Comparative Effectiveness and Safety of Trastuzumab Biosimilars to Herceptin for Adjuvant Treatment of HER2+ Breast Cancer

 and
and
Abstract
:1. Introduction
2. Methods
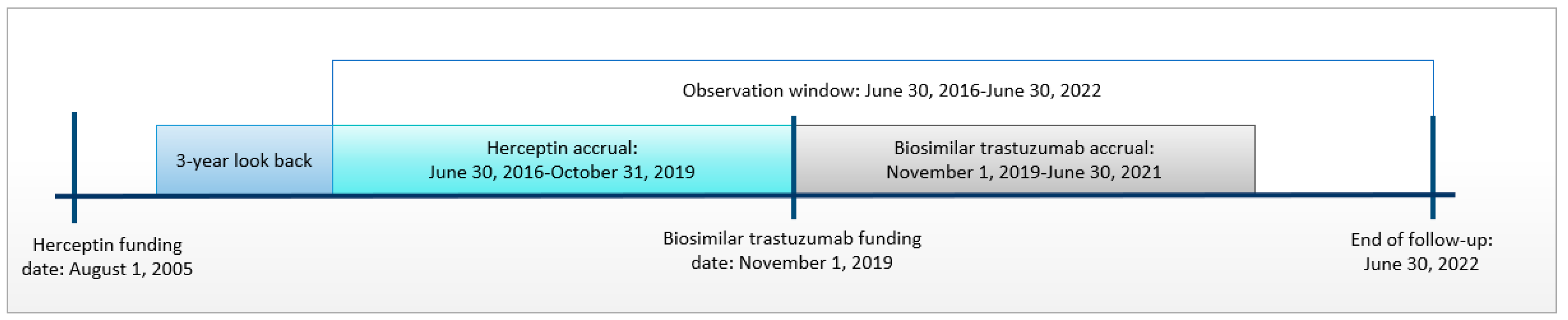
2.1. Study Design and Population
2.2. Data Sources
2.3. Outcomes
2.4. Covariates
2.5. Statistical Analysis
3. Results
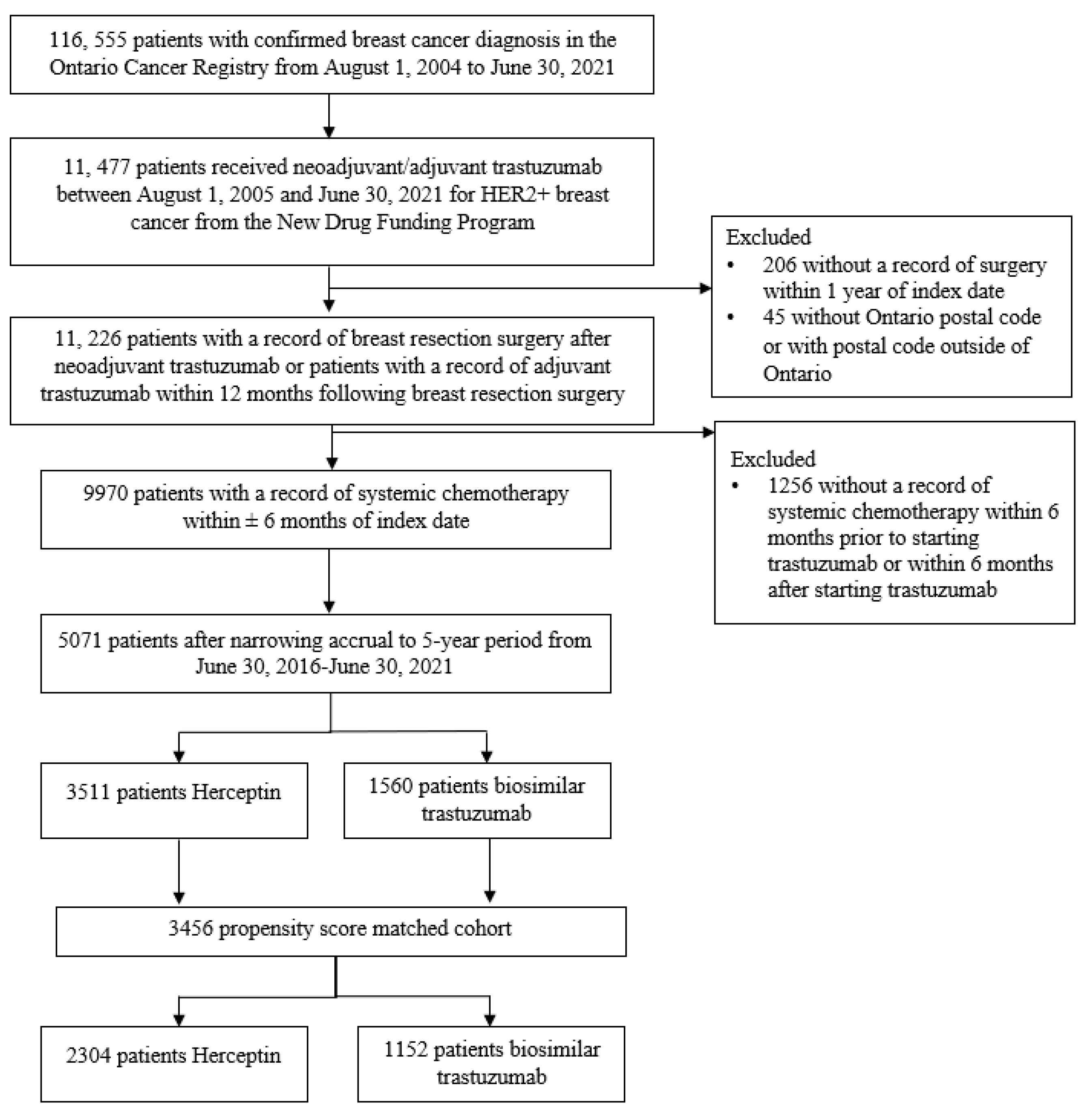
3.1. Study Cohort
3.2. Safety Analysis
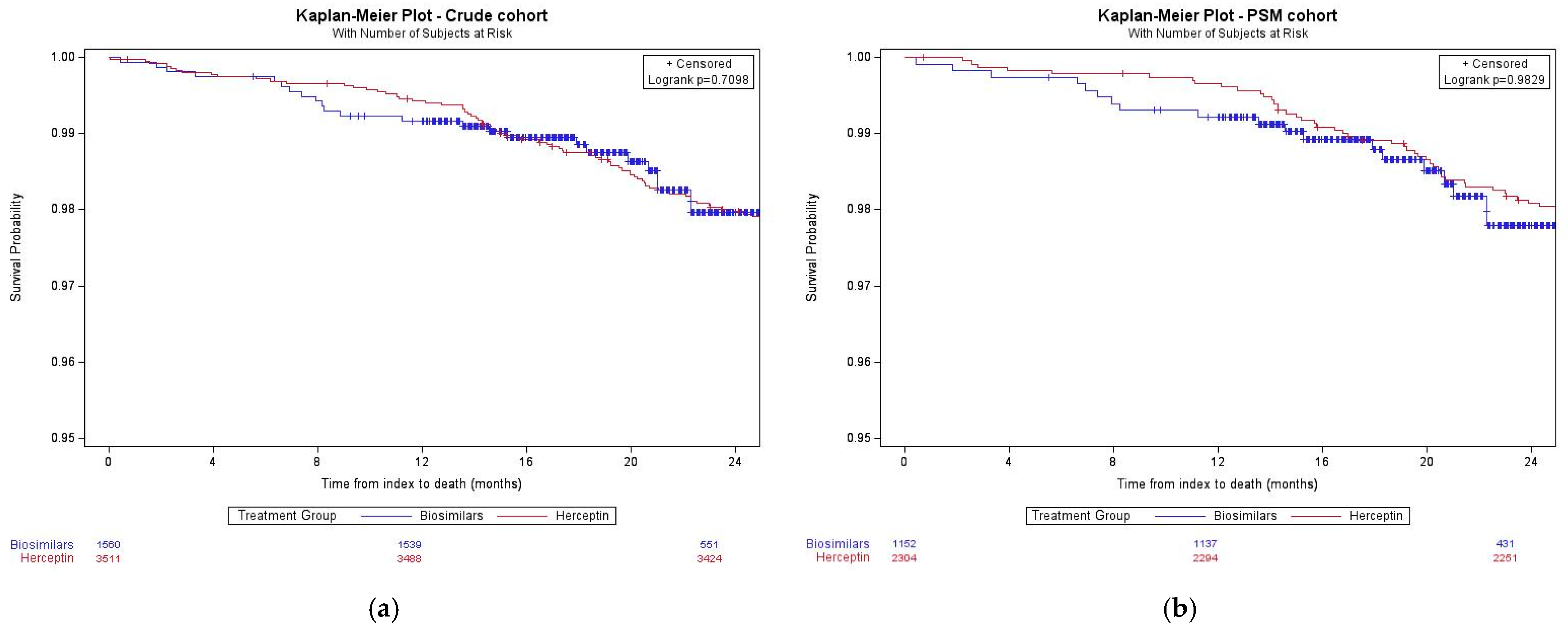
3.3. Effectiveness Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Slamon, D.; Godolphin, W.; Jones, L.; Holt, J.; Wong, S.; Keith, D.; Levin, W.; Stuart, S.; Udove, J.; Ullrich, A.; et al. Studies of the HER-2/Neu Proto-Oncogene in Human Breast and Ovarian Cancer. Science 1989, 244, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Wilson, F.; Coombes, M.; Brezden-Masley, C.; Yurchenko, M.; Wylie, C.; Douma, R.; Varu, A.; Hutton, B.; Skidmore, B.; Cameron, C. Herceptin® (trastuzumab) in HER2-positive early breast cancer: A systematic review and cumulative network meta-analysis. Syst. Rev. 2018, 7, 191. [Google Scholar] [CrossRef] [PubMed]
- Cancer Care Ontario New Drug Funding Program. Available online: https://www.cancercareontario.ca/en/Funding/New_Drug_Funding_Program (accessed on 14 October 2022).
- (pERC) pCODR ERC. Pertuzumab-Trastuzumab (Perjeta-Herceptin Combo Pack) EBC-PERC Final Recommendation. 2018. Available online: https://www.cadth.ca/sites/default/files/pcodr/pcodr_pertuzumab-trastuzumab_perjeta-herceptin-combo_ebc_fn_rec.pdf (accessed on 13 June 2022).
- Provincial Drug Reimbursement Programs-Ontario Health (Cancer Care Ontario). New Drug Funding Program Announcement-Trastuzumab (Ogivri or Trazimera) Biosimilar. Published Online 2019. Available online: https://www.cancercareontario.ca/en/drugformulary/drugs/trastuzumab (accessed on 13 June 2022).
- Government of Canada. Biosimilar Biologic Drugs in Canada: Fact Sheet. 27 August 2019. Available online: https://www.canada.ca/en/health-canada/services/drugs-health-products/biologics-radiopharmaceuticals-genetic-therapies/applications-submissions/guidance-documents/fact-sheet-biosimilars.html (accessed on 14 October 2022).
