The Effect of Contemporary Brachytherapy Practices on Prognosis in Women with Locally Advanced Cervical Cancer

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
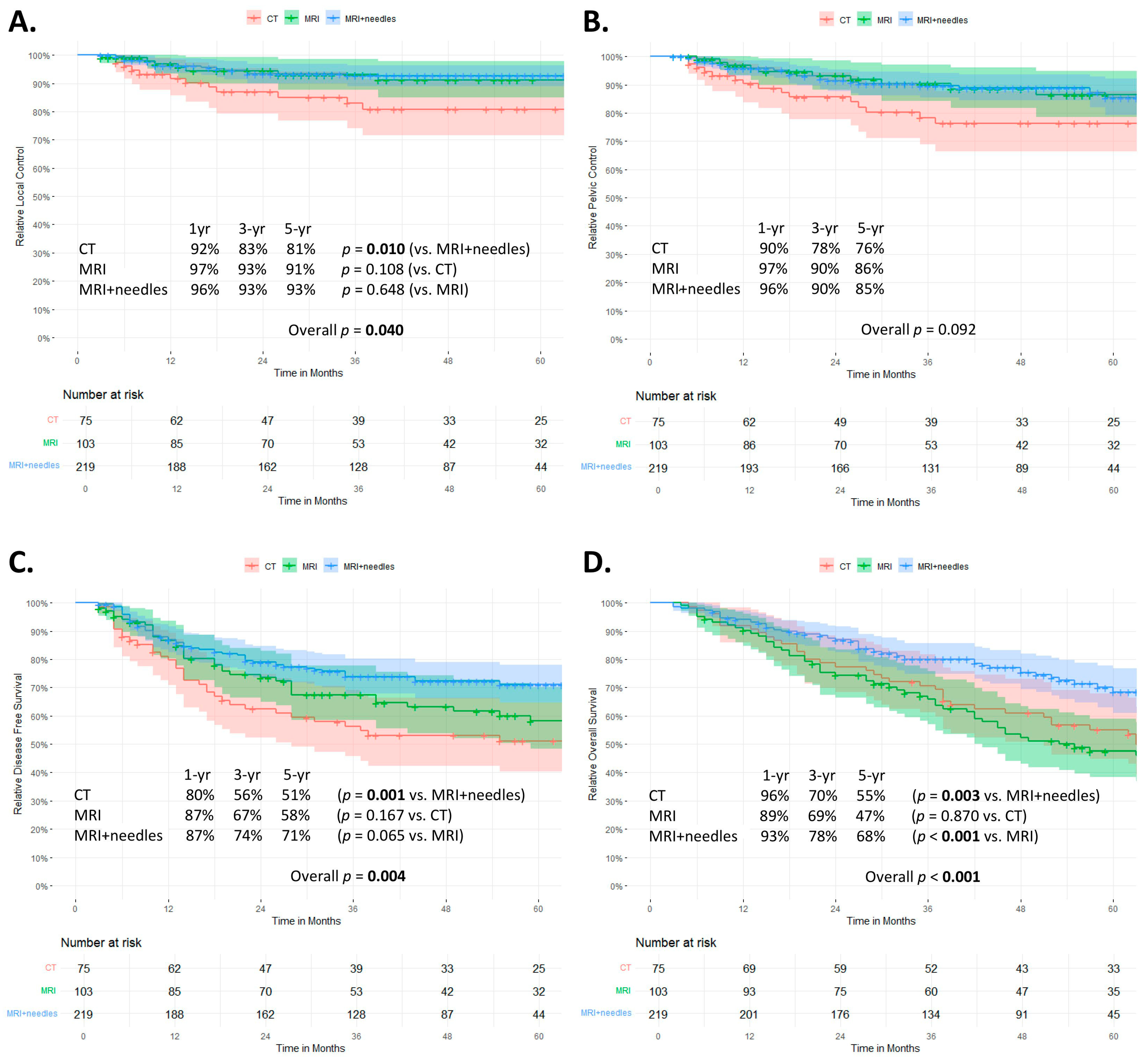
3.2. Survival
3.3. Risk Factors
3.4. Toxicity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rose, P.G.; Bundy, B.N.; Watkins, E.B.; Thigpen, J.T.; Deppe, G.; Maiman, M.A.; Clarke-Pearson, D.L.; Insalaco, S. Concurrent Cisplatin-Based Radiotherapy and Chemotherapy for Locally Advanced Cervical Cancer. N. Engl. J. Med. 1999, 340, 1144–1153. [Google Scholar] [CrossRef]
- Morris, M.; Eifel, P.J.; Lu, J.; Grigsby, P.W.; Levenback, C.; Stevens, R.E.; Rotman, M.; Gershenson, D.M.; Mutch, D.G. Pelvic Radiation with Concurrent Chemotherapy Compared with Pelvic and Para-Aortic Radiation for High-Risk Cervical Cancer. N. Engl. J. Med. 1999, 340, 1137–1143. [Google Scholar] [CrossRef]
- Tod, M.; Meredith, W.J. Treatment of Cancer of the Cervix Uteri, a Revised Manchester Method. Br. J. Radiol. 1953, 26, 252–257. [Google Scholar] [CrossRef]
- Haie-Meder, C.; Pötter, R.; Van Limbergen, E.; Briot, E.; De Brabandere, M.; Dimopoulos, J.; Dumas, I.; Hellebust, T.P.; Kirisits, C.; Lang, S.; et al. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (I): Concepts and Terms in 3D Image Based 3D Treatment Planning in Cervix Cancer Brachytherapy with Emphasis on MRI Assessment of GTV and CTV. Radiother. Oncol. 2005, 74, 235–245. [Google Scholar] [CrossRef]
- Pötter, R.; Haie-Meder, C.; Van Limbergen, E.; Barillot, I.; De Brabandere, M.; Dimopoulos, J.; Dumas, I.; Erickson, B.; Lang, S.; Nulens, A.; et al. Recommendations from Gynaecological (GYN) GEC ESTRO Working Group (II): Concepts and Terms in 3D Image-Based Treatment Planning in Cervix Cancer Brachytherapy—3D Dose Volume Parameters and Aspects of 3D Image-Based Anatomy, Radiation Physics, Radiobiolo. Radiother. Oncol. 2006, 78, 67–77. [Google Scholar] [CrossRef]
