Real-World Outcomes of Stage IV NSCLC with PD-L1 ≥ 50% Treated with First-Line Pembrolizumab: Uptake of Second-Line Systemic Therapy

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Population
2.2. Statistical Analysis
2.3. Ethics Statement
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Cancer Facts & Figures 2020; American Cancer Society: Atlanta, GA, USA, 2020; pp. 1–76. [Google Scholar]
- Duma, N.; Santana-Davila, R.; Molina, J.R. Non–Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin. Proc. 2019, 94, 1623–1640. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; de Marinis, F.; Dediu, M.; Thomas, M.; Pujol, J.L.; Bidoli, P.; Molinier, O.; Sahoo, T.P.; Laack, E.; Reck, M.; et al. Maintenance therapy with pemetrexed plus best supportive care versus placebo plus best supportive care after induction therapy with pemetrexed plus cisplatin for advanced non-squamous non-small-cell lung cancer (PARAMOUNT): A double-blind, phase 3, random. Lancet Oncol. 2012, 13, 247–255. [Google Scholar] [CrossRef]
- Solomon, B.J.; Mok, T.; Kim, D.W.; Wu, Y.L.; Nakagawa, K.; Mekhail, T.; Felip, E.; Cappuzzo, F.; Paolini, J.; Usari, T.; et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 2014, 371, 2167–2177. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv192–iv237. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated analysis of KEYNOTE-024: Pembrolizumab versus platinum-based chemotherapy for advanced non–small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csöszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Five-Year Outcomes with Pembrolizumab Versus Chemotherapy for Metastatic Non–Small-Cell Lung Cancer with PD-L1 Tumor Proportion Score ‡ 50%. J. Clin. Oncol. 2021, 39, 2339–2349. [Google Scholar] [CrossRef]
- Herbst, R.S.; Giaccone, G.; de Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for First-Line Treatment of PD-L1–Selected Patients with NSCLC. N. Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef]
- Sezer, A.; Kilickap, S.; Gümüş, M.; Bondarenko, I.; Özgüroğlu, M.; Gogishvili, M.; Turk, H.M.; Cicin, I.; Bentsion, D.; Gladkov, O.; et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: A multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet 2021, 397, 592–604. [Google Scholar] [CrossRef]
- Akinboro, O.; Vallejo, J.J.; Nakajima, E.C.; Ren, Y.; Mishra-Kalyani, P.S.; Larkins, E.A.; Vellanki, P.J.; Drezner, N.L.; Mathieu, L.N.; Donoghue, M.B.; et al. Outcomes of anti–PD-(L)1 therapy with or without chemotherapy (chemo) for first-line (1L) treatment of advanced non–small cell lung cancer (NSCLC) with PD-L1 score ≥ 50%: FDA pooled analysis. J. Clin. Oncol. 2022, 40, 9000. [Google Scholar] [CrossRef]
