Prognosis versus Actual Outcomes in Stereotactic Radiosurgery of Brain Metastases: Reliability of Common Prognostic Parameters and Indices

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
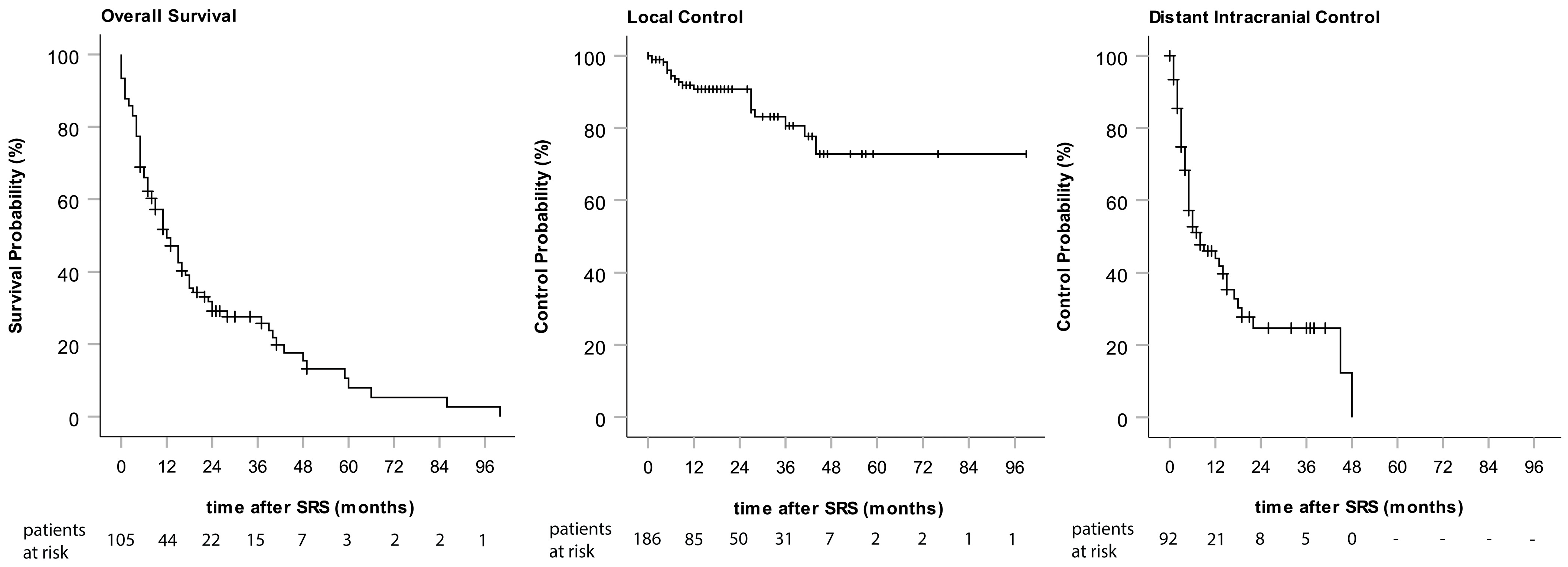
3.1. Outcomes
3.2. Prognostic Factor Evaluation
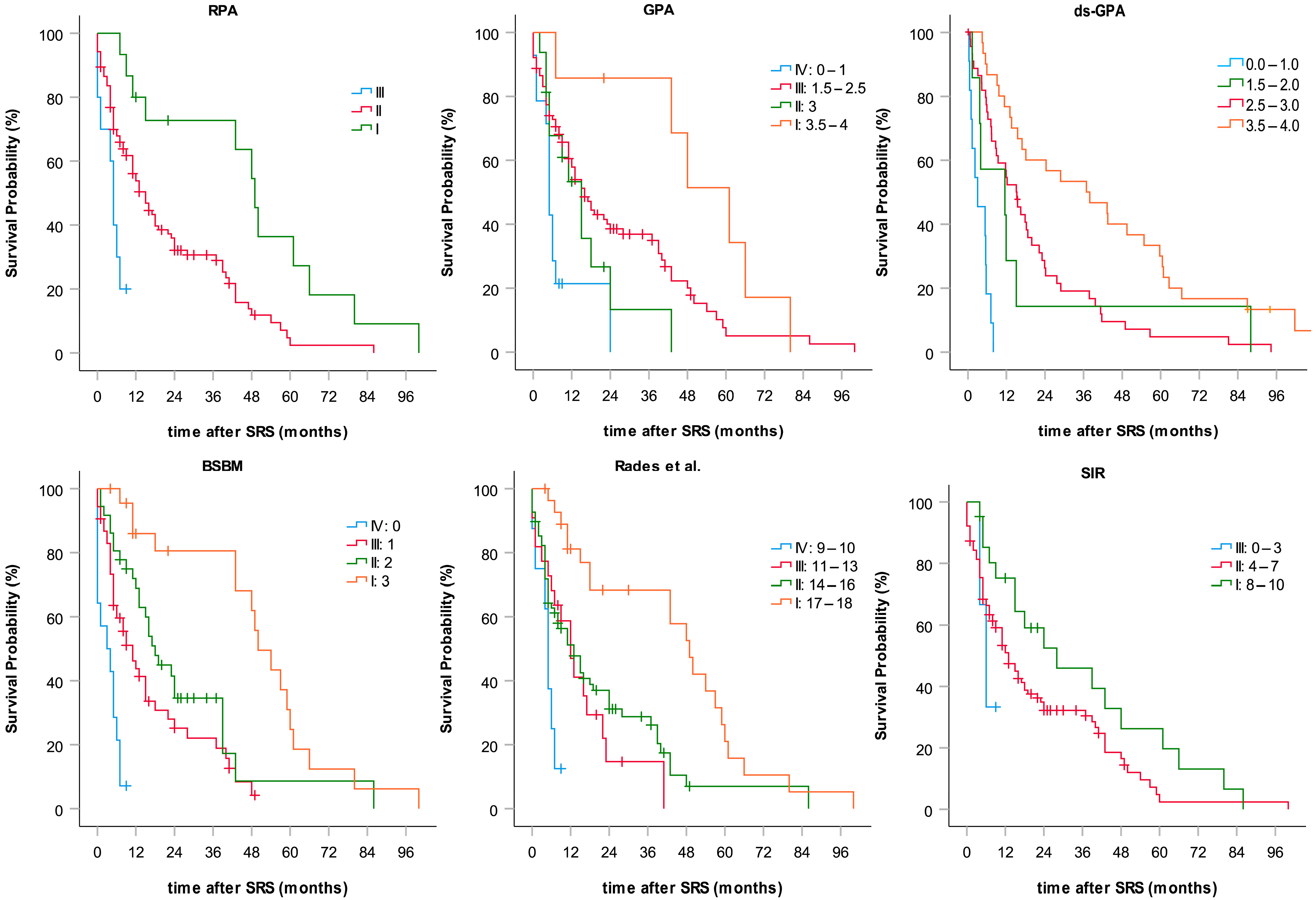
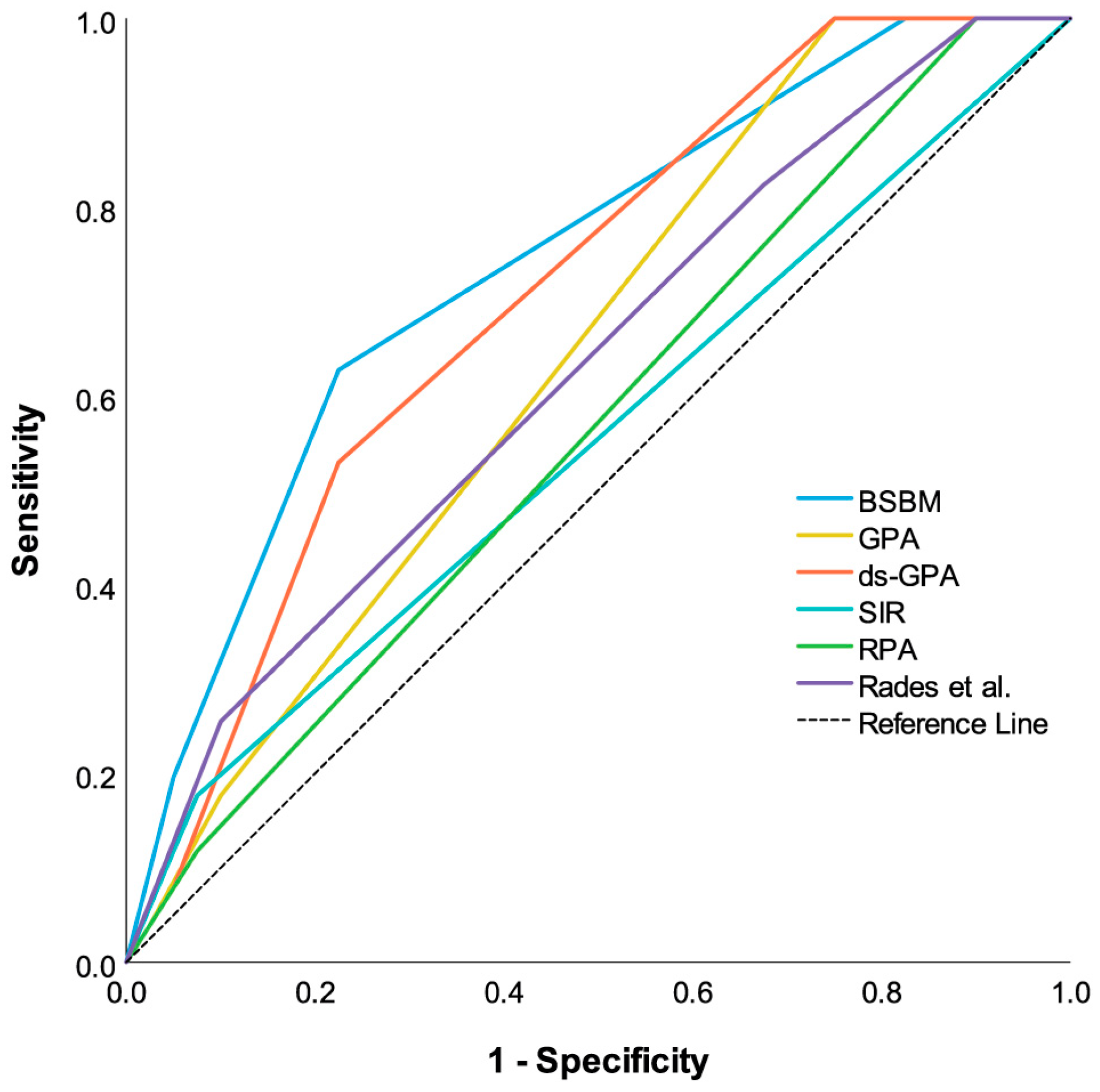
3.3. Evaluation of Prognostic Indices
3.4. Sex and OS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Linskey, M.E.; Andrews, D.W.; Asher, A.L.; Burri, S.H.; Kondziolka, D.; Robinson, P.D.; Ammirati, M.; Cobbs, C.S.; Gaspar, L.E.; Loeffler, J.S.; et al. The role of stereotactic radiosurgery in the management of patients with newly diagnosed brain metastases: A systematic review and evidence-based clinical practice guideline. J. Neurooncol. 2010, 96, 45–68. [Google Scholar] [CrossRef] [PubMed]
- Gavrilovic, I.T.; Posner, J.B. Brain metastases: Epidemiology and pathophysiology. J. Neurooncol. 2005, 75, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Schiff, D.; Messersmith, H.; Brastianos, P.K.; Brown, P.D.; Burri, S.; Dunn, I.F.; Gaspar, L.E.; Gondi, V.; Jordan, J.T.; Maues, J.; et al. Radiation Therapy for Brain Metastases: ASCO Guideline Endorsement of ASTRO Guideline. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2022, 40, JCO2200333. [Google Scholar] [CrossRef] [PubMed]
- Soffietti, R.; Kocher, M.; Abacioglu, U.M.; Villa, S.; Fauchon, F.; Baumert, B.G.; Fariselli, L.; Tzuk-Shina, T.; Kortmann, R.D.; Carrie, C.; et al. A European Organisation for Research and Treatment of Cancer phase III trial of adjuvant whole-brain radiotherapy versus observation in patients with one to three brain metastases from solid tumors after surgical resection or radiosurgery: Quality-of-life results. J. Clin. Oncol. 2013, 31, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Serizawa, T.; Shuto, T.; Akabane, A.; Higuchi, Y.; Kawagishi, J.; Yamanaka, K.; Sato, Y.; Jokura, H.; Yomo, S.; et al. Stereotactic radiosurgery for patients with multiple brain metastases (JLGK0901): A multi-institutional prospective observational study. Lancet Oncol. 2014, 15, 387–395. [Google Scholar] [CrossRef]
- Rogers, S.J.; Lomax, N.; Alonso, S.; Lazeroms, T.; Riesterer, O. Radiosurgery for Five to Fifteen Brain Metastases: A Single Centre Experience and a Review of the Literature. Front. Oncol. 2022, 12, 866542. [Google Scholar] [CrossRef] [PubMed]
