Particulate Production and Composite Dust during Routine Dental Procedures. A Systematic Review with Meta-Analyses


Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol, Registration and Reporting
2.2. Eligibility Criteria
2.3. Search Strategy and Study Selection
2.4. Data Collection
2.5. Risk of Bias in Individual Studies
2.6. Summary Measures and Data Synthesis
2.7. Risk of Bias Across Studies
3. Results
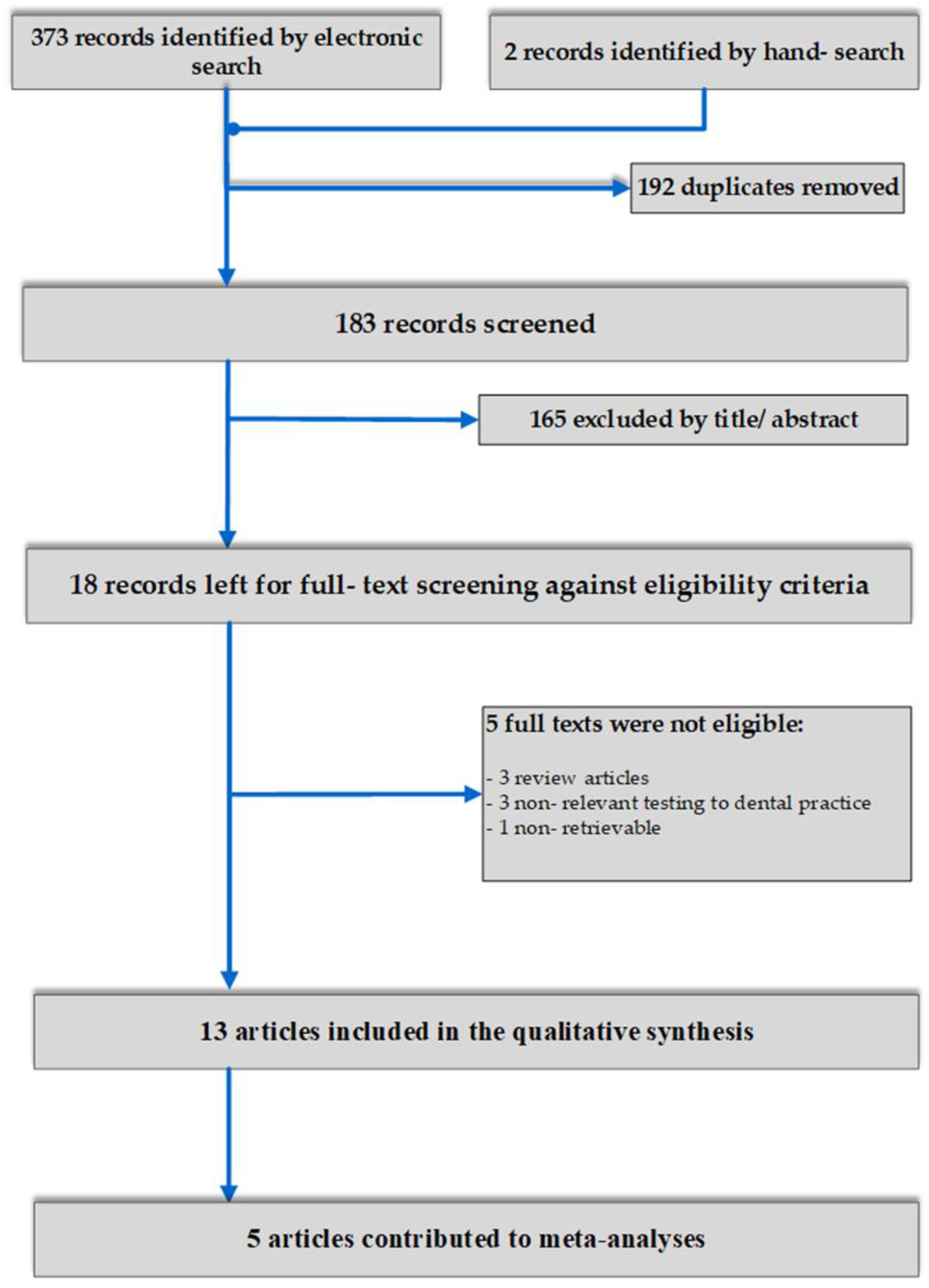
3.1. Search Details
3.2. Study Design and Characteristics
3.3. Risk of Bias within Studies
3.4. Effects of Interventions, Meta-Analyses, Additional Analyses
3.5. Risk of Bias across Studies
4. Discussion
4.1. Findings in Context
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Electronic Database | Hits |
|---|---|---|
| 1. | Medline via Pubmed | |
| composite AND dust AND dent * | 51 | |
| ((composite) OR (adhesive) OR (resin) OR (filler)) AND ((polishing) OR (grinding) OR (rotary instruments) OR (high speed handpiece) OR (slow speed handpiece) OR (high speed air turbine)) AND ((dental) OR (dentistry) OR (dent*)) AND ((aerosol) OR (suspended particle) OR (dust) OR (nano-dust) OR (nanodust) OR (airborne particle) OR (nanoparticle)) | 141 | |
| (composite OR resin) AND (dust OR particl*) AND (orthodontic debond*) | 27 | |
| 2. | Scopus | |
| composite AND dust AND dent * | 26 | |
| ((composite) OR (adhesive) OR (resin) OR (filler)) AND ((polishing) OR (grinding) OR (rotary instruments) OR (high speed handpiece) OR (slow speed handpiece) OR (high speed air turbine)) AND ((dental) OR (dentistry) OR (dent*)) AND ((aerosol) OR (suspended particle) OR (dust) OR (nano-dust) OR (nanodust) OR (airborne particle) OR (nanoparticle)) | 84 | |
| (composite OR resin) AND (dust OR particl*) AND (orthodontic debond*) | 23 | |
| 3. | Cochrane Central Register of Controlled Trials (CENTRAL) | |
| composite AND dust AND dent* | 2 | |
| ((composite) OR (adhesive) OR (resin) OR (filler)) AND ((polishing) OR (grinding) OR (rotary instruments) OR (high speed handpiece) OR (slow speed handpiece) OR (high speed air turbine)) AND ((dental) OR (dentistry) OR (dent*)) AND ((aerosol) OR (suspended particle) OR (dust) OR (nano-dust) OR (nanodust) OR (airborne particle) OR (nanoparticle)) | 8 | |
| (composite OR resin) AND (dust OR particl*) AND (orthodontic debond*) | 6 | |
| 4. | Cochrane Database of Systematic Reviews (CDSR) | |
| composite AND dust AND dent* | 0 | |
| ((composite) OR (adhesive) OR (resin) OR (filler)) AND ((polishing) OR (grinding) OR (rotary instruments) OR (high speed handpiece) OR (slow speed handpiece) OR (high speed air turbine)) AND ((dental) OR (dentistry) OR (dent*)) AND ((aerosol) OR (suspended particle) OR (dust) OR (nano-dust) OR (nanodust) OR (airborne particle) OR (nanoparticle)) | 0 | |
| (composite OR resin) AND (dust OR particl*) AND (orthodontic debond*) | 0 | |
| 5. | Open Grey | |
| composite AND dust | 4 | |
| 6. | ClinicalTrials.gov (www.clinicaltrials.gov) | |
| composite AND dust | 0 | |
| 7. | National Research Register (ISRCTN: www.controlled-trials.com) | |
| composite AND dust | 1 |
References
- Van Landuyt, K.L.; Yoshihara, K.; Geebelen, B.; Peumans, M.; Godderis, L.; Hoet, P.H.; Van Meerbeek, B. Should we be concerned about composite (nano-)dust? Dent. Mater. 2012, 28, 1162–1170. [Google Scholar] [CrossRef] [PubMed]
