One-Step Robot-Assisted Complete Urinary Tract Extirpation in Man with End-Stage Renal Disease on Dialysis: The First Case Report


Abstract
:Simple Summary
Abstract
1. Introduction
2. Case
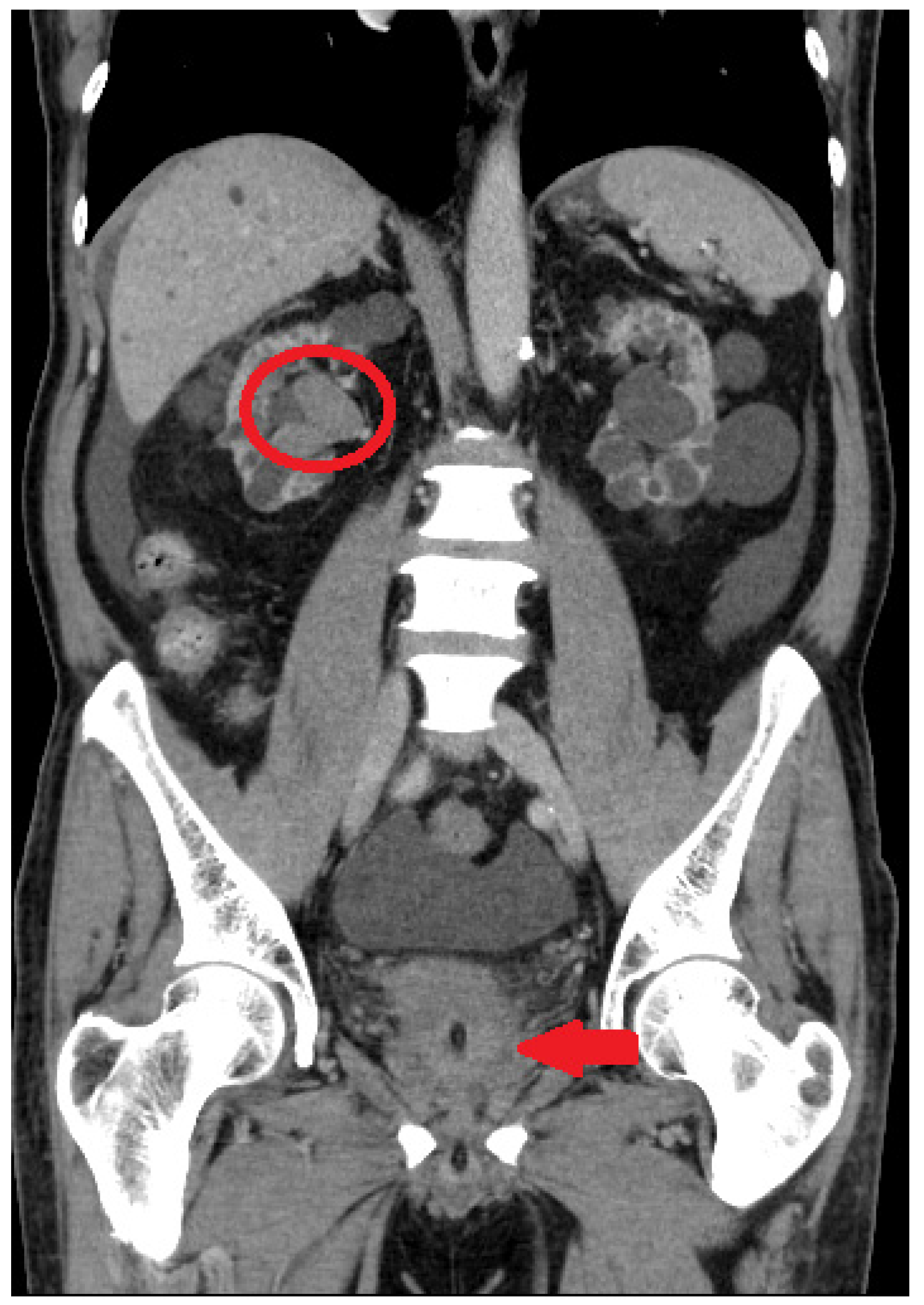
2.1. Initial Assessment
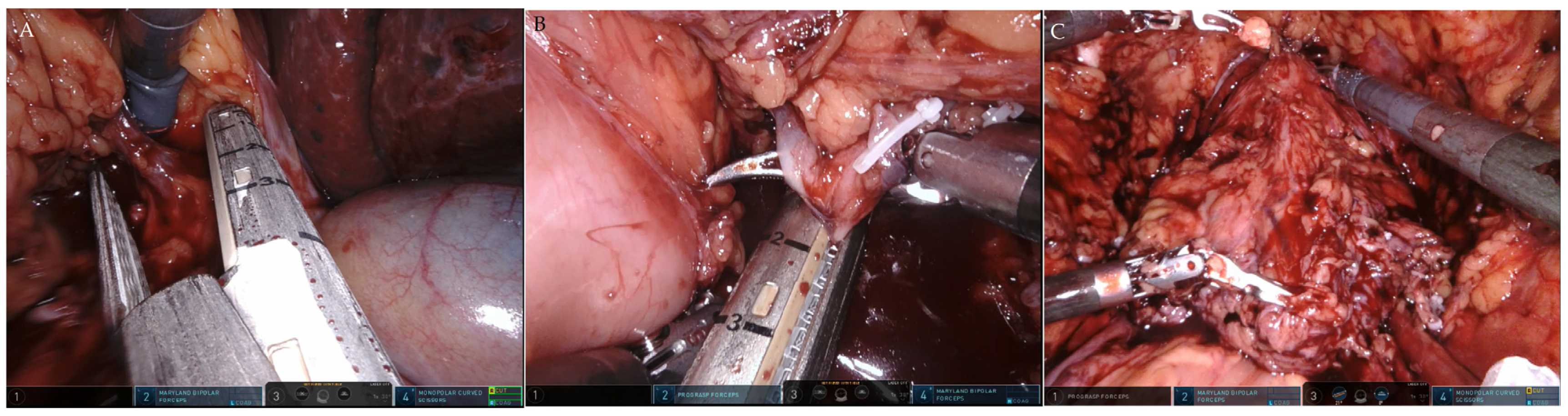
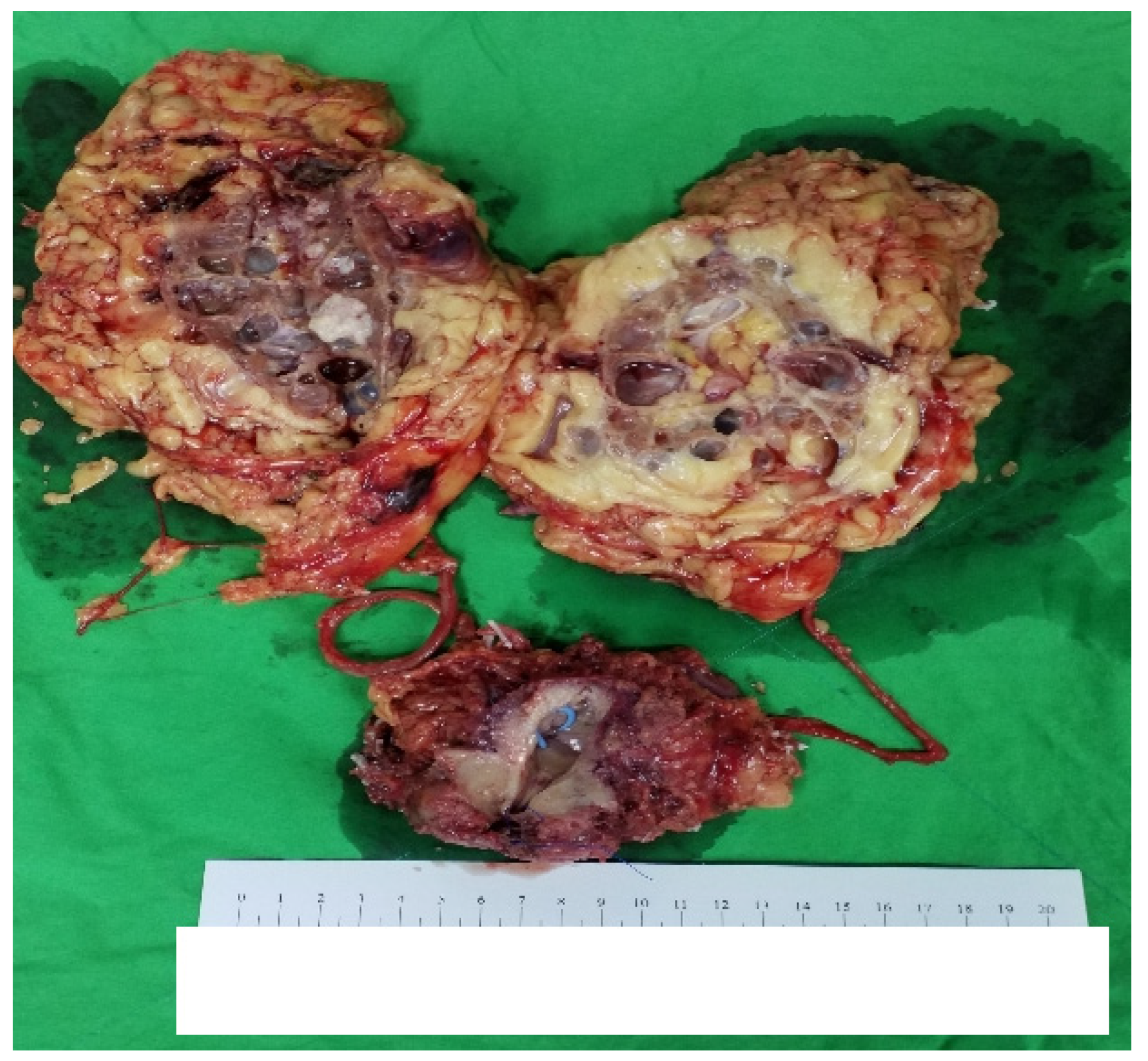
2.2. Robot-Assisted CUTE
2.3. Postoperative Care and Follow-Up
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Green, D.A.; Rink, M.; Xylinas, E.; Matin, S.F.; Stenzl, A.; Roupret, M.; Karakiewicz, P.I.; Scherr, D.; Shariat, S.F. Urothelial carcinoma of the bladder and the upper tract: Disparate twins. J. Urol. 2013, 189, 1214–1221. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.H.; Weng, W.C.; Ou, Y.C.; Lin, Y.S.; Huang, L.H.; Lu, C.H.; Tsao, T.Y.; Hsu, C.Y.; Tung, M.C. Diffusive Ki67 and vimentin are associated with worse recurrence-free survival of upper tract urothelial carcinoma: A retrospective cohort study from bench to bedside. Urol. Oncol. 2022, 40, e21–e109. [Google Scholar] [CrossRef] [PubMed]
- Palou, J.; Rodríguez-Rubio, F.; Huguet, J.; Segarra, J.; Ribal, M.J.; Alcaraz, A.; Villavicencio, H. Multivariate analysis of clinical parameters of synchronous primary superficial bladder cancer and upper urinary tract tumor. J. Urol. 2005, 174, 859–861. [Google Scholar] [CrossRef] [PubMed]
- Flaig, T.W.; Spiess, P.E.; Agarwal, N.; Bangs, R.; Boorjian, S.A.; Buyyounouski, M.K.; Chang, S.; Downs, T.M.; Efstathiou, J.A.; Friedlander, T.; et al. Bladder Cancer, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2020, 18, 329–354. [Google Scholar] [CrossRef]