- Tanderup, K.; Nielsen, S.K.; Nyvang, G.B.; Pedersen, E.M.; Røhl, L.; Aagaard, T.; Fokdal, L.; Lindegaard, J.C. From Point A to the Sculpted Pear: MR Image Guidance Significantly Improves Tumour Dose and Sparing of Organs at Risk in Brachytherapy of Cervical Cancer. Radiother. Oncol. 2010, 94, 173–180. [Google Scholar] [CrossRef]
- Harkenrider, M.M.; Alite, F.; Silva, S.R.; Small, W. Image-Based Brachytherapy for the Treatment of Cervical Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 921–934. [Google Scholar] [CrossRef]
- Kirisits, C.; Lang, S.; Dimopoulos, J.; Berger, D.; Georg, D.; Pötter, R. The Vienna Applicator for Combined Intracavitary and Interstitial Brachytherapy of Cervical Cancer: Design, Application, Treatment Planning, and Dosimetric Results. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 624–630. [Google Scholar] [CrossRef]
- Nomden, C.N.; De Leeuw, A.A.C.; Moerland, M.A.; Roesink, J.M.; Tersteeg, R.J.H.A.; Jürgenliemk-Schulz, I.M. Clinical Use of the Utrecht Applicator for Combined Intracavitary/ Interstitial Brachytherapy Treatment in Locally Advanced Cervical Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1424–1430. [Google Scholar] [CrossRef]
- Fokdal, L.; Sturdza, A.; Mazeron, R.; Haie-Meder, C.; Tan, L.T.; Gillham, C.; Šegedin, B.; Jürgenliemk-Schultz, I.; Kirisits, C.; Hoskin, P.; et al. Image Guided Adaptive Brachytherapy with Combined Intracavitary and Interstitial Technique Improves the Therapeutic Ratio in Locally Advanced Cervical Cancer: Analysis from the RetroEMBRACE Study. Radiother. Oncol. 2016, 120, 434–440. [Google Scholar] [CrossRef]
- Tan, L.T.; Coles, C.E.; Hart, C.; Tait, E. Clinical Impact of Computed Tomography-Based Image-Guided Brachytherapy for Cervix Cancer Using the Tandem-Ring Applicator—The Addenbrooke’s Experience. Clin. Oncol. 2009, 21, 175–182. [Google Scholar] [CrossRef]
- Charra-Brunaud, C.; Harter, V.; Delannes, M.; Haie-Meder, C.; Quetin, P.; Kerr, C.; Castelain, B.; Thomas, L.; Peiffert, D. Impact of 3D Image-Based PDR Brachytherapy on Outcome of Patients Treated for Cervix Carcinoma in France: Results of the French STIC Prospective Study. Radiother. Oncol. 2012, 103, 305–313. [Google Scholar] [CrossRef]