- Villarroel, M.; Fahl, N.; De Sousa, A.M.; De Oliveira, O.B. Direct Esthetic Restorations Based on Translucency and Opacity of Composite Resins. J. Esthet. Restor. Dent. 2011, 23, 73–87. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-H. Update on Dental Nanocomposites. J. Dent. Res. 2010, 89, 549–560. [Google Scholar] [CrossRef] [PubMed]
- Anusavice, K.J.; Shen, C.; Rawls, R. Phillips’ Science of Dental Materials, 12th ed.; Elsevier: St Louis, MO, USA, 2013. [Google Scholar]
- Ilie, N.; Hickel, R. Investigations on mechanical behaviour of dental composites. Clin. Oral Investig. 2009, 13, 427–438. [Google Scholar] [CrossRef] [PubMed]
- Meyer, G.; Ernst, C.; Willershausen, B. Determination of polymerization stress of conventional and new “clustered” microfill-composites in comparison with hybrid composites. J. Dent. Res. 2003, 81, 921–935. [Google Scholar]
- Leggat, P.A.; Kedjarune, U.; Smith, D. Occupational Health Problems in Modern Dentistry: A Review. Ind. Health 2007, 45, 611–621. [Google Scholar] [CrossRef] [Green Version]
- Klaassen, C. Casarett and Doul’s Toxicology: the Basic Science of Poisons, 7th ed.; The MacGrew Hill Company: Chicago, IL, USA; San Fransisco, CA, USA, 2008. [Google Scholar]
- Delfino, R.J.; Sioutas, C.; Malik, S. Potential Role of Ultrafine Particles in Associations between Airborne Particle Mass and Cardiovascular Health. Environ. Health Perspect. 2005, 113, 934–946. [Google Scholar] [CrossRef] [Green Version]
- Choudat, D.; Triem, S.; Weill, B.; Vicrey, C.; Ameille, J.; Brochard, P.; Letourneux, M.; Rossignol, C. Respiratory symptoms, lung function, and pneumoconiosis among self employed dental technicians. Occup. Environ. Med. 1993, 50, 443–449. [Google Scholar] [CrossRef] [Green Version]
- Iliadi, A.; Koletsi, D.; Eliades, T.; Eliades, G. Particulate Production and Composite Dust during Routine Dental Procedures. A Systematic Review Protocol. 2020. Available online: https://osf.io/st9mx/ (accessed on 29 April 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koletsi, D.; Pandis, N.; Polychronopoulou, A.; Eliades, T. What’s in a title? An assessment of whether randomized controlled trial in a title means that it is one. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 679–685. [Google Scholar] [CrossRef]
- Koletsi, D.; Pandis, N.; Polychronopoulou, A.; Eliades, T. Mislabeling Controlled Clinical Trials (CCTs) as “Randomized Clinical Trials (RCTs)” in Dental Specialty Journals. J. Évid. Based Dent. Pr. 2012, 12, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Koletsi, D.; Spineli, L.M.; Lempesi, E.; Pandis, N. Risk of bias and magnitude of effect in orthodontic randomized controlled trials: a meta-epidemiological review. Eur. J. Orthod. 2015, 38, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Fleming, P.S.; Koletsi, D.; Dwan, K.; Pandis, N. Outcome Discrepancies and Selective Reporting: Impacting the Leading Journals? PLoS ONE 2015, 10, e0127495. [Google Scholar] [CrossRef] [Green Version]
- Koufatzidou, M.; Koletsi, D.; Fleming, P.S.; Polychronopoulou, A.; Pandis, N. Outcome reporting discrepancies between trial entries and published final reports of orthodontic randomized controlled trials. Eur. J. Orthod. 2018, 41, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Bradna, P.; Ondráčková, L.; Zdimal, V.; Navrátil, T.; Pelclova, D. Detection of nanoparticles released at finishing of dental composite materials. Monatshefte Chem. Chem. Mon. 2017, 148, 531–537. [Google Scholar] [CrossRef]