- Stebbing, J.; Baranau, Y.; Baryash, V.; Manikhas, A.; Moiseyenko, V.; Dzagnidze, G.; Zhavrid, E.; Boliukh, D.; Stroyakovskii, D.; Pikiel, J.; et al. CT-P6 compared with reference trastuzumab for HER2-positive breast cancer: A randomised, double-blind, active-controlled, phase 3 equivalence trial. Lancet Oncol. 2017, 18, 917–928. [Google Scholar] [CrossRef] [PubMed]
- Stebbing, J.; Baranau, Y.V.; Baryash, V.; Manikhas, A.; Moiseyenko, V.; Dzagnidze, G.; Zhavrid, E.; Boliukh, D.; Pikiel, J.; Eniu, A.E.; et al. Long-term efficacy and safety of CT-P6 versus trastuzumab in patients with HER2-positive early breast cancer: Final results from a randomized phase III trial. Breast Cancer Res. Treat. 2021, 188, 631–640. [Google Scholar] [CrossRef] [PubMed]
- von Minckwitz, G.; Colleoni, M.; Kolberg, H.C.; Morales, S.; Santi, P.; Tomasevic, Z.; Zhang, N.; Hanes, V. Efficacy and safety of ABP 980 compared with reference trastuzumab in women with HER2-positive early breast cancer (LILAC study): A randomised, double-blind, phase 3 trial. Lancet Oncol. 2018, 19, 987–998. [Google Scholar] [CrossRef] [PubMed]
- Esteva, F.J.; Baranau, Y.V.; Baryash, V.; Manikhas, A.; Moiseyenko, V.; Dzagnidze, G.; Zhavrid, E.; Boliukh, D.; Stroyakovskiy, D.; Pikiel, J.; et al. Efficacy and safety of CT-P6 versus reference trastuzumab in HER2-positive early breast cancer: Updated results of a randomised phase 3 trial. Cancer Chemother. Pharmacol. 2019, 84, 839–847. [Google Scholar] [CrossRef] [PubMed]
- Pivot, X.; Bondarenko, I.; Nowecki, Z.; Dvorkin, M.; Trishkina, E.; Ahn, J.H.; Im, S.A.; Sarosiek, T.; Chatterjee, S.; Wojtukiewicz, M.Z.; et al. A phase III study comparing SB3 (a proposed trastuzumab biosimilar) and trastuzumab reference product in HER2-positive early breast cancer treated with neoadjuvant-adjuvant treatment: Final safety, immunogenicity and survival results. Eur. J. Cancer 2018, 93, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.J.; Kim, J.H.; Ahn, S.G.; Jeung, H.C.; Sohn, J.; Kim, G.M.; Kim, M.H.; Kim, S.I.; Park, S.; Park, H.S.; et al. Real-World Clinical Outcomes of Biosimilar Trastuzumab (CT-P6) in HER2-Positive Early-Stage and Metastatic Breast Cancer. Front. Oncol. 2021, 11, 689587. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [PubMed]
