Characterizing Variability in Lung Cancer Outcomes and Influence of a Lung Diagnostic Assessment Program in Southeastern Ontario, Canada


Abstract
:1. Introduction
2. Materials and Methods
2.1. Local Context
2.2. Study Design
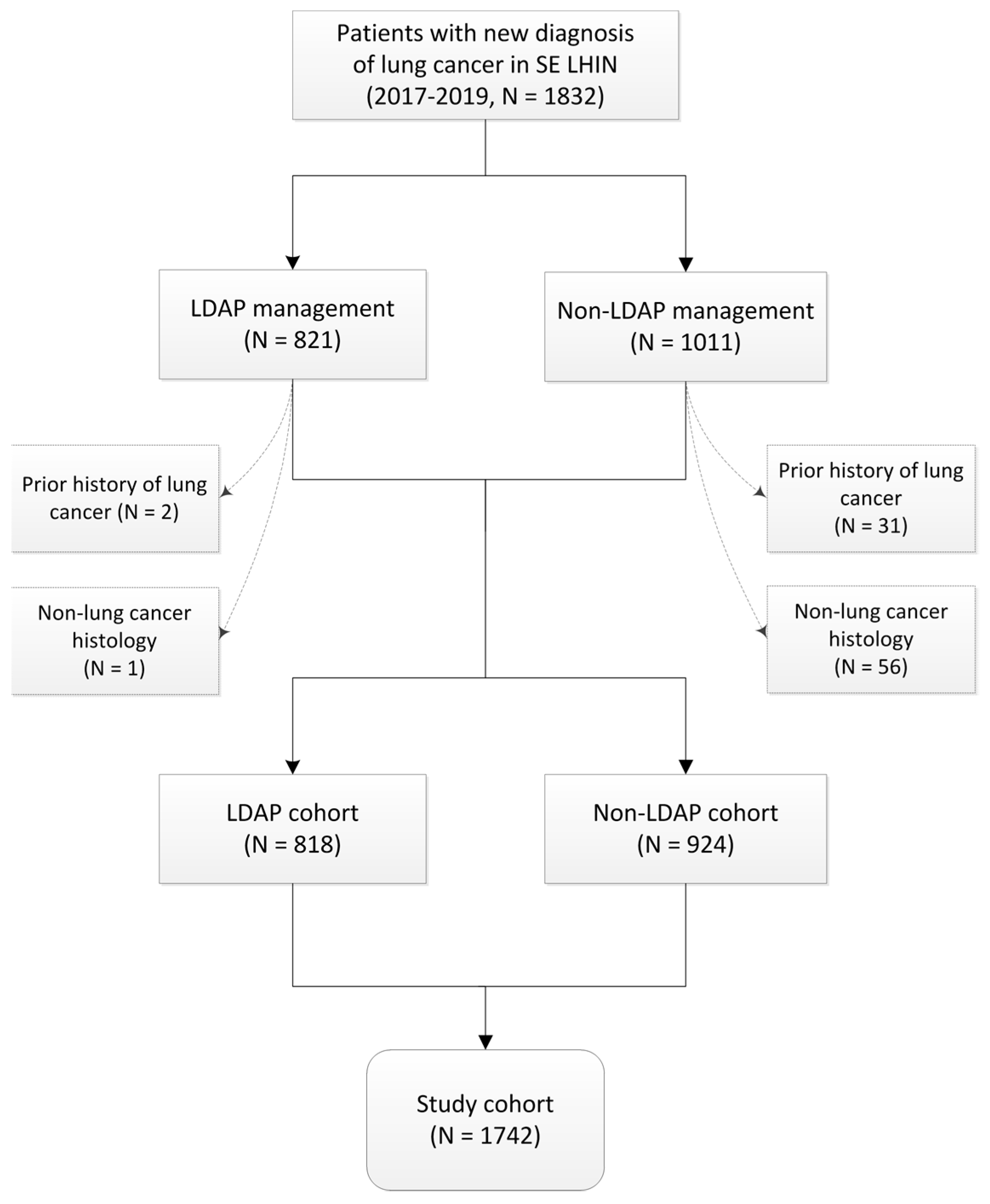
2.3. Study Participants
2.4. Study Variables and Data Collection
2.4.1. Independent Variables
2.4.2. Dependent Variables
2.5. Definitions
2.6. Study Outcome
2.7. Statistical Approach
3. Results
3.1. Patient and Disease Characteristics

{kind=link}
{kind=link}
{kind=link}
| Characteristic | LDAP Cohort (N = 818) | Non-LDAP Cohort (N = 924) | Overall (N = 1742) |
|---|---|---|---|
| Age | |||
| 18–60 | 118 (14.4%) | 161 (17.4%) | 279 (16.0%) |
| 61–70 | 288 (35.2%) | 275 (29.8%) | 563 (32.3%) |
| 71–80 | 290 (35.5%) | 334 (36.1%) | 624 (35.8%) |
| >80 | 122 (14.9%) | 154 (16.7%) | 276 (15.9%) |
| median (IQR) | 71 (64, 77) | 71 (63, 78) | 71 (64, 78) |
| Sex (female N/%) | 443 (54.2%) | 478 (51.7%) | 921 (52.9%) |
| Distance from LDAP (km) | |||
| <50 | 380 (46.5%) | 272 (29.5%) | 652 (37.4%) |
| 50–100 | 405 (49.5%) | 505 (54.7%) | 910 (52.2%) |
| >100 | 33 (4.0%) | 147 (15.9%) | 180 (10.3%) |
| median (IQR) | 56.9 (10.0, 76.6) | 74.3 (36.8, 88.7) | 70.8 (23.6, 84.4) |
| Income Quintile | |||
| 1 (lowest) | 139 (17.0%) | 185 (20.0%) | 324 (18.6%) |
| 2 | 238 (29.1%) | 284 (30.7%) | 522 (30.0%) |
| 3 | 270 (33.0%) | 272 (29.4%) | 542 (31.1%) |
| 4 | 130 (15.9%) | 158 (17.1%) | 288 (16.5%) |
| 5 (highest) | 41 (5.0%) | 25 (2.7%) | 66 (3.8%) |
| Histology Type | |||
| Adenocarcinoma | 346 (42.4%) | 329 (35.6%) | 675 (38.8%) |
| Squamous cell carcinoma | 162 (19.8%) | 134 (14.5%) | 296 (17.0%) |
| Poorly differentiated carcinoma | 195 (23.9%) | 322 (34.8%) | 517 (29.7%) |
