Comparative Effectiveness of Chemotherapy Alone Versus Radiotherapy-Based Regimens in Locally Advanced Pancreatic Cancer: A Real-World Multicenter Analysis (PAULA-1)

 ,
,  , , , , , , ,
, , , , , , ,  and add
Show full author list
and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility
2.3. Treatment
2.4. Follow-Up
2.5. Statistical Analysis
2.6. Ethical Issues
3. Results
3.1. Patients and Treatment Characteristics
3.2. Outcomes
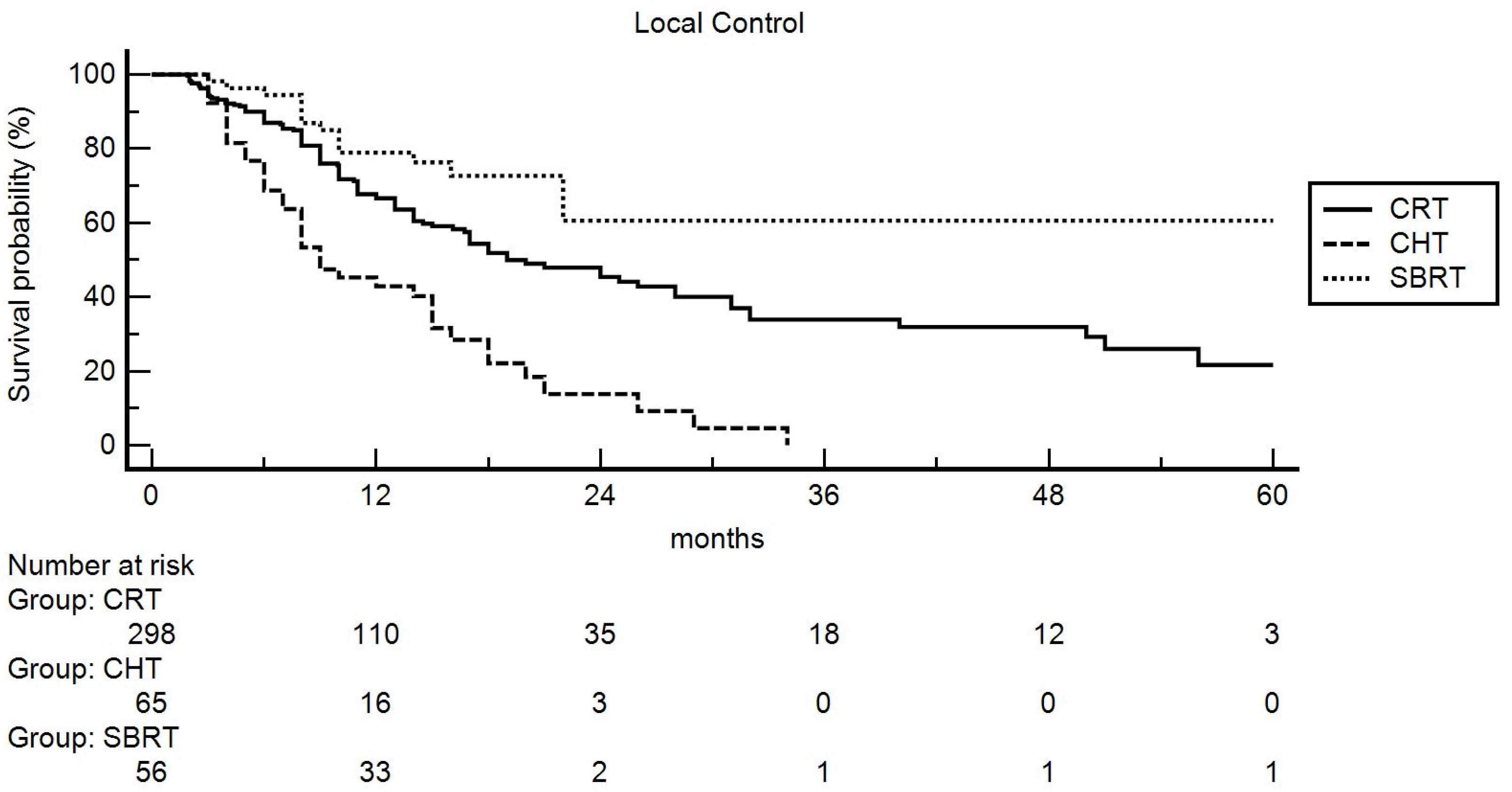
3.2.1. Local Control
3.2.2. Distant Metastasis-Free Survival
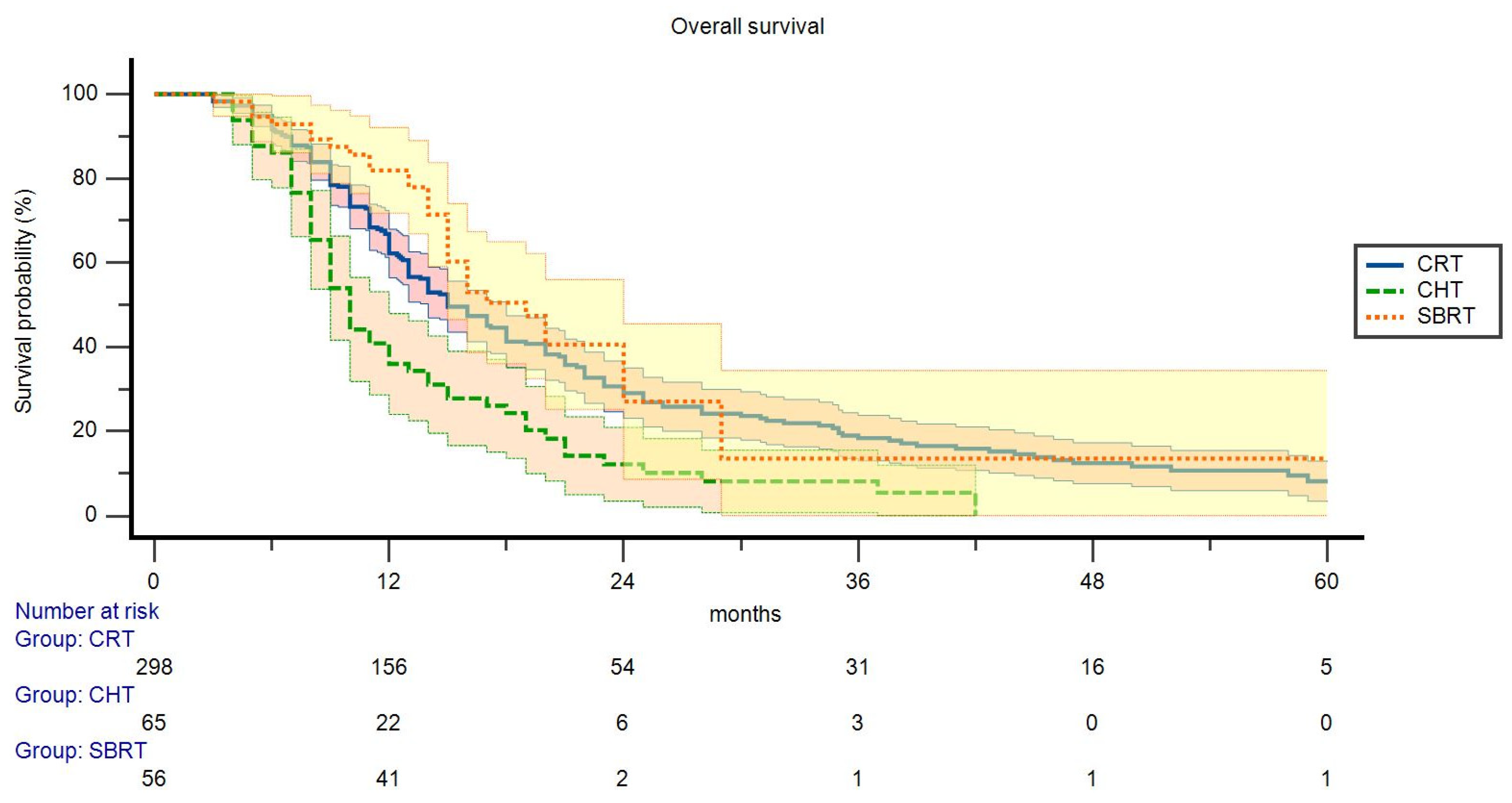
3.2.3. Overall Survival
4. Discussion
4.1. Summary and Contributions
4.2. Strenght and Limitations
4.3. Future Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, Z.J.; Heh, V.; Labiner, H.E.; Brock, G.N.; Ejaz, A.; Dillhoff, M.; Tsung, A.; Pawlik, T.M.; Cloyd, J.M. Surgical resection rates after neoadjuvant therapy for localized pancreatic ductal adenocarcinoma: Meta-analysis. Br. J. Surg. 2022, 110, 34–42. [Google Scholar] [CrossRef]
- 4. National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology (NCCN Guidelines) Pancreatic Ade-nocarcinoma. Version 2.2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf (accessed on 4 January 2023).
