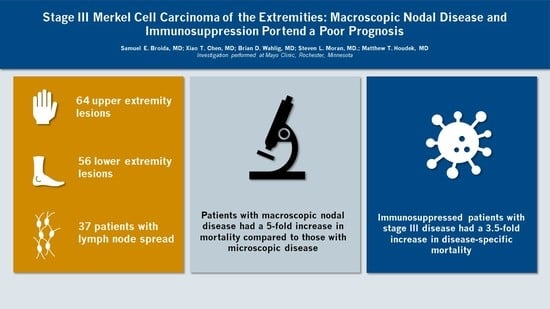
Multidisciplinary Treatment of Merkel Cell Carcinoma of the Extremities: Outcomes and Factors Associated with Poor Survival in Nodal Disease

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
3. Results
3.1. Lymph Node Investigation
3.2. Recurrence
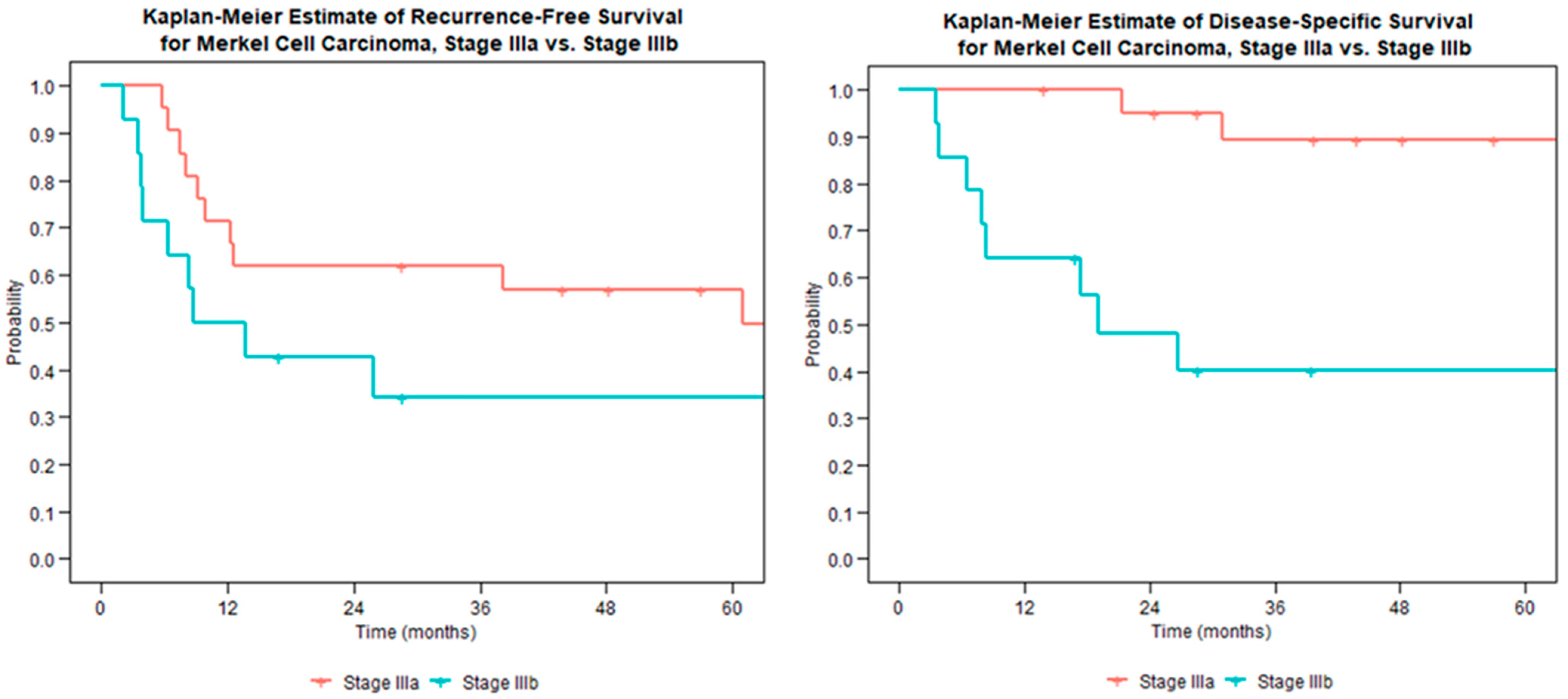
3.3. Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MCC | Merkel cell carcinoma |
| RFS | recurrence-free survival |
| DSS | disease-specific survival |
| PET | positron emission tomography |
| PPV | positive predictive value |
| NPV | negative predictive value |
| HR | hazard radio |
| CI | confidence interval |
| RT | Radiotherapy |
| LN | lymph node |
| LND | lymph node dissection |
| AJCC | American Joint Committee on Cancer |
References
- Becker, J.C.; Stang, A.; DeCaprio, J.A.; Cerroni, L.; Lebbé, C.; Veness, M.; Nghiem, P. Merkel cell carcinoma. Nat. Rev. Dis. Prim. 2017, 3, 17077. [Google Scholar] [CrossRef] [PubMed]
- Allen, P.J.; Bowne, W.B.; Jaques, D.P.; Brennan, M.F.; Busam, K.; Coit, D.G. Merkel Cell Carcinoma: Prognosis and Treatment of Patients From a Single Institution. J. Clin. Oncol. 2005, 23, 2300–2309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merkel Cell Carcinoma, Version 1.2021, NCCN Clinical Practice Guidelines in Oncology. Available online: https://merkelcell.org/wp-content/uploads/2021/02/NCCN-2021.pdf (accessed on 27 October 2022).
- Farley, C.R.; Perez, M.C.; Soelling, S.J.; Delman, K.A.; Harit, A.; Wuthrick, E.J.; Messina, J.L.; Sondak, V.K.; Zager, J.S.; Lowe, M.C. Merkel Cell Carcinoma Outcomes: Does AJCC8 Underestimate Survival? Ann. Surg. Oncol. 2020, 27, 1978–1985. [Google Scholar] [CrossRef] [PubMed]
- Bleicher, J.; Asare, E.A.; Flores, S.; Bowles, T.L.; Bowen, G.M.; Hyngstrom, J.R. Oncologic outcomes of patients with Merkel Cell Carcinoma (MCC): A multi-institutional cohort study. Am. J. Surg. 2020, 221, 844–849. [Google Scholar] [CrossRef] [PubMed]