- Chien, C.-C.; Han, M.-M.; Chiu, Y.-H.; Wang, J.-J.; Chu, C.-C.; Hung, C.-Y.; Sun, Y.-M.; Yeh, N.-C.; Ho, C.-H.; Lin, C.-C.; et al. Epidemiology of cancer in end-stage renal disease dialysis patients: A national cohort study in Taiwan. J. Cancer 2017, 8, 9–18. [Google Scholar] [CrossRef]
- Wu, C.-F.; Pang, S.-T.; Shee, J.-J.; Chang, P.-L.; Chuang, C.-K.; Chen, C.-S.; Liao, S.-K.; Weng, W.-H. Identification of genetic alterations in upper urinary tract urothelial carcinoma in end-stage renal disease patients. Genes Chromosomes Cancer 2010, 49, 928–934. [Google Scholar] [CrossRef]
- Tseng, S.F.; Chuang, Y.C.; Yang, W.C. Long-term outcome of radical cystectomy in ESDR patients with bladder urothelial carcinoma. Int. Urol. Nephrol. 2011, 43, 1067–1071. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.F.; Chang, P.L.; Chen, C.S.; Chuang, C.K.; Weng, H.H.; Pang, S.T. The outcome of patients on dialysis with upper urinary tract transitional cell carcinoma. J. Urol. 2006, 176, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-C.; Chang, Y.-H.; Shindel, A.W.; Lin, J.-H.; Ho, D.-R.; Chen, C.-S.; Chang, Y.-L. Perioperative Complications and Mortality in Patients with Urothelial Carcinoma and End-Stage Renal Disease Undergoing One-Stage Complete Urinary Tract Extirpation. Ann. Surg. Oncol. 2018, 25, 573–581. [Google Scholar] [CrossRef]
- Mikata, K.; Noguchi, S.; Jinza, S.; Masuda, M.; Noguchi, K.; Kubota, Y.; Hosaka, M. Extirpation of total urinary tract as a final treatment for asynchronous multicentric urothelial cancer: A case report. Hinyokika Kiyo Acta Urol. Jpn. 1996, 42, 377–380. [Google Scholar]
- Holton, M.R.; Van Zijl, P.S.; Oberle, W.T.; Jacobs, S.C.; Sklar, G.N. Complete urinary tract extirpation: The University of Maryland experience. Urology 2006, 68, 65–69. [Google Scholar] [CrossRef]