- Giantini-Larsen, A.M.; Juthani, R.G.; Pannullo, S.C.; Knisely, J.P.S. Novel approaches to the management of patients with 5-15 brain metastases: A narrative review. Chin. Clin. Oncol. 2022, 11, 17. [Google Scholar] [CrossRef]
- Kocher, M.; Soffietti, R.; Abacioglu, U.; Villa, S.; Fauchon, F.; Baumert, B.G.; Fariselli, L.; Tzuk-Shina, T.; Kortmann, R.D.; Carrie, C.; et al. Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: Results of the EORTC 22952-26001 study. J. Clin. Oncol. 2011, 29, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Minniti, G.; Clarke, E.; Lanzetta, G.; Osti, M.F.; Trasimeni, G.; Bozzao, A.; Romano, A.; Enrici, R.M. Stereotactic radiosurgery for brain metastases: Analysis of outcome and risk of brain radionecrosis. Radiat. Oncol. 2011, 6, 48. [Google Scholar] [CrossRef]
- Peng, L.; Grimm, J.; Gui, C.; Shen, C.J.; Redmond, K.J.; Sloan, L.; Hazell, S.; Moore, J.; Huang, E.; Spoleti, N.; et al. Updated risk models demonstrate low risk of symptomatic radionecrosis following stereotactic radiosurgery for brain metastases. Surg. Neurol. Int. 2019, 10, 32. [Google Scholar] [CrossRef]
- Vellayappan, B.; Tan, C.L.; Yong, C.; Khor, L.K.; Koh, W.Y.; Yeo, T.T.; Detsky, J.; Lo, S.; Sahgal, A. Diagnosis and Management of Radiation Necrosis in Patients With Brain Metastases. Front. Oncol. 2018, 8, 395. [Google Scholar] [CrossRef] [PubMed]
- Wiggenraad, R.; Verbeek-de Kanter, A.; Mast, M.; Molenaar, R.; Kal, H.B.; Lycklama à Nijeholt, G.; Vecht, C.; Struikmans, H. Local progression and pseudo progression after single fraction or fractionated stereotactic radiotherapy for large brain metastases. Strahlenther. Onkol. 2012, 188, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, L.; Scott, C.; Rotman, M.; Asbell, S.; Phillips, T.; Wasserman, T.; McKenna, W.G.; Byhardt, R. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int. J. Radiat. Oncol. Biol. Phys. 1997, 37, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Sperduto, P.W.; Berkey, B.; Gaspar, L.E.; Mehta, M.; Curran, W. A new prognostic index and comparison to three other indices for patients with brain metastases: An analysis of 1,960 patients in the RTOG database. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 510–514. [Google Scholar] [CrossRef]