- Chauffert, B.; Mornex, F.; Bonnetain, F.; Rougier, P.; Mariette, C.; Bouché, O.; Bosset, J.F.; Aparicio, T.; Mineur, L.; Azzedine, A.; et al. Phase III trial comparing intensive induction chemoradiotherapy (60 Gy, infusional 5-FU and intermittent cisplatin) followed by maintenance gemcitabine with gemcitabine alone for locally advanced unresectable pancreatic cancer. Definitive results of the 2000-01 FFCD/SFRO study. Ann. Oncol. 2008, 19, 1592–1599. [Google Scholar] [CrossRef] [PubMed]
- Hammel, P.; Huguet, F.; van Laethem, J.L.; Goldstein, D.; Glimelius, B.; Artru, P.; Borbath, I.; Bouché, O.; Shannon, J.; André, T.; et al. Effect of chemoradiotherapy vs. chemotherapy on survival in patients with locally advanced pancreatic cancer controlled after 4 months of gemcitabine with or without erlotinib: The LAP07 randomized clinical trial. JAMA 2016, 315, 1844–1853. [Google Scholar] [CrossRef]
- Loehrer, P.J.; Feng, Y.; Cardenes, H.; Wagner, L.; Brell, J.M.; Cella, D.; Flynn, P.; Ramanathan, R.K.; Crane, C.H.; Alberts, S.R.; et al. Gemcitabine alone versus gemcitabine plus radiotherapy in patients with locally advanced pancreatic cancer: An Eastern Cooperative Oncology Group trial. J. Clin. Oncol. 2011, 29, 4105–4112. [Google Scholar] [CrossRef]
- Herman, J.M.; Chang, D.T.; Goodman, K.A.; Dholakia, A.S.; Raman, S.P.; Hacker-Prietz, A.; Iacobuzio-Donahue, C.A.; Griffith, M.E.; Pawlik, T.M.; Pai, J.S.; et al. Phase 2 multiinstitutional trial evaluating gemcitabine and stereotactic body radiotherapy for patients with locally advanced unresectable pancreatic adenocarcinoma. Cancer 2015, 121, 1128–1137. [Google Scholar] [CrossRef]
- Schellenberg, D.; Goodman, K.A.; Lee, F.; Chang, S.; Kuo, T.; Ford, J.M.; Fisher, G.A.; Quon, A.; Desser, T.S.; Norton, J.; et al. Gemcitabine chemotherapy and single-fraction stereotactic body radiotherapy for locally advanced pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Schellenberg, D.; Kim, J.; Christman-Skieller, C.; Chun, C.L.; Columbo, L.A.; Ford, J.M.; Fisher, G.A.; Kunz, P.L.; Van Dam, J.; Quon, A.; et al. Single-fraction stereotactic body radiation therapy and sequential gemcitabine for the treatment of locally advanced pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 181–188. [Google Scholar] [CrossRef]
- Polistina, F.; Costantin, G.; Casamassima, F.; Francescon, P.; Guglielmi, R.; Panizzoni, G.; Febbraro, A.; Ambrosino, G.U. Unresectable locally advanced pancreatic cancer: A multimodal treatment using neoadjuvant chemoradiotherapy (gemcitabine plus stereotactic radiosurgery) and subsequent surgical exploration. Ann. Surg. Oncol. 2010, 17, 2092–2101. [Google Scholar] [CrossRef]
- Tchelebi, L.T.; Lehrer, E.J.; Trifiletti, D.M.; Sharma, N.K.; Gusani, N.J.; Crane, C.H.; Zaorsky, N.G. Conventionally fractionated radiation therapy versus stereotactic body radiation therapy for locally advanced pancreatic cancer (CRiSP): An international systematic review and meta-analysis. Cancer 2020, 126, 2120–2131. [Google Scholar] [CrossRef]
