Afatinib for the Treatment of NSCLC with Uncommon EGFR Mutations: A Narrative Review



Abstract
:1. Introduction
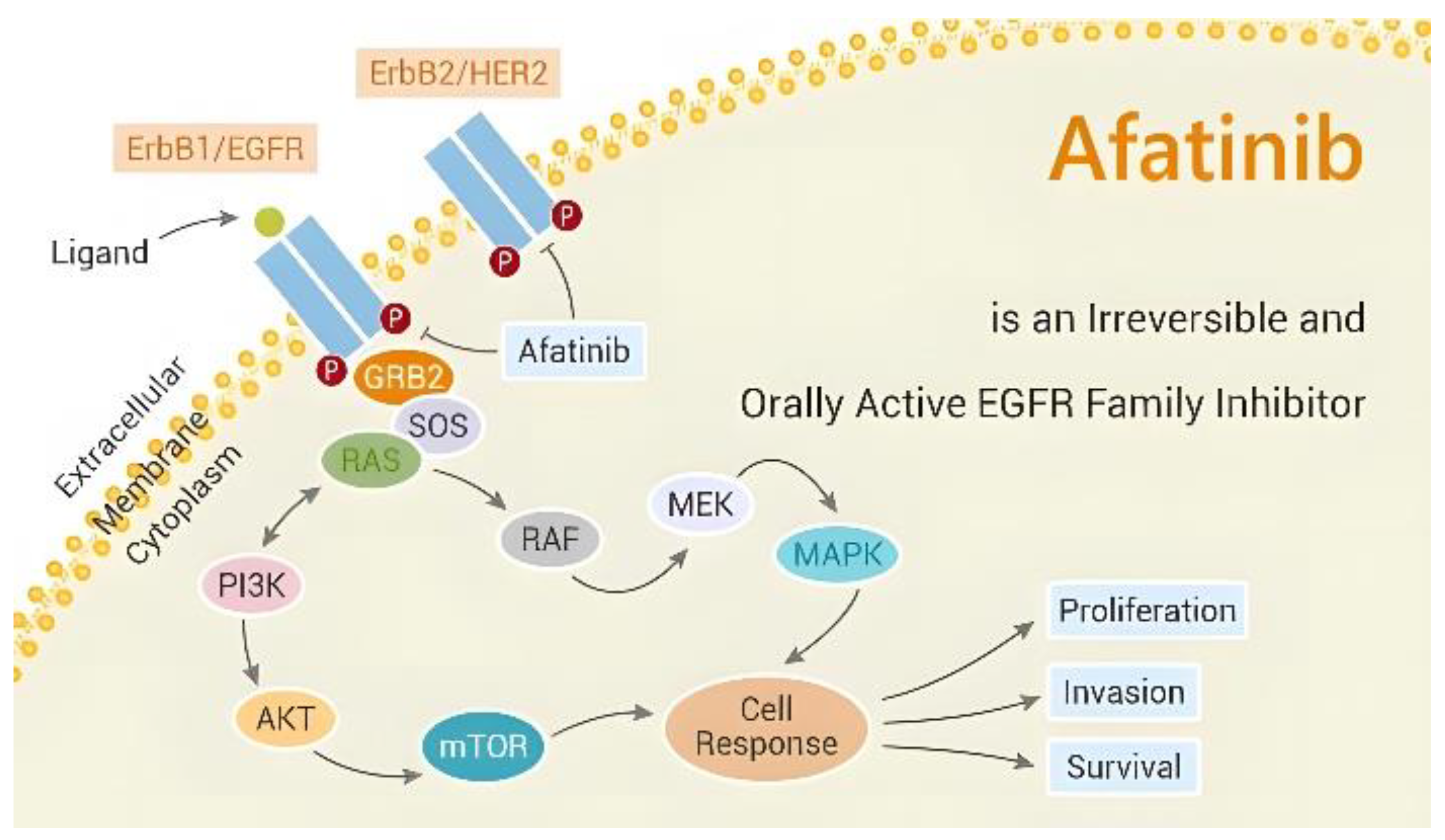
2. Anti-Tumor Mechanism
3. Afatinib’s Effectiveness in Curing Various Uncommon EGFR Mutations
3.1. Major Uncommon Mutations (G719X/S768I/L861Q)
3.2. Exon 18 Mutations (Except G719X)
3.3. Uncommon Mutations in Exon 19
3.4. Exon 20 Insertions and T790M Mutations
3.5. Uncommon Exon 21 Mutations
3.6. Compound Mutations
3.7. Rare Mutations following Resistance to Osimertinib
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Tankere, P.; Boidot, R.; Bonniaud, P.; Zouak, A.; Foucher, P.; Milliere, A.; Bertaut, A.; Favier, L.; Lagrange, A.; Ghiringhelli, F.; et al. Uncommon EGFR mutations in lung carcinoma: Features and treatment outcomes in a retrospective French cohort. J. Thorac. Dis. 2022, 14, 2034–2044. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Franchina, T.; Ricciardi, G.; Battaglia, A.; Picciotto, M.; Adamo, V. Heterogeneous Responses to Epidermal Growth Factor Receptor (EGFR) Tyrosine Kinase Inhibitors (TKIs) in Patients with Uncommon EGFR Mutations: New Insights and Future Perspectives in this Complex Clinical Scenario. Int. J. Mol. Sci. 2019, 20, 1431. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Yang, G.; Liu, R.; Yang, Y.; Li, W.; Li, J.; Hao, X.; Xing, P.; Wang, Y. EGFR uncommon alterations in advanced non-small cell lung cancer and structural insights into sensitivity to diverse tyrosine kinase inhibitors. Front. Pharmacol. 2022, 13, 976731. [Google Scholar] [CrossRef] [PubMed]
- Ullas, B.; Shrinidhi, N.; Mansi, S.; Narayan, S.; Parveen, J.; Surender, D.; Joslia, J.T.; Anurag, M. All EGFR mutations are (not) created equal: Focus on uncommon EGFR mutations. J. Cancer Res. Clin. Oncol. 2022, 149, 1541–1549. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Yang, H.; Jiang, T.; Li, X.; Zhao, C.; Zhang, L.; Zhao, S.; Liu, X.; Jia, Y.; Wang, Y.; et al. Uncommon EGFR mutations in a cohort of Chinese NSCLC patients and outcomes of first-line EGFR-TKIs and platinum-based chemotherapy. Chin. J. Cancer Res. 2017, 29, 543–552. [Google Scholar] [CrossRef]
- Chiu, C.H.; Yang, C.T.; Shih, J.Y.; Huang, M.S.; Su, W.C.; Lai, R.S.; Wang, C.C.; Hsiao, S.H.; Lin, Y.C.; Ho, C.L.; et al. Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitor Treatment Response in Advanced Lung Adenocarcinomas with G719X/L861Q/S768I Mutations. J. Thorac. Oncol. 2015, 10, 793–799. [Google Scholar] [CrossRef]
- Popat, S.; Hsia, T.C.; Hung, J.Y.; Jung, H.A.; Shih, J.Y.; Park, C.K.; Lee, S.H.; Okamoto, T.; Ahn, H.K.; Lee, Y.C.; et al. Tyrosine Kinase Inhibitor Activity in Patients with NSCLC Harboring Uncommon EGFR Mutations: A Retrospective International Cohort Study (UpSwinG). Oncologist 2022, 27, 255–265. [Google Scholar] [CrossRef]