- Day, C.J.; Price, R.; Sandy, J.R.; Ireland, A.J. Inhalation of aerosols produced during the removal of fixed orthodontic appliances: A comparison of 4 enamel cleanup methods. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 11–17. [Google Scholar] [CrossRef]
- Cokic, S.M.; Hoet, P.; Godderis, L.; Wiemann, M.; Asbach, C.; Reichl, F.X.; De Munck, J.; Van Meerbeek, B.; Van Landuyt, K.L. Cytotoxic effects of composite dust on human bronchial epithelial cells. Dent. Mater. 2016, 32, 1482–1491. [Google Scholar] [CrossRef]
- Cokic, S.; Duca, R.-C.; Godderis, L.; Hoet, P.H.; Seo, J.W.; Van Meerbeek, B.; Van Landuyt, K. Release of monomers from composite dust. J. Dent. 2017, 60, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Cokic, S.M.; Asbach, C.; De Munck, J.; Van Meerbeek, B.; Hoet, P.; Seo, J.W.; Van Landuyt, K.L. The effect of water spray on the release of composite nano-dust. Clin. Oral Investig. 2019, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Cokic, S.M.; Ghosh, M.; Hoet, P.; Godderis, L.; Van Meerbeek, B.; Van Landuyt, K.L. Cytotoxic and genotoxic potential of respirable fraction of composite dust on human bronchial cells. Dent. Mater. 2019, 36, 270–283. [Google Scholar] [CrossRef] [PubMed]
- Gioka, C.; Eliades, T.; Zinelis, S.; Pratsinis, H.; Athanasiou, A.; Eliades, G.; Kletsas, D. Characterization and in vitro estrogenicity of orthodontic adhesive particulates produced by simulated debonding. Dent. Mater. 2009, 25, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Ireland, A.J.; Moreno, T.; Price, R. Airborne particles produced during enamel cleanup after removal of orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 683–686. [Google Scholar] [CrossRef]
- Johnston, N.J.; Price, R.; Day, C.J.; Sandy, J.R.; Ireland, A.J. Quantitative and qualitative analysis of particulate production during simulated clinical orthodontic debonds. Dent. Mater. 2009, 25, 1155–1162. [Google Scholar] [CrossRef]
- Nilsen, B.W.; Jensen, E.; Örtengren, U.; Bang, B.; Michelsen, V.B. Airborne exposure to gaseous and particle-associated organic substances in resin-based dental materials during restorative procedures. Eur. J. Oral Sci. 2019, 127, 425–434. [Google Scholar] [CrossRef] [Green Version]
- Van Landuyt, K.; Hellack, B.; Van Meerbeek, B.; Peumans, M.; Hoet, P.H.; Wiemann, M.; Kuhlbusch, T.; Asbach, C. Nanoparticle release from dental composites. Acta Biomater. 2014, 10, 365–374. [Google Scholar] [CrossRef]
- Vig, P.; Atack, N.E.; Sandy, J.R.; Sherriff, M.; Ireland, A.J. Particulate production during debonding of fixed appliances: Laboratory investigation and randomized clinical trial to assess the effect of using flash-free ceramic brackets. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 767–778. [Google Scholar] [CrossRef]
- Zemouri, C.; De Soet, H.; Crielaard, W.; Laheij, A. A scoping review on bio-aerosols in healthcare and the dental environment. PLoS ONE 2017, 12, e0178007. [Google Scholar] [CrossRef]
- Koletsi, D.; Belibasakis, G.; Eliades, T. Interventions to reduce aerosolized pathogens in dental practice. A Protocol for a Systematic Review and Meta-Analysis. 2020. Available online: https://osf.io/ewph9/ (accessed on 1 May 2020).
- Coronavirus Situation Report Coronavirus Situation Report. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 22 April 2020).