- Lemos, B.D.; Storer, B.E.; Iyer, J.G.; Phillips, J.L.; Bichakjian, C.K.; Fang, L.C.; Johnson, T.M.; Liegeois-Kwon, N.J.; Otley, C.C.; Paulson, K.G.; et al. Pathologic nodal evaluation improves prognostic accuracy in Merkel cell carcinoma: Analysis of 5823 cases as the basis of the first consensus staging system. J. Am. Acad. Dermatol. 2010, 63, 751–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santamaria-Barria, J.A.; Boland, G.M.; Yeap, B.Y.; Nardi, V.; Dias-Santagata, D.; Cusack, J.C. Merkel Cell Carcinoma: 30-Year Experience from a Single Institution. Ann. Surg. Oncol. 2012, 20, 1365–1373. [Google Scholar] [CrossRef] [PubMed]
- Broida, S.E.; Alder, K.D.; Chen, X.T.; Moran, S.L.; Houdek, M.T. Outcome of Multidisciplinary Treatment of Merkel Cell Carcinoma of the Hand and Wrist. Anticancer Res. 2023, 43, 1549–1553. [Google Scholar] [CrossRef] [PubMed]
- American Joint Committee on Cancer. Merkel Cell Carcinoma. In AJCC Cancer Staging Manual, 8th ed.; Springer: Berlin/Heidelberg, Germany, 2017; p. 549. [Google Scholar]
- Senchenkov, A.; Moran, S.L. Merkel Cell Carcinoma: Diagnosis, Management, and Outcomes. Plast. Reconstr. Surg. 2013, 131, 771e–778e. [Google Scholar] [CrossRef] [PubMed]
- Broida, S.E.; Chen, X.T.; Baum, C.L.; Brewer, J.D.; Block, M.S.; Jakub, J.W.; Pockaj, B.A.; Foote, R.L.; Markovic, S.N.; Hieken, T.J.; et al. Merkel cell carcinoma of unknown primary: Clinical presentation and outcomes. J. Surg. Oncol. 2022, 126, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Perez, M.C.; Oliver, D.E.; Weitman, E.S.; Boulware, D.; Messina, J.L.; Torres-Roca, J.; Cruse, C.W.; Gonzalez, R.J.; Sarnaik, A.A.; Sondak, V.K.; et al. Management of Sentinel Lymph Node Metastasis in Merkel Cell Carcinoma: Completion Lymphadenectomy, Radiation, or Both? Ann. Surg. Oncol. 