- Moosavi, L.; Polineni, R. Afatinib; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Reid, A.; Vidal, L.; Shaw, H.; de Bono, J. Dual inhibition of ErbB1 (EGFR/HER1) and ErbB2 (HER2/neu). Eur. J. Cancer 2007, 43, 481–489. [Google Scholar] [CrossRef]
- Harvey, R.D.; Adams, V.R.; Beardslee, T.; Medina, P. Afatinib for the treatment of EGFR mutation-positive NSCLC: A review of clinical findings. J. Oncol. Pharm. Pract. 2020, 26, 1461–1474. [Google Scholar] [CrossRef]
- Giordano, P.; Manzo, A.; Montanino, A.; Costanzo, R.; Sandomenico, C.; Piccirillo, M.C.; Daniele, G.; Normanno, N.; Carillio, G.; Rocco, G.; et al. Afatinib: An overview of its clinical development in non-small-cell lung cancer and other tumors. Crit. Rev. Oncol. Hematol. 2016, 97, 143–151. [Google Scholar] [CrossRef]
- Solca, F.; Dahl, G.; Zoephel, A.; Bader, G.; Sanderson, M.; Klein, C.; Kraemer, O.; Himmelsbach, F.; Haaksma, E.; Adolf, G.R. Target binding properties and cellular activity of afatinib (BIBW 2992), an irreversible ErbB family blocker. J. Pharmacol. Exp. Ther. 2012, 343, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.; Sequist, L.V.; Geater, S.L.; Tsai, C.M.; Mok, T.S.; Schuler, M.; Yamamoto, N.; Yu, C.J.; Ou, S.H.; Zhou, C.; et al. Clinical activity of afatinib in patients with advanced non-small-cell lung cancer harbouring uncommon EGFR mutations: A combined post-hoc analysis of LUX-Lung 2, LUX-Lung 3, and LUX-Lung 6. Lancet Oncol. 2015, 16, 830–838. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.; Schuler, M.; Popat, S.; Miura, S.; Heeke, S.; Park, K.; Marten, A.; Kim, E.S. Afatinib for the Treatment of NSCLC Harboring Uncommon EGFR Mutations: A Database of 693 Cases. J. Thorac. Oncol. 2020, 15, 803–815. [Google Scholar] [CrossRef]
- Yang, J.C.; Schuler, M.; Popat, S.; Miura, S.; Park, K.; Passaro, A.; De Marinis, F.; Solca, F.; Marten, A.; Kim, E.S. Afatinib for the Treatment of Non-Small Cell Lung Cancer Harboring Uncommon EGFR Mutations: An Updated Database of 1023 Cases Brief Report. Front. Oncol. 2022, 12, 834704. [Google Scholar] [CrossRef]
- Hsu, P.C.; Lee, S.H.; Chiu, L.C.; Lee, C.S.; Wu, C.E.; Kuo, S.C.; Ju, J.S.; Huang, A.C.; Li, S.H.; Ko, H.W.; et al. Afatinib in Untreated Stage IIIB/IV Lung Adenocarcinoma with Major Uncommon Epidermal Growth Factor Receptor (EGFR) Mutations (G719X/L861Q/S768I): A Multicenter Observational Study in Taiwan. Target Oncol. 2023, 18, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Yang, G.; Li, W.; Li, J.; Hao, X.; Xing, P.; Yang, Y.; Wang, Y. EGFR Exon 18 Mutations in Advanced Non-Small Cell Lung Cancer: A Real-World Study on Diverse Treatment Patterns and Clinical Outcomes. Front. Oncol. 2021, 11, 713483. [Google Scholar] [CrossRef]
- Hao, Y.; Xu, M.; Zhou, H.; Si, J.; Fang, Y.; Xu, C.; Song, Z. Efficacy of EGFR-Tyrosine Kinase Inhibitors for advanced non-small cell lung cancer patients harboring rare EGFR mutations of exon 18 E709X. Med. Oncol. 2022, 40, 34. [Google Scholar] [CrossRef]
