Outcomes of Patients with Non-Small Cell Lung Cancer and Brain Metastases Treated with the Upfront Single Agent Pembrolizumab: A Retrospective and Multicentric Study of the ESCKEYP GFPC Cohort

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Assessments
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patients and Tumor Characteristics
3.2. Characteristics of Brain Metastases
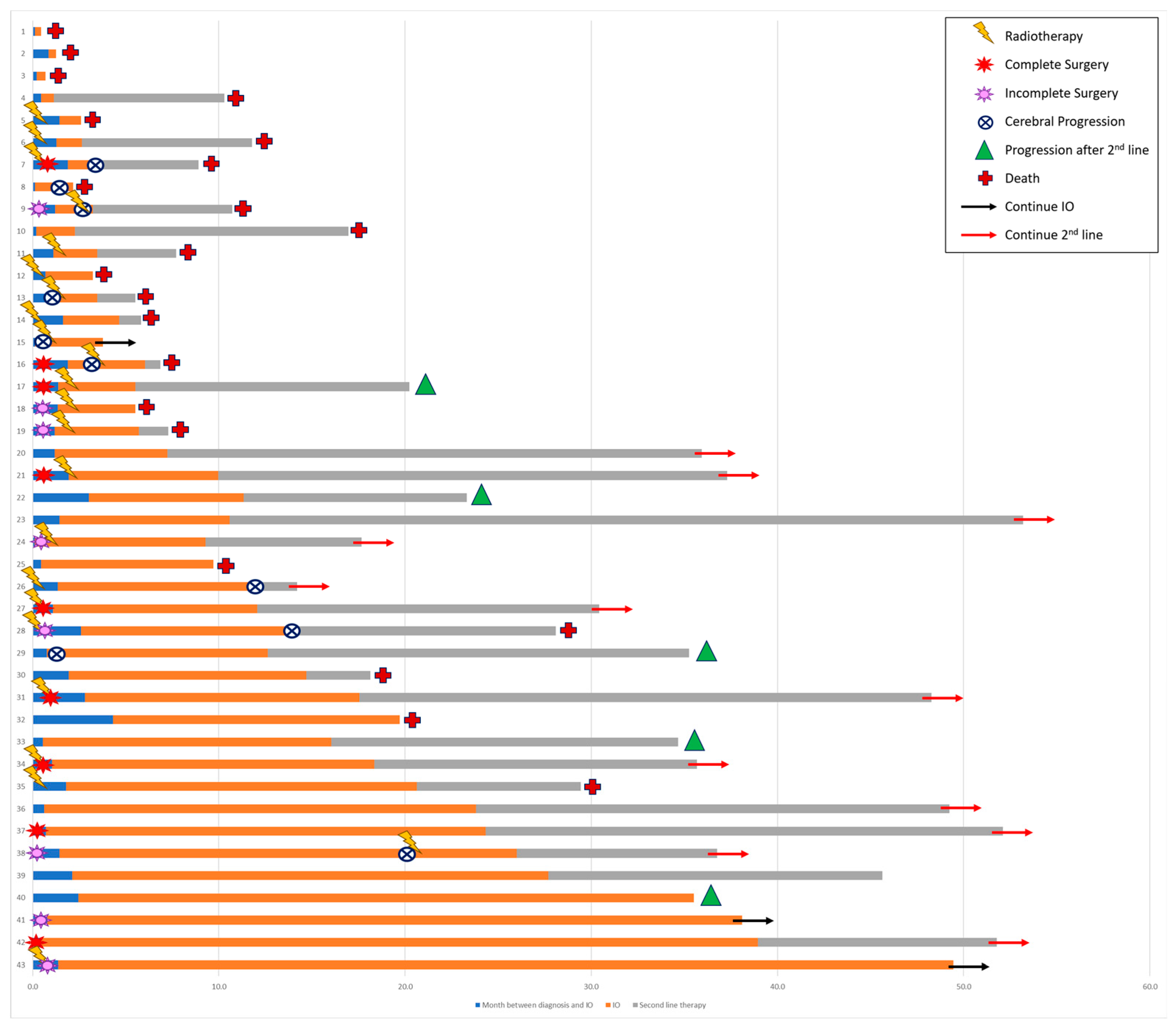
3.3. Local Management of Brain Metastasis
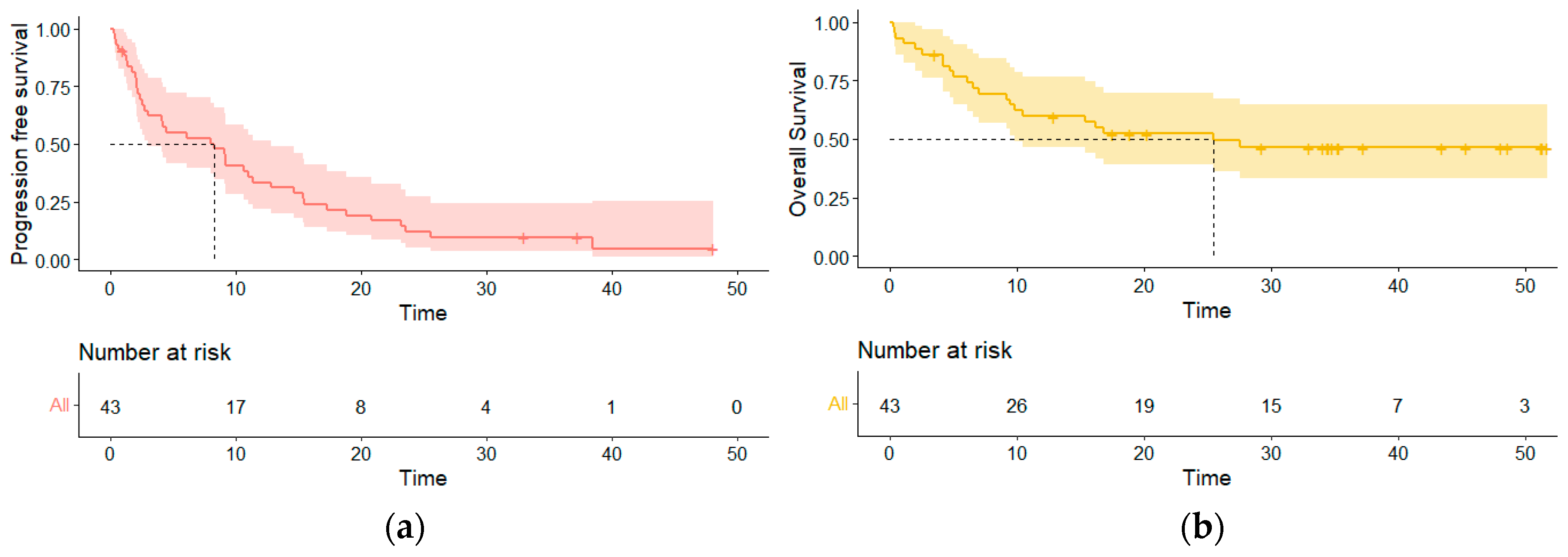
3.4. Outcomes
3.5. Following Therapy
3.6. Prognostic Factors for Cerebral Progression
3.7. Prognostic Factors for Systemic Progression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nayak, L.; Lee, E.Q.; Wen, P.Y. Epidemiology of brain metastases. Curr. Oncol. Rep. 2012, 14, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Waqar, S.N.; Samson, P.P.; Robinson, C.G.; Bradley, J.; Devarakonda, S.; Du, L.; Govindan, R.; Gao, F.; Puri, V.; Morgensztern, D. Non-small-cell lung cancer with brain metastasis at presentation. Clin. Lung Cancer 2018, 19, e373–e379. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Mesko, S.; Li, J.; Cagney, D.; Aizer, A.; Lin, N.U.; Nesbit, E.; Kruser, T.J.; Chan, J.; Braunstein, S.; et al. Survival in patients with brain metastases: Summary report on the updated diagnosis-specific graded prognostic assessment and definition of the eligibility quotient. J. Clin. Oncol. 2020, 38, 3773–3784. [Google Scholar] [CrossRef]
- Patel, R.R.; Verma, V.; Miller, A.B.; Lin, T.A.; Jethanandani, A.; Espinoza, A.F.; Mainwaring, W.; Augustyn, A.; Fuller, C.D.; Sulman, E.P.; et al. Exclusion of patients with brain metastases from cancer clinical trials. Neuro Oncol. 2020, 22, 577–579. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus chemotherapy in metastatic non–small-cell lung cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Şenler, F.Ç.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus chemotherapy for squamous non–small-cell lung cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus chemotherapy for PD-L1–positive non–small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Di Giacomo, A.M.; Valente, M.; Cerase, A.; Lofiego, M.F.; Piazzini, F.; Calabrò, L.; Gambale, E.; Covre, A.; Maio, M. Immunotherapy of brain metastases: Breaking a “dogma”. J. Exp. Clin. Cancer Res. 2019, 38, 419. [Google Scholar] [CrossRef]