- Cellini, F.; Arcelli, A.; Simoni, N.; Caravatta, L.; Buwenge, M.; Calabrese, A.; Brunetti, O.; Genovesi, D.; Mazzarotto, R.; Deodato, F.; et al. Basics and frontiers on pancreatic cancer for radiation oncology: Target delineation, SBRT, SIB technique, MRgRT, particle therapy, immunotherapy, and clinical guidelines. Cancers 2020, 12, 1729. [Google Scholar] [CrossRef]
- Arcelli, A.; Guido, A.; Buwenge, M.; Simoni, N.; Mazzarotto, R.; Macchia, G.; Deodato, F.; Cilla, S.; Bonomo, P.; Scotti, V.; et al. Higher Biologically Effective Dose Predicts Survival in SBRT of Pancreatic Cancer: A Multicentric Analysis (PAULA-1). Anticancer Res. 2020, 40, 465–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arcelli, A.; Buwenge, M.; Macchia, G.; Bertini, F.; Guido, A.; Deodato, F.; Cilla, S.; Scotti, V.; Rosetto, M.E.; Djan, I.; et al. Stereotactic body radiotherapy vs. conventionally fractionated chemoradiation in locally advanced pancreatic cancer: A multicenter case-control study (PAULA-1). Cancer Med. 2020, 9, 7879–7887. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.; Meier, P. Nonparametric Estimation from Incomplete Observations. Am. J. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Peto, R.; Peto, J. Asymptotically efficient rank invariant procedures. J. R. Stat. Soc. 1972, 135, 185–207. [Google Scholar] [CrossRef]
- Cox, D.R. Regression models and life tables (with discussion). J. R. Stat. Soc. Ser. B 1972, 74, 187–220. [Google Scholar]
- Mukherjee, S.; Hurt, C.N.; Bridgewater, J.; Falk, S.; Cummins, S.; Wasan, H.; Crosby, T.; Jephcott, C.; Roy, R.; Radhakrishna, G.; et al. Gemcitabine-based or capecitabine-based chemoradiotherapy for locally advanced pancreatic cancer (SCALOP): A multicentre, randomised, phase 2 trial. Lancet Oncol. 2013, 14, 317–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrelli, F.; Comito, T.; Ghidini, A.; Torri, V.; Scorsetti, M.; Barni, S. Stereotactic Body Radiation Therapy for Locally Advanced Pancreatic Cancer: A Systematic Review and Pooled Analysis of 19 Trials. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 313–322. [Google Scholar] [CrossRef]
- Lin, J.C.; Jen, Y.M.; Li, M.H.; Chao, H.L.; Tsai, J.T. Comparing outcomes of stereotactic body radiotherapy with intensity-modulated radio therapy for patients with locally advanced unresectable pancreatic cancer. Eur. J. Gastroenterol. Hepatol. 2015, 27, 259–264. [Google Scholar] [CrossRef]
- De Geus, S.W.L.; Eskander, M.F.; Kasumova, G.G.; Ng, S.C.; Kent, T.S.; Mancias, J.D.; Callery, M.P.; Mahadevan, A.; Tseng, J.F. Stereotactic body radiotherapy for unresected pancreatic cancer: A nationwide review. Cancer 2017, 123, 4158–4167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, J.; Patel, K.; Switchenko, J.; Cassidy, R.J.; Hall, W.A.; Gillespie, T.; Patel, P.R.; Kooby, D.; Landry, J. Outcomes for patients with locally advanced pancreatic adenocarcinoma treated with stereotactic body radiation therapy versus conventionally fractionated radiation. Cancer 2017, 123, 3486–3493. [Google Scholar] [CrossRef] [Green Version]
- Rudra, S.; Jiang, N.; Rosenberg, S.A.; Olsen, J.R.; Roach, M.C.; Wan, L.; Portelance, L.; Mellon, E.A.; Bruynzeel, A.; Lagerwaard, F.; et al. Using adaptive magnetic resonance image-guided radiation therapy for treatment of inoperable pancreatic cancer. Cancer Med. 2019, 8, 2123–2132. [Google Scholar] [CrossRef]
