The Establishment and Verification of a Nomogram Model for Predicting the Overall Survival of Medullary Thyroid Carcinoma: An Analysis Based on the SEER Database


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Selection from the SEER Database
2.2. Data Selection from Our Medical Center
2.3. Statistical Analyses
3. Results
3.1. Clinical and Pathological Characteristics of Patients
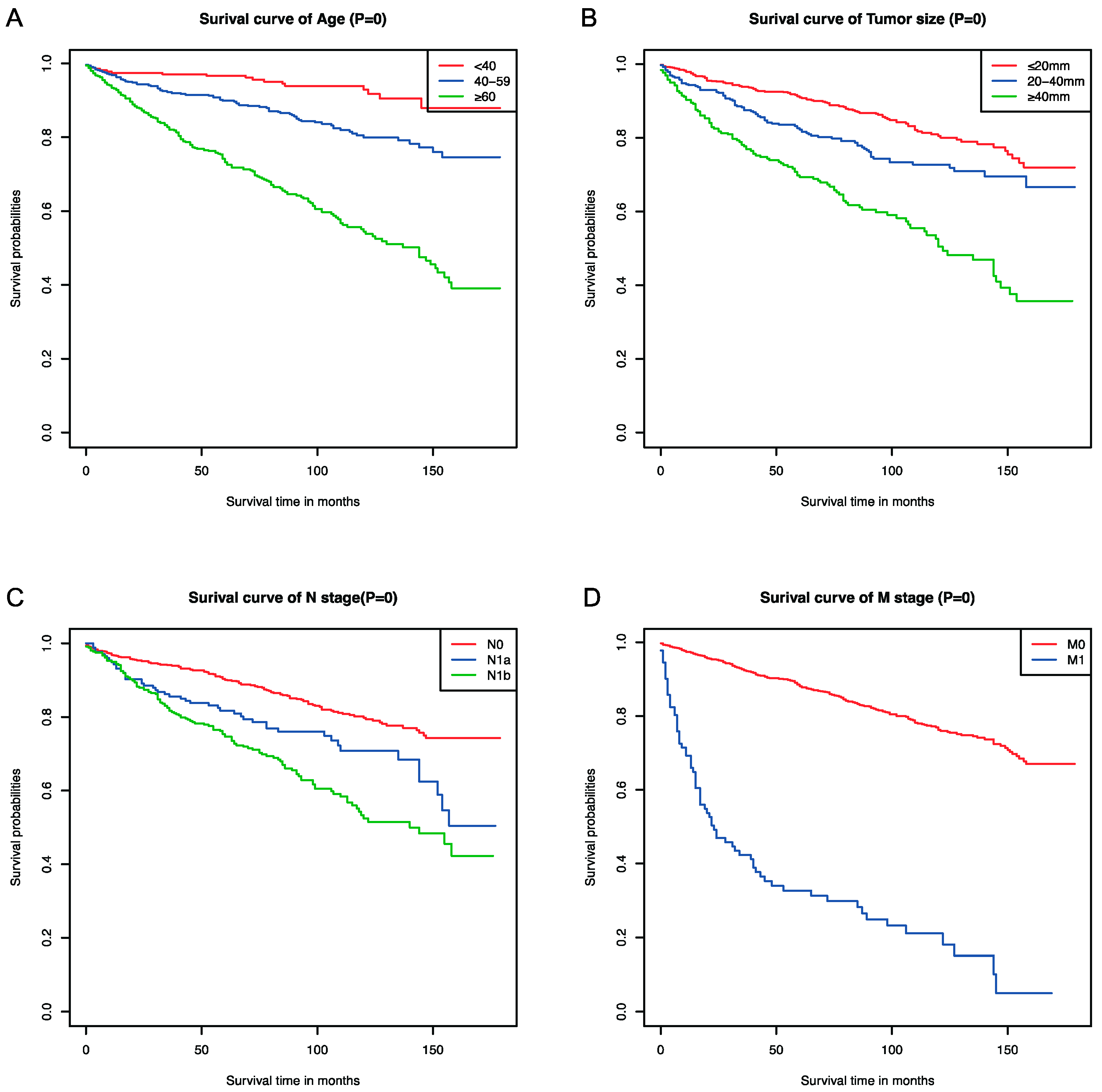
3.2. Selection of Independent Factors for the OS and K-M Curves
3.3. Nomogram Development and Validation for the Prediction of the Overall Survival of MTC Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Carling, T.; Udelsman, R. Thyroid cancer. Annu. Rev. Med. 2014, 65, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, C.M.; Sosa, J.A. The changing incidence of thyroid cancer. Nat. Rev. Endocrinol. 2016, 12, 646–653. [Google Scholar] [CrossRef] [PubMed]
- Jaber, T.; Dadu, R.; Hu, M.I. Medullary thyroid carcinoma. Curr. Opin. Endocrinol. Diabetes Obes. 2021, 28, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Angelousi, A.; Hayes, A.R.; Chatzellis, E.; Kaltsas, G.A.; Grossman, A.B. Metastatic medullary thyroid carcinoma: A new way forward. Endocr. Relat. Cancer 2022, 29, R85–R103. [Google Scholar] [CrossRef]
- Pacini, F.; Castagna, M.G.; Cipri, C.; Schlumberger, M. Medullary thyroid carcinoma. Clin. Oncol. 2010, 22, 475–485. [Google Scholar] [CrossRef]
- Rendl, G.; Manzl, M.; Hitzl, W.; Sungler, P.; Pirich, C. Long-term prognosis of medullary thyroid carcinoma. Clin. Endocrinol. 2008, 69, 497–505. [Google Scholar] [CrossRef]
- Lodish, M.B.; Stratakis, C.A. RET oncogene in MEN2, MEN2B, MTC and other forms of thyroid cancer. Expert Rev. Anticanc. 2008, 8, 625–632. [Google Scholar] [CrossRef]
- de Groot, J.W.B.; Links, T.P.; Plukker, J.T.M.; Lips, C.J.M.; Hofstra, R.M.W. as a diagnostic and therapeutic target in sporadic and hereditary endocrine tumors. Endocr. Rev. 2006, 27, 535–560. [Google Scholar] [CrossRef]
- Elisei, R.; Cosci, B.; Romei, C.; Bottici, V.; Renzini, G.; Molinaro, E.; Agate, L.; Vivaldi, A.; Faviana, P.; Basolo, F.; et al. Prognostic significance of somatic oncogene mutations in sporadic medullary thyroid cancer: A 10-year follow-up study. J. Clin. Endocr. Metab. 2008, 93, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Lairmore, T.C.; Wells, S.A., Jr. Medullary carcinoma of the thyroid: Current diagnosis and management. Semin. Surg. Oncol. 1991, 7, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.I.; Ying, A.K.; Jimenez, C. Update on medullary thyroid cancer. Endocrinol. Metab. Clin. N. Am. 2014, 43, 423–442. [Google Scholar] [CrossRef] [PubMed]