- Pötter, R.; Dimopoulos, J.; Georg, P.; Lang, S.; Waldhäusl, C.; Wachter-Gerstner, N.; Weitmann, H.; Reinthaller, A.; Knocke, T.H.; Wachter, S.; et al. Clinical Impact of MRI Assisted Dose Volume Adaptation and Dose Escalation in Brachytherapy of Locally Advanced Cervix Cancer. Radiother. Oncol. 2007, 83, 148–155. [Google Scholar] [CrossRef]
- Pötter, R.; Georg, P.; Dimopoulos, J.C.A.; Grimm, M.; Berger, D.; Nesvacil, N.; Georg, D.; Schmid, M.P.; Reinthaller, A.; Sturdza, A.; et al. Clinical Outcome of Protocol Based Image (MRI) Guided Adaptive Brachytherapy Combined with 3D Conformal Radiotherapy with or without Chemotherapy in Patients with Locally Advanced Cervical Cancer. Radiother. Oncol. 2011, 100, 116–123. [Google Scholar] [CrossRef]
- FIGO Committee on Gynecologic Oncology. Current FIGO Staging for Cancer of the Vagina, Fallopian Tube, Ovary, and Gestational Trophoblastic Neoplasia. Int. J. Gynaecol. Obstet. 2009, 105, 3–4. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Davis, T.E. Toxicology and Response Criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. Cancer Clin. Trials 1982, 5, 649–656. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN Guidelines on Definitions and Terminology of Clinical Nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Manders, D.B.; Morón, A.; McIntire, D.; Miller, D.S.; Richardson, D.L.; Kehoe, S.M.; Albuquerque, K.V.; Lea, J.S. Locally Advanced Cervical Cancer: Outcomes with Variable Adherence to Treatment. Am. J. Clin. Oncol. Cancer Clin. Trials 2018, 41, 447–451. [Google Scholar] [CrossRef]
- Song, S.; Rudra, S.; Hasselle, M.D.; Dorn, P.L.; Mell, L.K.; Mundt, A.J.; Yamada, S.D.; Lee, N.K.; Hasan, Y. The Effect of Treatment Time in Locally Advanced Cervical Cancer in the Era of Concurrent Chemoradiotherapy. Cancer 2013, 119, 325–331. [Google Scholar] [CrossRef]
- National Cancer Institute, National Institutes of Health. US Department of Health and Human Services: Common Terminology Criteria for Adverse Events (CTCAE) (Version 4.03). Available online: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf (accessed on 1 October 2021).