- Reyngold, M.; O’Reilly, E.M.; Varghese, A.M.; Fiasconaro, M.; Zinovoy, M.; Romesser, P.B.; Wu, A.; Hajj, C.; Cuaron, J.J.; Tuli, R.; et al. Association of Ablative Radiation Therapy with Survival among Patients with Inoperable Pancreatic Cancer. JAMA Oncol. 2021, 7, 735–738. [Google Scholar] [CrossRef]
- Dudeja, V.; Greeno, E.W.; Walker, S.P.; Jensen, E.H. Neoadjuvant chemoradiotherapy for locally advanced pancreas cancer rarely leads to radiological evidence of tumour regression. HPB 2013, 15, 661–667. [Google Scholar] [CrossRef] [Green Version]
- Wilson, J.M.; Mukherjee, S.; Brunner, T.B.; Partridge, M.; Hawkins, M.A. Correlation of 18F-Fluorodeoxyglucose Positron Emission Tomography Parameters with Patterns of Disease Progression in Locally Advanced Pancreatic Cancer after Definitive Chemoradiotherapy. Clin. Oncol. 2017, 29, 370–377. [Google Scholar] [CrossRef] [Green Version]
- Ozaka, M.; Nakachi, K.; Kobayashi, S.; Ohba, A.; Imaoka, H.; Terashima, T.; Ishii, H.; Mizusawa, J.; Katayama, H.; Kataoka, T.; et al. Hepatobiliary and Pancreatic Oncology Group of Japan Clinical Oncology Group (JCOG). A andomized phase II study of modified FOLFIRINOX versus gemcitabine plus nab-paclitaxel for locally advanced pancreatic cancer (JCOG1407). Eur. J. Cancer 2023, 181, 135–144. [Google Scholar] [CrossRef]
- Su, Y.Y.; Chiu, Y.F.; Li, C.P.; Yang, S.H.; Lin, J.; Lin, S.J.; Chang, P.Y.; Chiang, N.J.; Shan, Y.S.; Ch’ang, H.J.; et al. A phase II and omized trial of induction chemotherapy followed by concurrent chemoradiotherapy in locally advanced pancreatic cancer: The Taiwan Cooperative Oncology Group T2212 study. Br. J. Cancer 2022, 126, 1018–1026. [Google Scholar] [CrossRef]
- Suker, M.; Beumer, B.R.; Sadot, E.; Marthey, L.; Faris, J.E.; Mellon, E.A.; El-Rayes, B.F.; Wang-Gillam, A.; Lacy, J.; Hosein, P.J.; et al. FOLFIRINOX for locally advanced pancreatic cancer: A systematic review and patient-level meta-analysis. Lancet Oncol. 2016, 17, 801–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buwenge, M.; Macchia, G.; Arcelli, A.; Frakulli, R.; Fuccio, L.; Guerri, S.; Grassi, E.; Cammelli, S.; Cellini, F.; Morganti, A.G. Stereotactic radiotherapy of pancreatic cancer: A systematic review on pain relief. J. Pain Res. 2018, 11, 2169–2178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piper, M.; Hoen, M.; Darragh, L.B.; Knitz, M.W.; Nguyen, D.; Gadwa, J.; Durini, G.; Karakoc, I.; Grier, A.; Neupert, B.; et al. Simultaneous targeting of PD-1 and IL-2Rβγ with radiation therapy inhibits pancreatic cancer growth and metastasis. Cancer Cell 2023, 41, 950–969. [Google Scholar] [CrossRef]
- Cronin, K.A.; Scott, S.; Firth, A.U.; Sung, H.; Henley, S.J.; Sherman, R.L.; Siegel, R.L.; Anderson, R.N.; Kohler, B.A.; Benard, V.B.; et al. Annual report to the nation on the status of cancer, part 1: National cancer statistics. Cancer 2022, 128, 4251–4284. [Google Scholar] [CrossRef]