- Zarkesh, M.; Arab, N.; Tavangar, S.M.; Nozhat, Z.; Fanaei, S.M.; Hedayati, M. Utilizing the circulating tumor markers in diagnosis and management of medullary thyroid cancer. Pathol. Res. Pract. 2022, 229, 153694. [Google Scholar] [CrossRef] [PubMed]
- Nigam, A.; Xu, B.; Spanheimer, P.M.; Ganly, I.; Tuttle, R.M.; Wong, R.J.; Shaha, A.R.; Ghossein, R.A.; Untch, B.R. Tumor Grade Predicts for Calcitonin Doubling Times and Disease-Specific Outcomes after Resection of Medullary Thyroid Carcinoma. Thyroid 2022, 32, 1193–1200. [Google Scholar] [CrossRef] [PubMed]
- van Veelen, W.; de Groot, J.W.; Acton, D.S.; Hofstra, R.M.; Hoppener, J.W.; Links, T.P.; Lips, C.J. Medullary thyroid carcinoma and biomarkers: Past, present and future. J. Intern. Med. 2009, 266, 126–140. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Wu, L.; Jiang, M.; Li, D.; Jiang, T.; Hong, Z.; Wang, F.; Li, S. Clinical Nomogram for Predicting Survival Outcomes in Early Mucinous Breast Cancer. PLoS ONE 2016, 11, e0164921. [Google Scholar] [CrossRef]
- Roman, S.; Lin, R.; Sosa, J.A. Prognosis of medullary thyroid carcinoma: Demographic, clinical, and pathologic predictors of survival in 1252 cases. Cancer 2006, 107, 2134–2142. [Google Scholar] [CrossRef]
- Chen, L.; Wang, Y.; Zhao, K.; Wang, Y.; He, X. Postoperative Nomogram for Predicting Cancer-Specific and Overall Survival among Patients with Medullary Thyroid Cancer. Int. J. Endocrinol. 2020, 2020, 8888677. [Google Scholar] [CrossRef]
- Dottorini, M.E.; Assi, A.; Sironi, M.; Sangalli, G.; Spreafico, G.; Colombo, L. Multivariate analysis of patients with medullary thyroid carcinoma. Prognostic significance and impact on treatment of clinical and pathologic variables. Cancer 1996, 77, 1556–1565. [Google Scholar] [CrossRef]
- Frank-Raue, K.; Rondot, S.; Raue, F. Molecular genetics and phenomics of mutations: Impact on prognosis of MTC. Mol. Cell Endocrinol. 2010, 322, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Eng, C.; Clayton, D.; Schuffenecker, I.; Lenoir, G.; Cote, G.; Gagel, R.F.; vanAmstel, H.K.P.; Lips, C.J.M.; Nishisho, I.; Takai, S.I.; et al. The relationship between specific RET proto-oncogene mutations and disease phenotype in multiple endocrine neoplasia type 2—International RET mutation consortium analysis. JAMA 1996, 276, 1575–1579. [Google Scholar] [CrossRef]