- Kanda, H.; Hirasaki, Y.; Iida, T.; Kanao-Kanda, M.; Toyama, Y.; Chiba, T.; Kunisawa, T. Perioperative Management of Patients With End-Stage Renal Disease. J. Cardiothorac. Vasc. Anesth. 2017, 31, 2251–2267. [Google Scholar] [CrossRef] [PubMed]
- Akand, M.; Muilwijk, T.; Van Der Aa, F.; Gevaert, T.; Milenkovic, U.; Moris, L.; Blyweert, W.; Van Poppel, H.; Albersen, M.; Joniau, S. Prognostic score predicts overall survival following complete urinary tract extirpation. Scand. J. Urol. 2020, 54, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Carrion, A.; Raventós, C.; Lozano, F.; Semidey, M.E.; Gallardo, I.; Trilla, E. A Robot-Assisted Complete Urinary Tract Extirpation in a Patient with Simultaneous Panurothelial Carcinoma: A Case Report. J. Endourol. Case Rep. 2020, 6, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Yee, C.-H.; Chan, B.L.H.; Gudaru, K.; Wong, H.-F.; Tam, M.H.M.; Teoh, J.Y.C.; Chiu, P.K.F.; Hou, S.-M.; Ng, C.-F. Robotic radical cystectomy and bilateral nephrectomy in a renal transplant patient: The indocyanine green technique. Cent. Eur. J. Urol. 2021, 74, 272–273. [Google Scholar] [CrossRef]
- Kausz, A.; Pahari, D. The value of vaccination in chronic kidney disease. Semin. Dial. 2004, 17, 9–11. [Google Scholar] [CrossRef]
- Huang, G.L.; Luo, H.L.; Chen, Y.T.; Cheng, Y.T. Oncologic Outcomes of Post-Kidney Transplantation Superficial Urothelial Carcinoma. Transplant. Proc. 2018, 50, 998–1000. [Google Scholar] [CrossRef]
- Liu, Y.; Lu, J.; Hong, K.; Huang, Y.; Ma, L. Independent prognostic factors for initial intravesical recurrence after laparoscopic nephroureterectomy for upper urinary tract urothelial carcinoma. Urol. Oncol. 2014, 32, 146–152. [Google Scholar] [CrossRef]