- Derks, K.; Steenhuijsen, J.L.G.; Van Den Berg, H.A.; Houterman, S.; Cnossen, J.; Van Haaren, P.; De Jaeger, K. Impact of Brachytherapy Technique (2D versus 3D) on Outcome Following Radiotherapy of Cervical Cancer. J. Contemp. Brachyther. 2018, 10, 17–25. [Google Scholar] [CrossRef]
- Sturdza, A.; Pötter, R.; Fokdal, L.U.; Haie-Meder, C.; Tan, L.T.; Mazeron, R.; Petric, P.; Šegedin, B.; Jurgenliemk-Schulz, I.M.; Nomden, C.; et al. Image Guided Brachytherapy in Locally Advanced Cervical Cancer: Improved Pelvic Control and Survival in RetroEMBRACE, a Multicenter Cohort Study. Radiother. Oncol. 2016, 120, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Horeweg, N.; Creutzberg, C.L.; Rijkmans, E.C.; Laman, M.S.; Velema, L.A.; Coen, V.L.M.A.; Stam, T.C.; Kerkhof, E.M.; Kroep, J.R.; De Kroon, C.D.; et al. Efficacy and Toxicity of Chemoradiation with Image-Guided Adaptive Brachytherapy for Locally Advanced Cervical Cancer. Int. J. Gynecol. Cancer 2019, 29, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Hansen, H.; Loft, A.; Berthelsen, A.; Christensen, I.; Høgdall, C.; Engelholm, S. Introducing PET/CT in Cervical Cancer Staging Procedures Leads to Stage Migration and Selection Bias. Int. J. Radiat. Oncol. 2014, 90, S481–S482. [Google Scholar] [CrossRef]
- Rijkmans, E.C.; Nout, R.A.; Rutten, I.H.H.M.; Ketelaars, M.; Neelis, K.J.; Laman, M.S.; Coen, V.L.M.A.; Gaarenstroom, K.N.; Kroep, J.R.; Creutzberg, C.L. Improved Survival of Patients with Cervical Cancer Treated with Image-Guided Brachytherapy Compared with Conventional Brachytherapy. Gynecol. Oncol. 2014, 135, 231–238. [Google Scholar] [CrossRef]
- Pötter, R.; Tanderup, K.; Schmid, M.P.; Jürgenliemk-Schulz, I.; Haie-Meder, C.; Fokdal, L.U.; Sturdza, A.E.; Hoskin, P.; Mahantshetty, U.; Segedin, B.; et al. MRI-Guided Adaptive Brachytherapy in Locally Advanced Cervical Cancer (EMBRACE-I): A Multicentre Prospective Cohort Study. Lancet Oncol. 2021, 22, 538–547. [Google Scholar] [CrossRef]
- Majercakova, K.; Pötter, R.; Kirisits, C.; Banerjee, S.; Sturdza, A.E.; Georg, P.; Nesvacil, N.; Schmid, M.P. Evaluation of Planning Aims and Dose Prescription in Image-Guided Adaptive Brachytherapy and Radiochemotherapy for Cervical Cancer: Vienna Clinical Experience in 225 Patients from 1998 to 2008. Acta Oncol. 2015, 54, 1551–1557. [Google Scholar] [CrossRef]
- National Cancer Institute, National Institutes of Health. US Department of Health and Human Services: Common Terminology Criteria for Adverse Events (CTCAE) (Version 3.0). Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcaev3.pdf (accessed on 1 October 2022).