| Small cell carcinoma | 77 (9.4%) | 94 (10.2%) | 171 (9.8%) |
| Large cell carcinoma | 5 (0.6%) | 14 (1.5%) | 19 (1.1%) |
| Neuroendocrine NOS | 4 (0.5%) | 9 (1.0%) | 13 (0.7%) |
| Other | 28 (3.4%) | 22 (2.4%) | 50 (2.9%) |
| Stage (OCR best stage) | |||
| 0/I | 238 (29.1%) | 144 (15.6%) | 382 (21.9%) |
| II | 68 (8.3%) | 38 (4.1%) | 106 (6.1%) |
| III | 153 (18.7%) | 114 (12.4%) | 267 (15.3%) |
| IV | 264 (32.3%) | 404 (43.8%) | 668 (38.4%) |
| Unknown | 95 (11.6%) | 224 (24.3%) | 319 (18.3%) |
3.2. Factors Influencing Lung Cancer Survival
| Factor | N | Overall Survival | Unadjusted | Adjusted | |||
|---|---|---|---|---|---|---|---|
| Median (Months) | 2-Year | HR (95% CI) | p | HR (95% CI) | p | ||
| Age | |||||||
| 18–60 | 279 | 15.8 | 41.9% | reference | 0.0062 | reference | <0.0001 |
| 61–70 | 563 | 12.7 | 37.9% | 1.12 (0.93, 1.35) | 1.26 (1.05, 1.53) | ||
| 71–80 | 623 | 11.1 | 35.2% | 1.24 (1.03, 1.49) | 1.60 (1.33, 1.93) | ||
| >80 | 276 | 8.9 | 32.6% | 1.41 (1.14, 1.74) | 1.78 (1.43, 2.21) | ||
| Sex | |||||||
| Female | 920 | 15.8 | 43.0% | 0.68 (0.61, 0.77) | <0.0001 | 0.79 (0.70, 0.89) | 0.0001 |
| Male | 821 | 8.6 | 29.7% | reference | reference | ||
| Distance from LDAP (kilometers) | |||||||
| <50 | 652 | 15 | 41.8% | reference | 0.0045 | reference | 0.3302 |
| 50–100 | 909 | 10.2 | 34.7% | 1.22 (1.07, 1.39) | 1.10 (0.95, 1.26) | ||
| >100 | 180 | 10.1 | 28.9% | 1.28 (1.04, 1.56) | 0.99 (0.80, 1.23) | ||
| Income Quintile | |||||||
| 1 (lowest) | 324 | 8.4 | 31.1% | 2.27 (1.53, 3.36) | 0.0004 | 2.01 (1.35, 3.01) | 0.0026 |
| 2 | 522 | 12.4 | 38.2% | 1.79 (1.21, 2.62) | 1.56 (1.05, 2.33) | ||
| 3 | 541 | 11.2 | 34.8% | 1.89 (1.28, 2.77) | 1.75 (1.17, 2.61) | ||
| 4 | 288 | 11.7 | 39.4% | 1.81 (1.22, 2.70) | 1.69 (1.13, 2.53) | ||
