Real-World Evidence of the Impact of the COVID-19 Pandemic on Lung Cancer Survival: Canadian Perspective

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
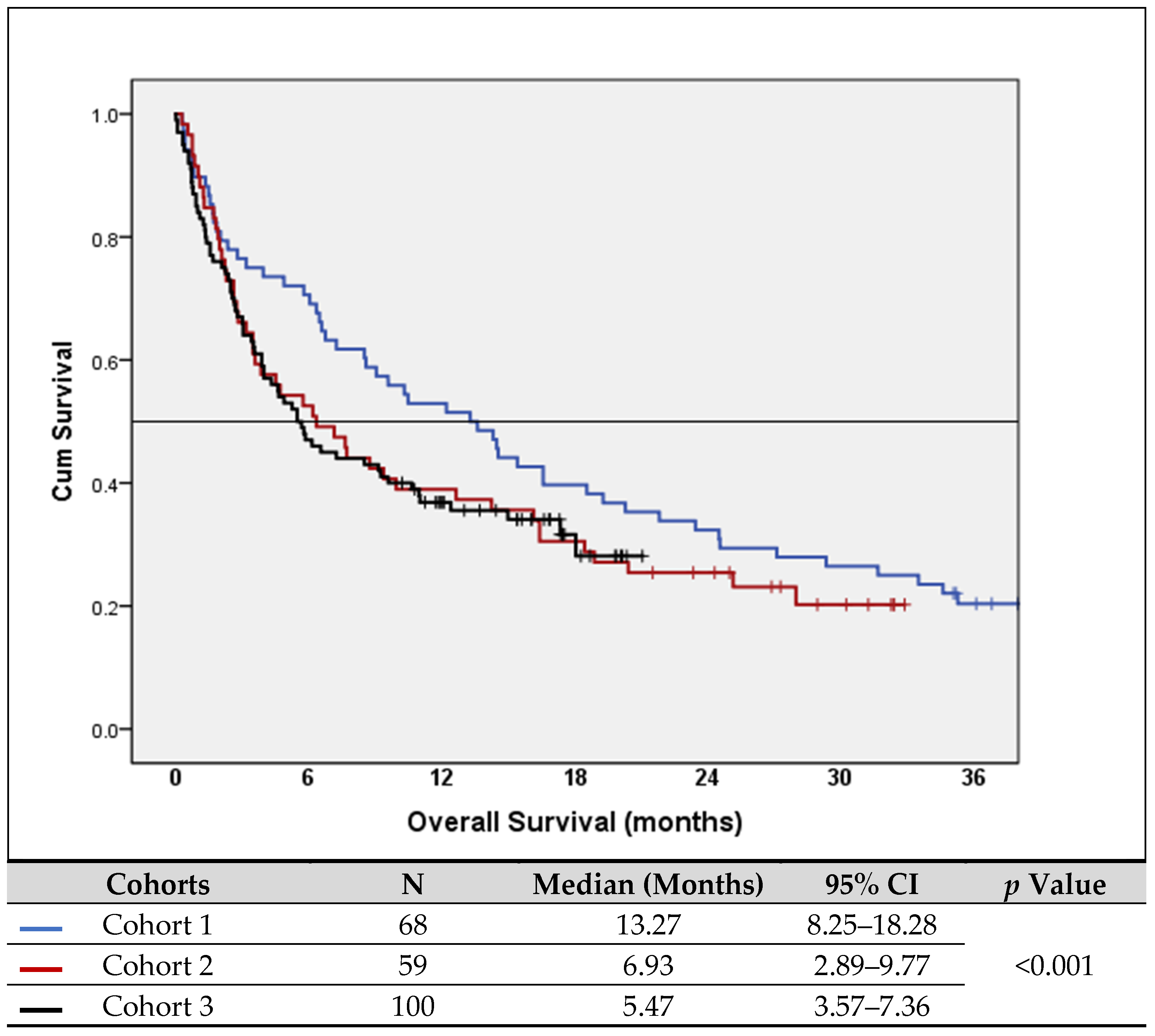
- Cohort #1 (2019): Pre-COVID-19
- Cohort #2 (2020): 1st year of COVID-19
- Cohort #3 (2021): 2nd year of COVID-19
2.2. Objectives
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Front-Line Treatment
3.3. Lung Cancer Mortality and Survival
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Caminha, I.; Tavora, F.; Sousa, J.; Martins Neto, F.; Cavalcanti, L.P.G. Impact of the COVID-19 pandemic on the diagnosis of lung cancer in northeastern Brazil. J. Bras. Pneumol. 2022, 48, e20220248. [Google Scholar] [CrossRef] [PubMed]
- Flores, R.; Alpert, N.; McCardle, K.; Taioli, E. Shift in lung cancer stage at diagnosis during the COVID-19 pandemic in New York City. Transl. Lung Cancer Res. 2022, 11, 1514–1516. [Google Scholar] [CrossRef] [PubMed]
- Fox, L.; Monroy-Iglesias, M.J.; Aggarwal, A.; Haire, K.; Purushotham, A.; Spicer, J.; Papa, S.; Rigg, A.; Dolly, S.; Sullivan, R.; et al. Association between COVID-19 burden and delays to diagnosis and treatment of cancer patients in England. J. Cancer Policy 2022, 31, 100316. [Google Scholar] [CrossRef] [PubMed]
- Gurney, J.K.; Dunn, A.; Liu, M.; Mako, M.; Millar, E.; Ruka, M.; Crengle, S.; Dawkins, P.; Jackson, C.; Laking, G.; et al. The impact of COVID-19 on lung cancer detection, diagnosis and treatment for Maori in Aotearoa New Zealand. N. Z. Med. J. 2022, 135, 23–43. [Google Scholar]
- Horita, N. Impact of the COVID-19 pandemic on cancer diagnosis and resection in a COVID-19 low-burden country: Nationwide registration study in Japan. Eur. J. Cancer 2022, 165, 113–115. [Google Scholar] [CrossRef] [PubMed]
- Johansson, A.L.V.; Laronningen, S.; Skovlund, C.W.; Kristiansen, M.F.; Morch, L.S.; Friis, S.; Johannesen, T.B.; Myklebust, T.A.; Skog, A.; Pettersson, D.; et al. The impact of the COVID-19 pandemic on cancer diagnosis based on pathology notifications: A comparison across the Nordic countries during 2020. Int. J. Cancer 2022, 151, 381–395. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Zhao, W.; Li, S.; Chen, L.; Zhou, C. Current status of diagnosis and treatment of advanced non-small cell lung cancer in China during the COVID-19 pandemic. Ann. Palliat. Med. 2022, 11, 1231–1240. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, C.M.; Correa, F.M.; Migowski, A. Short-term effects of the COVID-19 pandemic on cancer screening, diagnosis and treatment procedures in Brazil: A descriptive study, 2019–2020. Epidemiol. Serv. Saude. 2022, 31, e2021405. [Google Scholar] [CrossRef]