- Iwamoto, Y.; Ichihara, E.; Hara, N.; Nakasuka, T.; Ando, C.; Umeno, T.; Hirabae, A.; Maeda, Y.; Kiura, K. Efficacy of afatinib treatment for lung adenocarcinoma harboring exon 18 delE709_T710insD mutation. Jpn J. Clin. Oncol. 2019, 49, 786–788. [Google Scholar] [CrossRef]
- Ibrahim, U.; Saqib, A.; Atallah, J.P. EGFR exon 18 delE709_T710insD mutated stage IV lung adenocarcinoma with response to afatinib. Lung Cancer 2017, 108, 45–47. [Google Scholar] [CrossRef]
- An, N.; Wang, H.; Zhu, H.; Yan, W.; Jing, W.; Kong, L.; Zhang, Y.; Yu, J. Great efficacy of afatinib on a patient with lung adenocarcinoma harboring uncommon EGFR delE709_T710insD mutations: A case report. Oncol. Targets Ther. 2019, 12, 7399–7404. [Google Scholar] [CrossRef]
- Wei, Y.; Cui, Y.; Guo, Y.; Li, L.; Zeng, L. A Lung Adenocarcinoma Patient with a Rare EGFR E709_T710delinsD Mutation Showed a Good Response to Afatinib Treatment: A Case Report and Literature Review. Front. Oncol. 2021, 11, 700345. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Mitsudomi, T. Not all epidermal growth factor receptor mutations in lung cancer are created equal: Perspectives for individualized treatment strategy. Cancer Sci. 2016, 107, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Shan, B.B.; Li, Y.; Zhao, C.; An, X.Q.; Zhang, Q.M. Efficacy of EGFR-TKI sequential therapy in patients with EGFR exon 19 insertion-positive non-small-cell lung cancer: A case report. World J. Clin. Cases 2022, 10, 1883–1888. [Google Scholar] [CrossRef]
- Liang, S.K.; Ko, J.C.; Yang, J.C.; Shih, J.Y. Afatinib is effective in the treatment of lung adenocarcinoma with uncommon EGFR p.L747P and p.L747S mutations. Lung Cancer 2019, 133, 103–109. [Google Scholar] [CrossRef]
- Zhang, L.; Yang, L.; Sun, B.; Deng, Y.; Yang, J.; Wu, D.; Kong, F. Case Report: Afatinib Sensitivity in Rare EGFR E746_L747delinsIP Mutated LUAD With Peritoneal Metastases. Front. Oncol. 2022, 12, 861271. [Google Scholar] [CrossRef]
- Kanbe, M.; Sunaga, N.; Hara, K.; Sawada, H.; Wakamatsu, I.; Hara, K.; Muto, S.; Sawada, Y.; Masubuchi, H.; Sato, M.; et al. Durable response to afatinib rechallenge in a long-term survivor of non-small cell lung cancer harboring EGFR L858R and L747V mutations. Thorac. Cancer 2022, 13, 3225–3228. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.F.; Liu, P.C. Afatinib and osimertinib in lung adenocarcinoma harbored EGFR T751_I759delinsS mutation: A case report. Thorac. Cancer 2021, 12, 3429–3432. [Google Scholar] [CrossRef]
- Riess, J.W.; Gandara, D.R.; Frampton, G.M.; Madison, R.; Peled, N.; Bufill, J.A.; Dy, G.K.; Ou, S.I.; Stephens, P.J.; McPherson, J.D.; et al. Diverse EGFR Exon 20 Insertions and Co-Occurring Molecular Alterations Identified by Comprehensive Genomic Profiling of NSCLC. J. Thorac. Oncol. 2018, 13, 1560–1568. [Google Scholar] [CrossRef]
- Meador, C.B.; Sequist, L.V.; Piotrowska, Z. Targeting EGFR Exon 20 Insertions in Non-Small Cell Lung Cancer: Recent Advances and Clinical Updates. Cancer Discov. 2021, 11, 2145–2157. [Google Scholar] [CrossRef]