| 5 (highest) | 66 | 33.2 | 56.1% | reference | reference | ||
| Histology Type (OCR histology) | |||||||
| Adenocarcinoma | 675 | 29.3 | 53.1% | reference | <0.0001 | reference | <0.0001 |
| Squamous cell carcinoma | 296 | 14.3 | 37.1% | 1.45 (1.21, 1.73) | 1.49 (1.24, 1.80) | ||
| Poorly differentiated carcinoma | 517 | 4.1 | 22.3% | 2.55 (2.21, 2.96) | 2.13 (1.82, 2.48) | ||
| Small cell carcinoma | 171 | 6.7 | 12.0% | 2.66 (2.18, 3.24) | 1.75 (1.43, 2.14) | ||
| Other | 82 | 16.5 | 42.9% | 1.27 (0.93, 1.73) | 1.19 (0.87, 1.62) | ||
| Stage (OCR best stage) | |||||||
| 0/I | 381 | - | 75.8% | 0.16 (0.13, 0.20) | <0.0001 | 0.16 (0.13, 0.20) | <0.0001 |
| II | 106 | - | 62.1% | 0.24 (0.17, 0.32) | 0.27 (0.19, 0.37) | ||
| III | 267 | 14 | 31.8% | 0.50 (0.42, 0.59) | 0.51 (0.43, 0.61) | ||
| IV | 668 | 4.4 | 14.9% | reference | reference | ||
| unknown | 319 | 6.0 | 30.6% | 0.71 (0.61, 0.83) | 0.63 (0.53, 0.74) | ||
| LDAP | |||||||
| No | 924 | 7.5 | 29.8% | reference | <0.0001 | reference | <0.0001 |
| Yes | 817 | 18.5 | 44.7% | 0.61 (0.54, 0.69) | 0.76 (0.67, 0.87) | ||
| Factor | N | Overall Survival | Unadjusted | Adjusted | |||
|---|---|---|---|---|---|---|---|
| Median (Months) | 2-Year | HR (95% CI) | p | HR (95% CI) | p | ||
| Age | |||||||
| 18–60 | 271 | 17.5 | 42.9% | reference | 0.0247 | reference | <0.0001 |
| 61–70 | 539 | 14.5 | 38.6% | 1.13 (0.93, 1.36) | 1.33 (1.09, 1.61) | ||
| 71–80 | 593 | 13 | 38.2% | 1.21 (1.00, 1.45) | 1.64 (1.36, 1.99) | ||
| >80 | 258 | 11.3 | 34.2% | 1.38 (1.11, 1.71) | 1.80 (1.44, 2.25) | ||
| Sex | |||||||
| Female | 875 | 19.1 | 45.3% | 0.67 (0.60, 0.76) | <0.0001 | 0.78 (0.69, 0.89) | 0.0001 |
| Male | 786 | 10.3 | 30.9% | reference | reference | ||