- Weltman, E.; Salvajoli, J.V.; Brandt, R.A.; de Morais Hanriot, R.; Prisco, F.E.; Cruz, J.C.; de Oliveira Borges, S.R.; Wajsbrot, D.B. Radiosurgery for brain metastases: A score index for predicting prognosis. Int. J. Radiat. Oncol. Biol. Phys. 2000, 46, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Lorenzoni, J.; Devriendt, D.; Massager, N.; David, P.; Ruiz, S.; Vanderlinden, B.; Van Houtte, P.; Brotchi, J.; Levivier, M. Radiosurgery for treatment of brain metastases: Estimation of patient eligibility using three stratification systems. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Rades, D.; Dunst, J.; Schild, S.E. A new scoring system to predicting the survival of patients treated with whole-brain radiotherapy for brain metastases. Strahlenther. Onkol. 2008, 184, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Rades, D.; Pluemer, A.; Veninga, T.; Hanssens, P.; Dunst, J.; Schild, S.E. Whole-brain radiotherapy versus stereotactic radiosurgery for patients in recursive partitioning analysis classes 1 and 2 with 1 to 3 brain metastases. Cancer 2007, 110, 2285–2292. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.G.; Guo, Y.; Zhang, X.; Song, S.J.; Xia, J.L.; Fan, F.Y.; Shi, M.; Wei, L.C. Brain metastasis: Experience of the Xi-Jing hospital. Ster. Funct. Neurosurg. 2002, 78, 70–83. [Google Scholar] [CrossRef]
- Li, B.; Yu, J.; Suntharalingam, M.; Kennedy, A.S.; Amin, P.P.; Chen, Z.; Yin, R.; Guo, S.; Han, T.; Wang, Y.; et al. Comparison of three treatment options for single brain metastasis from lung cancer. Int. J. Cancer 2000, 90, 37–45. [Google Scholar] [CrossRef]
- Aoyama, H.; Shirato, H.; Tago, M.; Nakagawa, K.; Toyoda, T.; Hatano, K.; Kenjyo, M.; Oya, N.; Hirota, S.; Shioura, H.; et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: A randomized controlled trial. JAMA 2006, 295, 2483–2491. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.L.; Wefel, J.S.; Hess, K.R.; Allen, P.K.; Lang, F.F.; Kornguth, D.G.; Arbuckle, R.B.; Swint, J.M.; Shiu, A.S.; Maor, M.H.; et al. Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: A randomised controlled trial. Lancet Oncol. 2009, 10, 1037–1044. [Google Scholar] [CrossRef]