- Nadler, E.; Espirito, J.L.; Pavilack, M.; Boyd, M.; Vergara-Silva, A.; Fernandes, A. Treatment Patterns and Clinical Outcomes Among Metastatic Non–Small-Cell Lung Cancer Patients Treated in the Community Practice Setting. Clin. Lung Cancer 2018, 19, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, R.; Mezquita, L.; Texier, M.; Lahmar, J.; Audigier-Valette, C.; Tessonnier, L.; Mazieres, J.; Zalcman, G.; Brosseau, S.; Le Moulec, S.; et al. Comparison of Fast-Progression, Hyperprogressive Disease, and Early Deaths in Advanced Non–Small-Cell Lung Cancer Treated with PD-1/PD-L1 Inhibitors or Chemotherapy. JCO Precis. Oncol. 2020, 4, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Velcheti, V.; Hu, X.; Yang, L.; Pietanza, M.C.; Burke, T. Long-Term Real-World Outcomes of First-Line Pembrolizumab Monotherapy for Metastatic Non-Small Cell Lung Cancer with ≥50% Expression of Programmed Cell Death-Ligand 1. Front. Oncol. 2022, 12, 834761. [Google Scholar] [CrossRef]
- Cortellini, A.; Cannita, K.; Tiseo, M.; Cortinovis, D.L.; Aerts, J.G.J.V.; Baldessari, C.; Giusti, R.; Ferrara, M.G.; D’Argento, E.; Grossi, F.; et al. Post-progression outcomes of NSCLC patients with PD-L1 expression ≥50% receiving first-line single-agent pembrolizumab in a large multicentre real-world study. Eur. J. Cancer 2021, 148, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.; Ramsden, K.; Zhai, Y.; Murray, N.; Sun, S.; Melosky, B.; Laskin, J. Less toxic chemotherapy improves uptake of all lines of chemotherapy in advanced non-small-cell lung cancer: 10-year retrospective population-based review. J. Thorac. Oncol. 2014, 9, 1180–1186. [Google Scholar] [CrossRef]
- Park, K.; Bennouna, J.; Boyer, M.; Hida, T.; Hirsh, V.; Kato, T.; Lu, S.; Mok, T.; Nakagawa, K.; O’Byrne, K.; et al. Sequencing of therapy following first-line afatinib in patients with EGFR mutation-positive non-small cell lung cancer. Lung Cancer 2019, 132, 126–131. [Google Scholar] [CrossRef]
- Frost, N.; Kollmeier, J.; Misch, D.; Vollbrecht, C.; Grah, C.; Matthes, B.; Pultermann, D.; Olive, E.; Raspe, M.; Ochsenreither, S.; et al. Pembrolizumab as First-Line Palliative Therapy in PD-L1 Overexpressing (≥50%) NSCLC: Real-world Results with Special Focus on PS ≥2, Brain Metastases, and Steroids. Clin. Lung Cancer 2021, 22, 411–422. [Google Scholar] [CrossRef]