- Cherrie, J.W.; Loh, M.; Aitken, R.J. Protecting healthcare workers from inhaled SARS-CoV-2 virus. Occup. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Seaton, A.; Godden, D.; MacNee, W.; Donaldson, K. Particulate air pollution and acute health effects. Lancet 1995, 345, 176–178. [Google Scholar] [CrossRef]
- Steerenberg, P.A.; Van Amelsvoort, L.; Lovik, M.; Hetland, R.B.; Alberg, T.; Halatek, T.; Bloemen, H.J.T.; Rydzynski, K.; Swaen, G.; Schwarze, P.; et al. Relation Between Sources of Particulate Air Pollution and Biological Effect Parameters in Samples from Four European Cities: An Exploratory Study. Inhal. Toxicol. 2006, 18, 333–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmalz, G.; Hickel, R.; Van Landuyt, K.L.; Reichl, F.-X. Scientific update on nanoparticles in dentistry. Int. Dent. J. 2018, 68, 299–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO) Occupational and Environmental Health Team. Hazard Prevention and Control in the Work Environment: Airborne Dust. World Health Organization. 1999. Available online: https://apps.who.int/iris/handle/10665/66147 (accessed on 5 May 2020).
- Vankerckhoven, H.; Lambrechts, P.; Van Beylen, M.; Davidson, C.; Vanherle, G. Unreacted Methacrylate Groups on the Surfaces of Composite Resins. J. Dent. Res. 1982, 61, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Bogdan, A.; Buckett, M.I.; Japuntich, D.A. Nano-Sized Aerosol Classification, Collection and Analysis—Method Development Using Dental Composite Materials. J. Occup. Environ. Hyg. 2014, 11, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Turci, F.; Pavan, C.; Leinardi, R.; Tomatis, M.; Pastero, L.; Garry, D.; Anguissola, S.; Lison, D.; Fubini, B. Revisiting the paradigm of silica pathogenicity with synthetic quartz crystals: the role of crystallinity and surface disorder. Part. Fibre Toxicol. 2016, 13, 32. [Google Scholar] [CrossRef] [Green Version]
- Vig, P.S. Orthodontics: Current principles and techniques. Am. J. Orthod. 1985, 87, 347–348. [Google Scholar] [CrossRef]
- Koletsi, D.; Fleming, P.S.; Michelaki, I.; Pandis, N. Heterogeneity in Cochrane and non-Cochrane meta-analyses in orthodontics. J. Dent. 2018, 74, 90–94. [Google Scholar] [CrossRef] [Green Version]
- Garcia, E.; Newfang, D.; Coyle, J.; Blake, C.L.; Spencer, J.W.; Burrelli, L.G.; Johnson, G.; Harbison, R.D. Evaluation of airborne asbestos exposure from routine handling of asbestos-containing wire gauze pads in the research laboratory. Regul. Toxicol. Pharmacol. 2018, 96, 135–141. [Google Scholar] [CrossRef]




| Study ID | Sample/Participants | Intervention (one or > 1) | Comparator (one or >1) | Technical Data | Outcome(s) |
|---|---|---|---|---|---|