- Brown, P.D.; Jaeckle, K.; Ballman, K.V.; Farace, E.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Barker, F.G., 2nd; Deming, R.; Burri, S.H.; et al. Effect of Radiosurgery Alone vs Radiosurgery With Whole Brain Radiation Therapy on Cognitive Function in Patients With 1 to 3 Brain Metastases: A Randomized Clinical Trial. JAMA 2016, 316, 401–409. [Google Scholar] [CrossRef]
- Lutterbach, J.; Cyron, D.; Henne, K.; Ostertag, C.B. Radiosurgery followed by planned observation in patients with one to three brain metastases. Neurosurgery 2008, 62 (Suppl. S2), 776–784. [Google Scholar] [CrossRef]
- Pirzkall, A.; Debus, J.; Lohr, F.; Fuss, M.; Rhein, B.; Engenhart-Cabillic, R.; Wannenmacher, M. Radiosurgery alone or in combination with whole-brain radiotherapy for brain metastases. J. Clin. Oncol. 1998, 16, 3563–3569. [Google Scholar] [CrossRef]
- Rades, D.; Hornung, D.; Blanck, O.; Martens, K.; Khoa, M.T.; Trang, N.T.; Hüppe, M.; Terheyden, P.; Gliemroth, J.; Schild, S.E. Stereotactic radiosurgery for newly diagnosed brain metastases. Strahlenther. Onkol. 2014, 190, 786–791. [Google Scholar] [CrossRef]
- Lawrence, Y.R.; Li, X.A.; el Naqa, I.; Hahn, C.A.; Marks, L.B.; Merchant, T.E.; Dicker, A.P. Radiation dose-volume effects in the brain. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S20–S27. [Google Scholar] [CrossRef] [PubMed]
- Bohoudi, O.; Bruynzeel, A.M.; Lagerwaard, F.J.; Cuijpers, J.P.; Slotman, B.J.; Palacios, M.A. Isotoxic radiosurgery planning for brain metastases. Radiother. Oncol. 2016, 120, 253–257. [Google Scholar] [CrossRef]
- Shaw, E.; Scott, C.; Souhami, L.; Dinapoli, R.; Bahary, J.P.; Kline, R.; Wharam, M.; Schultz, C.; Davey, P.; Loeffler, J.; et al. Radiosurgery for the treatment of previously irradiated recurrent primary brain tumors and brain metastases: Initial report of radiation therapy oncology group protocol (90-05). Int. J. Radiat. Oncol. Biol. Phys. 1996, 34, 647–654. [Google Scholar] [CrossRef]
- Wiggenraad, R.; Verbeek-de Kanter, A.; Kal, H.B.; Taphoorn, M.; Vissers, T.; Struikmans, H. Dose-effect relation in stereotactic radiotherapy for brain metastases. A systematic review. Radiother. Oncol. 2011, 98, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Rades, D.; Kueter, J.-D.; Hornung, D.; Veninga, T.; Hanssens, P.; Schild, S.E.; Dunst, J. Comparison of stereotactic radiosurgery (SRS) alone and whole brain radiotherapy (WBRT) plus a stereotactic boost (WBRT + SRS) for one to three brain metastases. Strahlenther. Onkol. 