- Cortellini, A.; Tiseo, M.; Banna, G.L.; Cappuzzo, F.; Aerts, J.G.J.V.; Barbieri, F.; Giusti, R.; Bria, E.; Cortinovis, D.; Grossi, F.; et al. Clinicopathologic correlates of first-line pembrolizumab effectiveness in patients with advanced NSCLC and a PD-L1 expression of ≥50%. Cancer Immunol. Immunother. 2020, 69, 2209–2221. [Google Scholar] [CrossRef]
- Friedlaender, A.; Metro, G.; Signorelli, D.; Gili, A.; Economopoulou, P.; Roila, F.; Banna, G.; De Toma, A.; Camerini, A.; Christopoulou, A.; et al. Impact of performance status on non-small-cell lung cancer patients with a PD-L1 tumour proportion score ≥50% treated with front-line pembrolizumab. Acta Oncol. 2020, 59, 1058–1063. [Google Scholar] [CrossRef]
- Passaro, A.; Spitaleri, G.; Gyawali, B.; de Marinis, F. Immunotherapy in non–small-cell lung cancer patients with performance status 2: Clinical decision making with scant evidence. J. Clin. Oncol. 2019, 37, 1863–1867. [Google Scholar] [CrossRef]
- Lee, S.M.; Schulz, C.; Prabhash, K.; Han, B.; Szczesna, A.; Cortinovis, D.L.; Rittmeyer, A.; Al, E. IPSOS: Results from a phase III study of first-line (1L) atezolizumab (atezo) vs. single-agent chemotherapy (chemo) in patients (pts) with NSCLC not eligible for a platinum-containing regimen. ESMO 2022, 33, S1418–S1419. [Google Scholar] [CrossRef]
- Jodai, T.; Saruwatari, K.; Ikeda, T.; Moriyama, E.; Kashiwabara, K.; Shingu, N.; Iyonaga, K.; Inaba, M.; Ajishi, Y.; Honda, C.; et al. Clinical outcomes and predictive value of programmed cell death-ligand 1 expression in response to anti-programmed cell death 1/ligand 1 antibodies in non-small cell lung cancer patients with performance status 2 or greater. Int. J. Clin. Oncol. 2021, 26, 78–86. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
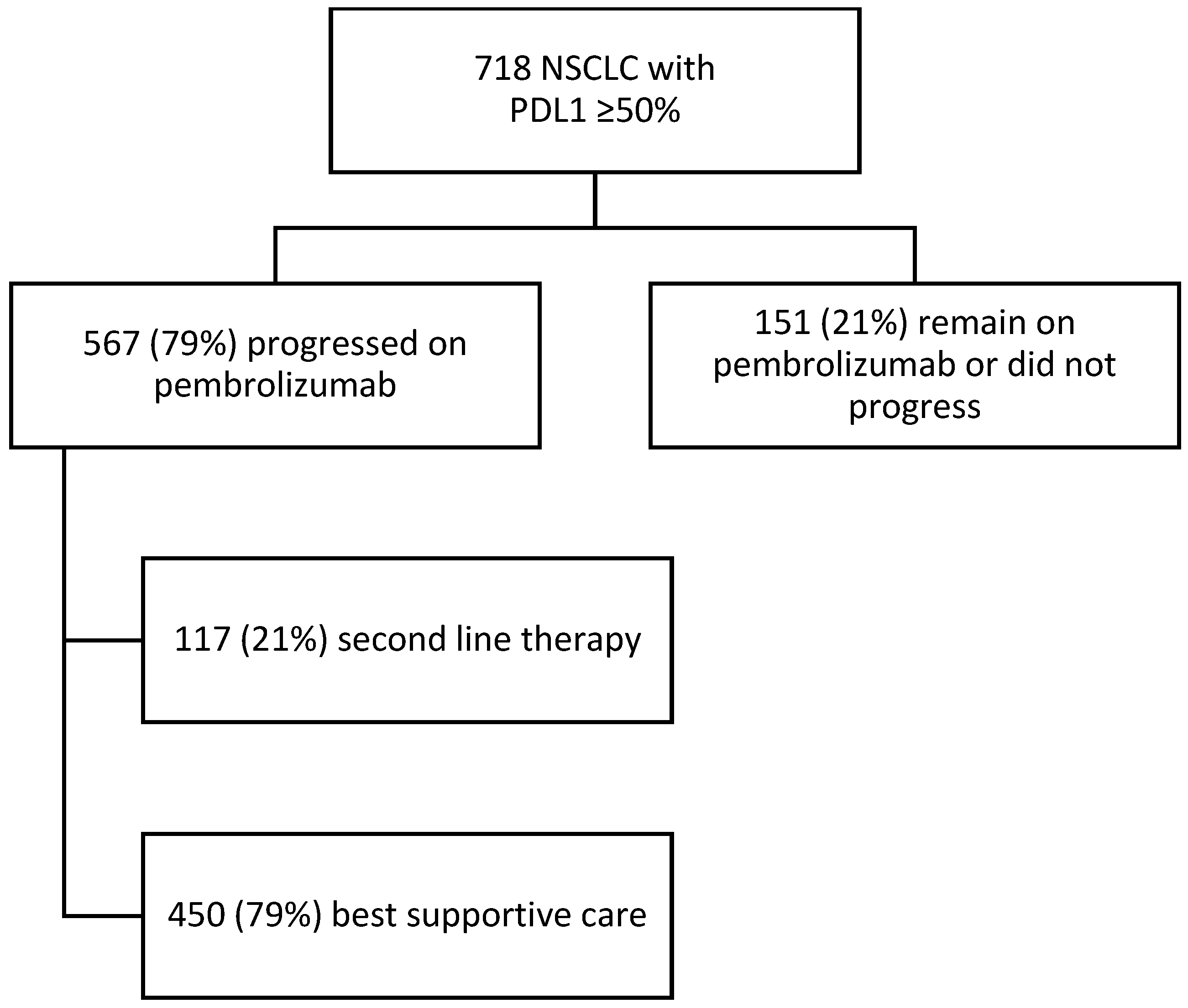
| N (%) | Overall (n = 718) | Patients with Progression (n = 567) | Progression Followed by Second Line Therapy (n = 118) | Progression Followed by BSC (n = 449) | p-Value for Second Line Treatment Versus BSC |
|---|---|---|---|---|---|
| Age (median), years | 70 | 70 | 67 | 71 | <0.001 |
| Sex | |||||
| Male | 331 (46%) | 260 (46%) | 51 (43%) | 209 (47%) | |
| Female | 387 (54%) | 307 (54%) | 67 (57%) | 240 (53%) | 0.519 |
| Histology | |||||
| Non-Squamous | 573 (80%) | 437 (77%) | 97 (82%) | 340 (76%) | |
| Squamous | 145 (20%) | 130 (23%) | 21 (18%) | 109 (24%) | 0.136 |
| Smoking Status | |||||
| Never | 44 (6%) | 40 (7%) | 12 (10%) | 28 (6%) | |
| Former | 521 (73%) | 410 (72%) | 82 (70%) | 328 (73%) | |
| Active | 132 (18%) | 103 (18%) | 20 (17%) | 83 (19%) | |