| Distance from LDAP (kilometers) | |||||||
| <50 | 630 | 17.1 | 43.5% | reference | 0.0074 | reference | 0.6509 |
| 50–100 | 864 | 12.4 | 36.6% | 1.20 (1.05, 1.37) | 1.03 (0.90, 1.19) | ||
| >100 | 167 | 12.1 | 29.9% | 1.30 (1.05, 1.60) | 0.94 (0.75, 1.17) | ||
| Income Quintile | |||||||
| 1 (lowest) | 302 | 10 | 33.3% | 2.18 (1.46, 3.26) | 0.0019 | 2.02 (1.34, 3.04) | 0.0048 |
| 2 | 499 | 14.5 | 38.9% | 1.78 (1.20, 2.64) | 1.63 (1.08, 2.44) | ||
| 3 | 519 | 13 | 36.6% | 1.88 (1.27, 2.78) | 1.84 (1.22, 2.76) | ||
| 4 | 277 | 14.5 | 42.0% | 1.74 (1.16, 2.62) | 1.64 (1.09, 2.48) | ||
| 5 (highest) | 64 | 35.4 | 59.4% | reference | reference | ||
| Histology Type (OCR histology) | |||||||
| Adenocarcinoma | 648 | 31.4 | 54.5% | reference | <0.0001 | reference | <0.0001 |
| Squamous cell carcinoma | 291 | 16.4 | 39.1% | 1.43 (1.19, 1.71) | 1.45 (1.20, 1.76) | ||
| Poorly differentiated carcinoma | 483 | 5.9 | 24.1% | 2.48 (2.13, 2.88) | 2.10 (1.79, 2.46) | ||
| Small cell carcinoma | 162 | 7.5 | 12.1% | 2.82 (2.30, 3.44) | 1.78 (1.45, 2.19) | ||
| Other | 77 | 22.6 | 46.5% | 1.21 (0.87, 1.67) | 1.13 (0.82, 1.57) | ||
| Stage (OCR best stage) | |||||||
| 0/I | 374 | - | 77.2% | 0.15 (0.12, 0.18) | <0.0001 | 0.15 (0.12, 0.19) | <0.0001 |
| II | 105 | - | 63.8% | 0.22 (0.16, 0.30) | 0.25 (0.18, 0.35) | ||
| III | 261 | 14.9 | 32.1% | 0.49 (0.41, 0.58) | 0.51 (0.43, 0.61) | ||
| IV | 627 | 5.4 | 15.7% | reference | reference | ||
| unknown | 294 | 8 | 33.7% | 0.63 (0.53, 0.75) | 0.56 (0.47, 0.67) | ||
| LDAP | |||||||
| No | 844 | 9.2 | 31.4% | reference | <0.0001 | reference | 0.0161 |
| Yes | 817 | 20.6 | 45.9% | 0.61 (0.54, 0.69) | 0.72 (0.63, 0.82) | ||
3.3. Factors Associated with LDAP Management
| Factor | N (%) with LDAP | OR (95% CI) | p-Value |
