Financial Toxicity and Out-of-Pocket Costs for Patients with Head and Neck Cancer



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Overview of Australian Healthcare System
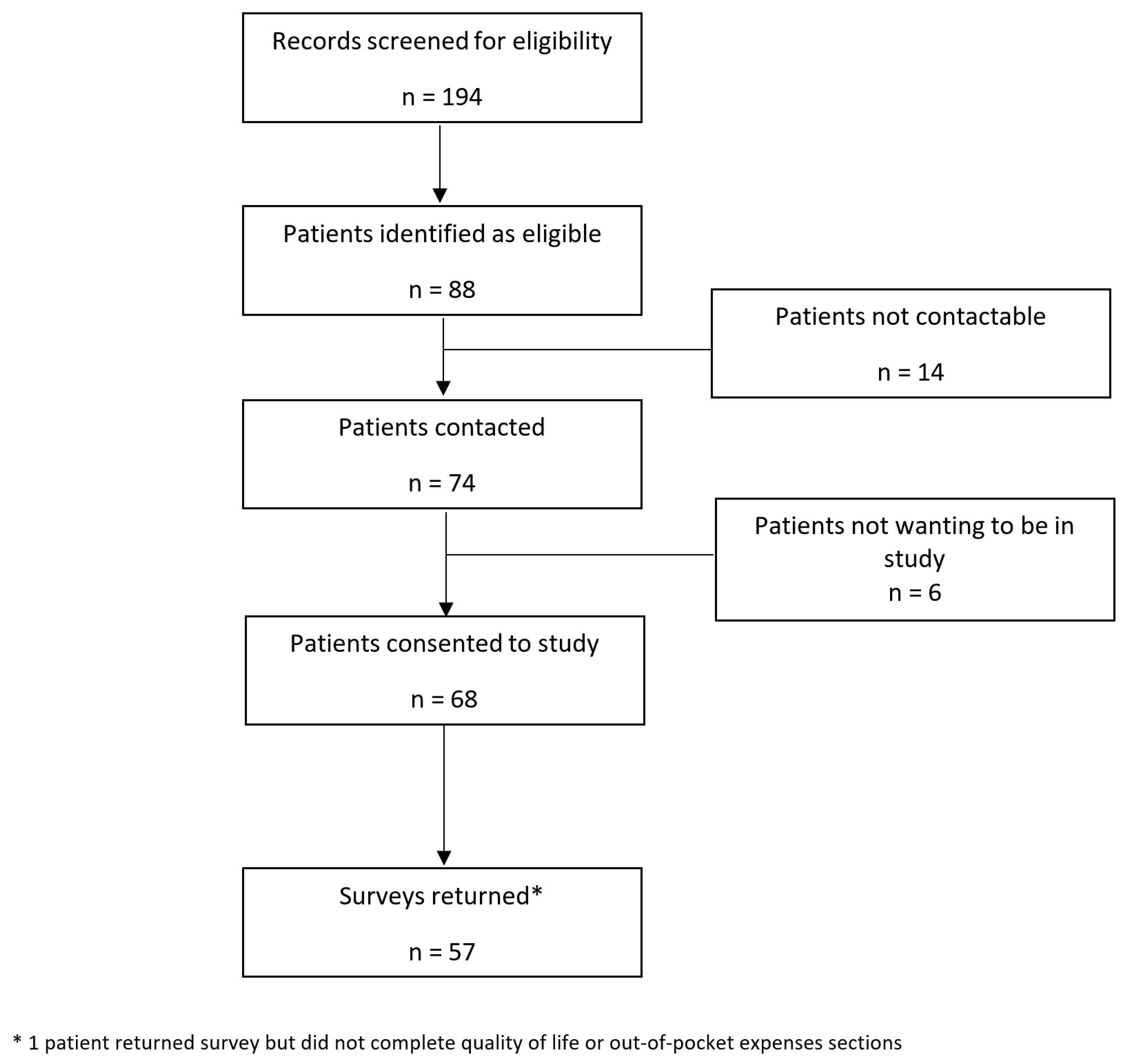
2.3. Participants and Recruitment
- Completed radiotherapy for mucosal SCC of the head and neck region (either as definitive or adjuvant treatment ± chemotherapy);
- One to three years after completion of radiotherapy treatment;
- Aged >18 years;
- Disease-free and well-enough to complete the survey as determined by the study investigator.