- Gurka, M.K.; Collins, S.P.; Slack, R.; Tse, G.; Charabaty, A.; Ley, L.; Berzcel, L.; Lei, S.; Suy, S.; Haddad, N.; et al. Stereotactic body radiation therapy with concurrent full-dose gemcitabine for locally advanced pancreatic cancer: A pilot trial demonstrating safety. Radiat. Oncol. 2013, 8, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.J.; Hajj, C.; Reyngold, M.; Shi, W.; Zhang, Z.; Cuaron, J.J.; Crane, C.H.; O’Reilly, E.M.; Lowery, M.A.; Yu, K.H.; et al. Stereotactic body radiation vs. intensity-modulated radiation for unresectable pancreatic cancer. Acta Oncol. 2017, 56, 1746–1753. [Google Scholar] [CrossRef] [Green Version]
- Rwigema, J.C.; Parikh, S.D.; Heron, D.E.; Howell, M.; Zeh, H.; Moser, A.J.; Bahary, N.; Quinn, A.; Burton, S. A Stereotactic body radiotherapy in the treatment of advanced adenocarcinoma of the pancreas. Am. J. Clin. Oncol. 2011, 34, 63–69. [Google Scholar] [CrossRef]
- Rajagopalan, M.S.; Heron, D.E.; Wegner, R.E.; Zeh, H.J.; Bahary, N.; Krasinskas, A.M.; Lembersky, B.; Brand, R.; Moser, A.J.; Quinn, A.E.; et al. Pathologic response with neoadjuvant chemotherapy and stereotactic body radiotherapy for borderline resectable and locally-advanced pancreatic cancer. Radiat. Oncol. 2013, 8, 254. [Google Scholar] [CrossRef] [Green Version]
- Moningi, S.; Dholakia, A.S.; Raman, S.P.; Blackford, A.; Cameron, J.L.; Le, D.T.; De Jesus-Acosta, A.M.; Hacker-Prietz, A.; Rosati, L.M.; Assadi, R.K.; et al. The role of stereotactic body radiation therapy for pancreatic cancer: A single-institution experience. Ann. Surg. Oncol. 2015, 22, 2352–2358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tozzi, A.; Comito, T.; Alongi, F.; Navarria, P.; Iftode, C.; Mancosu, P.; Reggiori, G.; Clerici, E.; Rimassa, L.; Zerbi, A.; et al. SBRT in unresectable advanced pancreatic cancer: Preliminary results of a mono-institutional experience. Radiat. Oncol. 2013, 8, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Value | Total (%) | CRT (%) | CHT (%) | SBRT (%) | p |
|---|---|---|---|---|---|---|
| Age (years) | Median (range) | 66 (34–90) | 67 (34–90) | 63 (44–88) | 68 (36–89) | |
| ≤65 | 199 (47.5) | 140 (47.0) | 35 (53.8) | 24 (42.9) | 0.457 | |
| >65 | 220 (52.5) | 158 (53.0) | 30 (46.2) | 32 (57.1) | ||
| Gender | M | 226 (53.9) | 164 (55.0) | 31 (47.7) | 31 (55.4) | 0.546 |
| F | 193 (46.1) | 134 (45.0) | 34 (52.3) | 25 (44.6) | ||
| ECOG | 0 | 167 (39.9) | 121 (40.7) | 19 (29.2) | 27 (48.2) | 0.005 |
| 1 | 131 (31.2) | 71 (23.8) | 37 (56.9) | 23 (41.1) | ||
| 2 | 33 (7.9) | 21 (7.0) | 7 (10.8) | 5 (8.9) | ||
| Missing | 88 (21.0) | 85 (28.5) | 2 (3.1) | 1 (1.8) | ||
| Tumor site | Head | 283 (67.5) | 207 (69.5) | 43 (66.2) | 33 (58.9) | 0.004 |
| Body | 105 (25.1) | 75 (25.2) | 11 (16.9) | 19 (33.9) | ||
| Tail | 26 (6.2) | 12 (4.0) | 10 (15.4) | 4 (7.2) | ||
| Missing | 5 (1.2) | 4 (1.3) | 1 (1.5) | 0 (0.0) | ||
| Tumor diameter (cm) | Median (range) | 3.9 (1.2–10.0) | 3.6 (1.4–10.0) | 4.0 (2.0–7.0) | 3.9 (1.2–8.7) | |
| <3.0 | 59 (14.1) | 44 (14.8) | 8 (12.2) | 7 (12.5) | 0.271 | |
| ≥3.0 and <3.9 | 112 (26.7) | 84 (28.2) | 9 (13.9) | 19 (33.9) | ||
| ≥3.9 | 248 (59.2) | 170 (57.0) | 48 (73.9) | 30 (53.6) | ||
| Clinical T stage | 3 | 144 (34.4) | 117 (39.3) | 10 (15.4) | 17 (30.4) | 0.012 |
| 4 | 275 (65.6) | 181 (60.7) | 55 (84.6) | 39 (69.6) | ||
| Clinical N stage | 0 | 165 (39.4) | 131 (44.0) | 0 (0.0) | 34 (60.7) | <0.001 |