- Wirth, L.J.; Sherman, E.; Robinson, B.; Solomon, B.; Kang, H.; Lorch, J.; Worden, F.; Brose, M.; Patel, J.; Leboulleux, S.; et al. Efficacy of Selpercatinib in RET-Altered Thyroid Cancers. N. Engl. J. Med. 2020, 383, 825–835. [Google Scholar] [CrossRef] [PubMed]
- Klein Hesselink, E.N.; Steenvoorden, D.; Kapiteijn, E.; Corssmit, E.P.; van der Horst-Schrivers, A.N.; Lefrandt, J.D.; Links, T.P.; Dekkers, O.M. Therapy of endocrine disease: Response and toxicity of small-molecule tyrosine kinase inhibitors in patients with thyroid carcinoma: A systematic review and meta-analysis. Eur. J. Endocrinol. 2015, 172, R215–R225. [Google Scholar] [CrossRef]
- Vodopivec, D.M.; Hu, M.I. RET kinase inhibitors for RET-altered thyroid cancers. Ther. Adv. Med. Oncol. 2022, 14, 17588359221101691. [Google Scholar] [CrossRef] [PubMed]
- Subbiah, V.; Velcheti, V.; Tuch, B.B.; Ebata, K.; Busaidy, N.L.; Cabanillas, M.E.; Wirth, L.J.; Stock, S.; Smith, S.; Lauriault, V.; et al. Selective RET kinase inhibition for patients with RET-altered cancers. Ann. Oncol. 2018, 29, 1869–1876. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Bradford, D.; Larkins, E.; Pai-Scherf, L.H.; Chatterjee, S.; Mishra-Kalyani, P.S.; Wearne, E.; Helms, W.S.; Ayyoub, A.; Bi, Y.; et al. FDA Approval Summary: Pralsetinib for the Treatment of Lung and Thyroid Cancers With RET Gene Mutations or Fusions. Clin. Cancer Res. 2021, 27, 5452–5456. [Google Scholar] [CrossRef]
- Wirth, L.J.; Brose, M.S.; Elisei, R.; Capdevila, J.; Hoff, A.O.; Hu, M.I.; Tahara, M.; Robinson, B.; Gao, M.; Xia, M.; et al. LIBRETTO-531: A phase III study of selpercatinib in multikinase inhibitor-naive RET-mutant medullary thyroid cancer. Future Oncol. 2022, 18, 3143–3150. [Google Scholar] [CrossRef]
- Choi, J.B.; Lee, S.G.; Kim, M.J.; Kim, T.H.; Ban, E.J.; Lee, C.R.; Lee, J.; Kang, S.W.; Jeong, J.J.; Nam, K.H.; et al. Dynamic risk stratification in medullary thyroid carcinoma: Single institution experiences. Medicine 2018, 97, e9686. [Google Scholar] [CrossRef]
- Jin, L.; Zhang, X.; Ni, S.; Yan, D.; Wang, M.; Li, Z.; Liu, S.; An, C. A nomogram to predict lateral lymph node metastases in lateral neck in patients with medullary thyroid cancer. Front. Endocrinol. 2022, 13, 902546. [Google Scholar] [CrossRef]