2008, 184, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Sperduto, P.W.; Yang, T.J.; Beal, K.; Pan, H.; Brown, P.D.; Bangdiwala, A.; Shanley, R.; Yeh, N.; Gaspar, L.E.; Braunstein, S.; et al. Estimating Survival in Patients With Lung Cancer and Brain Metastases: An Update of the Graded Prognostic Assessment for Lung Cancer Using Molecular Markers (Lung-molGPA). JAMA Oncol. 2017, 3, 827–831. [Google Scholar] [CrossRef] [PubMed]
- Sperduto, P.W.; Mesko, S.; Li, J.; Cagney, D.; Aizer, A.; Lin, N.U.; Nesbit, E.; Kruser, T.J.; Chan, J.; Braunstein, S.; et al. Survival in Patients With Brain Metastases: Summary Report on the Updated Diagnosis-Specific Graded Prognostic Assessment and Definition of the Eligibility Quotient. J. Clin. Oncol. 2020, 38, 3773–3784. [Google Scholar] [CrossRef] [PubMed]
- Tomasini, P.; Serdjebi, C.; Khobta, N.; Metellus, P.; Ouafik, L.H.; Nanni, I.; Greillier, L.; Loundou, A.; Fina, F.; Mascaux, C.; et al. EGFR and KRAS Mutations Predict the Incidence and Outcome of Brain Metastases in Non-Small Cell Lung Cancer. Int. J. Mol. Sci. 2016, 17, 2132. [Google Scholar] [CrossRef] [PubMed]
- Kondziolka, D.; Parry, P.V.; Lunsford, L.D.; Kano, H.; Flickinger, J.C.; Rakfal, S.; Arai, Y.; Loeffler, J.S.; Rush, S.; Knisely, J.P.; et al. The accuracy of predicting survival in individual patients with cancer. J. Neurosurg. 2014, 120, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Rades, D.; Pluemer, A.; Veninga, T.; Schild, S.E. Comparison of different treatment approaches for one to two brain metastases in elderly patients. Strahlenther. Onkol. 2008, 184, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Yang, X.; Zhang, L.; Xu, M. Prognostic and Predictive Markers of Limited (1-4) Brain Metastases in Patients with Lung Adenocarcinoma After Stereotactic Radiosurgery: A Retrospective Analysis. World Neurosurg. 2022, 164, e671–e680. [Google Scholar] [CrossRef] [PubMed]
- Willmann, J.; Badra, E.V.; Adilovic, S.; Christ, S.M.; Ahmadsei, M.; Mayinger, M.; Tanadini-Lang, S.; Guckenberger, M.; Andratschke, N. Distant metastasis velocity as a novel prognostic score for overall survival after disease progression following stereotactic body radiotherapy for oligometastatic disease. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, 871–882. [Google Scholar] [CrossRef] [PubMed]