| Bradna et al, 2017 In vitro Setting: composite specimens in Teflon molds | Composite grinding (no water cooling); air sampling 30 sec after end of grinding, closed cabinet (2 × 1.3 × 2.5 m) 4 composites | Filtek Ultimate (mixture of primary SiO2 and ZrO2 nanoparticles and zirconia- silica agglomerates) Estellite Sigma Quick, Supra-nano fill, silica-zirconia | Charisma Microhybrid (with Ba glass microparticles) Unfilled resin (LC Varnish) | Diamond round bur (medium and fine)/tungsten carbide (20 blade) Assessment: on-line spectrometer | Aerosol particle concentration Particle size distribution |
| Day et al, 2008 In vitro Setting: extracted teeth/impactor simulating lung | 24 teeth; orthodontic debond procedures; air sampling 15 min, at 30 cm sampling distance | High speed handpiece (water +/-) | Slow speed handpiece (water +/-) Control; no procedure | Spiral fluted tungsten carbide bur; Transbond XT adhesive and primer; Assessment: SEM, X-ray | Particulate matter Particulate composition |
| Cokic et al, 2016 In vitro Setting: composite sticks in metal mold | Composite grinding (no water cooling); laminar flow cabinet and dust transferred for to cell culture for toxicity assessment (96-well plates) 4 types composites | Filtek Supreme XTE nanocomposite Grandio and Tetric nanohybrid | Grandia Direct Microhybrid Z-100 MP conventional hybrid | All samples ground with rough diamond bur (100 μm) (micromotor, 200.000 rpm) Assessment: WST-1 assay; LDH leakage assay | Cytotoxicity against human bronchial cells IL-1β, IL-6 cytokine release Characterization of composite particles/dust |
| Cokic et al, 2017 In vitro Setting: composite sticks in metal mold | Composite grinding, (no water cooling), plexiglass chamber 27 × 27 × 42 cm; air sampling immediately before grinding until 10 min thereafter 4 types of composites (n = 5/per composite) | Filtek Supreme XTE nanocomposite Grandio (nanohybrid composite) | Gradia Direct Microhybrid Z100 MP conventional hybrid | All samples ground with rough diamond bur (100 μm) (micromotor, 200.000 rpm) Assessment: LC–MS/MS, TEM-EDS | Release of methacrylate monomers and BPA in water and ethanol Ultra-morphological and chemical analysis of dust |
| Cokic et al, 2019 In vitro Setting: composite sticks in metal mold | Composite grinding, closed chamber 1 m3; measurement 3 min during grinding and additional 10 min water +/- 7 types of composites (n = 3/per composite) | Filtek Supreme XTE nanocomposite GrandioSO and Herculite XRV Ultra nanohybrid composite | Spectrum TPH3 micromatrix with nanotechnology Herculite XRV microhybrid Durafill VS microfilled anterior composite Heliomolar flow microfill, flowable Control: no composite grinding | All samples ground with rough diamond bur (100 μm) (micromotor, 200.000 rpm) Assessment: SMPS, TEM-EDS | Particle number concentration, particle size distribution and average particle size Ultra-morphological and chemical analysis of dust |