- Jiang, T.; Huang, C.; Xu, Y.; Su, Y.; Zhang, G.; Xie, L.; Huang, L.; You, S.; Zha, J. Ratio of positive lymph nodes: The prognostic value in stage IV thyroid cancer. Oncotarget 2017, 8, 79462–79468. [Google Scholar] [CrossRef] [PubMed]
- Santarpia, L.; Gagel, R.F.; Sherman, S.I.; Sarlis, N.J.; Evans, D.B.; Hoff, A.O. Diabetes insipidus and panhypopituitarism due to intrasellar metastasis from medullary thyroid cancer. Head Neck 2009, 31, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Kattan, M.W.; Leung, D.H.; Brennan, M.F. Postoperative nomogram for 12-year sarcoma-specific death. J. Clin. Oncol. 2002, 20, 791–796. [Google Scholar] [CrossRef]
- Han, L.; Zhu, Y.; Liu, Z.; Yu, T.; He, C.; Jiang, W.; Kan, Y.; Dong, D.; Tian, J.; Luo, Y. Radiomic nomogram for prediction of axillary lymph node metastasis in breast cancer. Eur. Radiol. 2019, 29, 3820–3829. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Modeling Group (%) (n = 1389) | Internal Validation Group (%) (n = 592) | External Validation Group (%) (n = 85) | |
|---|---|---|---|
| Age (Years) | |||
| <40 | 282 (20.3) | 100 (16.9) | 20 (23.5) |
| 40–59 | 545 (39.2) | 263 (44.4) | 47 (55.3) |
| ≥60 | 562 (40.5) | 229 (38.7) | 18 (21.2) |
| Sex | |||
| Female | 832 (59.9) | 351 (59.3) | 52 (61.2) |
| Male | 557 (40.1) | 241 (40.7) | 33 (38.8) |
| Race | |||
| White | 1178 (84.8) | 514 (86.8) | 0 (0) |
| Black | 129 (9.3) | 38 (6.4) | 0 (0) |
| Asian or Pacific Islander | 77 (5.5) | 34 (5.7) | 85 (0) |
| American Indian/Alaska Native | 5 (0.4) | 6 (1.0) | 0 (0) |
| Tumor Size (mm) | |||
| ≤20 | 736 (53.0) | 290 (49.0) | 54 (63.5) |
| 20–40 | 392 (28.2) | 172 (29.1) | 23 (27.1) |
| ≥40 | 261 (18.8) | 130 (21.9) | 8 (9.4) |
| Stage | |||
| I | 542 (39.0) | 210 (35.5) | 24 (28.2) |
| II | 291 (21.0) | 135 (22.8) | 11 (12.9) |
| III | 140 (10.1) | 66 (11.1) | 18 (21.2) |
| IV | 416 (29.9) | 181 (30.6) | 32 (37.6) |
| T Stage | |||
| T1 | 672 (48.4) | 257 (43.4) | 49 (57.6) |
| T2 | 323 (23.3) | 165 (27.9) | 25 (29.4) |
| T3 | 284 (20.4) | 122 (20.6) | 5 (5.9) |
| T4 | 110 (7.9) | 48 (8.1) | 6 (7.1) |
| N Stage | |||
| N0 | 857 (61.7) | 359 (60.6) | 35 (41.2) |
| N1a | 166 (12.0) | 77 (13.0) | 18 (21.2) |
| N1b | 366 (26.3) | 156 (26.4) | 32 (37.6) |
| M Stage | |||
| M0 | 1297 (93.4) | 547 (92.4) | 77 (90.6) |
| M1 | 92 (6.6) | 45 (7.6) | 8 (9.4) |
| Variable | Univariate Survival Analysis | Multivariate Survival Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age (Years) | ||||||