- Roengvoraphoj, O.; Eze, C.; Niyazi, M.; Li, M.; Hildebrandt, G.; Fietkau, R.; Belka, C.; Manapov, F. Prognostic role of patient gender in limited-disease small-cell lung cancer treated with chemoradiotherapy. Strahlenther. Onkol. 2017, 193, 150–155. [Google Scholar] [CrossRef]
- Müller, A.C.; Gani, C.; Rehm, H.M.E.; Eckert, F.; Bamberg, M.; Hehr, T.; Weinmann, M. Are there biologic differences between male and female breast cancer explaining inferior outcome of men despite equal stage and treatment?! Strahlenther. Onkol. 2012, 188, 782–787. [Google Scholar] [CrossRef]
- Jung, K.-W.; Park, S.; Shin, A.; Oh, C.-M.; Kong, H.-J.; Jun, J.K.; Won, Y.-J. Do Female Cancer Patients Display Better Survival Rates Compared with Males? Analysis of the Korean National Registry Data, 2005–2009. PLoS ONE 2012, 7, e52457. [Google Scholar] [CrossRef] [PubMed]
- Cook, M.B.; McGlynn, K.A.; Devesa, S.S.; Freedman, N.D.; Anderson, W.F. Sex disparities in cancer mortality and survival. Cancer Epidemiol. Biomark. Prev. 2011, 20, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Zindler, J.D.; Jochems, A.; Lagerwaard, F.J.; Beumer, R.; Troost, E.G.C.; Eekers, D.B.P.; Compter, I.; van der Toorn, P.P.; Essers, M.; Oei, B.; et al. Individualized early death and long-term survival prediction after stereotactic radiosurgery for brain metastases of non-small cell lung cancer: Two externally validated nomograms. Radiother. Oncol. 2017, 123, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Mangesius, J.; Seppi, T.; Bates, K.; Arnold, C.R.; Minasch, D.; Mangesius, S.; Kerschbaumer, J.; Lukas, P.; Ganswindt, U.; Nevinny-Stickel, M. Hypofractionated and single-fraction radiosurgery for brain metastases with sex as a key predictor of overall survival. Sci. Rep. 2021, 11, 8639. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | n (%) | |
|---|---|---|
| Patients | n | 108 |
| Number of SRSs | n | 132 |
| Number of SRSs per patient | Median | 1 |
| Range | 1–5 | |
| Only one SRS in lifetime | 82 (75.9%) | |
| Number of metastases | n | 213 |
| Number of metastases treated per SRS | Median | 1 |
| Range | 1–5 | |
| Only one metastasis treated | 75 (56.8%) | |
| Sex | Female | 51 (47.2%) |