- Pivot, X.; Cortés, J.; Lüftner, D.; Lyman, G.H.; Curigliano, G.; Bondarenko, I.M.; Ahn, J.-H.; Im, S.-A.; Litwiniuk, M.; Shparyk, Y.V.; et al. Cardiac Safety and Efficacy of SB3 Trastuzumab Biosimilar for ERBB2-Positive Early Breast Cancer: Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e235822. [Google Scholar] [CrossRef] [PubMed]
- Beca, J.; Dai, W.; Pataky, R.; Tran, D.; Dvorani, E.; Isaranuwatchai, W.; Peacock, S.; Alvi, R.; Cheung, W.; Earle, C.; et al. Real-world Safety of Bevacizumab with First-line Combination Chemotherapy in Patients with Metastatic Colorectal Cancer: Population-based Retrospective Cohort Studies in Three Canadian Provinces. Clin. Oncol. (R. Coll. Radiol.) 2022, 34, e7–e17. [Google Scholar] [CrossRef]
- Eskander, A.; Li, Q.; Yu, J.; Hallet, J.; Coburn, N.; Dare, A.; Chan, K.K.W.; Singh, S.; Parmar, A.; Earle, C.C.; et al. Assessing the Impact of the COVID-19 Pandemic on Emergency Department Use for Patients Undergoing Cancer-Directed Surgeries. Curr. Oncol. 2022, 29, 1877–1889. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Crude Cohort | PSM Cohort | ||||||
|---|---|---|---|---|---|---|---|
| Herceptin | Biosimilar Trastuzumab | p-Value | Herceptin | Biosimilar Trastuzumab | Standardized Difference | ||
| N = 3511 | N = 1560 | N = 2304 | N = 1152 | ||||
| Age at index, years | Mean ± SD | 57.5 ± 12.3 | 57.9 ± 12.7 | 0.24 | 57.6 ± 11.9 | 57.2 ± 11.9 | 0.04 |
| Sex, n (%) | Female | 3495 (99.5) | 1554 (99.6) | 0.82 | 2304 (100.0) | 1152 (100.0) | 0 |
| Rurality, n (%) | Rural | 403 (11.5) | 157 (10.1) | 0.09 | 239 (10.4) | 118 (10.2) | 0 |
| Urban | 3082 (87.8) | 1384 (88.7) | 2065 (89.6) | 1034 (89.8) | |||
| Unknown | 26 (0.7) | 19 (1.2) | 0 (0) | 0 (0) | |||
| Local Health Integration Networks, n (%) | Central | 446 (12.7) | 223 (14.5) | 0.04 | 324 (14.1) | 163 (14.2) | <0.01 |