|---|---|---|---|
| Age | |||
| 18–60 | 118 (42.3%) | reference | 0.0122 |
| 61–70 | 288 (51.2%) | 1.56 (1.15, 2.13) | |
| 71–80 | 289 (46.4%) | 1.15 (0.85, 1.56) | |
| >80 | 122 (44.2%) | 1.09 (0.75, 1.57) | |
| Sex | |||
| Male | 375 (45.7%) | reference | 0.6808 |
| Female | 442 (48.0%) | 0.96 (0.78, 1.18) | |
| Distance from LDAP (kilometers) | |||
| <50 | 380 (58.3%) | reference | <0.0001 |
| 50–100 | 404 (44.4%) | 0.55 (0.44, 0.69) | |
| >100 | 33 (18.3%) | 0.14 (0.09, 0.22) | |
| Income Quintile | |||
| 1 (lowest) | 139 (42.9%) | reference | 0.0209 |
| 2 | 238 (45.6%) | 1.24 (0.92, 1.67) | |
| 3 | 269 (49.7%) | 1.53 (1.13, 2.06) | |
| 4 | 130 (45.1%) | 0.97 (0.69, 1.37) | |
| 5 (highest) | 41 (62.1%) | 1.35 (0.76, 2.44) | |
| Stage | |||
| 0/I | 237 (62.2%) | 2.41 (1.84, 3.17) | <0.0001 |
| II | 68 (64.2%) | 2.76 (1.78, 4.34) | |
| III | 153 (57.3%) | 2.19 (1.63, 2.97) | |
| IV | 264 (39.5%) | reference | |
| unknown | 95 (29.8%) | 0.73 (0.54, 0.98) | |
| Histology Type (OCR histology) | |||
| Adenocarcinoma | 346 (51.3%) | reference | 0.0629 |
| Non-adenocarcinoma | 471 (44.2%) | 0.82 (0.66, 1.01) | |
3.4. Influence of LDAP Management on Subsequent LC Care (Specialist Assessment, Treatment, and Health Resource Utilization)
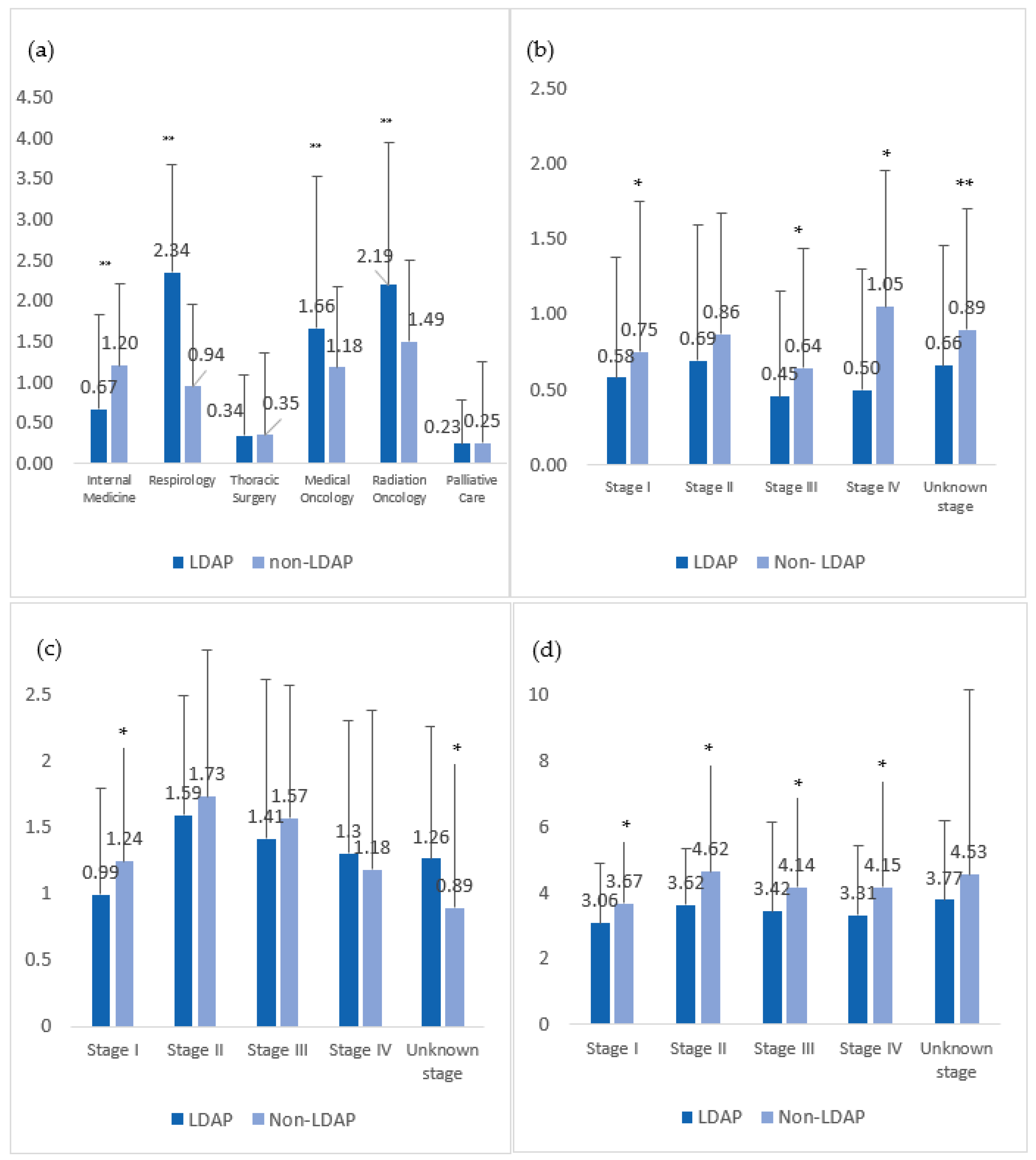
3.4.1. Specialist Assessment
3.4.2. Health Resource Utilization
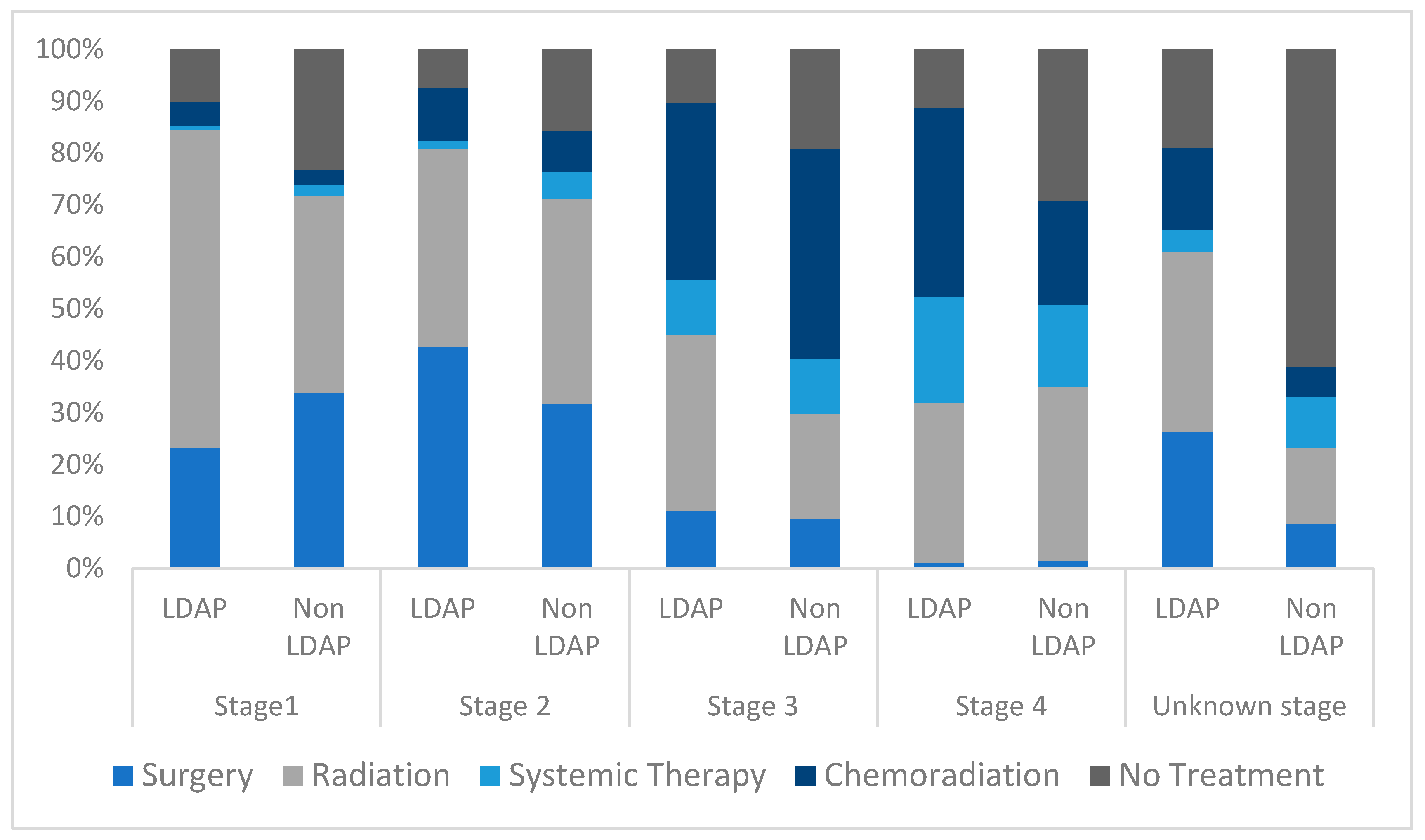
3.4.3. Treatment
4. Discussion
4.1. Association between LDAP Management and Treatment
4.2. Identifying Barriers to LDAP Management
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Lung and Bronchus Cancer Statistics|Canadian Cancer Society. 2022. Available online: https://cancer.ca/en/cancer-information/cancer-types/lung/statistics (accessed on 1 August 2022).