2019, 26, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Keeling, E.; O’Leary, E.; Deady, S.; O Neill, J.P.; Conlon, P.J.; Moloney, F.J. Gender and immunosuppression impact on Merkel cell carcinoma diagnosis and prognosis. A population based cohort study. Ski. Health Dis. 2021, 2, e80. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.C.; Lemos, B.; Douglas, J.; Iyer, J.; Nghiem, P. Radiation monotherapy as regional treatment for lymph node-positive Merkel cell carcinoma. Cancer 2010, 116, 1783–1790. [Google Scholar] [CrossRef] [PubMed]
- Cramer, J.D.; Suresh, K.; Sridharan, S. Completion lymph node dissection for merkel cell carcinoma. Am. J. Surg. 2020, 220, 982–986. [Google Scholar] [CrossRef] [PubMed]
- Tanda, E.T.; D’amato, A.L.; Rossi, G.; Croce, E.; Boutros, A.; Cecchi, F.; Spagnolo, F.; Queirolo, P. Merkel Cell Carcinoma: An Immunotherapy Fairy-Tale? Front. Oncol. 2021, 11, 3779. [Google Scholar] [CrossRef] [PubMed]
- Clarke, C.A.; Robbins, H.A.; Tatalovich, Z.; Lynch, C.F.; Pawlish, K.S.; Finch, J.L.; Hernandez, B.Y.; Fraumeni, J.F., Jr.; Madeleine, M.M.; Engels, E.A. Risk of Merkel Cell Carcinoma After Solid Organ Transplantation. J. Natl. Cancer Inst. 2014, 107, dju382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulson, K.; Iyer, J.G.; Blom, A.; Warton, E.M.; Sokil, M.; Yelistratova, L.; Schuman, L.; Nagase, K.; Bhatia, S.; Asgari, M.M.; et al. Systemic Immune Suppression Predicts Diminished Merkel Cell Carcinoma–Specific Survival Independent of Stage. J. Investig. Dermatol. 2013, 133, 642–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDonald, M.; You, J. Merkel Cell Polyomavirus: A New DNA Virus Associated with Human Cancer. Adv. Exp. Med. Biol. 2017, 1018, 35–56. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Ghidini, A.; Torchio, M.; Prinzi, N.; Trevisan, F.; Dallera, P.; De Stefani, A.; Russo, A.; Vitali, E.; Bruschieri, L.; et al. Adjuvant radiotherapy for Merkel cell carcinoma: A systematic review and meta-analysis. Radiother. Oncol. 