| 1–2 | 232 (55.4) | 156 (52.3) | 54 (98.2) | 22 (39.3) | ||
| Missing | 22 (5.2) | 11 (3.7) | 11 (1.8) | 0 (0.0) | ||
| CHT | Gemcitabine-based | 238 (56.8) | 165 (55.4) | 50 (76.9) | 23 (41.1) | 0.098 |
| Fluopyrimidine-based | 148 (35.3) | 123 (41.2) | 7 (10.8) | 18 (32.1) | ||
| Others | 18 (4.3) | 10 (3.4) | 8 (12.3) | / | / | |
| No | 15 (3.6) | / | / | 15 (26.8) | / | |
| Total dose (Gy) | Median (range) | 50.4 (10.8–66.0) | 50.4 (10.8–66.0) | / | 30.0 (18.0–45.0) | / |
| Ca 19-9 (U/mL) | Median (range) | 235 (1–25,663) | 220 (1–25,663) | 290 (1–6206) | 203 (1–20,000) | 0.389 |
| BEDα/β 10 Gy | Median (range) | 59.4 (12.7–115.1) | 59.4 (12.7–115.1) | / | 48.0 (28.0–78.7) | / |
| BEDα/β 10 Gy | <59.4 Gy | 109 (26.0) | 58 (19.5) | / | 51 (91.1) | <0.001 |
| ≥59.4 Gy | 245 (58.5) | 240 (80.5) | / | 5 (8.9) | ||
| Missing | 65 (15.5) | / | 65 (100.0) | / | / | |
| Treatment | CRT | 298 (71.1) | / | / | / | / |
| CHT | 65 (15.5) | / | / | / | ||
| SBRT | 56 (13.4) | / | / | / |
| Univariate Analysis | LC Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Value | 1-Year LC (%) | 2-Year LC (%) | Median LC (Months) | p | HR | 95% CI | p |
| Age | ≤65 | 68.3 | 46.2 | 21 | 0.124 | |||
| >65 | 60.5 | 39.3 | 17 | |||||
| Gender | M | 64.3 | 42.8 | 18 | 0.629 | |||
| F | 64.0 | 41.8 | 20 | |||||
| ECOG | 0 | 63.8 | 47.7 | 21 | 0.108 | |||
| 1 | 52.6 | 34.2 | 14 | |||||
| 2 | 62.2 | 0.0 | 15 | |||||
| Tumor site | Head | 61.3 | 37.5 | 17 | 0.020 | |||
| Body | 71.1 | 33.5 | 28 | |||||
| Tail | 58.8 | 29.8 | 17 | |||||
| Tumor diameter (cm) | <3.0 | 60.0 | 39.9 | 15 | 0.191 | |||
| ≥3.0 and <3.9 | 57.2 | 33.1 | 15 | |||||
| ≥3.9 | 68.3 | 47.3 | 22 | |||||
| cT stage | 3 | 63.1 | 39.9 | 17 | 0.695 | |||
| 4 | 64.7 | 43.7 | 20 | |||||
| cN stage | 0 | 69.4 | 48.9 | 21 | 0.081 | |||
| 1-2 | 60.7 | 39.3 | 17 | |||||
| Ca 19-9 (U/mL) | ≤235 | 39.6 | 23.7 | 16 | 0.801 | |||
| >235 | 42.1 | 21.5 | 19 | |||||
| Treatment | CRT | 66.6 | 45.4 | 19 | <0.001 | |||
| CHT | 42.9 | 13.8 | 9 | |||||
| SBRT | 79.0 | 60.6 | NR | |||||
| CHT vs. CRT | CRT | 0.61 | 0.37–1.00 | 0.053 | ||||
| tumor site: body | 0.58 | 0.35–0.95 | 0.032 | |||||
| CRT vs. CHT vs. SBRT | CRT | 0.56 | 0.34–0.92 | 0.022 | ||||
| SBRT | 0.27 | 0.13–0.54 | <0.001 | |||||
| CRT vs. SBRT | tumor site: body | 0.53 | 0.32–0.88 | 0.015 | ||||
| SBRT | 0.46 | 0.25–0.83 | 0.011 | |||||
| CHT vs. CRT + SBRT | tumor site: body | 0.54 | 0.33–0.90 | 0.019 | ||||
| CHT vs. SBRTT | tumor site: body | 0.30 | 0.11–0.79 | 0.015 | ||||
| Univariate Analysis | DMFS Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Value | 1-Year DMFS (%) | 2-Year DMFS (%) | Median DMFS (Months) | p | HR | 95% CI | p |
| Age | ≤65 | 56.3 | 37.8 | 15 | 0.539 | |||
| >65 | 50.9 | 32.2 | 13 | |||||
| Gender | M | 57.1 | 39.4 | 16 | 0.061 | |||
| F | 49.6 | 30.1 | 12 | |||||
| ECOG | 0 | 55.1 | 34.2 | 14 | 0.824 | |||
| 1 | 53.7 | 31.3 | 14 | |||||
| 2 | 48.9 | 29.3 | 12 | |||||
| Tumor site | Head | 47.8 | 32.6 | 12 | 0.289 | |||
| Body | 60.7 | 35.4 | 14 | |||||
| Tail | 73.6 | 43.6 | 24 | |||||
| Tumor diameter (cm) | <3.0 | 53.9 | 26.6 | 13 | 0.273 | |||
| ≥3.0 and <3.9 | 48.5 | 27.8 | 12 | |||||