- dela Cruz, C.S.; Tanoue, L.T.; Matthay, R.A. Lung Cancer: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2011, 32, 605–644. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, A.; Damadoglu, E.; Salturk, C.; Okur, E.; Tuncer, L.Y.; Halezeroglu, S. Delays in the diagnosis and treatment of primary lung cancer: Are longer delays associated with advanced pathological stage? Upsala J. Med. Sci. 2008, 113, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Cancer Quality Council of Ontario. Cancer System Quality Index. 2021. Available online: https://www.csqi.on.ca/sites/csqipub/files/assets/CSQI2021Report.pdf (accessed on 5 January 2022).
- Canadian Partnership Against Cancer. Lung Cancer and Equity: A Focus on Income and Geography; Canadian Partnership Against Cancer: Toronto, ON, Canada, 2020. [Google Scholar]
- Lofters, A.K.; Gatov, E.; Lu, H.; Baxter, N.N.; Guilcher SJ, T.; Kopp, A.; Vahabi, M.; Datta, G.D. Lung Cancer Inequalities in Stage of Diagnosis in Ontario, Canada. Curr. Oncol. 2021, 28, 1946–1956. [Google Scholar] [CrossRef] [PubMed]
- South East Local Health Integration Network. South East LHIN Annual Business Plan 2017–2018; Government of Ontario. 2018. Available online: http://www.southeastlhin.on.ca/Accountability/AnnualBusinessPlan.aspx (accessed on 5 January 2022).
- Mullin ML, L.; Tran, A.; Golemiec, B.; Stone CJ, L.; Noseworthy, C.; O’Callaghan, N.; Parker, C.M.; Digby, G.C. Improving Timeliness of Lung Cancer Diagnosis and Staging Investigations Through Implementation of Standardized Triage Pathways. JCO Oncol. Pract. 2020, 16, e1202–e1208. [Google Scholar] [CrossRef] [PubMed]
- Habbous, S.; Khan, Y.; Langer, D.; Kaan, M.; Green, B.; Forster, K.; Darling, G.; Holloway, C. The effect of diagnostic assessment programs on the diagnosis and treatment of patients with lung cancer in Ontario, Canada. Ann. Thorac. Med. 2021, 16, 81–101. [Google Scholar] [CrossRef]
- Evans, W.K.; Ung, Y.C.; Assouad, N.; Chyjek, A.; Sawka, C. Improving the quality of lung cancer care in Ontario: The lung cancer disease pathway initiative. J. Thorac. Oncol. 2013, 8, 876–882. [Google Scholar] [CrossRef]
- Stone CJ, L.; Vaid, H.M.; Selvam, R.; Ashworth, A.; Robinson, A.; Digby, G.C. Multidisciplinary Clinics in Lung Cancer Care: A Systematic Review. Clin. Lung Cancer 2018, 19, 323–330.e3. [Google Scholar] [CrossRef]
- Brocken, P.; van der Heijden, E.H.F.M.; Oud, K.T.M.; Bootsma, G.; Groen, H.J.M.; Donders, A.R.T.; Dekhuijzen, P.N.R.; Prins, J.B. Distress in suspected lung cancer patients following rapid and standard diagnostic programs: A prospective observational study. Psycho-Oncology 2015, 24, 433–441. [Google Scholar] [CrossRef]
- Mullin, M.L.; Shellenberger, J.; Whitehead, M.; Brundage, M.; Eisenhauer, E.A.; Lougheed, M.D.; Parker, C.M.; Digby, G.C. Characterizing Regional Variability in Lung Cancer Outcomes across Ontario—A Population-Based Analysis. Curr. Oncol. 2022, 29, 9640–9659. [Google Scholar] [CrossRef]
- Stone CJ, L.; Robinson, A.; Brown, E.; Mates, M.; Falkson, C.B.; Owen, T.; Ashworth, A.; Parker, C.M.; Mahmud, A.; Tomiak, A.; et al. Improving timeliness of oncology assessment and cancer treatment through implementation of a multidisciplinary lung cancer clinic. J. Oncol. Pract. 2019, 15, E169–E177. [Google Scholar] [CrossRef] [PubMed]
- Hunnibell, L.S. Improving lung cancer care through nurse navigation. Lung Cancer Manag. 2014, 3, 229–231. [Google Scholar] [CrossRef]
- Stone CJ, L.; Johnson, A.P.; Robinson, D.; Katyukha, A.; Egan, R.; Linton, S.; Parker, C.; Robinson, A.; Digby, G.C. Health resource and cost savings achieved in a multidisciplinary lung cancer clinic. Curr. Oncol. 2021, 28, 1681–1695. [Google Scholar] [CrossRef] [PubMed]
- Canada, S. PCCF+ Version 8A Postal Code OM Conversion File Plus (PCCF+), Reference Guide. Available online: www.statcan.gc.ca (accessed on 20 April 2023).