- Abid, H.; Watthanasuntorn, K.; Shah, O.; Gnanajothy, R. Efficacy of pembrolizumab and nivolumab in crossing the blood brain barrier. Cureus 2019, 11, e4446. [Google Scholar] [CrossRef] [PubMed]
- Le Rhun, E.; Guckenberger, M.; Smits, M.; Dummer, R.; Bachelot, T.; Sahm, F.; Galldiks, N.; de Azambuja, E.; Berghoff, A.S.; Metellus, P.; et al. EANO–ESMO clinical practice guidelines for diagnosis, treatment and follow-up of patients with brain metastasis from solid tumours. Ann. Oncol. 2021, 32, 1332–1347. [Google Scholar] [CrossRef]
- Sas-Korczynska, B.; Rucinska, M. WBRT for brain metastases from non-small cell lung cancer: For whom and when?-Contemporary point of view. J. Thorac. Dis. 2021, 13, 3246–3257. [Google Scholar] [CrossRef] [PubMed]
- Nieder, C.; Guckenberger, M.; Gaspar, L.E.; Rusthoven, C.G.; De Ruysscher, D.; Sahgal, A.; Nguyen, T.; Grosu, A.L.; Mehta, M.P. Management of patients with brain metastases from non-small cell lung cancer and adverse prognostic features: Multi-national radiation treatment recommendations are heterogeneous. Radiat. Oncol. 2019, 14, 33. [Google Scholar] [CrossRef] [PubMed]
- Powell, S.F.; Rodríguez-Abreu, D.; Langer, C.J.; Tafreshi, A.; Paz-Ares, L.; Kopp, H.G.; Rodríguez-Cid, J.; Kowalski, D.M.; Cheng, Y.; Kurata, T.; et al. Outcomes with pembrolizumab plus platinum-based chemotherapy for patients with NSCLC and stable brain metastases: Pooled analysis of KEYNOTE-021, -189, and -407. J. Thorac. Oncol. 2021, 16, 1883–1892. [Google Scholar] [CrossRef]
- Langer, C.J.; Gadgeel, S.M.; Borghaei, H.; Papadimitrakopoulou, V.A.; Patnaik, A.; Powell, S.F.; Gentzler, R.D.; Martins, R.G.; Stevenson, J.P.; Jalal, S.I.; et al. Carboplatin and pemetrexed with or without pembrolizumab for advanced, non-squamous non-small-cell lung cancer: A randomised, phase 2 cohort of the open-label KEYNOTE-021 study. Lancet Oncol. 2016, 17, 1497–1508. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, S.B.; Schalper, K.A.; Gettinger, S.N.; Mahajan, A.; Herbst, R.S.; Chiang, A.C.; Lilenbaum, R.; Wilson, F.H.; Omay, S.B.; Yu, J.B.; et al. Pembrolizumab for management of patients with NSCLC and brain metastases: Long-term results and biomarker analysis from a non-randomised, open-label, phase 2 trial. Lancet Oncol. 2020, 21, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, L.E.L.; Henon, C.; Auclin, E.; Mezquita, L.; Ferrara, R.; Audigier-Valette, C.; Mazieres, J.; Lefebvre, C.; Rabeau, A.; Le Moulec, S.; et al. Outcome of patients with non-small cell lung cancer and brain metastases treated with checkpoint inhibitors. J. Thorac. Oncol. 2019, 14, 1244–1254. [Google Scholar] [CrossRef]
