Understanding Real-World Treatment Patterns and Clinical Outcomes among Metastatic Melanoma Patients in Alberta, Canada

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Measures and Outcomes
2.3. BRAF Testing
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
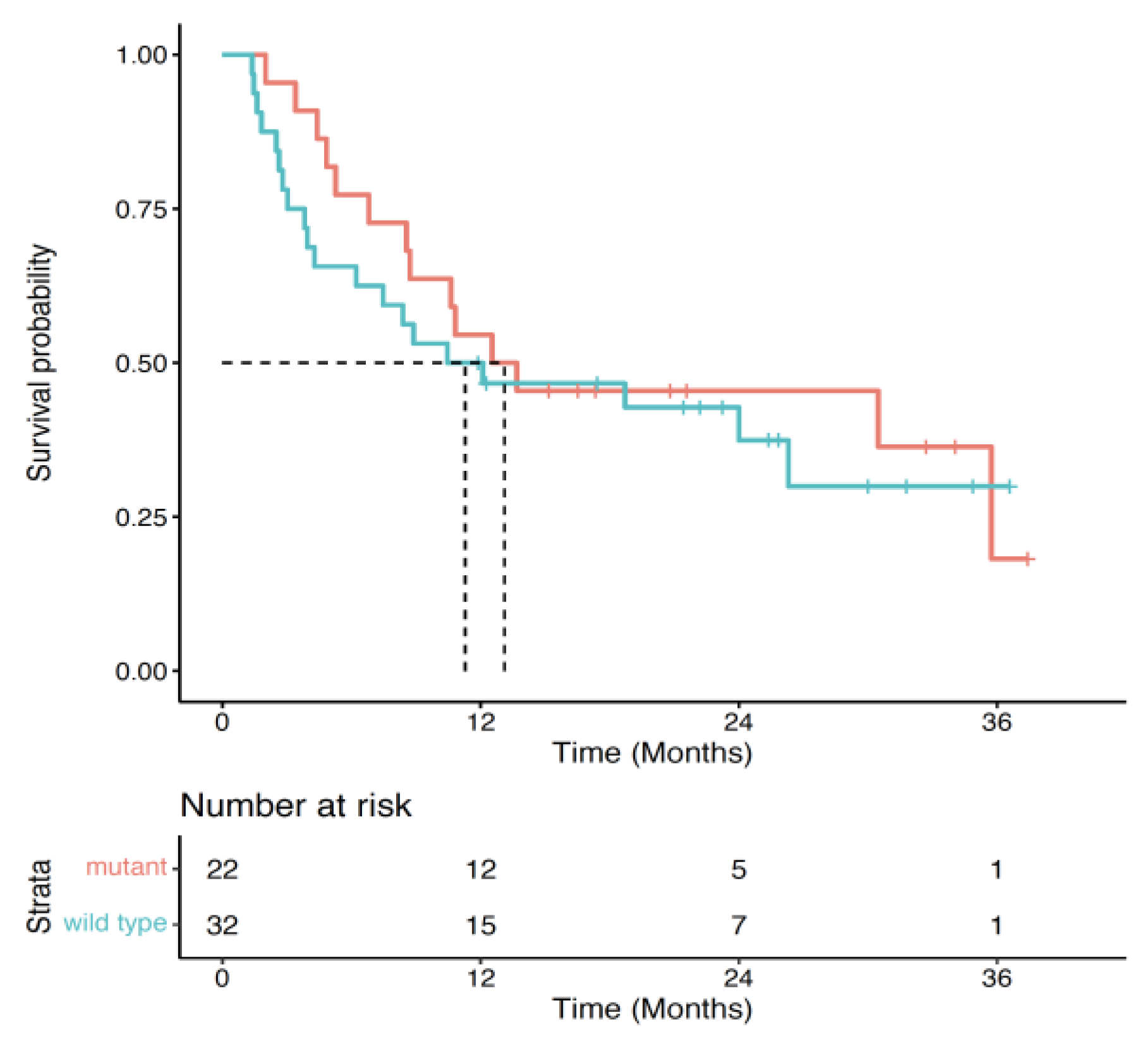
3.2. BRAF Testing
3.3. Treatment Patterns
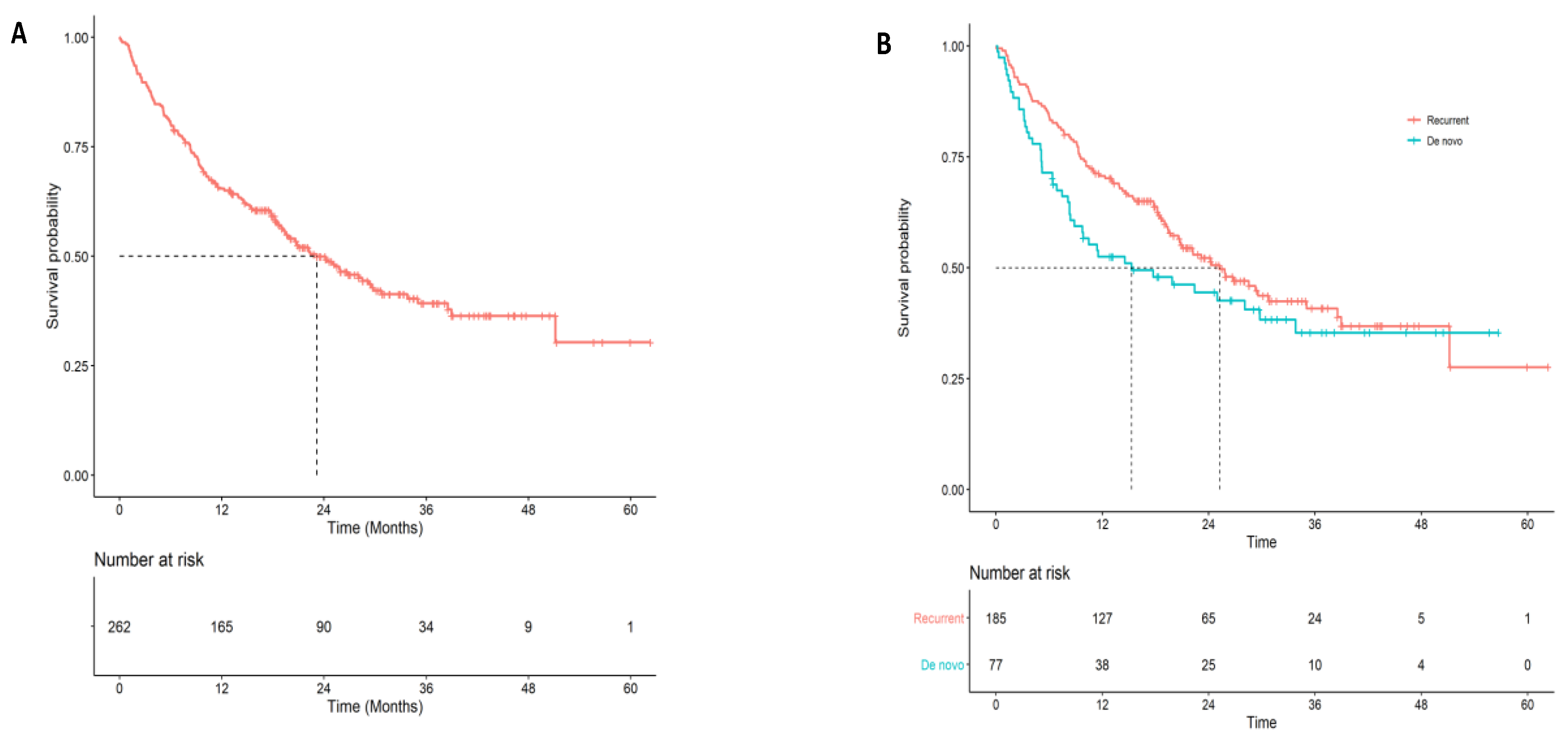
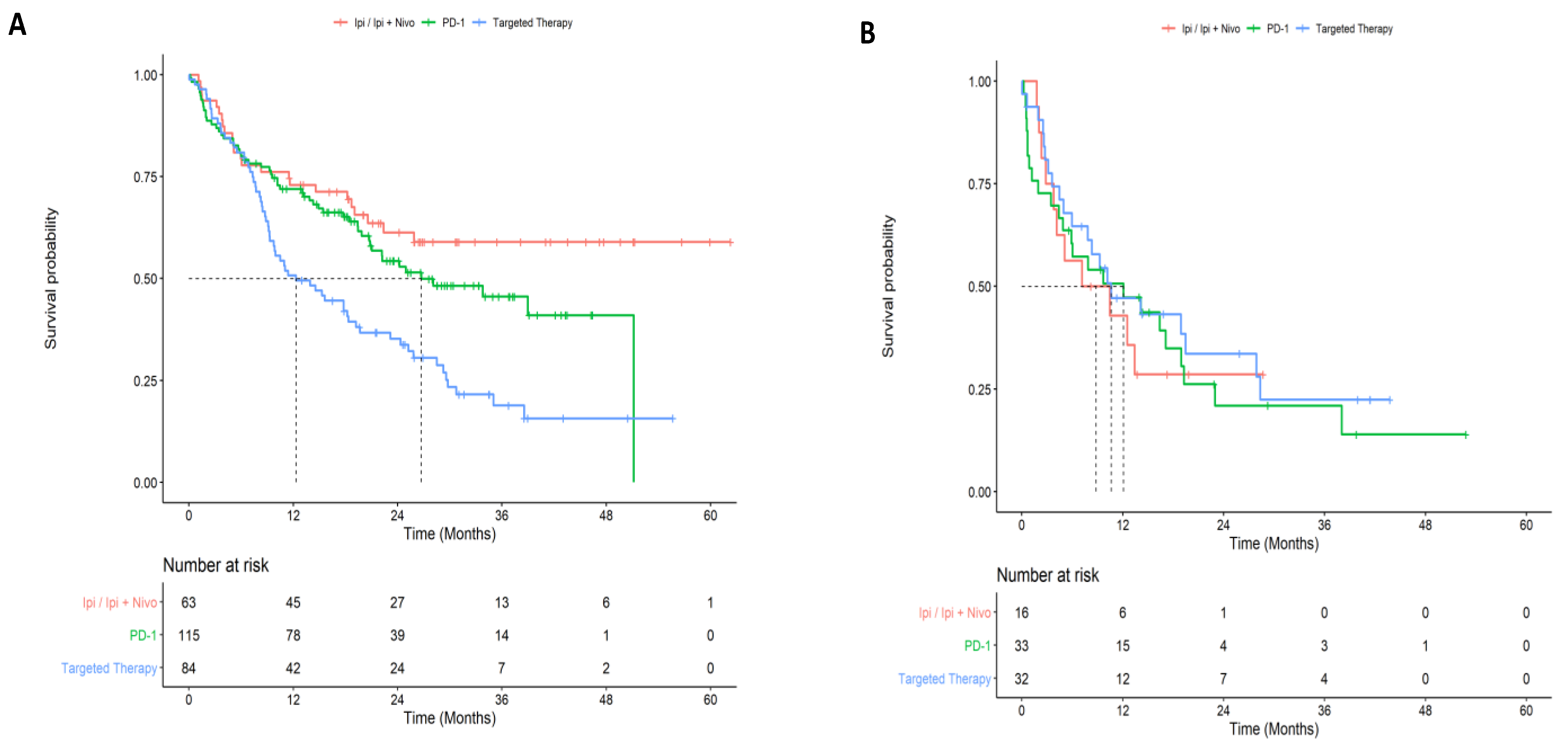
3.4. Survival Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bandarchi, B.; Ma, L.; Navab, R.; Rasty, G. From melanocyte to metastatic malignant melanoma. Dermatol. Res. Pract. 2010, 2010, 583748. [Google Scholar] [CrossRef]
- Balch, C.M.; Buzaid, A.C.; Soong, S.J.; Atkins, M.B.; Cascinelli, N.; Coit, D.G.; Fleming, I.D.; Gershenwald, J.E.; Houghton, A., Jr.; Kirkwood, J.M.; et al. Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma. J. Clin. Oncol. 2001, 19, 3635–3648. [Google Scholar] [CrossRef]