2.4. Data Collection
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nigro, C.L.; Denaro, N.; Merlotti, A.; Merlano, M. Head and neck cancer: Improving outcomes with a multidisciplinary approach. Cancer Manag. Res. 2017, 9, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Cramer, J.D.; Burtness, B.; Le, Q.T.; Ferris, R.L. The changing therapeutic landscape of head and neck cancer. Nat. Rev. Clin. Oncol. 2019, 16, 669–683. [Google Scholar] [CrossRef] [PubMed]
- Pollaers, K.; Massingham, I.; Friedland, P.L.; Farah, C.S. The economic burden of oral squamous cell carcinoma in Australia. J. Oral Pathol. Med. 2019, 48, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Leeuw, I.V.-D.; Dawson, C.; Licitra, L.; Eriksen, J.G.; Hosal, S.; Singer, S.; Laverty, D.P.; Golusinski, W.; Machczynski, P.; Gomes, A.V.; et al. European Head and Neck Society recommendations for head and neck cancer survivorship care. Oral Oncol. 2022, 133, 106047. [Google Scholar] [CrossRef]
- Zafar, S.Y. Financial toxicity of cancer care: It’s time to intervene. Gynecol. Oncol. 2016, 108, djv370. [Google Scholar] [CrossRef]
- Gordon, L.G.; Merollini, K.; Lowe, A.; Chan, R. A systematic review of financial toxicity among cancer survivors: We can’t pay the co-pay. Patient 2017, 10, 295–309. [Google Scholar] [CrossRef]
- Massa, S.T.; Osazuwa-Peters, N.; Boakye, E.A.; Walker, R.J.; Ward, G.M. Comparison of the financial burden of survivors of head and neck cancer with other cancer survivors. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 239–249. [Google Scholar] [CrossRef]
- Ma, S.J.; Iovoli, A.J.; Attwood, K.; Wooten, K.E.; Arshad, H.; Gupta, V.; McSpadden, R.P.; Kuriakose, M.A.; Markiewicz, M.R.; Chan, J.M.; et al. Association of significant financial burden with survival for head and neck cancer patients treated with radiation therapy. Oral Oncol. 2021, 115, 105196. [Google Scholar] [CrossRef]
- Mady, L.J.; Lyu, L.; Owoc, M.S.; Peddada, S.D.; Thomas, T.H.; Sabik, L.M.; Johnson, J.T.; Nilsen, M.L. Understanding financial toxicity in head and neck cancer survivors. Oral Oncol. 2019, 95, 187–193. [Google Scholar] [CrossRef]
- Beeler, W.H.; Bellile, E.L.; Casper, K.A.; Jaworski, E.; Burger, N.J.; Malloy, K.M.; Spector, M.E.; Shuman, A.G.; Rosko, A.; Stucken, C.L.; et al. Patient-reported financial toxicity and adverse medical consequences in head and neck cancer. Oral Oncol. 2020, 101, 104521. [Google Scholar] [CrossRef]
