.5Ca | 25.5 ± 5Ba | 40.5 ± 12.6Ca | 26.5 ± 6.3Ba | 41.3 ± 11.3Ca | <0.001 * |
| Canine | 19.8 ± 1.3Ab | 25 ± 0.3Acd | 39.9 ± 12.6Ba | 25.9 ± 4.2Aa | 51.9 ± 6.2Cab | 23.8 ± 5.6Aa | 39 ± 10.7Ba | <0.001 * |
| First premolar | 20.8 ± 1.6Ab | 23.5 ± 0.3ABd | 39.7 ± 12Ca | 26.3 ± 5.2ABa | 65 ± 7.9Eabc | 30.3 ± 10.7Ba | 51.4 ± 10.5Dab | <0.001 * |
| Second premolar | 27.3 ± 2.1ABc | 23.9 ± 0.3Ad | 43.5 ± 15.1Ca | 32 ± 7.3ABCab | 76.8 ± 11.2Dbc | 38.5 ± 15.4BCab | 66.6 ± 14.3Db | <0.001 * |
| First molar | 20.6 ± 1Ab | 25.9 ± 0.4Abc | 60.7 ± 18Bb | 41 ± 15.4ABb | 88 ± 29Cc | 50.6 ± 25.6Bb | 100.7 ± 22.2Cc | <0.001 * |
| Second molar | 14.5 ± 1Ad | 34.2 ± 3.5ABe | 117.3 ± 32.3Dc | 56.9 ± 21.2BCc | 127.5 ± 59.4Dd | 78.4 ± 36.3Cc | 171 ± 23.4Ed | <0.001 * |
| P | <0.001 * | < 0.001 * | <0.001 * | < 0.001 * | <0.001 * | < 0.001 * | <0.001 * | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Son, K.; Lee, K.-b. Effect of Tooth Types on the Accuracy of Dental 3D Scanners: An In Vitro Study. Materials 2020, 13, 1744. https://doi.org/10.3390/ma13071744
Son K, Lee K-b. Effect of Tooth Types on the Accuracy of Dental 3D Scanners: An In Vitro Study. Materials. 2020; 13(7):1744. https://doi.org/10.3390/ma13071744
Chicago/Turabian StyleSon, Keunbada, and Kyu-bok Lee. 2020. "Effect of Tooth Types on the Accuracy of Dental 3D Scanners: An In Vitro Study" Materials 13, no. 7: 1744. https://doi.org/10.3390/ma13071744