- Yang, G.; Li, J.; Xu, H.; Yang, Y.; Yang, L.; Xu, F.; Xia, B.; Zhu, V.W.; Nagasaka, M.; Yang, Y.; et al. EGFR exon 20 insertion mutations in Chinese advanced non-small cell lung cancer patients: Molecular heterogeneity and treatment outcome from nationwide real-world study. Lung Cancer 2020, 145, 186–194. [Google Scholar] [CrossRef]
- Qin, Y.; Jian, H.; Tong, X.; Wu, X.; Wang, F.; Shao, Y.W.; Zhao, X. Variability of EGFR exon 20 insertions in 24 468 Chinese lung cancer patients and their divergent responses to EGFR inhibitors. Mol. Oncol. 2020, 14, 1695–1704. [Google Scholar] [CrossRef] [PubMed]
- Zochbauer-Muller, S.; Kaserer, B.; Prosch, H.; Cseh, A.; Solca, F.; Bauer, M.J.; Mullauer, L. Case Report: Afatinib Treatment in a Patient with NSCLC Harboring a Rare EGFR Exon 20 Mutation. Front. Oncol. 2020, 10, 593852. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Wu, X.; Yan, S.; Zhu, Y.; Yan, Z.; Lv, D.; Ge, H. Response to Afatinib in a Patient with NSCLC Harboring Novel EGFR Exon 20 Insertion Mutations. Oncol. Targets Ther. 2020, 13, 9753–9757. [Google Scholar] [CrossRef]
- Chan, R.T. Afatinib for an EGFR exon 20 insertion mutation: A case report of progressive stage IV metastatic lung adenocarcinoma with 54 months’ survival. Asia Pac. J. Clin. Oncol. 2018, 14 (Suppl. S1), 7–9. [Google Scholar] [CrossRef] [PubMed]
- Urban, L.; Doczi, R.; Vodicska, B.; Tihanyi, D.; Horvath, M.; Kormos, D.; Takacs, I.; Papai-Szekely, Z.; Poka-Farkas, Z.; Varkondi, E.; et al. Major Clinical Response to Afatinib Monotherapy in Lung Adenocarcinoma Harboring EGFR Exon 20 Insertion Mutation. Clin. Lung Cancer 2021, 22, e112–e115. [Google Scholar] [CrossRef]
- Cai, Y.; Wang, X.; Guo, Y.; Sun, C.; Xu, Y.; Qiu, S.; Ma, K. Successful treatment of a lung adenocarcinoma patient with a novel EGFR exon 20-ins mutation with afatinib: A case report. Medicine 2019, 98, e13890. [Google Scholar] [CrossRef]
- Oyamada, Y.; Wada, S.; Fujimoto, K. A Case of Advanced Lung Adenocarcinoma Harboring an Epidermal Growth Factor Receptor(EGFR) Exon 20 Insertion, D770_N771insSVD. Gan Kagaku Ryoho 2021, 48, 845–847. [Google Scholar]
- Van Veggel, B.; de Langen, A.J.; Hashemi, S.M.S.; Monkhorst, K.; Heideman, D.A.M.; Thunnissen, E.; Smit, E.F. Afatinib and Cetuximab in Four Patients with EGFR Exon 20 Insertion-Positive Advanced NSCLC. J. Thorac. Oncol. 2018, 13, 1222–1226. [Google Scholar] [CrossRef]
- Hasegawa, H.; Yasuda, H.; Hamamoto, J.; Masuzawa, K.; Tani, T.; Nukaga, S.; Hirano, T.; Kobayashi, K.; Manabe, T.; Terai, H.; et al. Efficacy of afatinib or osimertinib plus cetuximab combination therapy for non-small-cell lung cancer with EGFR exon 20 insertion mutations. Lung Cancer 2019, 127, 146–152. [Google Scholar] [CrossRef]