- Detterbeck, F.C.; Boffa, D.J.; Kim, A.W.; Tanoue, L.T. The Eighth Edition Lung Cancer Stage Classification. Chest 2017, 151, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Chadha, A.S.; Ganti, A.K.; Sohi, J.S.; Sahmoun, A.E.; Mehdi, S.A. Survival in Untreated Early Stage Non-small Cell Lung Cancer. Anticancer Res. 2005, 25, 3517–3520. Available online: https://ar.iiarjournals.org/content/25/5/3517 (accessed on 1 November 2022). [PubMed]
- Wao, H.; Mhaskar, R.; Kumar, A.; Miladinovic, B.; Djulbegovic, B. Survival of patients with non-small cell lung cancer without treatment: A systematic review and meta-analysis. Syst. Rev. 2013, 2, 10. [Google Scholar] [CrossRef]
- Prabhakar, C.N.; Fong, K.M.; Peake, M.D.; Lam, D.C.; Barnes, D.J. The effectiveness of lung cancer MDT and the role of respiratory physicians. Respirology 2015, 20, 884–888. [Google Scholar] [CrossRef]
- Hardavella, G.; Frille, A.; Theochari, C.; Keramida, E.; Bellou, E.; Fotineas, A.; Bracka, I.; Pappa, L.; Zagana, V.; Palamiotou, M.; et al. Multidisciplinary care models for patients with lung cancer. Breathe 2020, 16, 200076. [Google Scholar] [CrossRef]
- Shin, S.H.; Shin, S.; Im, Y.; Lee, G.; Jeong, B.H.; Lee, K.; Um, S.W.; Kim, H.; Kwon, O.J.; Cho, J.H.; et al. Effect of perioperative bronchodilator therapy on postoperative pulmonary function among lung cancer patients with COPD. Sci. Rep. 2021, 11, 8359. [Google Scholar] [CrossRef]
- Bölükbas, S.; Eberlein, M.; Eckhoff, J.; Schirren, J. Short-term effects of inhalative tiotropium/formoterol/budenoside versus tiotropium/formoterol in patients with newly diagnosed chronic obstructive pulmonary disease requiring surgery for lung cancer: A prospective randomized trial. Eur. J. Cardio-Thorac. Surg. 2011, 39, 995–1000. [Google Scholar] [CrossRef]
- Kobayashi, S.; Suzuki, S.; Niikawa, H.; Sugawara, T.; Yanai, M. Preoperative use of inhaled tiotropium in lung cancer patients with untreated COPD. Respirology 2009, 14, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Ajimizu, H.; Ozasa, H.; Sato, S.; Funazo, T.; Sakamori, Y.; Nomizo, T.; Kuninaga, K.; Ogimoto, T.; Hosoya, K.; Yamazoe, M.; et al. Survival impact of treatment for chronic obstructive pulmonary disease in patients with advanced non-small-cell lung cancer. Sci. Rep. 2021, 11, 23677. [Google Scholar] [CrossRef]
- Goffini, J.R.; Corriveau, S.; Tang, G.H.; Pond, G.R. Management and outcomes of patients with chronic obstructive lung disease and lung cancer in a public healthcare system. PLoS ONE 2021, 16, e0251886. [Google Scholar] [CrossRef] [PubMed]
- Su, S.F.; Hu, Y.X.; Ouyang, W.W.; Ma, Z.; Lu, B.; Li, Q.S.; Li, H.Q.; Wang, Z.Y.; Wang, Y. The survival outcomes and prognosis of stage IV non-small-cell lung cancer treated with thoracic three-dimensional radiotherapy combined with chemotherapy. Radiat. Oncol. 2014, 9, 290. [Google Scholar] [CrossRef] [PubMed]
- Golemiec, B.; Mullin, M.L.; Linton, S.; Howard, T.; Dhillon, G.R.; DaBreo, D.; Parker, C.M.; Digby, G.C. Expediting specialist referral for patients with suspected lung cancer through standardization of radiologist reporting. Can. J. Respir. Crit. Care Sleep Med. 2022, 6, 221–228. [Google Scholar] [CrossRef]



| LDAP | Non-LDAP | |||
|---|---|---|---|---|
| N (%) | 95% CI | N (%) | 95% CI | |