| Cokic et al, 2020 In vitro Setting: composite sticks in metal mold | Composite grinding (no water cooling), plexiglass chamber 27 × 27 × 42 cm; measurement 3 min during grinding and additional 10 min; dust transferred for to cell culture for toxicity assessment (96-well plates) | Filtek Supreme XTE nanocomposite Grandio nanohybrid composite | Transbond XT | All samples ground with rough diamond bur (100 μm) (micromotor, 200.000 rpm) Assessment: DLS/ELS, WST-1 assay, LDH assay, comet assay, TEM | Particle size distribution Cell viability Membrane integrity DNA damage in individual cells Cellular uptake of particles by epithelial cells |
| Gioka et al, 2009 In vitro Setting: composite applied to cellulose-covered brackets | Composite grinding in simulated debonding, in a glass tube; no water cooling (n = 20/per composite) | Blugloo light cure | System 1 + chemical cure | All samples ground with 8-fluted tungsten carbide bur; high speed handpiece Assessment: micro-ATR FTIR spectroscopy, Scanning electron microscopy, X-ray microanalysis | Molecular characterization of particles Morphologic condition and structure Elemental composition of particles Estrogenicity |
| Ireland et al, 2003 In vivo (small cohort) Setting: dust collection during debonding in patients | Enamel clean up after debonding, air sampling 5–10 min | Transbond XT Ketac-Cem (glass polyalkenoate cement)-for bands | none | spiral fluted tungsten carbide bur; slow-speed handpiece Assessment: SEM, EDX | Particle size Chemical composition |
| Johnston et al, 2009 In vitro Setting: debonding of extracted teeth/impactor simulating lung | Enamel clean up after debonding; total sampling time 20 min (n = 20/group) | Stainless steel brackets, slow/high handpiece, water +/-, surgical facemask +/-, HVE +/- | Ceramic brackets, slow handpiece, no water, no facemask, no HVE. Fractured ceramic, high and slow handpiece, water +/-, surgical facemask +/-, HVE +/- | Carbide spiral fluted bur (ss, ceramic brackets) Diamond fissure bur + tungsten carbide bur (fractured ceramic brackets) Adhesive for brackets: Transbond XT Assessment: SEM, EDX | Qualitative/ quantitative analysis of particle size and composition |
| Nilsen et al, 2019 In vitro Setting: restorative treatment on phantoms | Restoration polishing; sampling period from the start of bonding procedure sampling pumps + water collection | Ceram.x universal | Clearfil SE Bond (primer) Clearfil SE Bond (bond) | Identoflex composite polisher, polishing diamonds (40, 20 μm), coarse, medium, fine, superfine grits (Sof-Lex) Assessment: GC/MS, (UHP)LC-MS | Qualitative and quantitative (molecular weight, retention times, molecular and characteristic ions) analysis |