- Chang, J.W.; Huang, C.Y.; Fang, Y.F.; Chang, C.F.; Yang, C.T.; Kuo, C.S.; Hsu, P.C.; Wu, C.E. Epidermal growth factor receptor tyrosine kinase inhibitors for de novo T790M mutation: A retrospective study of 44 patients. Thorac. Cancer 2022, 13, 1888–1897. [Google Scholar] [CrossRef]
- Hochmair, M.J.; Buder, A.; Schwab, S.; Burghuber, O.C.; Prosch, H.; Hilbe, W.; Cseh, A.; Fritz, R.; Filipits, M. Liquid-Biopsy-Based Identification of EGFR T790M Mutation-Mediated Resistance to Afatinib Treatment in Patients with Advanced EGFR Mutation-Positive NSCLC, and Subsequent Response to Osimertinib. Target. Oncol 2019, 14, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Liu, Q.; Cao, L.; Sun, W.; Gu, X.; Liu, B.; Xiao, N.; Teng, F.; Li, X.; Chen, M.; et al. Osimertinib versus afatinib in patients with T790M-positive, non-small-cell lung cancer and multiple central nervous system metastases after failure of initial EGFR-TKI treatment. BMC Pulm. Med. 2021, 21, 172. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro Gomes, J.; Cruz, M.R. Combination of afatinib with cetuximab in patients with EGFR-mutant non-small-cell lung cancer resistant to EGFR inhibitors. Oncol. Targets Ther. 2015, 8, 1137–1142. [Google Scholar] [CrossRef]
- Kudo, K.; Ohashi, K.; Makimoto, G.; Higo, H.; Kato, Y.; Kayatani, H.; Kurata, Y.; Takami, Y.; Minami, D.; Ninomiya, T.; et al. Triplet therapy with afatinib, cetuximab, and bevacizumab induces deep remission in lung cancer cells harboring EGFR T790M in vivo. Mol. Oncol. 2017, 11, 670–681. [Google Scholar] [CrossRef] [PubMed]
- Long, X.; Qin, T.; Lin, J. Great Efficacy of Afatinib in a Patient with Lung Adenocarcinoma Harboring EGFR L833V/H835L Mutations: A Case Report. Oncol. Targets Ther. 2020, 13, 10689–10692. [Google Scholar] [CrossRef]
- Qin, B.D.; Jiao, X.D.; Yuan, L.Y.; Liu, K.; Wang, Z.; Qin, W.X.; Zang, Y.S. The effectiveness of afatinib and osimertinib in a Chinese patient with advanced lung adenocarcinoma harboring a rare triple EGFR mutation (R670W/H835L/L833V): A case report and literature review. Oncol. Targets Ther. 2018, 11, 4739–4745. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.W.; Huang, C.Y.; Fang, Y.F.; Chang, C.F.; Yang, C.T.; Kuo, C.S.; Hsu, P.C.; Wu, C.E. Epidermal growth factor receptor tyrosine kinase inhibitors for non-small cell lung cancer harboring uncommon EGFR mutations: Real-world data from Taiwan. Thorac. Cancer 2023, 14, 12–23. [Google Scholar] [CrossRef]
- Kim, M.H.; Choi, C.M.; Lee, S.Y.; Park, C.K.; Chang, Y.S.; Lee, K.Y.; Kim, S.J.; Yang, S.H.; Ryu, J.S.; Lee, J.E.; et al. First-line Afatinib in Patients with Non-small-cell Lung Cancer with Uncommon EGFR Mutations in South Korea. Anticancer Res. 2022, 42, 1615–1622. [Google Scholar] [CrossRef]
- Starrett, J.H.; Guernet, A.A.; Cuomo, M.E.; Poels, K.E.; van Alderwerelt van Rosenburgh, I.K.; Nagelberg, A.; Farnsworth, D.; Price, K.S.; Khan, H.; Ashtekar, K.D.; et al. Drug Sensitivity and Allele Specificity of First-Line Osimertinib Resistance EGFR Mutations. Cancer Res. 2020, 80, 2017–2030. [Google Scholar] [CrossRef]