- Descourt, R.; Greillier, L.; Perol, M.; Ricordel, C.; Auliac, J.B.; Falchero, L.; Demontrond, P.; Veillon, R.; Vieillot, S.; Guisier, F.; et al. First-line pembrolizumab monotherapy for PD-L1-positive (TPS ≥ 50%) advanced non-small cell lung cancer (aNSCLC) in the real world: A national French bispective multicentric cohort—ESCKEYP trial (GFPC 05-2018). J. Clin. Oncol. 2021, 39, 9091. [Google Scholar] [CrossRef]
- Brastianos, P.K.; Kim, A.E.; Giobbie-Hurder, A.; Lee, E.Q.; Lin, N.U.; Overmoyer, B.; Wen, P.Y.; Nayak, L.; Cohen, J.V.; Dietrich, J.; et al. Pembrolizumab in brain metastases of diverse histologies: Phase 2 trial results. Nat. Med. 2023, 29, 1728–1737. [Google Scholar] [CrossRef]
- Nadal, E.; Rodríguez-Abreu, D.; Simó, M.; Massutí, B.; Juan, O.; Huidobro, G.; López, R.; De Castro, J.; Estival, A.; Mosquera, J.; et al. Phase II trial of atezolizumab combined with carboplatin and pemetrexed for patients with advanced nonsquamous non-small-cell lung cancer with untreated brain metastases (Atezo-Brain, GECP17/05). J. Clin. Oncol. 2023, 41, 4478–4485. [Google Scholar] [CrossRef]
- Arvanitis, C.D.; Ferraro, G.B.; Jain, R.K. The blood-brain barrier and blood-tumour barrier in brain tumours and metastases. Nat. Rev. Cancer 2020, 20, 26–41. [Google Scholar] [CrossRef]
- Eguren-Santamaria, I.; Sanmamed, M.F.; Goldberg, S.B.; Kluger, H.M.; Idoate, M.A.; Lu, B.Y.; Corral, J.; Schalper, K.A.; Herbst, R.S.; Gil-Bazo, I. PD-1/PD-L1 blockers in NSCLC brain metastases: Challenging paradigms and clinical practice. Clin. Cancer Res. 2020, 26, 4186–4197. [Google Scholar] [CrossRef]
- Kim, N.; Kim, H.K.; Lee, K.; Hong, Y.; Cho, J.H.; Choi, J.W.; Lee, J.I.; Suh, Y.L.; Ku, B.M.; Eum, H.H.; et al. Single-cell RNA sequencing demonstrates the molecular and cellular reprogramming of metastatic lung adenocarcinoma. Nat. Commun. 2020, 11, 2285. [Google Scholar] [CrossRef]
- Brastianos, P.; Carter, S.; Santagata, S.; Cahill, D.; Taylor-Weiner, A.; Jones, R.; Ligon, K.; Tabernero, J.; Seoane, J.; Martinez Saez, E.; et al. 2905 Genomic characterization of brain metastases and paired primary tumors reveals branched evolution and potential therapeutic targets. Eur. J. Cancer 2015, 51, S586. [Google Scholar] [CrossRef]