| Central East | 419 (11.9) | 152 (9.7) | 124 (5.4) | 49 (4.3) | |||
| Central West | 189 (5.4) | 70 (4.5) | 194 (8.4) | 99 (8.6) | |||
| Champlain | 380 (10.8) | 147 (9.4) | 69 (3.0) | 31 (2.7) | |||
| Erie St. Clair | 187 (5.3) | 92 (5.9) | 123 (5.3) | 65 (5.6) | |||
| Hamilton Niagara Haldimand Brant | 407 (11.6) | 159 (10.2) | 204 (8.9) | 123 (10.7) | |||
| Mississauga Halton | 267 (7.6) | 121 (7.8) | 249 (10.8) | 131 (11.4) | |||
| North East | 157 (4.5) | 64 (4.1) | 115 (5) | 54 (4.7) | |||
| North Simcoe Muskoka | 105 (3.0) | 38 (2.4) | 197 (8.6) | 97 (8.4) | |||
| North West | 44 (1.3) | 21 (1.4) | 286 (12.4) | 128 (11.1) | |||
| South East | 137 (3.9) | 68 (4.4) | 85 (3.7) | 56 (4.3) | |||
| South West | 307 (8.7) | 169 (10.8) | 195 (8.5) | 95 (8.3) | |||
| Toronto Central | 271 (7.7) | 131 (8.4) | 31 (1.4) | 12 (1.0) | |||
| Waterloo Wellington | 169 (4.8) | 86 (5.5) | 108 (4.7) | 49 (4.3) | |||
| Days from Dx date to index | Mean ± SD | 116.7 ± 44.8 | 101.0 ± 44.7 | <0.01 | 108.7 ± 38.3 | 104.8 ± 39.0 | 0.08 |
| Ontario Marginalization Index score quintiles, n (%) | 1 (lowest | 827 (23.6) | 399 (25.6) | 0.14 | 557 (21.2) | 290 (25.1) | 0 |
| 2 | 423 (12.1) | 211 (13.5) | 302 (13.1) | 151 (13.1) | |||
| 3 | 774 (22.1) | 328 (21.0) | 533 (23.1) | 250 (21.7) | |||
| 4 | 630 (17.9) | 281 (18.0) | 393 (17.1) | 221 (19.2) | |||
| 5 (highest) | 808 (23.0) | 316 (20.3) | 519 (22.5) | 240 (20.8) | |||
| Missing | 49 (1.4) | 25 (1.6) | 0 (0) | 0 (0) | |||
| Stage, n (%) | I | 1397 (39.8) | 794 (50.9) | <0.01 | 1144 (49.7) | 572 (49.7) | 0 |
| II | 1491 (42.5) | 558 (35.8) | 858 (37.2) | 429 (37.2) | |||
| III | 623 (17.7) | 208 (13.3) | 302 (13.1) | 151 (13.1) | |||
| Estrogen–progesterone receptor status, n (%) | Positive | 2453 (69.9) | 945 (60.6) | <0.01 | 1538 (66.7) | 769 (66.7) | 0 |
| Both negative/ indeterminate | 1058 (30.1) | 615 (39.4) | 766 (33.3) | 383 (33.3) | |||
| Charlson Comorbidity Index score, n (%) | No hospitalization | NR * | NR * | 0.08 | 0 (0) | 0 (0) | <0.01 |
| 0 | 3034 (86.4) | 1375 (88.1) | 2031 (88.2) | 1025 (88.9) | |||