- Liu, Y.; Li, Y.; Ou, Q.; Wu, X.; Wang, X.; Shao, Y.W.; Ying, J. Acquired EGFR L718V mutation mediates resistance to osimertinib in non-small cell lung cancer but retains sensitivity to afatinib. Lung Cancer 2018, 118, 1–5. [Google Scholar] [CrossRef]
- Fassunke, J.; Muller, F.; Keul, M.; Michels, S.; Dammert, M.A.; Schmitt, A.; Plenker, D.; Lategahn, J.; Heydt, C.; Bragelmann, J.; et al. Overcoming EGFR(G724S)-mediated osimertinib resistance through unique binding characteristics of second-generation EGFR inhibitors. Nat. Commun. 2018, 9, 4655. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.P.; Zhang, Y.K.; Westover, D.; Yan, Y.; Qiao, H.; Huang, V.; Du, Z.; Smith, J.A.; Ross, J.S.; Miller, V.A.; et al. On-target Resistance to the Mutant-Selective EGFR Inhibitor Osimertinib Can Develop in an Allele-Specific Manner Dependent on the Original EGFR-Activating Mutation. Clin. Cancer Res. 2019, 25, 3341–3351. [Google Scholar] [CrossRef]
- Fang, W.; Gan, J.; Huang, Y.; Zhou, H.; Zhang, L. Acquired EGFR L718V Mutation and Loss of T790M-Mediated Resistance to Osimertinib in a Patient with NSCLC Who Responded to Afatinib. J. Thorac. Oncol. 2019, 14, e274–e275. [Google Scholar] [CrossRef] [PubMed]
- Song, Z.; Ren, G.; Wang, X.; Du, H.; Sun, Y.; Hu, L. Durable clinical benefit from afatinib in a lung adenocarcinoma patient with acquired EGFR L718V mutation-mediated resistance towards osimertinib: A case report and literature review. Ann. Palliat. Med. 2022, 11, 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Qin, J.; Xie, F.; Gong, L.; Han, N.; Lu, H. L718Q/V mutation in exon 18 of EGFR mediates resistance to osimertinib: Clinical features and treatment. Discov. Oncol. 2022, 13, 72. [Google Scholar] [CrossRef]
- Wei, Y.; Jiang, B.; Liu, S.; Zhang, Z.; Fang, W.; Yang, Y.; Li, X.; Zhao, J.; Zhao, H. Afatinib as a Potential Therapeutic Option for Patients with NSCLC With EGFR G724S. JTO Clin. Res. Rep. 2021, 2, 100193. [Google Scholar] [CrossRef]
- Cortiula, F.; Pelizzari, G.; Corvaja, C.; De Maglio, G.; Fasola, G. Non-small cell lung cancer harboring EGFR G724S mutation and exon 19 deletion responded to afatinib monotherapy after multiple lines of target therapies. Anticancer Drugs 2022, 33, 960–962. [Google Scholar] [CrossRef]
- Fang, W.; Huang, Y.; Gan, J.; Zheng, Q.; Zhang, L. Emergence of EGFR G724S After Progression on Osimertinib Responded to Afatinib Monotherapy. J. Thorac. Oncol. 2020, 15, e36–e37. [Google Scholar] [CrossRef]
- Sini, C.; Tuzi, A.; Rossi, G.; Russo, A.; Pezzuto, A. Acquired resistance in oncogene-addicted non-small-cell lung cancer. Future Oncol. 2018, 14, 29–40. [Google Scholar] [CrossRef]
- Qin, Y.; Long, Y.; Tang, Y.; Tian, Y.; Li, J.; Duan, P.; Luo, J.; Yu, M.; Li, Y.; Zhou, X.; et al. Real-world clinical analysis in 190 advanced NSCLC patients with uncommon EGFR mutations: A multi-center study. Cancer Sci. 2023, 1–8. [Google Scholar] [CrossRef]