| Male | 57 (52.8%) | |
| Age | Median | 63 |
| Range | 22–85 | |
| Primary tumor | NSCLC | 51 (47.2%) |
| NSCLC adeno | 40 (37%) | |
| NSCLC squamous cell | 9 (8.3%) | |
| Breast | 11 (10.2%) | |
| Melanoma | 20 (18.5%) | |
| RCC | 9 (8.3%) | |
| Others | 19 (17.6%) | |
| Time to brain metastasis [months] | Median | 14.5 months |
| Range | 0–439 months | |
| KPI | <80 | 24 (18.2%) |
| ≥80 | 108 (81.8%) | |
| Immobilization | Stereotactic ring | 121 (91.7%) |
| Thermoplastic mask | 11 (8.3%) | |
| SRS dose (80% isodose) | Median | 20 Gy |
| Range | 13–22 Gy | |
| Volume of largest metastasis | <5 ccm | 99 (87.6%) |
| 5–13 | 13 (11.5%) | |
| >13 ccm | 1 (0.9%) | |
| Extracranial metastases | Yes | 95 (74.8%) |
| No | 32 (25.2%) | |
| Controlled primary | Yes | 59 (46.5%) |
| No | 68 (53.5%) |
| Factor | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | ||
| Age | 1.01 (0.99–1.01) | 0.489 | |||
| Time to metastasis | 1.00 (1.00–1.00) | 0.844 | |||
| Number of metastases | 0.88 (0.68–1.13) | ns (0.309) | |||
| Volume of largest metastasis | 1.06 (0.97–1.14) | 0.188 | |||
| Extra cerebral metastases | Present | 2.60 (1.56–4.33) | <0.001 | 1.26 (0.60–2.66) | 0.538 |
| Not present | 1.0 (ref) | NA | 1.0 (ref) | NA | |
| Dose | 1.33 (0.97–1.83) | 0.077 | |||
| Sex | Female | 0.52 (0.34–0.78) | 0.001 | 0.56 (0.34–0.91) | 0.020 |
| Male | 1.0 (ref) | NA | 1.0 (ref) | NA | |
| Histology | NSCLC adeno | 1.0 (ref) | 0.018 | 1.0 (ref) | 0.36 |
| NSCLC squamous | 2.16 (0.99–4.71) | 0.054 | 2.42 (1.07–5.47) | 0.033 | |
| Breast | 0.69 (0.35–1.34) | 0.270 | 1.13 (0.52–2.44) | 0.756 | |
| Melanoma | 1.02 (0.57–1.82) | 0.953 | 1.41 (0.75–2.67) | 0.288 | |
| RCC | 1.92 (0.94–3.89) | 0.072 | 1.49 (0.68–3.24) | 0.319 | |
| Other | 2.16 (1.18–3.94) | 0.012 | 1.54 (0.82–2.90) | 0.184 | |
| KPI | 0.77 (0.67–0.89) | <0.001 | 0.77 (0.66-0.90) | <0.001 | |
| Systemic disease status | 1.57 (1.30–1.91) | <0.001 | 1.45 (1.10–1.92) | 0.008 | |
| NSCLC EGFR | Mutated | 0.66 (0.24–1.712) | 0.404 | ||
| Negative or unknown | 1.0 (ref) | NA | |||
| Melanoma BRAF | Mutated | 0.71 (0.27–1.91) | 0.501 | ||
| Negative or unknown | 1.0 (ref) | NA | |||
| Breast subtype | Luminal A | 1.0 (ref) | NA | ||
| Luminal B | 0.12 ( 0.02–1.32) | 0.084 | |||
| Her2-positive | 0.06 (0.01–1.13) | 0.060 | |||