- Gandhi, A.K.; Sharma, D.N.; Rath, G.K.; Julka, P.K.; Subramani, V.; Sharma, S.; Manigandan, D.; Laviraj, M.A.; Kumar, S.; Thulkar, S. Early Clinical Outcomes and Toxicity of Intensity Modulated versus Conventional Pelvic Radiation Therapy for Locally Advanced Cervix Carcinoma: A Prospective Randomized Study. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 542–548. [Google Scholar] [CrossRef]
- Dröge, L.H.; von Sivers, F.F.; Schirmer, M.A.; Wolff, H.A. Conventional 3D Conformal Radiotherapy and Volumetric Modulated Arc Therapy for Cervical Cancer: Comparison of Clinical Results with Special Consideration of the Influence of Patient- and Treatment-Related Parameters. Strahlenther. Onkol. 2021, 197, 520–527. [Google Scholar] [CrossRef]
- Tanderup, K.; Fokdal, L.U.; Sturdza, A.; Haie-Meder, C.; Mazeron, R.; van Limbergen, E.; Jürgenliemk-Schulz, I.; Petric, P.; Hoskin, P.; Dörr, W.; et al. Effect of Tumor Dose, Volume and Overall Treatment Time on Local Control after Radiochemotherapy Including MRI Guided Brachytherapy of Locally Advanced Cervical Cancer. Radiother. Oncol. 2016, 120, 441–446. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | CT | MRI | MRI+Needles | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| n = 75 | (%) IQR | n = 103 | (%) IQR | n = 219 | (%) IQR | |||
| Age 1 | Median | 55 | 42–71 | 60 | 44–72 | 53 | 41–67 | 0.136 |
| WHO Performance score | 0 | 43 | (57) | 58 | (56) | 142 | (65) | 0.254 |
| ≥1 | 32 | (43) | 45 | (44) | 77 | (35) | ||
| Smoking | Smoker * | 36 a,b | (48) | 47 b | (46) | 128 a | (58) | 0.023 |
| never smoked | 38 a,b | (51) | 56 b | (54) | 83 a | (38) | ||
| missing | 1 | (1) | 0 | (0) | 8 | (11) | ||
| Nutritional status | malnourished | 8 | (10) | 8 | (8) | 15 | (7) | 0.209 |
| not malnourished | 47 | (63) | 79 | (77) | 196 | (89) | ||
| missing | 20 | (27) | 16 | (15) | 8 | (4) | ||
| Hypertension | yes | 20 a,b | (27) | 36 b | (35) | 44 a | (20) | 0.016 |
| no | 55 a,b | (73) | 67 b | (65) | 175 a | (80) | ||
| Diabetes Mellitus | yes | 6 | (8) | 9 | (9) | 15 | (7) | 0.842 |
| no | 69 | (92) | 94 | (91) | 204 | (93) | ||
| FIGO stage 2 | I | 18 a | (24) | 19 a | (18) | 62 a | (28) | 0.043 |
| II | 32 a | (43) | 43 a | (42) | 100 a | (46) | ||
| III | 18 a | (24) | 29 a | (28) | 46 a | (21) | ||
| IV | 7 a,b | (9) | 12 b | (12) | 11 a | (5) | ||
| Histology | SCC | 67 | (89) | 88 | (85) | 185 | (85) | 0.612 |
| Adeno(squamous) | 8 | (11) | 15 | (15) | 34 | (15) | ||
| Nodal status | N1 | 37 | (49) | 46 | (45) | 115 | (52) | 0.417 |
| N0 | 38 | (51) | 57 | (55) | 104 | (48) | ||
| PET-CT scan | yes | 34 a | (45) | 76 b | (74) | 189 c | (86) | <0.001 |
| no | 41 a | (55) | 27 b | (26) | 30 c | (14) | ||
| EBRT technique | Box/3D-CRT | 62 a | (83) | 66 b | (64) | 2 c | (1) | <0.001 |
| IMRT/VMAT | 1 a | (1) | 22 b | (21) | 212 c | (97) | ||