- Baddour, K.; Fadel, M.; Zhao, M.; Corcoran, M.; Owoc, M.S.; Thomas, T.H.; Sabik, L.M.; Nilsen, M.L.; Ferris, R.L.; Mady, L.J. The cost of cure: Examining objective and subjective financial toxicity in head and neck cancer survivors. Head Neck 2021, 43, 3062–3075. [Google Scholar] [CrossRef] [PubMed]
- Diao, K.; Lei, X.; Smith, G.L.; Jagsi, R.; Peterson, S.E.; Sumer, B.D.; Smith, B.D.; Sher, D.J. Patient-reported financial toxicity in a population-based cohort of oropharynx cancer survivors. Int. J. Radiat. Oncol. Biol. Phys. 2023, 116, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Hueniken, K.; Douglas, C.M.; Jethwa, A.R.; Mirshams, M.; Eng, L.; Hope, A.; Chepeha, D.B.; Goldstein, D.P.; Ringash, J.; Hansen, A.; et al. Measuring financial toxicity incurred after treatment of head and neck cancer: Development and validation of the Financial Index of Toxicity questionnaire. Cancer 2020, 126, 4042–4050. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed]
- Pulok, M.H.; van Gool, K.; Hall, J. Horizontal inequity in the utilisation of healthcare services in Australia. Health Policy 2020, 124, 1263–1271. [Google Scholar] [CrossRef]
- Rana, R.H.; Alam, K.; Gow, J. Selection of private or public hospital care: Examining the care-seeking behaviour of patients with private health insurance. BMC Health Serv. Res. 2020, 20, 380. [Google Scholar] [CrossRef]
- List, M.A.; D’Antonio, L.L.; Cella, D.F.; Siston, A.; Mumby, P.; Haraf, D.; Vokes, E. The performance status scale for head and neck cancer patients and the functional assessment of cancer therapy-head and neck scale: A study of utility and validity. Cancer 1996, 77, 2294–2301. [Google Scholar] [CrossRef]
- Carrera, P.M.; Kantarjian, H.M.; Blinder, V.S. The financial burden and distress of patients with cancer: Understanding and stepping-up action on the financial toxicity of cancer treatment. CA Cancer J. Clin. 2018, 68, 153–165. [Google Scholar] [CrossRef]
- Durber, K.; Halkett, G.K.; McMullen, M.; Nowak, A.K. Measuring financial toxicity in Australian cancer patients—Validation of the Comprehensive Score for financial Toxicity (FACT COST) measuring financial toxicity in Australian cancer patients. Asia-Pac. J. Clin. Oncol. 2021, 17, 377–387. [Google Scholar] [CrossRef]
- Farrugia, M.; Yu, H.; Ma, S.J.; Iovoli, A.J.; Erickson, K.; Wendel, E.; Attwood, K.; Wooten, K.E.; Gupta, V.; McSpadden, R.P.; et al. Financial counseling is associated with reduced financial difficulty scores in head and neck cancer patients treated with radiation therapy. Cancers 2021, 13, 2516. [Google Scholar] [CrossRef]