- Skovlund, C.W.; Friis, S.; Christensen, J.; Nilbert, M.C.; Morch, L.S. Drop in cancer diagnosis during the COVID-19 pandemic in Denmark: Assessment of impact during 2020. Acta Oncol. 2022, 61, 658–661. [Google Scholar] [CrossRef]
- Valvi, N.; Patel, H.; Bakoyannis, G.; Haggstrom, D.A.; Mohanty, S.; Dixon, B.E. COVID-19 Diagnosis and Risk of Death Among Adults With Cancer in Indiana: Retrospective Cohort Study. JMIR Cancer 2022, 8, e35310. [Google Scholar] [CrossRef]
- Wasim, U.; Tahir, M.J.; Siddiqi, A.R.; Jabbar, A.; Ullah, I. The impact of the COVID-19 pandemic on impending cancer deaths due to delays in diagnosis in the UK. J. Med. Virol. 2022, 94, 20–21. [Google Scholar] [CrossRef] [PubMed]
- Kasymjanova, G.; Anwar, A.; Cohen, V.; Sultanem, K.; Pepe, C.; Sakr, L.; Friedmann, J.; Agulnik, J.S. The Impact of COVID-19 on the Diagnosis and Treatment of Lung Cancer at a Canadian Academic Center: A Retrospective Chart Review. Curr. Oncol. 2021, 28, 4247–4255. [Google Scholar] [CrossRef]
- Kasymjanova, G.; Rizzolo, A.; Pepe, C.; Friedmann, J.E.; Small, D.; Spicer, J.; Lecavalier-Barsoum, M.; Sultanem, K.; Wang, H.; Spatz, A.; et al. The Impact of COVID-19 on the Diagnosis and Treatment of Lung Cancer over a 2-Year Period at a Canadian Academic Center. Curr. Oncol. 2022, 29, 8677–8685. [Google Scholar] [CrossRef] [PubMed]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]
- Cattaruzza, M.S.; Gorini, G. COVID-19 and the role of smoking: The protocol of the multicentric prospective study COSMO-IT (COvid19 and SMOking in ITaly). Acta Biomed. 2020, 91, e2020062. [Google Scholar] [CrossRef]
- Mangone, L.; Mrinelli, L.; Bisceglia, I.; Pinta, C. The incidence of cancer at the time of COVID-19 in Northern Italy. Ann. Res. Oncol. 2022, 2, 105–115. [Google Scholar] [CrossRef]
- Orelaru, F.; Edwards, M.; Raleigh, R.; Abunayla, A.; Bush, R.; Porter, S.; Schumaker, K.; Albright, J.; Adams, K.N. Short-Term Outcomes of COVID-19 Pandemic on Non-Small Cell Lung Cancer Screening and Management. Surg. J. 2023, 9, e156–e161. [Google Scholar] [CrossRef]
- Garassino, M.C.; Whisenant, J.G.; Huang, L.C.; Trama, A.; Torri, V.; Agustoni, F.; Baena, J.; Banna, G.; Berardi, R.; Bettini, A.C.; et al. COVID-19 in patients with thoracic malignancies (TERAVOLT): First results of an international, registry-based, cohort study. Lancet Oncol. 2020, 21, 914–922. [Google Scholar] [CrossRef]