2019, 134, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Nghiem, P.T.; Bhatia, S.; Lipson, E.J.; Kudchadkar, R.R.; Miller, N.J.; Annamalai, L.; Berry, S.; Chartash, E.K.; Daud, A.; Fling, S.P.; et al. PD-1 Blockade with Pembrolizumab in Advanced Merkel-Cell Carcinoma. N. Engl. J. Med. 2016, 374, 2542–2552. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Exam Modality | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|
| Clinical Exam (n = 103) | 35% (12/34) | 97% (67/69) | 86% (12/14) | 75% (67/89) |
| FDG-PET (n = 57) | 35% (8/23) | 91% (31/34) | 73% (8/11) | 67% (31/46) |
| Recurrence-Free Survival | Disease-Specific Survival | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Male gender | 2.0 | [0.8, 5.2] | 0.14 | 2.5 | [0.7, 9.4] | 0.16 |
| Age at Diagnosis | 1.1 | [1.0, 1.1] | 0.05 | 1.1 | [1.0, 1.1] | 0.06 |
| Upper Extremity Location | 1.4 | [0.6, 3.2] | 0.44 | 1.7 | [0.6, 5.3] | 0.35 |
| Max Diameter | 1.1 | [0.9, 1.4] | 0.68 | 1.1 | [0.8, 1.7] | 0.50 |
| Immunosuppressed | 2.1 | [0.9, 4.9] | 0.10 | 3.6 | [1.1, 11] | 0.03 * |
| Macroscopically-Positive Node | 2.0 | [0.8, 4.7] | 0.12 | 5.7 | [1.7, 19] | <0.01 ** |
| Palpable Lymphadenopathy | 2.4 | [0.9, 6.2] | 0.07 | 5.1 | [1.6, 17] | <0.01 ** |
| Hypermetabolic Node on PET | 5.0 | [1.4, 18] | <0.01 ** | 24.7 | [2.8, 220] | <0.01 ** |
| Complete Node Dissection | 1.1 | [0.5, 2.5] | 0.90 | 1.6 | [0.5, 4.8] | 0.40 |
| Radiation to Primary Site | 0.6 | [0.1, 2.6] | 0.48 | 1.2 | [0.2, 10] | 0.84 |
| Radiation to Lymph Nodes | 1.1 | [0.4, 3.3] | 0.90 | 0.8 | [0.2, 3.0] | 0.74 |
| XRT alone (ref. RLND alone) | 1.0 | [0.4, 2.6] | 0.95 | 0.7 | [0.2, 2.3] | 0.54 |
| Systemic Therapy | 0.7 | [0.2, 2.3] | 0.52 | 0.5 | [0.1, 3.6] | 0.46 |
| Disease Recurrence | Disease-Specific Survival | |||||||
|---|---|---|---|---|---|---|---|---|
| Total n. | Loc. | Reg. | Dist. | None | 1 Year | 3 Years | 5 Years | |