- Thamm, C.; Fox, J.; Hart, N.H.; Rhee, J.; Koczwara, B.; Emery, J.; Milley, K.; Nund, R.L.; Chan, R.J. Exploring the role of general practitioners in addressing financial toxicity in cancer patients. Support. Care Cancer 2022, 30, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.N.; Hueniken, K.; Manojlovic-Kolarski, M.; Eng, L.; Mirshams, M.; Khan, K.; Simpson, C.; Au, M.; Liu, G.; Xu, W.; et al. Out-of-pocket costs associated with head and neck cancer treatment. Cancer Rep. 2022, 5, e1528. [Google Scholar] [CrossRef] [PubMed]
- Gordon, L.G.; Nabukalu, D.; Chan, R.J.; Goldsbury, D.E.; Hobbs, K.; Hunt, L.; Karikios, D.J.; Mackay, G.; Muir, L.; Leigh, L.; et al. Opinions and strategies of Australian health professionals on tackling cancer-related financial toxicity: A nationwide survey. Asia-Pac. J. Clin. Oncol. 2023, 19, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Merollini, K.M.D.; Gordon, L.G.; Ho, Y.M.; Aitken, J.F.; Kimlin, M.G. Cancer survivors’ long-term health service costs in Queensland, Australia: Results of a population-level data linkage study (Cos-Q). Int. J. Environ. Res. Public Health 2022, 19, 9473. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Characteristics (n = 57) | n (%) | Patient Characteristics (n = 57) | n (%) |
|---|---|---|---|
| Age (at survey completion) Mean + SD | 63.8 + 9.2 | Time from treatment completion to survey (years) Mean + SD | 1.9 + 0.63 |
| Sex | Private health insurance * | 19 (34%) | |
| Male | 43 (75%) | Yes | 37 (66%) |
| Female | 14 (25%) | No | 19 (34%) |
| Ethnicity | Total annual household income (diagnosis) | ||
| Aboriginal | 1 (2%) | 0 to AUD 18,200 | 9 (16%) |
| Torres Strait Islander | 0 (0%) | AUD 18,201 to AUD 45,000 | 21 (37%) |
| Both Aboriginal and Torres Strait Islander | 1 (2%) | AUD 45,001 to AUD 120,000 | 17 (30%) |
| Neither | 55 (96%) | >AUD 120,000 | 10 (18%) |
| Distance to Townsville Hospital | 23 (40%) | Employment status (at diagnosis) | |
| <50 km | 3 (5%) | Full-time work | 23 (40%) |
| 50–99 km | 3 (5%) | Part-time work | 2 (4%) |
| 100–199 km | 7 (12%) | Casual work | 4 (7%) |
| 200–299 km | 13 (23%) | Retired | 24 (42%) |
| 300–399 km | 8 (14%) | Unemployed | 3 (5%) |
| ≥400 km | 23 (40%) | Volunteer/unpaid work | 1 (2%) |
| Charlson Comorbidity Index (CCI) Mean + SD | 2.5 + 1.6 | Sole income earner * | |
| Yes | 27 (48%) | ||
| No | 29 (52%) | ||
| ECOG | Self-employed | ||
| 0 1 | 26 (46%) 31 (54%) | Yes No N/A (not working) | 10 (18%) 35 (61%) 12 (21%) |
| Smoking status | Marital status | ||
| Married/de facto | 33 (58%) | ||