| missing | 12 | (16) | 15 | (15) | 5 | (2) | ||
| Chemotherapy | yes | 56 | (75) | 74 | (72) | 154 | (70) | 0.798 |
| no | 19 | (25) | 29 | (28) | 65 | (30) | ||
| Hyperthermia | yes | 16 | (21) | 22 | (21) | 45 | (20) | 0.971 |
| no | 59 | (79) | 81 | (79) | 174 | (80) | ||
| Overall Treatment Time 3 | >50 days | 10 a | (13) | 27 b | (26) | 27 a | (12) | 0.008 |
| Median | 44 | 39–48 | 46 | 43–51 | 45 | 41–49 | 0.027 | |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| Local Control | p-Value | HR (95% CI) | p-Value | HR (95% CI) |
| Smoking: current or former smoker (v never smoked) | 0.800 | 0.92 (0.47–1.80) | ||
| Nutritional status: malnourished at baseline (v not malnourished at baseline) | 0.298 | 0.04 (0.00–15.90) | ||
| Hypertension (v no hypertension) | 0.004 | 2.69 (1.36–5.31) | NA | |
| Diabetes mellitus (v no diabetes mellitus) | 0.744 | 1.22 (0.37–3.99) | ||
| FIGO stage III/IV (v stage I/II) | 0.004 | 2.71 (1.38–5.32) | NA | |
| Histology: adeno (squamous) (v squamous cell) | 0.032 | 2.30 (0.07–4.93) | NA | |
| Overall treatment time 1: >50 (v ≤ 50 days) | 0.397 | 1.43 (0.62–3.30) | NA | |
| Treatment subgroup (v MRI+needles) | 0.049 | NA | ||
| CT | 0.017 | 2.57 (1.19–5.58) | NA | |
| MRI | 0.609 | 1.26 (0.53–3.00) | ||
| Pelvic control | ||||
| Smoking: current or former smoker (v never smoked) | 0.845 | 0.95 (0.54–1.67) | ||
| Nutritional status: malnourished at baseline (v not malnourished at baseline) | 0.441 | 0.57 (0.14–2.37) | ||
| Hypertension (v no hypertension) | 0.143 | 1.58 (0.86–2.90) | ||
| Diabetes mellitus (v no diabetes mellitus) | 0.797 | 1.14 (0.41–3.18) | ||
| FIGO stage III/IV (v stage I/II) | 0.004 | 2.28 (1.30–4.02) | 0.006 | 2.20 (1.25–3.88) |
| Histology: adeno(squamous) (v squamous cell) | 0.163 | 1.64 (0.82–3.29) | ||
| Overall treatment time 1: >50 (v ≤ 50 days) | 0.542 | 1.25 (0.61–2.59) | ||
| Nodal status: N1 (v N0) | 0.021 | 1.99 (1.11–3.59) | 0.031 | 1.91 (1.06–3.45) |
| Treatment subgroup (v MRI+needles) | 0.101 | NS | ||
| CT | 0.041 | 1.98 (1.03–3.80) | ||
| MRI | 0.881 | 1.06 (0.51–2.17) | ||
| Disease-free survival | ||||
| WHO PS: PS 1–4 (v PS 0) | 0.424 | 1.15 (0.81–1.63) | ||
| Smoking: current or former smoker (v never smoked) | 0.397 | 0.86 (0.61–1.22) | ||
| Nutritional status: malnourished at baseline (v not malnourished at baseline) | 0.571 | 0.80 (0.37–1.72) | ||
| Hypertension (v no hypertension) | 0.459 | 1.16 (0.78–1.72) | ||
| Diabetes mellitus (v no diabetes mellitus) | 0.754 | 0.90 (0.46–1.77) | ||
| FIGO stage III/IV (v stage I/II) | <0.001 | 2.21 (1.56–3.12) | <0.001 | 2.13 (1.50–3.03) |
| Histology: adeno(squamous) (v squamous cell) | <0.001 | 2.23 (1.49–3.32) | <0.001 | 2.83 (1.88–4.26) |
| Nodal status: N1 (v N0) | <0.001 | 1.94 (1.36–2.76) | <0.001 | 2.13 (1.49–3.05) |
| Overall treatment time 1: >50 (v ≤ 50 days) | 0.017 | 1.65 (1.09–2.50) | NS | |