| Stage I&II Disease | 78 | 3 | 16 | 13 | 54 | 97% | 92% | 88% |
| Wide local excision | 70 | 3 | 14 | 12 | 49 | 97% | 91% | 86% |
| Adjuvant RT to primary | 51 | 1 | 10 | 9 | 36 | 96% | 94% | 90% |
| Adjuvant RT to LN | 9 | 1 | 2 | 4 | 6 | 100% | 89% | 89% |
| (+) Adjuvant Chemo | 3 | 0 | 1 | 0 | 2 | 100% | 100% | 100% |
| Stage III Disease | 38 | 1 | 10 | 17 | 17 | 86% | 71% | 71% |
| Wide local excision | 34 | 1 | 10 | 14 | 16 | 91% | 73% | 73% |
| Therapeutic LND | 14 | 1 | 3 | 7 | 4 | 94% | 59% | 59% |
| Adjuvant RT to primary | 33 | 1 | 10 | 15 | 13 | 88% | 74% | 74% |
| Adjuvant RT to LN | 29 | 1 | 9 | 12 | 14 | 86% | 74% | 74% |
| (+) Adjuvant Chemo | 6 | 0 | 2 | 2 | 3 | 83% | 83% | 83% |
| All Stages | 120 | 4 | 26 | 31 | 70 | 93% | 84% | 82% |
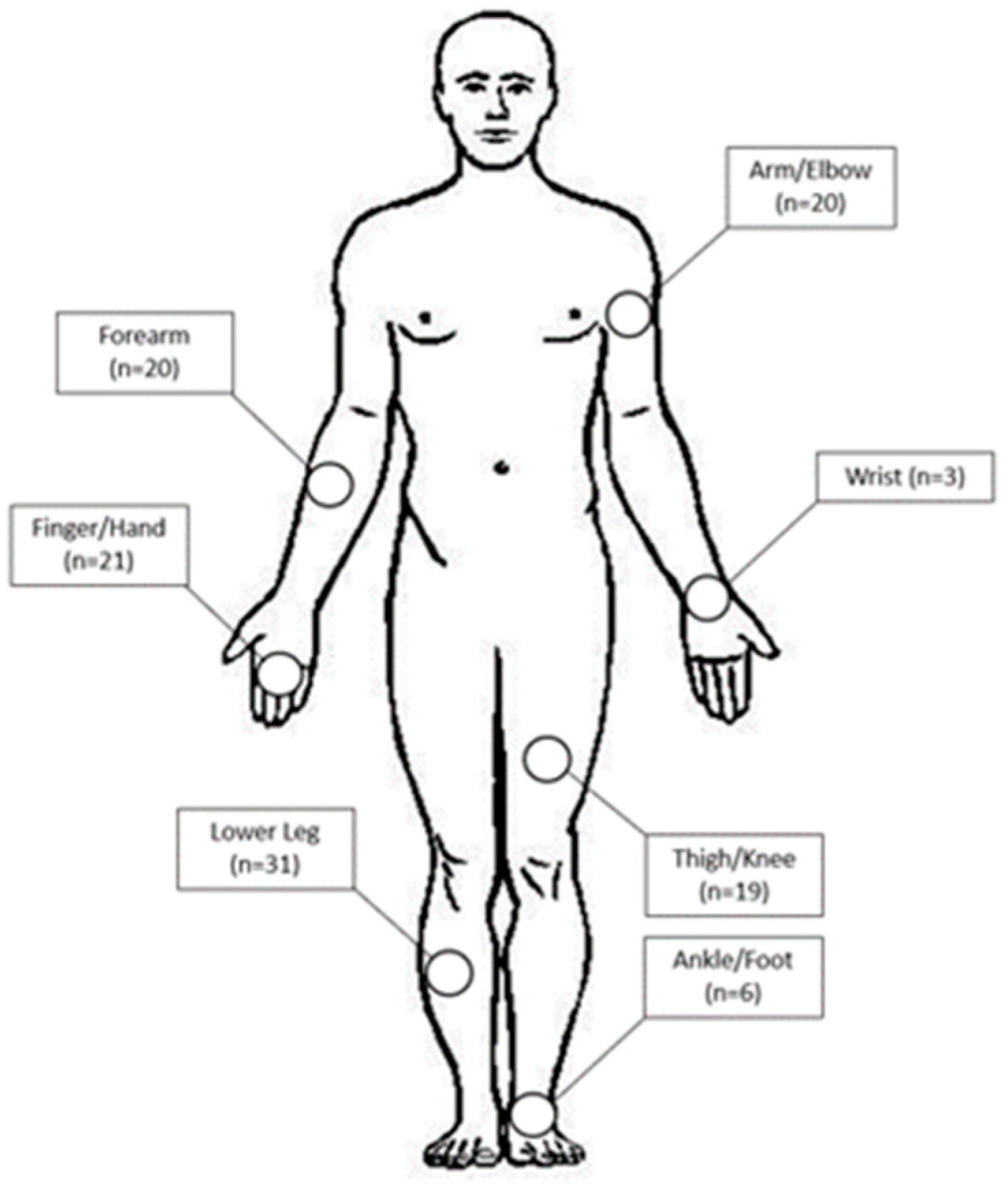
| Upper extremity | 64 | 0 | 11 | 12 | 41 | 94% | 82% | 82% |
| Lower extremity | 56 | 4 | 15 | 19 | 29 | 91% | 87% | 80% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Broida, S.E.; Chen, X.T.; Wahlig, B.D.; Moran, S.L.; Houdek, M.T. Multidisciplinary Treatment of Merkel Cell Carcinoma of the Extremities: Outcomes and Factors Associated with Poor Survival in Nodal Disease. Curr. Oncol. 2023, 30, 6246-6254. https://doi.org/10.3390/curroncol30070462
Broida SE, Chen XT, Wahlig BD, Moran SL, Houdek MT. Multidisciplinary Treatment of Merkel Cell Carcinoma of the Extremities: Outcomes and Factors Associated with Poor Survival in Nodal Disease. Current Oncology. 2023; 30(7):6246-6254. https://doi.org/10.3390/curroncol30070462
Chicago/Turabian StyleBroida, Samuel E., Xiao T. Chen, Brian D. Wahlig, Steven L. Moran, and Matthew T. Houdek. 2023. "Multidisciplinary Treatment of Merkel Cell Carcinoma of the Extremities: Outcomes and Factors Associated with Poor Survival in Nodal Disease" Current Oncology 30, no. 7: 6246-6254. https://doi.org/10.3390/curroncol30070462