| Stage I (p < 0.0001) | ||||
| Surgery | 55 (23.1%) | 16.9–30.8% | 48 (33.8%) | 24.5–44.5% |
| Radiation Therapy | 146 (61.3%) | 53.0–69.1% | 54 (38.0%) | 28.3–48.8% |
| Systemic Therapy | 2 (0.8%) | 0.2–4.2% | 3 (2.1%) | 0.5–8.0% |
| Chemoradiation | 11 (4.6%) | 2.2–9.5% | 4 (2.8%) | 0.8–9.0% |
| No Treatments | 24 (10.1%) | 6.1–16.2% | 33 (23.2%) | 15.4–33.4% |
| Stage II (p = 0.4160) | ||||
| Surgery | 29 (42.6%) | 28.5–58.1% | 12 (31.6%) | 16.2–52.4% |
| Radiation Therapy | 26 (38.2%) | 24.8–53.8% | 15 (39.5%) | 22.1–59.9% |
| Systemic Therapy | 1 (1.5%) | 0.2–11.4% | 2 (5.3%) | 1.0–22.8% |
| Chemoradiation | 7 (10.3%) | 4.1–23.5% | 3 (7.9%) | 2.0–26.3% |
| No Treatments | 5 (7.4%) | 2.5–19.8% | 6 (15.8) | 5.9–35.8% |
| Stage III (p = 0.0627) | ||||
| Surgery | 17 (11.1%) | 6.1–19.3% | 11 (9.6%) | 4.6–19.1% |
| Radiation Therapy | 52 (34.0%) | 25.0–44.3% | 23 (20.2%) | 12.3–31.4% |
| Systemic Therapy | 16 (10.5%) | 5.6–18.6% | 12 (10.5%) | 5.2–20.2% |
| Chemoradiation | 52 (34.0%) | 25.0–44.3% | 46 (40.4%) | 29.4–52.4% |
| No Treatments | 16 (10.5%) | 5.6–18.6% | 22 (19.3%) | 11.6–30.4% |
| Stage IV (p < 0.0001) | ||||
| Surgery | 3 (1.1%) | 0.3–4.4% | 6 (1.5%) | 0.5–4.0% |
| Radiation Therapy | 81 (30.7%) | 23.9–38.4% | 135 (33.4%) | 27.7–39.7% |
| Systemic Therapy | 54 (20.5%) | 14.8–27.5% | 64 (15.8%) | 11.7–21.1% |
| Chemoradiation | 96 (36.4%) | 29.2–44.2% | 81 (20.0%) | 15.4–25.6% |
| No Treatments | 30 (11.4%) | 7.3–17.4% | 118 (29.2%) | 23.8–35.3% |
| Unknown Stage (p < 0.0001) | ||||
| Surgery | 25 (26.3%) | 16.5–39.2% | 19 (8.5%) | 4.8–14.6% |
| Radiation Therapy | 33 (34.7%) | 23.5–47.9% | 33 (14.7%) | 9.7–21.8% |
| Systemic Therapy | 4 (4.2%) | 1.3–13.1% | 22 (9.8%) | 5.8–16.2% |
| Chemoradiation | 15 (15.8%) | 8.4–27.6% | 13 (5.8%) | 2.9–11.2% |
| No Treatments | 18 (18.9%) | 10.8–31.2% | 137 (61.2%) | 52.6–69.1% |
| Overall (p < 0.0001) | ||||
| Surgery | 129 (15.8%) | 12.8–19.3% | 97 (10.5%) | 8.1–13.3% |
| Radiation Therapy | 338 (41.3%) | 37.0–45.8% | 260 (28.2%) | 24.5–32.1% |
| Systemic Therapy | 77 (9.4%) | 7.1–12.4% | 103 (11.2%) | 8.8–14.1% |
| Chemoradiation | 181 (22.1%) | 18.6–26.1% | 147 (15.9%) | 13.1–19.3% |
| No Treatments | 93 (11.4%) | 8.8–14.5% | 317 (34.3%) | 30.4–38.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlGhamdi, S.; Kong, W.; Brundage, M.; Eisenhauer, E.A.; Parker, C.M.; Digby, G.C. Characterizing Variability in Lung Cancer Outcomes and Influence of a Lung Diagnostic Assessment Program in Southeastern Ontario, Canada. Curr. Oncol. 2023, 30, 4880-4896. https://doi.org/10.3390/curroncol30050368
AlGhamdi S, Kong W, Brundage M, Eisenhauer EA, Parker CM, Digby GC. Characterizing Variability in Lung Cancer Outcomes and Influence of a Lung Diagnostic Assessment Program in Southeastern Ontario, Canada. Current Oncology. 2023; 30(5):4880-4896. https://doi.org/10.3390/curroncol30050368
Chicago/Turabian StyleAlGhamdi, Shahad, Weidong Kong, Michael Brundage, Elizabeth A. Eisenhauer, Christopher M. Parker, and Geneviève C. Digby. 2023. "Characterizing Variability in Lung Cancer Outcomes and Influence of a Lung Diagnostic Assessment Program in Southeastern Ontario, Canada" Current Oncology 30, no. 5: 4880-4896. https://doi.org/10.3390/curroncol30050368