| Treatment subgroup (v MRI+needles) | 0.005 | 0.003 | ||
| CT | 0.001 | 2.00 (1.32–3.04) | <0.001 | 2.09 (1.37–3.19) |
| MRI | 0.071 | 1.46 (0.97–2.21) | 0.105 | 1.41 (0.93–2.15) |
| Overall survival | ||||
| Age 2 | <0.001 | 1.03 (1.02–1.04) | <0.001 | 1.03 (1.02–1.04) |
| WHO PS: PS 1–4 (v PS 0) | 0.011 | 1.50 (1.10–2.05) | NS | |
| Smoking: current or former smoker (vs. never smoked) | 0.113 | 0.78 (0.57–1.06) | ||
| Nutritional status: malnourished at baseline (v not malnourished at baseline) | 0.832 | 0.93 (0.50–1.74) | ||
| Hypertension (v no hypertension) | <0.001 | 1.81 (1.30–2.53) | NS | |
| Diabetes mellitus (v no diabetes mellitus) | 0.089 | 1.55 (0.93–2.56) | NS | |
| FIGO stage III/IV (v stage I/II) | <0.001 | 2.26 (1.65–3.10) | <0.001 | 2.11 (1.53–2.90) |
| Histology: adeno (squamous) (v squamous cell) | 0.017 | 1.62 (1.09–2.42) | 0.002 | 1.87 (1.25–2.81) |
| Nodal status: N1 (v N0) | 0.074 | 1.33 (0.97–1.82) | <0.001 | 1.80 (1.28–2.50) |
| Overall treatment time 1: >50 (v ≤ 50 days) | 0.099 | 1.38 (0.94–2.03) | NS | |
| Treatment subgroup (v MRI+needles) | <0.001 | 0.015 | ||
| CT | 0.001 | 1.92 (1.29–2.86) | 0.010 | 1.71 (1.14–2.57) |
| MRI | <0.001 | 1.98 (1.36–2.88) | 0.014 | 1.63 (1.10–2.40) |
| CT | MRI | MRI+Needles | Entire Cohort | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Toxicity Type | n = 75 | (%) | n = 103 | (%) | n = 219 | (%) | n = 397 | (%) | |
| Gastro-intestinal | 9 | (12) | 13 | (13) | 19 | (9) | 41 | (10) | |
| Vaginal | 8 | (11) | 10 | (10) | 20 | (9) | 38 | (10) | |
| Genitourinary | 5 | (7) | 10 | (10) | 4 | (2) | 19 | (5) | |
| Other | 4 | (5) | 2 | (2) | 6 | (3) | 12 | (3) | |
| Overall * | events | 26 | 35 | 49 | 110 | ||||
| patients | 20 | (27) | 27 | (26) | 44 | (20) | 91 | (23) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laan, J.J.; van Lonkhuijzen, L.R.C.W.; Stokking, J.A.; Barten, D.L.J.; Hinnen, K.A.; Pieters, B.R.; Stalpers, L.J.A.; Westerveld, H. The Effect of Contemporary Brachytherapy Practices on Prognosis in Women with Locally Advanced Cervical Cancer. Curr. Oncol. 2023, 30, 4275-4288. https://doi.org/10.3390/curroncol30040326
Laan JJ, van Lonkhuijzen LRCW, Stokking JA, Barten DLJ, Hinnen KA, Pieters BR, Stalpers LJA, Westerveld H. The Effect of Contemporary Brachytherapy Practices on Prognosis in Women with Locally Advanced Cervical Cancer. Current Oncology. 2023; 30(4):4275-4288. https://doi.org/10.3390/curroncol30040326
Chicago/Turabian StyleLaan, Janna J., Luc R. C. W. van Lonkhuijzen, Jaap A. Stokking, Danique L. J. Barten, Karel A. Hinnen, Bradley R. Pieters, Lukas J. A. Stalpers, and Henrike Westerveld. 2023. "The Effect of Contemporary Brachytherapy Practices on Prognosis in Women with Locally Advanced Cervical Cancer" Current Oncology 30, no. 4: 4275-4288. https://doi.org/10.3390/curroncol30040326