- Ketsuwan, C.; Sangkum, P.; Sirisreetreerux, P.; Viseshsindh, W.; Patcharatrakul, S.; Kongcharoensombat, W. Laparoscopic Bilateral Nephro-Ureterectomy Approach for Complete Urinary Tract Extirpation for the Treatment of Multifocal Urothelial Carcinoma in a Kidney Transplant Patient: A Case Report and Literature Review. Transplant. Proc. 2015, 47, 2265–2269. [Google Scholar] [CrossRef]
- Yasin, S.; Holley, J.L. When ESKD complicates cancer screening and cancer treatment. Semin. Dial. 2020, 33, 236–244. [Google Scholar] [CrossRef]
- Chinnadurai, R.; Flanagan, E.; Kalra, P.A. Distribution and association of cancer with mortality in end-stage renal disease patients receiving dialysis. J. Nephrol. 2019, 32, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.M.; Lai, M.N.; Chen, P.C.; Wang, J.D. Increased risk of urothelial cancer in young and middle aged patients with end-stage renal disease. J. Formos. Med. Assoc. 2015, 114, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Liu, Y.L.; Chen, M.F.; Chen, C.S.; Wu, C.T. Treatment Strategy for Dialysis Patient with Urothelial Carcinoma. Diagnostics 2021, 11, 1966. [Google Scholar] [CrossRef] [PubMed]
- Arhuidese, I.J.; Orandi, B.J.; Nejim, B.; Malas, M. Utilization, patency, and complications associated with vascular access for hemodialysis in the United States. J. Vasc. Surg. 2018, 68, 1166–1174. [Google Scholar] [CrossRef]
- Buse, S.; Alexandrov, A.; Mazzone, E.; Mottrie, A.; Haferkamp, A. Surgical benchmarks, mid-term oncological outcomes, and impact of surgical team composition on simultaneous enbloc robot-assisted radical cystectomy and nephroureterectomy. BMC Urol. 2021, 21, 73. [Google Scholar] [CrossRef]