| Van Landuyt et al, 2012 In vitro Setting: composite sticks in silicon mold [limited clinical part] | Composite grinding (no water cooling); composite blocks in a silicon mold, plexiglass box 27 × 27 × 42 mm; air sampling 30 min 7 types of composites (n = 5/ per composite) | Filtek Supreme XTE nanocomposite Premise and Ceram.X and Tetric EvoCeram and Herculite nanohybrid | Grandia Direct Microhybrid Z-100 MP conventional hybrid | All samples ground with rough diamond bur [grain size: 100 μm] (micromotor) Assessment: TEM | Dust concentration Number and distribution of submicron particles |
| Van Landuyt et al, 2014 In vitro Setting: composite sticks in metal mold [limited clinical part] | Composite grinding (no water cooling); composite blocks in a metal mold; plexiglass box 270 × 270 × 420 mm; air sampling NR 5 types of composites (n = 5/per composite) | Filtek Supreme XTE nanocomposite GrandiO and Tetric EvoCeram nanohybrid | Grandia Direct Microhybrid Z-100 MP conventional hybrid | All samples ground with rough diamond bur [grain size: 100 μm] (micromotor) Assessment: mini DiSC; TEM; SMPS; ESP; EPR | Number and distribution of submicron particles Chemical identity of sampled particles Size distribution of composite dust OH-generation and non-specific surface activity index |
| Vig et al, 2019 RCT Setting: hospital orthodontic department | 18 patients (6 per group); age NR; debonding procedures | Ceramic brackets with Transbond adhesive Ceramic adhesive pre-coated | Metal brackets with Transbond adhesive | All teeth ground with tungsten bur and slow-handpiece Assessment: (pDR)-1200 real-time monitor, Cascade impactor, SEM, EDX | Particulate concentration (respirable fraction) |
| Study | Baseline Similarity of Experimental Conditions (Selection Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Reporting (Reporting Bias) | Other Bias |
|---|---|---|---|---|---|
| Bradna et al, 2017 | low | unclear | low | unclear | low |
| Day et al, 2008 | low | unclear | low | unclear | low |
| Cokic et al, 2016 | low | unclear | low | unclear | low |
| Cokic et al, 2017 | low | unclear | low | unclear | low |
| Cokic et al, 2019 | low | unclear | low | unclear | low |
| Cokic et al, 2020 | low | unclear | low | unclear | low |
| Gioka et al, 2009 | low | unclear | low | unclear | low |
| Ireland et al, 2003 | high | unclear | low | unclear | unclear |
| Johnston et al, 2009 | low | unclear | low | unclear | low |
| Nilsen et al, 2019 | low | unclear | low | unclear | low |
| Van Landuyt et al, 2012 | low | unclear | low | unclear | low |
| Van Landuyt et al, 2014 | low | unclear | low | unclear | low |
| Study | Randomization Process | Deviations from Intended Interventions | Missing Outcome Data | Measurement of the Outcome | Selection of the Reported Result | Overall |