- Fischer, G.M.; Jalali, A.; Kircher, D.A.; Lee, W.C.; McQuade, J.L.; Haydu, L.E.; Joon, A.Y.; Reuben, A.; de Macedo, M.P.; Carapeto, F.C.L.; et al. Molecular profiling reveals unique immune and metabolic features of melanoma brain metastases. Cancer Discov. 2019, 9, 628–645. [Google Scholar] [CrossRef]
- Masson, F.; Calzascia, T.; Berardino-Besson, W.D.; de Tribolet, N.; Dietrich, P.Y.; Walker, P.R. Brain microenvironment promotes the final functional maturation of tumor-specific effector CD8+ T cells. J. Immunol. 2007, 179, 845–853. [Google Scholar] [CrossRef]
- Goldberg, S.B.; Gettinger, S.N.; Mahajan, A.; Chiang, A.C.; Herbst, R.S.; Sznol, M.; Tsiouris, A.J.; Cohen, J.; Vortmeyer, A.; Jilaveanu, L.; et al. Pembrolizumab for patients with melanoma or non-small-cell lung cancer and untreated brain metastases: Early analysis of a non-randomised, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 976–983. [Google Scholar] [CrossRef]
- Sun, L.; Davis, C.W.; Hwang, W.T.; Jeffries, S.; Sulyok, L.F.; Marmarelis, M.E.; Singh, A.P.; Berman, A.T.; Feigenberg, S.J.; Levin, W.; et al. Outcomes in Patients with Non-small-cell Lung Cancer with Brain Metastases Treated with Pembrolizumab-based Therapy. Clin. Lung Cancer 2021, 22, 58–66.e3. [Google Scholar] [CrossRef]
- de Alencar, V.T.L.; Camandaroba, M.P.G.; Pirolli, R.; Fogassa, C.A.Z.; de Lima, V.C.C. Immunotherapy as Single Treatment for Patients with NSCLC with Brain Metastases: A Systematic Review and Meta-Analysis—The META-L-BRAIN Study. J. Thorac. Oncol. 2021, 16, 1379–1391. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Lin, N.U.; Lee, E.Q.; Aoyama, H.; Barani, I.J.; Barboriak, D.P.; Baumert, B.G.; Bendszus, M.; Brown, P.D.; Camidge, D.R.; Chang, S.M.; et al. Response assessment criteria for brain metastases: Proposal from the RANO group. Lancet Oncol. 2015, 16, e270–e278. [Google Scholar] [CrossRef] [PubMed]
- Nishijima, T.F.; Shachar, S.S.; Nyrop, K.A.; Muss, H.B. Safety and tolerability of PD-1/PD-L1 inhibitors compared with chemotherapy in patients with advanced cancer: A meta-analysis. Oncologist 2017, 22, 470–479. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Population, n (%) |
|---|---|
| Age (years), Median (range) | 64 (44–84) |
| Sex | |