| Unknown | 21 (3%) | 14 (3%) | 4 (3%) | 10 (2%) | 0.416 |
| Smoking years (median) | 40 | 40 | 35 | 40 | 0.217 |
| Baseline ECOG PS | |||||
| 0–1 | 436 (61%) | ||||
| ≥2 | 280 (39%) | 324 (57%) | 90 (76%) | 234 (52%) | |
| Unknown | 2 (<1%) | 243 (43%) | 28 (24%) | 215 (48%) | <0.001 |
| CNS Metastases | 65 (9%) | 56 (10%) | 10 (9%) | 46 (10%) | 0.566 |
| Mutation (tested n = 600) | |||||
| KRAS | 110 (32%) | 80 (30%) | 18 (31%) | 62 (30%) | |
| BRAF | 15 (4%) | 12 (5%) | 1 (2%) | 11 (5%) | |
| KRAS and BRAF | 4 (1%) | 2 (1%) | 0 (0%) | 2 (1%) | |
| Other | 8 (2%) | 6 (2%) | 2 (3%) | 4 (2%) | 0.672 |
| Median duration pembrolizumab treatment, months (IQR) | 4.44 (1.38–12.92) | 2.99 (0.69–7.23) | 5.37 (2.76–11.59) | 2.63 (0.69–6.31) | <0.001 |
| OR (95% CI) Multivariate Analysis | p-Value | |
|---|---|---|
| Age | 0.949 (0.927–0.972) | <0.001 |
| ECOG PS 0–1 versus ≥ 2 | 2.591 (1.610–4.167) | <0.001 |
| Duration of Pembrolizumab | 1.053 (1.023–1.085) | <0.001 |
| HR (95% CI) Univariate Analysis | p-Value | HR (95% CI) Multivariate Analysis | p-Value | |
|---|---|---|---|---|
| Age | 1.001 (0.991–1.011) | 0.872 | 0.997 (0.987–1.007) | 0.520 |
| Sex | ||||
| Female versus Male | 1.071 (0.888–1.291) | 0.473 | 1.041 (0.863–1.256) | 0.675 |
| ECOG PS | ||||
| 0–1 versus ≥ 2 | 1.894 (1.567–2.229) | <0.001 | 1.892 (1.562–2.291) | <0.001 |
| 0–1 versus unknown | 1.336 (0.728–2.45) | 0.349 | 1.459 (0.790–2.695) | 0.227 |
| Pembrolizumab schedule | ||||
| Q3W versus Q6W | 0.616 (0.368–1.032) | 0.066 | 0.637 (0.378–1.072) | 0.089 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rittberg, R.; Leung, B.; Shokoohi, A.; Pender, A.; Wong, S.; Al-Hashami, Z.; Wang, Y.; Ho, C. Real-World Outcomes of Stage IV NSCLC with PD-L1 ≥ 50% Treated with First-Line Pembrolizumab: Uptake of Second-Line Systemic Therapy. Curr. Oncol. 2023, 30, 5299-5308. https://doi.org/10.3390/curroncol30060402
Rittberg R, Leung B, Shokoohi A, Pender A, Wong S, Al-Hashami Z, Wang Y, Ho C. Real-World Outcomes of Stage IV NSCLC with PD-L1 ≥ 50% Treated with First-Line Pembrolizumab: Uptake of Second-Line Systemic Therapy. Current Oncology. 2023; 30(6):5299-5308. https://doi.org/10.3390/curroncol30060402
Chicago/Turabian StyleRittberg, Rebekah, Bonnie Leung, Aria Shokoohi, Alexandra Pender, Selina Wong, Zamzam Al-Hashami, Ying Wang, and Cheryl Ho. 2023. "Real-World Outcomes of Stage IV NSCLC with PD-L1 ≥ 50% Treated with First-Line Pembrolizumab: Uptake of Second-Line Systemic Therapy" Current Oncology 30, no. 6: 5299-5308. https://doi.org/10.3390/curroncol30060402