| 1 | 374 (10.7) | 155 (9.9) | 225 (9.8) | 110 (9.6) | |||
| 2+ | 103 (2.9) | 30 (1.9) | 48 (2.1) | 17 (1.5) | |||
| History of prior breast cancer, n (%) | Yes | 161 (4.6) | 76 (4.9) | 0.05 | 92 (4.0) | 51 (4.4) | 0.02 |
| History of prior non-breast cancer, n (%) | Yes | 304 (8.7) | 147 (9.4) | 0.03 | 210 (9.1) | 102 (8.9) | <0.01 |
| CHF within 3 years prior to index date, n (%) | Yes | 30 (0.9) | 17 (1.1) | 0.09 | 16 (0.7) | 8 (0.7) | 0 |
| Receipt of trastuzumab with respect to breast resection date, n (%) | Neoadjuvant | 1152 (32.8) | 751 (48.1) | <0.01 | 857 (37.2) | 487 (42.3) | 0 |
| Adjuvant | 2359 (67.2) | 809 (51.9) | 1447 (62.8) | 665 (57.7) | |||
| Receipt of systemic chemotherapy with respect to breast resection date, n (%) | Neoadjuvant | 1183 (33.7) | 769 (49.3) | <0.01 | 865 (37.5) | 496 (43.1) | 0 |
| Adjuvant | 2328 (66.3) | 791 (50.7) | 1439 (62.5) | 656 (56.9) | |||
| History of RT to breast tissue for prior breast cancer, n (%) | Yes | 87 (2.5) | 52 (3.3) | 0.02 | 53 (2.3) | 34 (2.9) | 0.04 |
| RT to breast tissue between index and 1 year after breast cancer Dx, n (%) | Yes | 1876 (53.4) | 787 (50.5) | <0.01 | 1249 (54.2) | 622 (54.0) | <0.01 |
| Systemic chemotherapy regimen, n (%) | Anthracycline-based only | 62 (1.8) | 8 (0.5) | <0.01 | 8 (0.4) | NR * | 0 |
| Anthracycline taxane | 2198 (62.6) | 867 (55.6) | 1502 (65.2) | 755 (65.6) | |||
| Platinum taxane | 295 (8.4) | 235 (15.1) | 186 (8.1) | 93 (8.1) | |||
| 1st-generation CMF | 14 (0.4) | NR * | 0 (0) | 0 (0) | |||
| 2nd-generation taxane | 371 (10.6) | 125 (8.0) | 182 (7.9) | 91 (7.9) | |||
| APT | 571 (16.3) | 325 (20.8) | 426 (18.5) | 213 (18.5) | |||
| Crude Cohort | PSM-Adjusted Cohort | ||||||
|---|---|---|---|---|---|---|---|
| Herceptin | Biosimilar Trastuzumab | p-Value | Herceptin | Biosimilar Trastuzumab | p-Value | ||
| N = 3511 | N = 1560 | N = 2304 | N = 1152 | ||||
| Treatment-related death | n (%) | NR * | NR * | 0.43 | 0 (0) | NR * | 0.33 |
| OR (95% CI) | 0.44 (0.03–7.11) | 0.57 | - | - | |||