| Current | 19 (33%) | Divorced or separated | 15 (26%) |
| Former | 24 (42%) | Single or never married | 6 (11%) |
| Never | 14 (25%) | Widowed | 3 (5%) |
| Level of education | Occupation (ISCO-08 classification) | ||
| Primary School | 5 (9%) | Retired or Unemployed | 15 (26%) |
| Managers | 6 (11%) | ||
| Secondary School (Grade 10) | 20 (35%) | Professionals | 3 (5%) |
| Technicians | 4 (7%) | ||
| Secondary School (Grade 12) | 6 (11%) | Service and Sales Workers | 7 (12%) |
| Agricultural, Forestry, and Fishery | 2 (4%) | ||
| Technical College, Diploma, or Certificate | 21 (37%) | Craft Workers | 6 (11%) |
| Plant and Machine Operators | 10 (18%) | ||
| University Degree | 5 (9%) | Elementary Occupations | 4 (7%) |
| Living arrangements | |||
| Live with partner | 25 (44%) | ||
| Live alone | 21 (37%) | ||
| Live with partner and children | 6 (11%) | ||
| Live with children | 2 (4%) | ||
| Assisted living | 1 (2%) | ||
| Other | 2 (4%) | ||
| Clinical Characteristics | |||
| Tumour location | |||
| Oral cavity | 7 (12%) | ||
| Nasopharynx | 2 (4%) | Treatment | |
| Oropharynx–p16-positive | 30 (53%) | Chemo RT | 35 (61%) |
| Oropharynx–p16-negative | 7 (12%) | RT alone | 11 (19%) |
| Hypopharynx | 2 (4%) | Surgery + RT | 7 (12%) |
| Larynx | 8 (14%) | Surgery + chemo RT | 4 (7%) |
| Unknown | 1 (2%) | ||
| Tumour stage (AJCC 8th edition) | |||
| I | 16 (28%) | ||
| II | 12 (21%) | ||
| III | 16 (28%) | ||
| IV | 1 (2%) | ||
| IVA | 11 (19%) | ||
| IVB | 1 (2%) | ||
| Financial Support | |||
| Has a member of your treating team asked if you have any financial concerns? | |||
| Yes | 19 (33%) | ||
| No | 38 (67%) | ||
| How comfortable are you in discussing financial difficulties with your medical team? | |||
| Median (SD) | 10 (3) * | ||
| Financial support during RT | Financial support 12 months after treatment | ||
| Worked during treatment | 3 (5%) | Returned to work | 18 (32%) |
| Sick leave | 7 (12%) | Sick leave | 1 (2%) |
| Superannuation | 6 (11%) | Superannuation | 4 (7%) |
| Income protection | 4 (7%) | Income protection | 4 (7%) |
| JobSeeker ** | 7 (12%) | JobSeeker ** | 5 (9%) |
| Age pension | 21 (37%) | Pension | 24 (42%) |
| Disability pension | 4 (7%) | Other | 8 (14%) |
| Other | 14 (25%) | ||
| Employment status 12 months post cancer treatment | Income 12 months post cancer treatment | ||
| Full-time work | 11 (19%) | Same income | 22 (39%) |
| Part-time work | 8 (14%) | Lower income | 13 (23%) |
| Did not return to work | 10 (18%) | Higher income | 2 (4%) |