- Alagoz, O.; Lowry, K.P.; Kurian, A.W.; Mandelblatt, J.S.; Ergun, M.A.; Huang, H.; Lee, S.J.; Schechter, C.B.; Tosteson, A.N.A.; Miglioretti, D.L.; et al. Impact of the COVID-19 Pandemic on Breast Cancer Mortality in the US: Estimates From Collaborative Simulation Modeling. J. Natl. Cancer Inst. 2021, 113, 1484–1494. [Google Scholar] [CrossRef]
- Hartman, H.E.; Sun, Y.; Devasia, T.P.; Chase, E.C.; Jairath, N.K.; Dess, R.T.; Jackson, W.C.; Morris, E.; Li, P.; Hochstedler, K.A.; et al. Integrated Survival Estimates for Cancer Treatment Delay Among Adults With Cancer During the COVID-19 Pandemic. JAMA Oncol. 2020, 6, 1881–1889. [Google Scholar] [CrossRef]
- Sud, A.; Jones, M.E.; Broggio, J.; Loveday, C.; Torr, B.; Garrett, A.; Nicol, D.L.; Jhanji, S.; Boyce, S.A.; Gronthoud, F.; et al. Collateral damage: The impact on outcomes from cancer surgery of the COVID-19 pandemic. Ann. Oncol. 2020, 31, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Reyes, R.; López-Castro, R.; Auclin, E.; García, T.; Chourio, M.J.; Rodriguez, A.; López, L.; Laguna, J.C.; Lucena, C.; Molins, L.; et al. Impact of COVID-19 Pandemic in the Diagnosis and Prognosis of Lung Cancer. J. Thorac. Oncol. 2021, 16, S141. [Google Scholar] [CrossRef]


{kind=link}
| Study Cohorts | Included in the Study | Second Opinion (Excluded) | Total | p Value |
|---|---|---|---|---|
| Cohort 1 (2019) | 130 | 40 | 170 | 0.004 |
| Cohort 2 (2020) | 103 | 8 | 111 | |
| Cohort 3 (2021) | 184 | 35 | 219 | |
| Total | 417 | 83 | 500 |
| Characteristics | 2019 n = 130 | 2020 n = 103 | 2021 n = 184 | ||
|---|---|---|---|---|---|
| Age (mean; range) | 70 (40–96) | 71 (42–92) | 71 (41–92) | 0.991 | |
| Sex n (%) | Male | 73 (56) | 56 (54) | 88 (48) | 0.145 |
| Female | 57 (44) | 47 (46) | 96 (52) | ||
| Smoking n (%) | Former/current | 99 (76) | 74 (74) | 156 (85) | 0.054 |
| Non-smoker | 31 (24) | 29 (26) | 28 (15) | ||
| ECOG PS n (%) | 0–1 | 106 (82) | 84 (82) | 148 (80) | 0.960 |
| >1 | 24 (18) | 19 (18) | 36 (20) | ||
| Stage | Early 1 | 42 (32) | 33(32) | 55 (30) | 0.787 |
| Locoregional 2 | 20 (15) | 11 (11) | 29 (16) | ||
| Advanced/Metastatic 3 | 68 (52) | 59 (57) | 100 (54) |
| M Status | Cohort 1 n = 68 | Cohort 2 n = 59 | Cohort 3 n = 100 |
|---|---|---|---|
| M1a 1 n (%) | 20 (29) | 14 (24) | 31 (31) |
| M1b 2 n (%) | 27 (40) | 11 (19) | 18 (18) |
| M1c 3 n (%) | 21 (31) | 34 (57) | 51 (51) |
| The two-tailed p value (2020 vs. 2019) | 0.002 | ||
| The two-tailed p value (2021 vs. 2019) | 0.013 | ||
| Type of FTD | Cohort 1 n = 110 | Cohort 2 n = 84 | Cohort 3 n = 151 | p-Value | |
|---|---|---|---|---|---|
| Surgery (n/%) | 42 (38) | 24 (29) | 54 (36) | 0.01 | |