| Male | 30 (69.7) |
| ECOG PS | |
| 0–1 | 31 (72.1) |
| ≥2 | 12 (27.9) |
| Smoking status | |
| Never smoker | 5 (11.6) |
| Former smoker (>1 year) | 18 (41.9) |
| Current smoker | 19 (44.2) |
| Unknown | 1 (2.3) |
| Histology | |
| Adenocarcinoma | 34 (79.1) |
| Squamous | 4 (9.3) |
| Others | 5 (11.6) |
| Tumor PD-L1 expression † | |
| 50–75% | 19 (46.3) |
| ≥75% | 22 (51.2) |
| Mutational status | |
| KRAS | 14 (32.6) |
| P53 | 5 (11.6) |
| BRAF | 1 (2.3) |
| MET | 1 (2.3) |
| ROS1 | 1 (2.3) |
| Others | 2 (4.6) |
| Characteristics | Patients, n (%) |
|---|---|
| Imaging for BM diagnosis | |
| MRI | 23 (53.5) |
| CT-scan | 20 (46.5) |
| Timing of diagnosis | |
| Synchronous | 38 (88.4) |
| Metachronous | 5 (11.6) |
| Symptomatic BM | |
| Yes | 28 (65.1) |
| Localization | |
| Parietal | 19 (44.2) |
| Temporal | 15 (34.9) |
| Frontal | 14 (32.6) |
| Occipital | 14 (32.6) |
| Infratentorial | 12 (27.9) |
| Number of BM, Median (range) | 2 (1–12) |
| Size’s sum of all BM, mm, Median (range) | 28.4 (5.0–136.2) |
| Size of the largest BM, mm, Median (range) | 19.3 (4.4–41.1) |
| Surface of the largest BM, cm2, Median (range) | 3.1 (0.1–27.2) |
| Biggest area of edema, cm2, Median (range) | 14.2 (0.3–87.9) |
| Necrosis, (n = 39) † | |
| ≤25% | 16 (41) |
| 25–50% | 5 (12.8) |
| 50–75% | 4 (10.3) |
| ≥75% | 14 (35.9) |
| Local Treatment | Patients, n (%) |
|---|---|
| Surgery | 18 (41.9) |
| Complete | 10 (23.3) |
| Incomplete | 8 (18.6) |
| Radiotherapy | |
| SRS | 8 (18.6) |
| WBRT | 5 (11.6) |
| Post-surgery SRS | 12 (27.9) |
| Timing between radiotherapy and ICI administration | |
| Radiotherapy before ICI | 12 (48) |
| Concomitant | 13 (52) |
| Delay between radiotherapy and start of ICI, weeks, Median (range) | 1 (1–4) |
| Brain response after local therapy and before ICI | |
| CR | 10 (40) |
| PR | 9 (36) |
| SD | 0 (0) |
| PD | 3 (12) |
| Death before new imaging | 3 (12) |
| Characteristics | Patients, n (%) |
|---|---|
| Delay between diagnosis and start of ICI, days, Median (range) | 36 (3–132) |
| Best responses characteristics for BM according to RECIST criteria | |
| CR | 15 (34.9) |
| PR | 13 (30.2) |
| SD | 3 (7) |
| PD | 12 (27.9) |
| Best responses characteristics for BM according to RANO criteria | |
| CR | 16 (37.2) |
| PR | 10 (23.3) |
| SD | 3 (7) |
| PD | 14 (32.6) |
| Number of cycles before best responses †, Median (range) | 5 (1–13) |