| Not working previously | 28 (49%) | N/A—not working before diagnosis | 20 (35%) |
| Reasons for not returning to work (n = 10) ^ | |||
| Side effects from treatment | 9 (90%) | ||
| Work-related issues | 1 (10%) | ||
| Other | 1 (10%) | ||
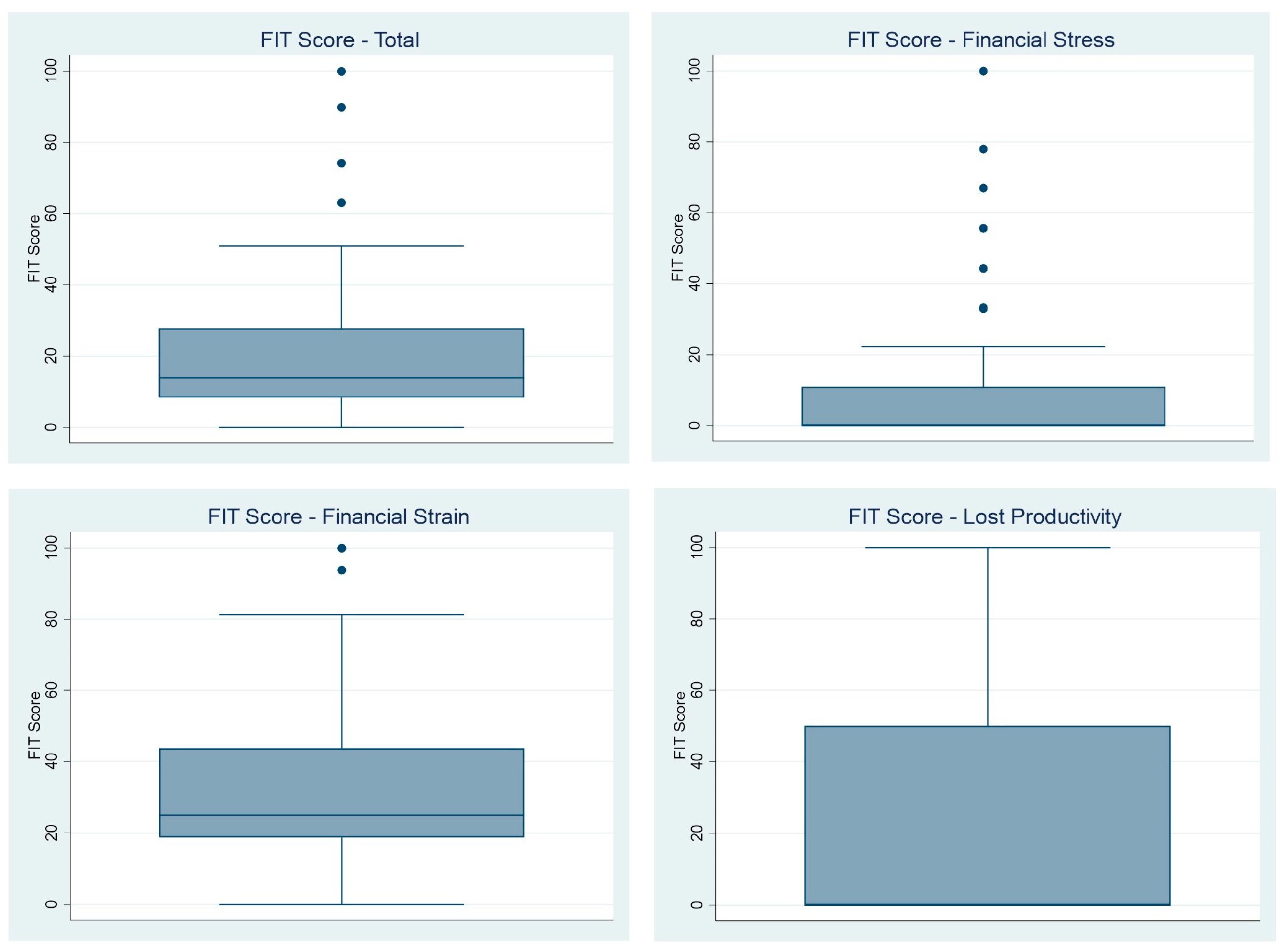
| FIT Scores * | ||
|---|---|---|
| Total Score—13.9 (19.5) | ||
| Financial Stress—0 (11) | ||
| Financial Strain—25 (25) | ||
| Lost Productivity—0 (50) | ||
| Factors Associated with Financial Toxicity | ||
| Variable | FIT Total Scores * | p Value |
| Age | 0.99 | |
| ≤60 | 13.9 (38.1) | |
| >60 | 13.9 (13.9) | |
| Sex | 0.14 | |
| Male | 12 (19.5) | |
| Female | 18.4 (19.5) | |
| Distance to Townsville Hospital | 0.47 | |
| 0–99 km | 17.1 (13.9) | |
| >100 km | 12 (22.3) | |
| Smoking Status | ||
| Current | 19.4 (35.3) | 0.23 |
| Former/Never | 13.9 (11.1) | |
| Level of Education | 0.06 | |
| Primary/High School | 19.3 (25.1) | |
| TAFE/University | 11.1 (12) | |
| Marital Status | 0.01 | |
| Married | 11.1 (11) | |
| Not Married | 23.1 (34.2) | |
| Private Health Insurance | 0.01 | |
| Yes | 8.3 (13.8) | |
| No | 17.6 (22.3) | |
| Annual Household Income | 0.10 | |
| ≤AUD 45,000 | 17.1 (16.7) | |
| >AUD 45,000 | 11.1(24.9) | |
| Sole Income Earner | 0.12 | |
| Yes | 17.6 (36) | |
| No | 12 (11.1) | |
| Employment Status at Diagnosis | 0.37 | |
| Working | 17.6 (31.5) | |
| Not Working | 12 (11.1) | |
| Self-Employed | 0.80 | |
| Yes | 15.3 (19.5) | |
| No or N/A | 13.9 (22.3) | |
| Tumour Location | 0.90 | |
| Oropharyngeal | 15.7 (19.5) | |
| Other | 13.9 (18.1) | |
| Tumour Stage | 0.85 | |
| Early | 18.4 (22.3) | |
| Advanced | 13.9 (13.9) | |
| Treatment Received | 0.60 | |
| ChemoRT ± Surgery | 13.9 (22.2) | |
| RT alone or Surgery + RT | 12.5 (25.1) | |
| Quality of Life—FACT H&N | |||||
|---|---|---|---|---|---|
| Overall Cohort Median (IQR) | High FT (n = 14) Median (IQR) | Low FT (n = 42) Median (IQR) | p Value | Spearman’s Rho | |
| Physical Wellbeing | 23 (8) | 16 (10) | 24.5 (6) | <0.001 | −0.52 |
| Social/Family Wellbeing | 22 (9.5) | 15.6 (11) | 24 (8.2) | <0.001 | −0.55 |
| Emotional Wellbeing | 20 (6.5) | 16 (7) | 20 (6) | 0.004 | −0.40 |
| Functional Wellbeing | 18.5 (9) | 13.5 (8) | 21 (9) | 0.002 | −0.45 |
| Head and Neck Cancer Subscale | 25 (11) | 22 (16) | 25 (10) | 0.13 | −0.29 |
| Total Score | 105.5 (33.4) | 76.5 (43.2) | 114.5 (29) | <0.001 | −0.55 |
| Out-of-Pocket Expenses | Number of Participants with Out-of-Pocket Expenses (%) n = 56 | Total Expense (12-Month Period) * |