| <40 | Reference | Reference | ||||
| 40–59 | 2.558 | 1.540–4.250 | <0.001 | 2.920 | 1.750–4.872 | <0.001 |
| ≥60 | 7.354 | 4.543–11.905 | <0.001 | 7.610 | 4.674–12.392 | <0.001 |
| Sex | ||||||
| Female | Reference | Reference | ||||
| Male | 1.743 | 1.398–2.172 | <0.001 | 1.011 | 0.797–1.283 | 0.928 |
| Race | ||||||
| White | Reference | |||||
| Black | 0.904 | 0.613–1.334 | 0.611 | - | - | - |
| Asian or Pacific Islander | 0.405 | 0.201–0.818 | 0.012 | - | - | - |
| American Indian/Alaska Native | 2.160 | 0.537–8.686 | 0.278 | - | - | - |
| Tumor Size | ||||||
| ≤20 | Reference | Reference | ||||
| 20–40 | 1.651 | 1.253–2.174 | <0.001 | 2.338 | 1.219–4.483 | 0.011 |
| ≥40 | 3.386 | 2.605–4.401 | <0.001 | 3.330 | 1.826–6.073 | <0.001 |
| Stage | ||||||
| I | Reference | |||||
| II | 1.299 | 0.900–1.873 | 0.162 | - | - | - |
| III | 1.275 | 0.794–2.048 | 0.314 | - | - | - |
| IV | 4.241 | 3.201–5.620 | <0.001 | - | - | - |
| T Stage | ||||||
| T1 | Reference | |||||
| T2 | 1.299 | 0.942–1.792 | 0.110 | - | - | - |
| T3 | 2.508 | 1.889–3.328 | <0.001 | - | - | - |
| T4 | 5.136 | 3.753–7.030 | <0.001 | - | - | - |
| N Stage | ||||||
| N0 | Reference | Reference | ||||
| N1a | 1.612 | 1.136–2.287 | 0.007 | 1.327 | 0.981–1.793 | 0.066 |
| N1b | 3.007 | 2.373–3.809 | <0.001 | 1.874 | 1.493–2.351 | <0.001 |
| M Stage | ||||||
| M0 | Reference | Reference | ||||
| M1 | 8.317 | 6.364–10.870 | <0.001 | 3.868 | 2.805–5.335 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, W.; Wang, X.; Che, G.; Qiao, J.; Chen, Z.; Liu, J. The Establishment and Verification of a Nomogram Model for Predicting the Overall Survival of Medullary Thyroid Carcinoma: An Analysis Based on the SEER Database. Curr. Oncol. 2024, 31, 84-96. https://doi.org/10.3390/curroncol31010006
Wang W, Wang X, Che G, Qiao J, Chen Z, Liu J. The Establishment and Verification of a Nomogram Model for Predicting the Overall Survival of Medullary Thyroid Carcinoma: An Analysis Based on the SEER Database. Current Oncology. 2024; 31(1):84-96. https://doi.org/10.3390/curroncol31010006
Chicago/Turabian StyleWang, Wankun, Xujin Wang, Gang Che, Jincheng Qiao, Zhendong Chen, and Jian Liu. 2024. "The Establishment and Verification of a Nomogram Model for Predicting the Overall Survival of Medullary Thyroid Carcinoma: An Analysis Based on the SEER Database" Current Oncology 31, no. 1: 84-96. https://doi.org/10.3390/curroncol31010006