| Direct hospital admission | n (%) | 965 (27.5) | 360 (23.0) | <0.01 | 647 (28.1) | 263 (22.8) | <0.01 |
| RR (95% CI) | 0.92 (0.82–1.04) | 0.21 | 0.85 (0.74–0.98) | 0.03 | |||
| ED visit leading to hospitalization | n (%) | 428 (12.2) | 168 (10.8) | 0.15 | 266 (11.6) | 121 (10.5) | 0.36 |
| RR (95% CI) | 0.99 (0.82–1.21) | 0.98 | 0.96 (0.77–1.20) | 0.72 | |||
| Crude Cohort | PSM-Adjusted Cohort | ||||||
|---|---|---|---|---|---|---|---|
| Herceptin | Biosimilar Trastuzumab | p-Value | Herceptin | Biosimilar Trastuzumab | p-Value | ||
| N = 3488 | N = 1539 | N = 2294 | N = 1137 | ||||
| In-patient hospital admission for CHF | n (%) | 27 (0.77) | 15 (0.97) | 0.50 | 18 (0.78) | 10 (0.88) | 0.77 |
| OR (95% CI) | 1.26 (0.67–2.38) | 0.47 | 1.12 (0.52–2.44) | 0.77 | |||
| Crude Cohort | PSM-Adjusted Cohort | ||||||
|---|---|---|---|---|---|---|---|
| Herceptin | Biosimilar Trastuzumab | p-Value | Herceptin | Biosimilar Trastuzumab | p-Value | ||
| N = 2792 | N = 1013 | N = 1588 | N = 794 | ||||
| Early treatment discontinuation | n (%) | 694 (24.9) | 252 (24.9) | 0.99 | 396 (24.9) | 185 (23.3) | 0.38 |
| OR (95% CI) | 0.99 (0.85–1.18) | 0.99 | 0.91 (0.75–1.12) | 0.38 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz, C.; Tai, X.; Arias, J.; Eisen, A.; Chaudhry, M.; Gavura, S.; Chan, K.K.W. Comparative Effectiveness and Safety of Trastuzumab Biosimilars to Herceptin for Adjuvant Treatment of HER2+ Breast Cancer. Curr. Oncol. 2024, 31, 1633-1644. https://doi.org/10.3390/curroncol31030124
Muñoz C, Tai X, Arias J, Eisen A, Chaudhry M, Gavura S, Chan KKW. Comparative Effectiveness and Safety of Trastuzumab Biosimilars to Herceptin for Adjuvant Treatment of HER2+ Breast Cancer. Current Oncology. 2024; 31(3):1633-1644. https://doi.org/10.3390/curroncol31030124
Chicago/Turabian StyleMuñoz, Caroline, Xiaochen Tai, Jessica Arias, Andrea Eisen, Munaza Chaudhry, Scott Gavura, and Kelvin K. W. Chan. 2024. "Comparative Effectiveness and Safety of Trastuzumab Biosimilars to Herceptin for Adjuvant Treatment of HER2+ Breast Cancer" Current Oncology 31, no. 3: 1633-1644. https://doi.org/10.3390/curroncol31030124