|---|---|---|
| Dental | 16 (29%) | 388 (825) |
| Allied Health | 5 (9%) | 500 (3284) |
| Mental Health | 3 (5%) | 300 (440) |
| GP | 15 (27%) | 250 (380) |
| Specialist | 7 (13%) | 600 (1100) |
| Accommodation | 10 (18%) | 520 (300) |
| Travel | 20 (36%) | 525 (825) |
| Home Services | 6 (11%) | 716 (700) |
| Dietary Supplements | 23 (41%) | 600 (950) |
| Investigations | 8 (14%) | 575 (1190) |
| Medications | 23 (41%) | 400 (600) |
| Total | 41 (73%) | 1796 (2700) |
| Minimum—18 | ||
| Maximum 25,050 |
| Variable | Out-of-Pocket Expense * | p Value |
|---|---|---|
| Age | 0.20 | |
| ≤60 | 2000 (2500) | |
| >60 | 1400 (3078) | |
| Sex | 0.53 | |
| Male | 1570 (2500) | |
| Female | 1798 (3585.5) | |
| Distance to Townsville Hospital | 0.01 | |
| 0–99 km | 730 (1300) | |
| ≥100 km | 2655 (2450) | |
| Smoking Status | 0.25 | |
| Current | 1400 (2900) | |
| Former/Never | 1825 (2606) | |
| Level of Education | 0.03 | |
| Primary/High School | 1167 (1380) | |
| TAFE/University | 2680 (2230) | |
| Marital Status | 0.44 | |
| Married | 1500 (2750) | |
| Not Married | 1865 (2233) | |
| Private Health Insurance | 0.12 | |
| Yes | 2680 (2400) | |
| No | 1400 (2700) | |
| Annual Household Income | 0.01 | |
| ≤AUD 45,000 | 1134 (1878) | |
| >AUD 45,000 | 2740 (2492) | |
| Sole Income Earner | 0.42 | |
| Yes | 1850 (2666) | |
| No | 1300 (2250) | |
| Employment Status at Diagnosis | 0.01 | |
| Working | 2655 (2684) | |
| Not Working | 730 (1890) | |
| Self-Employed | 0.33 | |
| Yes | 3185 (2858) | |
| No or N/A | 1632 (2250) | |
| Tumour Location | 0.69 | |
| Oropharyngeal | 1800 (3010) | |
| Other | 1714 (2650) | |
| Tumour Stage | 0.23 | |
| Early | 1500 (2300) | |
| Advanced | 2000 (3354) | |
| Treatment Received | 0.04 | |
| ChemoRT ± Surgery | 1850 (2600) | |
| RT alone or Surgery + RT | 600 (2035) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, J.; Yu, J.; Gordon, L.G.; Chilkuri, M. Financial Toxicity and Out-of-Pocket Costs for Patients with Head and Neck Cancer. Curr. Oncol. 2023, 30, 4922-4935. https://doi.org/10.3390/curroncol30050371
Smith J, Yu J, Gordon LG, Chilkuri M. Financial Toxicity and Out-of-Pocket Costs for Patients with Head and Neck Cancer. Current Oncology. 2023; 30(5):4922-4935. https://doi.org/10.3390/curroncol30050371
Chicago/Turabian StyleSmith, Justin, Justin Yu, Louisa G. Gordon, and Madhavi Chilkuri. 2023. "Financial Toxicity and Out-of-Pocket Costs for Patients with Head and Neck Cancer" Current Oncology 30, no. 5: 4922-4935. https://doi.org/10.3390/curroncol30050371