| Shrinkage of BM after start of ICI, Median (range) | 51 (0–100) |
| Shrinkage of brain edema after start of ICI, Median (range) | 82 (−6–100) |
| Type of progressive disease, n (%) ∆ | |
| New BM | 2 (20) |
| Existing BM | 4 (40) |
| Both | 4 (40) |
| Progression free survival, month, Median [95% CI] | 8.3 [3.0; 13.8] |
| Cerebral progression free survival, month, Median [95% CI] | 5.3 [3.0; 14.7] |
| Systemic progression free survival, month, Median [95% CI] | 9.2 [4.5; 17.3] |
| Dissociate response between BM and extracerebral metastasis | |
| No | 3 (11.5) |
| Only systemic progression | 16 (61.5) |
| Only cerebral progression | 7 (26.9) |
| Reason of definitive interruption of ICI ‖ | |
| Progressive disease | 15 (55.6) |
| Adverse event | 4 (14.8) |
| Death | 3 (11.1) |
| Other | 5 (18.5) |
| Overall survival, month, Median [95% CI] | 25.5 [9.8–NR] |
| Characteristics | HR (95% CI) |
|---|---|
| Surgery | 0.327 [0.138; 0.770] (p = 0.011) |
| Ratio of cumulative size of BM (mm)/number of BM | 1.050 [1.008; 1.093] (p = 0.018) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nannini, S.; Guisier, F.; Curcio, H.; Ricordel, C.; Demontrond, P.; Abdallahoui, S.; Baloglu, S.; Greillier, L.; Chouaid, C.; Schott, R. Outcomes of Patients with Non-Small Cell Lung Cancer and Brain Metastases Treated with the Upfront Single Agent Pembrolizumab: A Retrospective and Multicentric Study of the ESCKEYP GFPC Cohort. Curr. Oncol. 2024, 31, 1656-1666. https://doi.org/10.3390/curroncol31030126
Nannini S, Guisier F, Curcio H, Ricordel C, Demontrond P, Abdallahoui S, Baloglu S, Greillier L, Chouaid C, Schott R. Outcomes of Patients with Non-Small Cell Lung Cancer and Brain Metastases Treated with the Upfront Single Agent Pembrolizumab: A Retrospective and Multicentric Study of the ESCKEYP GFPC Cohort. Current Oncology. 2024; 31(3):1656-1666. https://doi.org/10.3390/curroncol31030126
Chicago/Turabian StyleNannini, Simon, Florian Guisier, Hubert Curcio, Charles Ricordel, Pierre Demontrond, Safa Abdallahoui, Seyyid Baloglu, Laurent Greillier, Christos Chouaid, and Roland Schott. 2024. "Outcomes of Patients with Non-Small Cell Lung Cancer and Brain Metastases Treated with the Upfront Single Agent Pembrolizumab: A Retrospective and Multicentric Study of the ESCKEYP GFPC Cohort" Current Oncology 31, no. 3: 1656-1666. https://doi.org/10.3390/curroncol31030126