- Pang, L.L.; Gan, J.D.; Tan, J.R.; Huang, Y.H.; Liao, J.; Liang, W.T.; Deng, P.B.; Fang, W.F. Efficacy and potential resistance mechanisms of afatinib in advanced non-small cell lung cancer patients with EGFR G719X/L861Q/S768I. Cancer 2022, 128, 3804–3814. [Google Scholar] [CrossRef] [PubMed]
- Li, H.S.; Wang, S.Z.; Xu, H.Y.; Yan, X.; Zhang, J.Y.; Lei, S.Y.; Li, T.; Hao, X.Z.; Zhang, T.; Yang, G.J.; et al. Afatinib and Dacomitinib Efficacy, Safety, Progression Patterns, and Resistance Mechanisms in Patients with Non-Small Cell Lung Cancer Carrying Uncommon EGFR Mutations: A Comparative Cohort Study in China (AFANDA Study). Cancers 2022, 14, 5307. [Google Scholar] [CrossRef] [PubMed]
- Bar, J.; Peled, N.; Schokrpur, S.; Wolner, M.; Rotem, O.; Girard, N.; Aboubakar Nana, F.; Derijcke, S.; Kian, W.; Patel, S.; et al. UNcommon EGFR Mutations: International Case Series on Efficacy of Osimertinib in Real-Life Practice in First-LiNe Setting (UNICORN). J. Thorac. Oncol. 2023, 18, 169–180. [Google Scholar] [CrossRef]
- Cho, J.H.; Lim, S.H.; An, H.J.; Kim, K.H.; Park, K.U.; Kang, E.J.; Choi, Y.H.; Ahn, M.S.; Lee, M.H.; Sun, J.M.; et al. Osimertinib for Patients with Non-Small-Cell Lung Cancer Harboring Uncommon EGFR Mutations: A Multicenter, Open-Label, Phase II Trial (KCSG-LU15-09). J. Clin. Oncol. 2020, 38, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Brindel, A.; Althakfi, W.; Barritault, M.; Watkin, E.; Maury, J.M.; Bringuier, P.P.; Girard, N.; Brevet, M. Uncommon EGFR mutations in lung adenocarcinoma: Features and response to tyrosine kinase inhibitors. J. Thorac. Dis. 2020, 12, 4643–4650. [Google Scholar] [CrossRef]
- Li, H.; Wang, C.; Wang, Z.; Hu, Y.; Zhang, G.; Zhang, M.; Zheng, X.; Zhang, X.; Yang, J.; Ma, Z.; et al. Efficacy and long-term survival of advanced lung adenocarcinoma patients with uncommon EGFR mutations treated with 1st generation EGFR-TKIs compared with chemotherapy as first-line therapy. Lung Cancer 2019, 130, 42–49. [Google Scholar] [CrossRef]
- Yamada, T.; Hirai, S.; Katayama, Y.; Yoshimura, A.; Shiotsu, S.; Watanabe, S.; Kikuchi, T.; Hirose, K.; Kubota, Y.; Chihara, Y.; et al. Retrospective efficacy analysis of immune checkpoint inhibitors in patients with EGFR-mutated non-small cell lung cancer. Cancer Med. 2019, 8, 1521–1529. [Google Scholar] [CrossRef]


{kind=link}
| Study | n | Mutation | Tumor Staging | Therapy Line | Response | PFS (mos) (95% CI) | OS (mos) (95% CI) |
|---|---|---|---|---|---|---|---|
| Hao Y., 2022 [18] | 11 | E709A/G/K, E709-T710delinsD | IV | first or above | N/A | 13.5 | 17.1 |
| Iwamoto Y., 2019 [19] | 1 | E709-T710delinsD | IV | sixth | PR | 7 | N.R. |
| Ibrahim U., 2017 [20] | 1 | E709-T710delinsD | IV | first | PR | N.R. | N.R. |
| An N., 2019 [21] | 1 | E709-T710delinsD | IIIA | second | PR | 11 | >21 |