|---|---|---|---|---|---|---|
| Vig et al, 2019 | Low | Low | Low | Some concerns | Some concerns | Some concerns |
| # | Study ID | Comparison | Outcome | MD or SMD (95% CIs) | p-Value | Heterogeneity (I2%) |
|---|---|---|---|---|---|---|
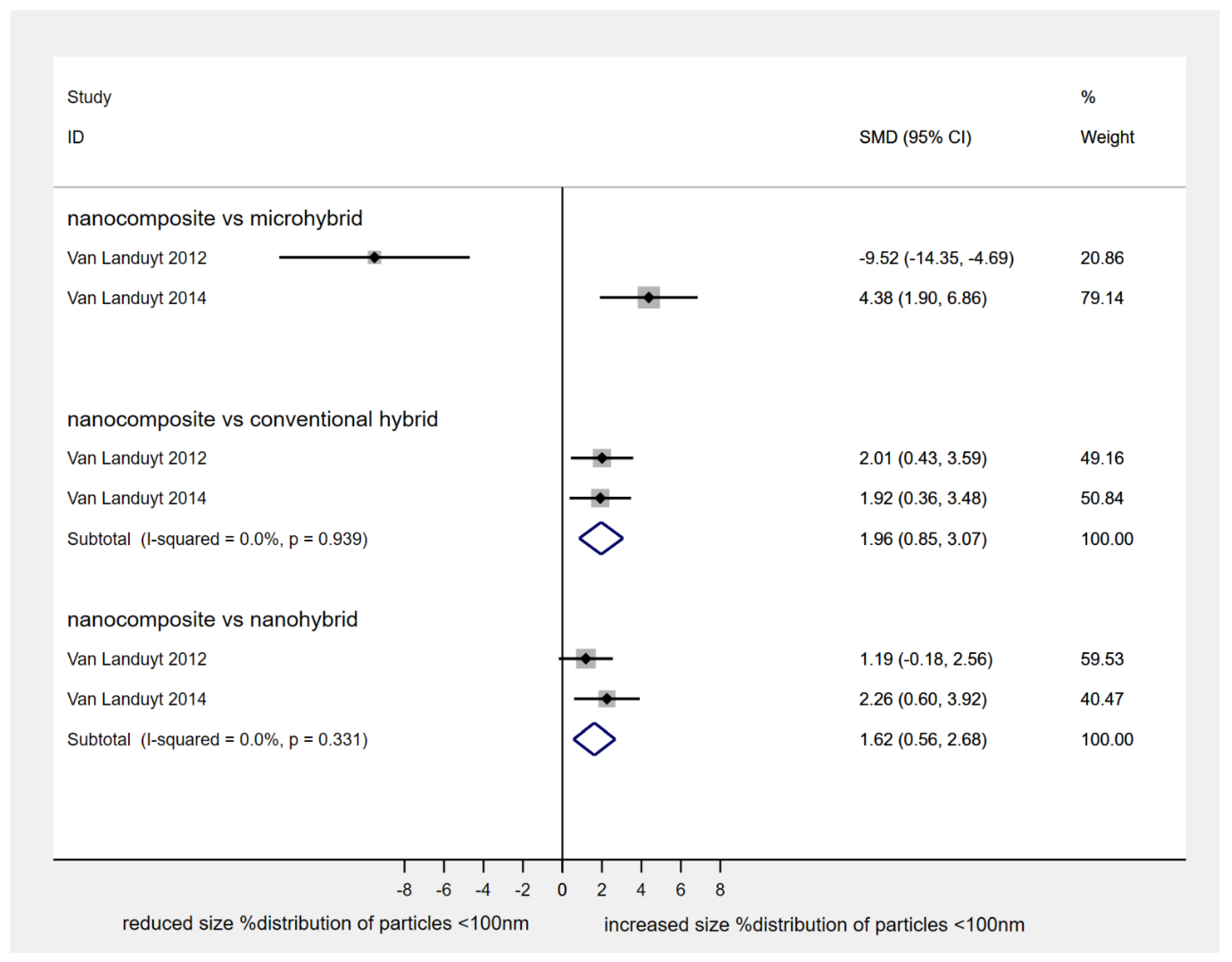
| 1 | 2 studies | Filtek Supreme XTE vs. Z100 MP | size% distribution of particles < 100 nm | SMD: 1.96 (0.85, 3.07) | 0.001 | 0 |
| Filtek Supreme XTE vs. Tetric EvoCeram | size% distribution of particles < 100 nm | SMD: 1.62 (0.56, 2.68) | 0.003 | 0 | ||
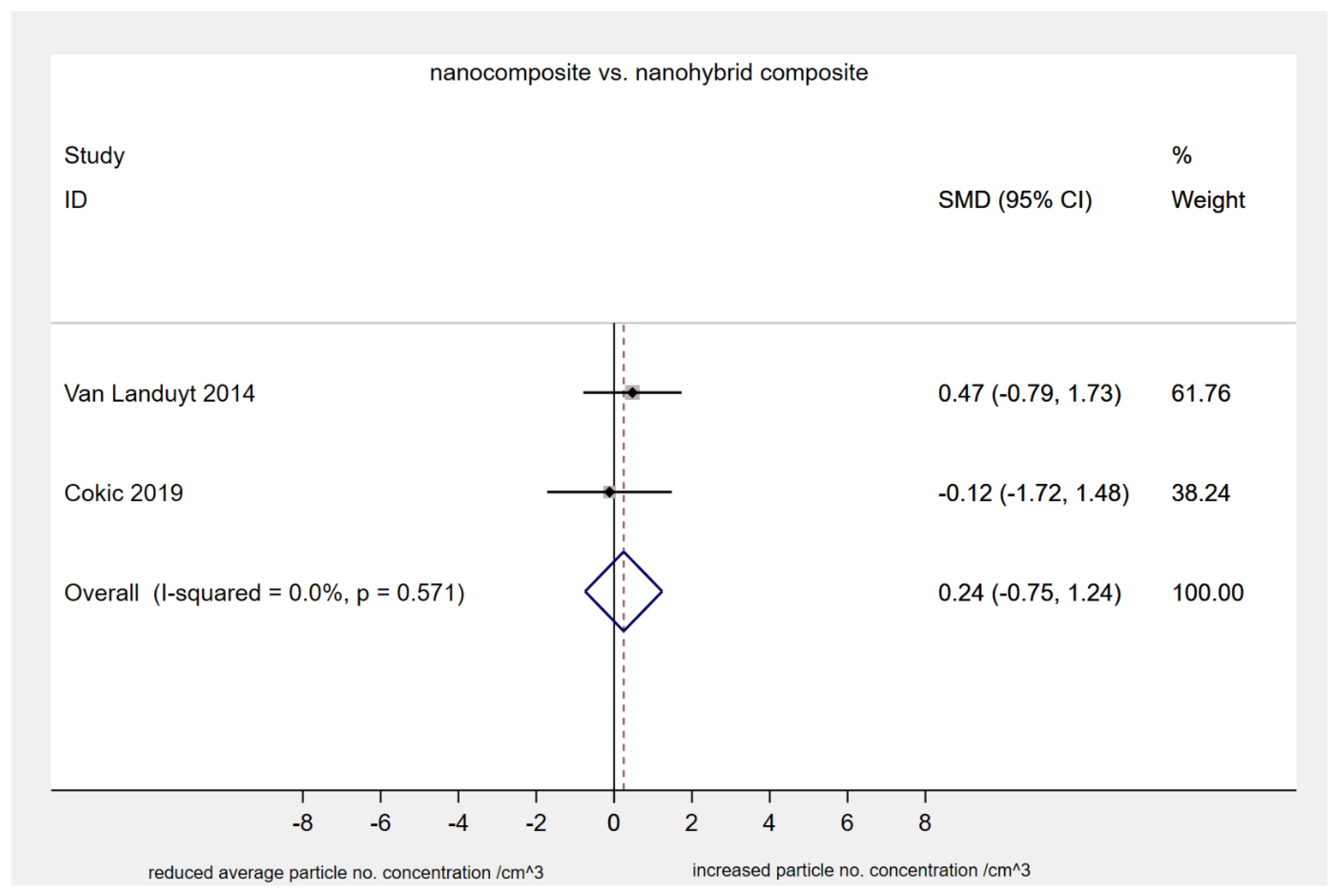
| 2 | 2 studies | Filtek Supreme XTE vs. GradiO | average particle number concentration (#/cm3 × 106) | SMD: 0.24 (−0.75, 1.24) | 0.63 | 0 |
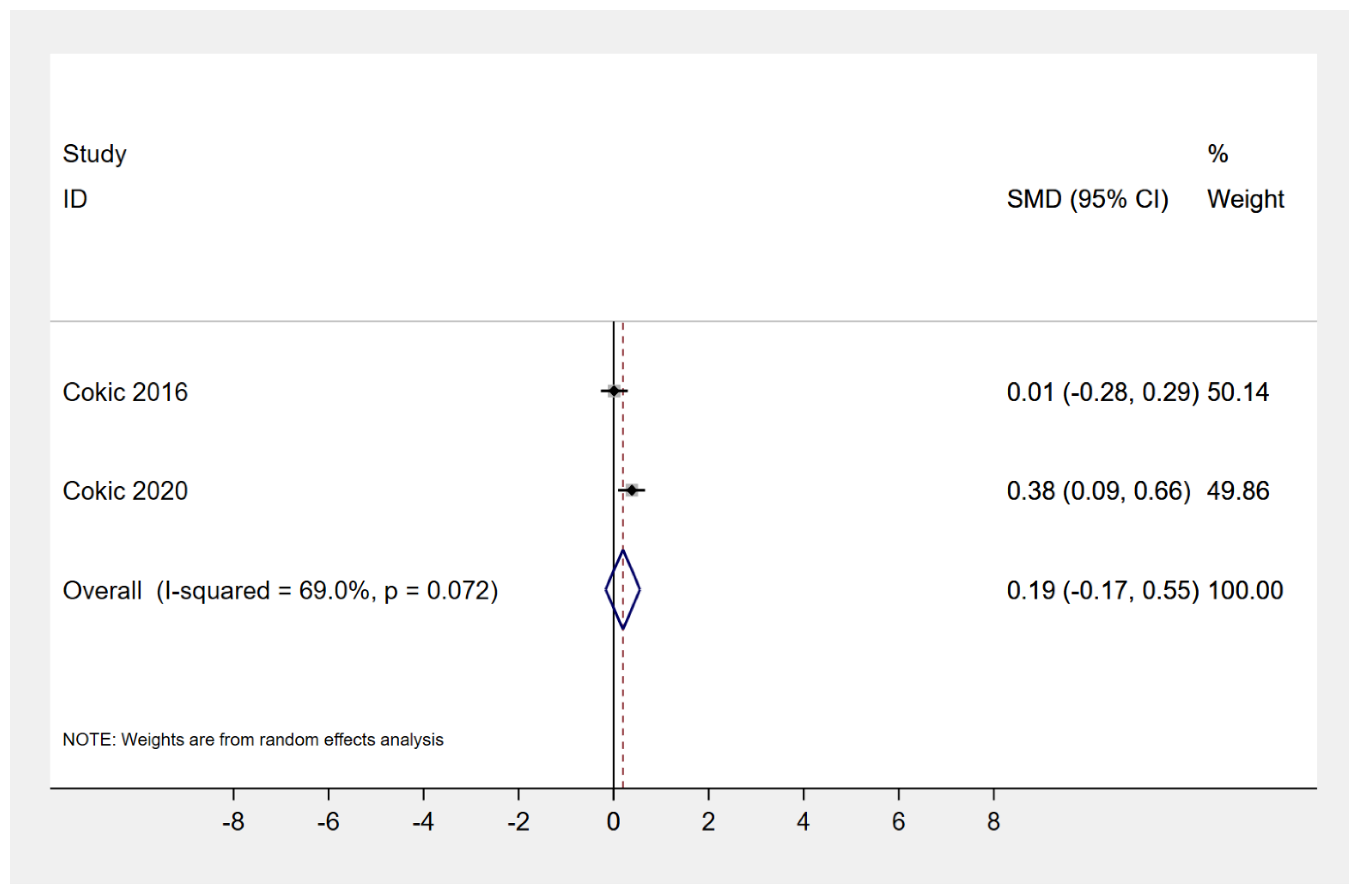
| 3 | 2 studies | Filtek Supreme XTE vs. GradiO | % formazan reduction at 330–400 μg/mL (cell viability, WST-1 assay) | SMD: 0.19 (−0.17, 0.55) | 0.30 | 69.0 |
| 4 | Cokic 2019 | Grinding of nanocomposite w/o water cooling vs. with water cooling (micromotor) | average particle number concentration (#/cm3 × 106) | MD: 1.5 (1.2, 1.7) | < 0.001 | − |
| 5 | Gioka 2009 | CC vs. control | MCF-7 cell proliferation (% control) | MD: 60 (51.5, 68.5) | < 0.001 | − |
| LC vs. control | MCF-7 cell proliferation (% control) | MD: 28 (22.4, 33.6) | < 0.001 | − | ||
| 6 | Cokic 2020 | Transbond XT (orthodontic) vs. Supreme XTE | % formazan reduction at 400 μg/mL (cell viability, WST-1 assay) 24 h | MD: 6.8 (4.7, 8.9) | < 0.001 | − |
| Transbond XT (orthodontic) vs. GradiO | % formazan reduction at 400 μg/mL (cell viability, WST-1 assay) 24 h | MD: 10.6 (7.3, 13.9) | < 0.001 | − | ||
| 7 | Cokic 2020 | Transbond XT (orthodontic) vs. Filtek Supreme XTE | % cell membrane integrity reduction (LDH assay) 72 h | MD: 6.1 (2.5, 9.7) | 0.001 | − |
| Transbond XT (orthodontic) vs. GradiO (nanohybrid) | % cell membrane integrity reduction (LDH assay) 72 h | MD: 10.9 (7.8, 14.0) | < 0.001 | − |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iliadi, A.; Koletsi, D.; Eliades, T.; Eliades, G. Particulate Production and Composite Dust during Routine Dental Procedures. A Systematic Review with Meta-Analyses. Materials 2020, 13, 2513. https://doi.org/10.3390/ma13112513
Iliadi A, Koletsi D, Eliades T, Eliades G. Particulate Production and Composite Dust during Routine Dental Procedures. A Systematic Review with Meta-Analyses. Materials. 2020; 13(11):2513. https://doi.org/10.3390/ma13112513
Chicago/Turabian StyleIliadi, Anna, Despina Koletsi, Theodore Eliades, and George Eliades. 2020. "Particulate Production and Composite Dust during Routine Dental Procedures. A Systematic Review with Meta-Analyses" Materials 13, no. 11: 2513. https://doi.org/10.3390/ma13112513