| Radiosurgery (n/%) | 8 (7) | 20 (24) | 12 (8) | 0.009 | |
| CTX 2 (n/%) | Total | 60 (54) | 40 (47) | 85 (56) | >0.05 |
| SOC 1 | 20 (33) | 12 (30) | 25 (29) | ||
| IO ± CTX 3 | 23 (38) | 16 (40) | 37 (44) | ||
| Targeted CTX | 17 (29) | 12 (30) | 23 (27) | ||
| Stage | Cohort | n | Died at 6 Months n (%) | p Value |
|---|---|---|---|---|
| Early stage 1 | 1 (2019) | 42 | 1 (2) | |
| 2 (2020) | 33 | 3 (9) | >0.05 | |
| 3 (2021) | 55 | 0 (0) | ||
| Locoregional 2 | 1 (2019) | 20 | 3 (15) | 0.407 |
| 2 (2020) | 11 | 3 (27) | ||
| 3 (2021) | 29 | 4 (14) | ||
| Advanced/metastatic stage 3 | 1 (2019) | 68 | 20 (29) | 0.004 |
| 2 (2020) | 59 | 28 (47) | ||
| 3 (2021) | 100 | 53 (53) |
| Model #1 Description | Variables Included in the Model | Reference | Exp(B) | 95% CI | p Value |
| All subjects | Year of diagnosis | 2019 | 1.098 | 0.926–1.302 | 0.284 |
| Age | ≤65 | 1.024 | 1.021–1.269 | 0.005 | |
| Events = 199 | Sex | Female | 1.106 | 0.824–1.485 | 0.502 |
| Censored = 218 | ECOG PS | 0–1 | 2.360 | 1.721–3.237 | <0.001 |
| Missing = 0 | Smoking | Smoker | 0.729 | 0.598–0.897 | 0.002 |
| Total = 417 | Stage | 1–3A | 3.438 | 2.663–4.438 | <0.001 |
| Model #2 Description | Variables Included in the Model | Exp(B) | 95% CI | p Value | |
| Advanced/metastatic stage | Year of diagnosis | 2019 | 1.156 | 1.021–1.393 | 0.042 |
| Age | ≤65 | 1.035 | 1.018–1053 | <0.001 | |
| Events = 167 | Sex | Female | 1.108 | 0.803–1.530 | 0.532 |
| Censored = 60 | ECOG PS | 0–1 | 2.483 | 1.780–3.463 | <0.001 |
| Total = 227 | Smoking | Smoker | 0.723 | 0.584–0.894 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agulnik, J.; Kasymjanova, G.; Pepe, C.; Friedmann, J.; Small, D.; Sakr, L.; Wang, H.; Spatz, A.; Sultanem, K.; Cohen, V. Real-World Evidence of the Impact of the COVID-19 Pandemic on Lung Cancer Survival: Canadian Perspective. Curr. Oncol. 2024, 31, 1562-1571. https://doi.org/10.3390/curroncol31030119
Agulnik J, Kasymjanova G, Pepe C, Friedmann J, Small D, Sakr L, Wang H, Spatz A, Sultanem K, Cohen V. Real-World Evidence of the Impact of the COVID-19 Pandemic on Lung Cancer Survival: Canadian Perspective. Current Oncology. 2024; 31(3):1562-1571. https://doi.org/10.3390/curroncol31030119
Chicago/Turabian StyleAgulnik, Jason, Goulnar Kasymjanova, Carmela Pepe, Jennifer Friedmann, David Small, Lama Sakr, Hangjun Wang, Alan Spatz, Khalil Sultanem, and Victor Cohen. 2024. "Real-World Evidence of the Impact of the COVID-19 Pandemic on Lung Cancer Survival: Canadian Perspective" Current Oncology 31, no. 3: 1562-1571. https://doi.org/10.3390/curroncol31030119