| Wei Y., 2021 [22] | 1 | E709-T710delinsD | IIB | first | PR | 23 | N.R. |
| Study | n | Mutation | Tumor Staging | Therapy Line | ORR (%) | Response | PFS (mos) (95% CI) | OS (mos) (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Liang S.K., 2019 [25] | 5 | L747S or L747P | IV | first | 80 | N/A | 11.97 (6.37–17.57) | 16.62 (3.05–30.19) |
| Shan B.B., 2022 [24] | 1 | I740_K745dup | IV | second | 0 | SD | 13.4 | 21.3 |
| Zhang L., 2022 [26] | 1 | E746_L747delinsIP | IV | fourth | 100 | PR | >6.5 | N.R. |
| Kanbe M., 2022 [27] | 1 | L747V and 21 L858R | IV | sixth | 100 | PR | 12 | N.R. |
| Fang Y.F., 2021 [28] | 1 | T751_I759delinsS | IV | second | 100 | PR | 9 | N.R. |
| Study | n | Mutation | ORR (%) | TTF (mos) (95% CI) |
|---|---|---|---|---|
| Yang J.C., 2022 [15] | 42 | Overall | 33 | 9.1 (7.4–14.2) |
| 4 | A763_Y764insFQEA; A763_V765dup | 50 | 39.0 (8.2–39.0) | |
| 5 | A767_S768insSVA; _V769dup/ASV; insASVD | 0 | 3.7 (1.0–36.0) | |
| 3 | D770_N771insGL/SVD | 0 | 3.8 (3.0–20.1) | |
| 9 | H773_R776insYNPY; _V774dup/insH; dup | 0 | 24.0 (6.1–NE) | |
| 2 | M766delinsMATL; insASV | 100 | 12.9 (11.6–14.2) | |
| 7 | N771_H773dup; _772insPHGH; delinsKG; _P772insGY | 71 | 10.0 (5.2–NE) | |
| 5 | S768_D770dup | 0 | 8.5 (NE–NE) | |
| 7 | V769_770INSV; _D770insASV/GVV | 75 | 8.0 (1.2–14.3) |
| Study | n | Mutation | Tumor Staging | Therapy Line | ORR (%) | Response | PFS (mos) (95% CI) |
|---|---|---|---|---|---|---|---|
| Zochbauer-Muller S., 2020 [33] | 1 | H773dup | N.R. | first | 0 | SD | >54 |
| Lin L., 2020 [34] | 1 | N771delinsKG | IV | first | 100 | PR | 10 |
| Chan R.T., 2018 [35] | 1 | A767_S768insSVA | IV | third | 0 | SD | 36 |
| Cai Y., 2019 [37] | 1 | A767delinsASVD | IV | second | 0 | SD | 7.4 |
| Urban L., 2021 [36] | 1 | H773_V774insNPH | IV | second | 100 | PR | >36 |
| Oyamada Y., 2021 [38] | 1 | D770_N771insSVD | IV | fourth | 100 | PR | N/A |
| van Veggel B., 2018 (with cetuximab) [39] | 4 | Overall | IV | second/ third | 75 | N/A | 5.4 (0.0–14.2) |
| 1 | S768_A770dup | second | 100 | PR | 17.6 | ||
| 1 | A771_H773dup | second | 100 | PR | 4.4 | ||
| 1 | H773dup | third | 0 | SD | 2.7 | ||
| 1 | A767_V769dup | third | 100 | PR | >6.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, Y.; Fang, X.; Xiang, Y.; Fang, T.; Liu, J.; Lu, K. Afatinib for the Treatment of NSCLC with Uncommon EGFR Mutations: A Narrative Review. Curr. Oncol. 2023, 30, 5337-5349. https://doi.org/10.3390/curroncol30060405
Jiang Y, Fang X, Xiang Y, Fang T, Liu J, Lu K. Afatinib for the Treatment of NSCLC with Uncommon EGFR Mutations: A Narrative Review. Current Oncology. 2023; 30(6):5337-5349. https://doi.org/10.3390/curroncol30060405
Chicago/Turabian StyleJiang, Yingying, Xiaoxu Fang, Yan Xiang, Tingwen Fang, Jingwen Liu, and Kaihua Lu. 2023. "Afatinib for the Treatment of NSCLC with Uncommon EGFR Mutations: A Narrative Review" Current Oncology 30, no. 6: 5337-5349. https://doi.org/10.3390/curroncol30060405