| ≥3.9 | 55.8 | 40.2 | 15 | |||||
| cT stage | 3 | 39.0 | 25.1 | 10 | <0.001 | |||
| 4 | 61.0 | 40.0 | 16 | |||||
| cN stage | 0 | 53.5 | 40.9 | 15 | 0.274 | |||
| 1–2 | 52.6 | 33.0 | 13 | |||||
| Ca 19-9 (U/mL) | ≤235 | 33.5 | 26.8 | 13 | 0.930 | |||
| >235 | 31.9 | 22.8 | 13 | |||||
| BED (α/β 10 Gy) | <59.4 Gy | 47.6 | 20.1 | 12 | 0.039 | |||
| ≥59.4 Gy | 55.0 | 41.4 | 16 | |||||
| Treatment | CRT | 52.2 | 34.8 | 13 | 0.819 | |||
| CHT | 59.1 | 42.2 | 15 | |||||
| SBRT | 55.6 | 24.0 | 14 | |||||
| CRT vs. CHT vs. SBRT | cT4 | 0.68 | 0.47–1.00 | 0.056 | ||||
| Univariate Analysis | OS Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Value | 1-Year OS (%) | 2-Year OS (%) | Median OS (Months) | p | HR | 95% CI | p |
| Age | ≤65 | 61.4 | 31.0 | 16 | 0.177 | |||
| >65 | 60.0 | 22.2 | 14 | |||||
| Gender | M | 61.1 | 25.9 | 15 | 0.605 | |||
| F | 60.2 | 26.6 | 15 | |||||
| ECOG | 0 | 72.8 | 39.1 | 19 | 0.007 | |||
| 1 | 58.2 | 23.9 | 15 | |||||
| 2 | 56.1 | 10.9 | 13 | |||||
| Tumor site | Head | 56.9 | 21.1 | 14 | 0.025 | |||
| Body | 65.8 | 32.6 | 17 | |||||
| Tail | 76.2 | 54.3 | 28 | |||||
| Tumor diameter (cm) | <3.0 | 64.2 | 30.5 | 14 | 0.088 | |||
| ≥3.0 and <3.9 | 70.1 | 33.0 | 16 | |||||
| ≥3.9 | 62.0 | 22.3 | 15 | |||||
| cT stage | 3 | 52.7 | 19.7 | 13 | 0.078 | |||
| 4 | 65.0 | 29.9 | 16 | |||||
| cN stage | 0 | 68.4 | 23.9 | 16 | 0.068 | |||
| 1-2 | 55.8 | 26.6 | 14 | |||||
| Ca 19-9 (U/mL) | ≤235 | 35.5 | 12.2 | 18 | 0.042 | |||
| >235 | 25.5 | 4.7 | 15 | |||||
| Treatment | CRT | 62.2 | 29.1 | 15 | <0.001 | |||
| CHT | 36.0 | 12.2 | 10 | |||||
| SBRT | 81.9 | 27.1 | 19 | |||||
| CHT vs. CRT | CRT | 0.44 | 0.27–0.70 | <0.001 | ||||
| CRT vs. CHT vs. SBRT | CRT | 0.44 | 0.28–0.70 | <0.001 | ||||
| SBRT | 0.40 | 0.22–0.74 | 0.003 | |||||
| CRT vs. SBRT | tumor site: tail | 0.30 | 0.11–0.82 | 0.019 | ||||
| CHT vs. CRT + SBRT | tumor site: tail | 0.30 | 0.11–0.82 | 0.019 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arcelli, A.; Tarantino, G.; Cellini, F.; Buwenge, M.; Macchia, G.; Bertini, F.; Guido, A.; Deodato, F.; Cilla, S.; Scotti, V.; et al. Comparative Effectiveness of Chemotherapy Alone Versus Radiotherapy-Based Regimens in Locally Advanced Pancreatic Cancer: A Real-World Multicenter Analysis (PAULA-1). Curr. Oncol. 2023, 30, 5690-5703. https://doi.org/10.3390/curroncol30060427
Arcelli A, Tarantino G, Cellini F, Buwenge M, Macchia G, Bertini F, Guido A, Deodato F, Cilla S, Scotti V, et al. Comparative Effectiveness of Chemotherapy Alone Versus Radiotherapy-Based Regimens in Locally Advanced Pancreatic Cancer: A Real-World Multicenter Analysis (PAULA-1). Current Oncology. 2023; 30(6):5690-5703. https://doi.org/10.3390/curroncol30060427
Chicago/Turabian StyleArcelli, Alessandra, Giuseppe Tarantino, Francesco Cellini, Milly Buwenge, Gabriella Macchia, Federica Bertini, Alessandra Guido, Francesco Deodato, Savino Cilla, Valerio Scotti, and et al. 2023. "Comparative Effectiveness of Chemotherapy Alone Versus Radiotherapy-Based Regimens in Locally Advanced Pancreatic Cancer: A Real-World Multicenter Analysis (PAULA-1)" Current Oncology 30, no. 6: 5690-5703. https://doi.org/10.3390/curroncol30060427