| Triple-negative | 3.75 (0.32–44.41) | 0.295 | |||
| Score | Group | Patients in Group (n) | Median OS (Months) | Lower 95% KI | Upper 95% KI | p-Value (Log Rank) |
|---|---|---|---|---|---|---|
| Overall OS | 15 | 9.87 | 20.13 | |||
| BSBM | 0 | 14 | 3 | 0.00 | 8.50 | <0.0001 |
| 1 | 53 | 10 | 6.21 | 15.79 | ||
| 2 | 36 | 18 | 13.52 | 22.48 | ||
| 3 | 17 | 50 | 40.40 | 59.60 | ||
| GPA | 0–1 | 14 | 5 | 4.09 | 5.91 | 0.001 |
| 1.5–2.5 | 89 | 16 | 11.16 | 20.84 | ||
| 3 | 16 | 15 | 8.77 | 21.23 | ||
| 3.5–4 | 7 | 61 | 40.92 | 81.08 | ||
| ds-GPA | 0–1 | 11 | 4 | 0.00 | 7.43 | <0.0001 |
| 1.5–2.5 | 7 | 19 | 0.05 | 30.61 | ||
| 3 | 45 | 20 | 10.05 | 19.98 | ||
| 3.5–4 | 30 | 42 | 11.39 | 61.72 | ||
| SIR | 0–3 | 3 | 6 | 2.80 | 9.20 | 0.095 |
| 4–7 | 102 | 16 | 8.72 | 17.28 | ||
| 8–10 | 21 | 39 | 12.74 | 52.98 | ||
| RPA | III | 10 | 5 | 3.48 | 6.52 | <0.0001 |
| II | 104 | 15 | 10.65 | 19.35 | ||
| I | 15 | 49 | 41.74 | 56.26 | ||
| Rades et al. | 9–10 | 8 | 5 | 3.66 | 6.34 | <0.0001 |
| 11–13 | 22 | 12 | 6.99 | 17.01 | ||
| 14–16 | 68 | 13 | 7.68 | 18.32 | ||
| 17–18 | 28 | 49 | 39.54 | 58.46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mangesius, J.; Seppi, T.; Arnold, C.R.; Mangesius, S.; Kerschbaumer, J.; Demetz, M.; Minasch, D.; Vorbach, S.M.; Sarcletti, M.; Lukas, P.; et al. Prognosis versus Actual Outcomes in Stereotactic Radiosurgery of Brain Metastases: Reliability of Common Prognostic Parameters and Indices. Curr. Oncol. 2024, 31, 1739-1751. https://doi.org/10.3390/curroncol31040132
Mangesius J, Seppi T, Arnold CR, Mangesius S, Kerschbaumer J, Demetz M, Minasch D, Vorbach SM, Sarcletti M, Lukas P, et al. Prognosis versus Actual Outcomes in Stereotactic Radiosurgery of Brain Metastases: Reliability of Common Prognostic Parameters and Indices. Current Oncology. 2024; 31(4):1739-1751. https://doi.org/10.3390/curroncol31040132
Chicago/Turabian StyleMangesius, Julian, Thomas Seppi, Christoph Reinhold Arnold, Stephanie Mangesius, Johannes Kerschbaumer, Matthias Demetz, Danijela Minasch, Samuel Moritz Vorbach, Manuel Sarcletti, Peter Lukas, and et al. 2024. "Prognosis versus Actual Outcomes in Stereotactic Radiosurgery of Brain Metastases: Reliability of Common Prognostic Parameters and Indices" Current Oncology 31, no. 4: 1739-1751. https://doi.org/10.3390/curroncol31040132