- Andras, I.; Pecoraro, A.; Telecan, T.; Piana, A.; Boissier, R.; Hevia, V.; Prudhomme, T.; Amparore, D.; Bertolo, R.; Carbonara, U.; et al. How to manage renal masses in kidney transplant recipients? A collaborative review by the EAU-YAU kidney transplantation and renal cancer working groups. Actas Urol. Esp. (Engl. Ed.), 2023; ahead of print. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Operative Time | Blood Loss | Postoperative Morbidity or Mortality | Tumor and Pathological Stage | |
|---|---|---|---|---|---|
| Carrion et al. [14] |
| 360 min |
| Glans infection (Clavien–Dindo grade 2) |
|
| Yee et al. [15] |
| 543 min | 500 mL; no blood transfusion | No |
|
| This case |
| 384 min |
| No |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, C.-H.; Hsu, C.-Y.; Lin, Y.-S.; Tung, M.-C.; Ou, Y.-C. One-Step Robot-Assisted Complete Urinary Tract Extirpation in Man with End-Stage Renal Disease on Dialysis: The First Case Report. Curr. Oncol. 2023, 30, 5093-5102. https://doi.org/10.3390/curroncol30050385
Yang C-H, Hsu C-Y, Lin Y-S, Tung M-C, Ou Y-C. One-Step Robot-Assisted Complete Urinary Tract Extirpation in Man with End-Stage Renal Disease on Dialysis: The First Case Report. Current Oncology. 2023; 30(5):5093-5102. https://doi.org/10.3390/curroncol30050385
Chicago/Turabian StyleYang, Che-Hsueh, Chao-Yu Hsu, Yi-Sheng Lin, Min-Che Tung, and Yen-Chuan Ou. 2023. "One-Step Robot-Assisted Complete Urinary Tract Extirpation in Man with End-Stage Renal Disease on Dialysis: The First Case Report" Current Oncology 30, no. 5: 5093-5102. https://doi.org/10.3390/curroncol30050385