- Tas, F.; Keskin, S.; Karadeniz, A.; Dağoğlu, N.; Sen, F.; Kilic, L.; Yildiz, I. Noncutaneous melanoma have distinct features from each other and cutaneous melanoma. Oncology 2011, 81, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, D.K.; Nathan, P.D. Therapeutic opportunities in noncutaneous melanoma. Ther. Adv. Med. Oncol. 2009, 1, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Brenner, D.R.; Poirier, A.; Woods, R.R.; Ellison, L.F.; Billette, J.M.; Demers, A.A.; Zhang, S.X.; Yao, C.; Finley, C.; Fitzgerald, N.; et al. Projected estimates of cancer in Canada in 2022. CMAJ 2022, 194, E601–E607. [Google Scholar] [CrossRef] [PubMed]
- Ghazawi, F.M.; Le, M.; Alghazawi, N.; Rahme, E.; Moreau, L.; Netchiporouk, E.; Zubarev, A.; Roshdy, O.; Glassman, S.J.; Sasseville, D.; et al. Trends in incidence of cutaneous malignant melanoma in Canada: 1992–2010 versus 2011–2015. J. Am. Acad. Dermatol. 2019, 80, 1157–1159. [Google Scholar] [CrossRef] [Green Version]
- O’Sullivan, D.E.; Brenner, D.R.; Villeneuve, P.J.; Walter, S.D.; Demers, P.A.; Friedenreich, C.M.; King, W.D.; ComPARe Study Team. Estimates of the current and future burden of melanoma attributable to ultraviolet radiation in Canada. Prev. Med. 2019, 122, 81–90. [Google Scholar] [CrossRef]
- Abbasi, N.R.; Shaw, H.M.; Rigel, D.S.; Friedman, R.J.; McCarthy, W.H.; Osman, I.; Kopf, A.W.; Polsky, D. Early diagnosis of cutaneous melanoma: Revisiting the ABCD criteria. JAMA 2004, 292, 2771–2776. [Google Scholar] [CrossRef]
- Markovic, S.N.; Erickson, L.A.; Rao, R.D.; Weenig, R.H.; Pockaj, B.A.; Bardia, A.; Vachon, C.M.; Schild, S.E.; McWilliams, R.R.; Hand, J.L.; et al. Malignant melanoma in the 21st century, part 1: Epidemiology, risk factors, screening, prevention, and diagnosis. Mayo Clin. Proc. 2007, 82, 364–380. [Google Scholar] [CrossRef] [PubMed]
- Ernst, D.S.; Petrella, T.; Joshua, A.M.; Hamou, A.; Thabane, M.; Vantyghem, S.; Gwadry-Sridhar, F. Burden of illness for metastatic melanoma in Canada, 2011–2013. Curr. Oncol. 2016, 23, e563–e570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fusi, S.; Ariyan, S.; Sternlicht, A. Data on first recurrence after treatment for malignant melanoma in a large patient population. Plast. Reconstr. Surg. 1993, 91, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Francken, A.B.; Accortt, N.A.; Shaw, H.M.; Colman, M.H.; Wiener, M.; Soong, S.J.; Hoekstra, H.J.; Thompson, J.F. Follow-up schedules after treatment for malignant melanoma. Br. J. Surg. 2008, 95, 1401–1407. [Google Scholar] [CrossRef] [PubMed]
- Maverakis, E.; Cornelius, L.A.; Bowen, G.M.; Phan, T.; Patel, F.B.; Fitzmaurice, S.; He, Y.; Burrall, B.; Duong, C.; Kloxin, A.M.; et al. Metastatic melanoma—A review of current and future treatment options. Acta. Derm. Venereol. 2015, 95, 516–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domingues, B.; Lopes, J.M.; Soares, P.; Pópulo, H. Melanoma treatment in review. Immunotargets Ther. 2018, 7, 35–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, D.S.; Mellman, I. Elements of cancer immunity and the cancer-immune set point. Nature 2017, 541, 321–330. [Google Scholar] [CrossRef]
- Aroldi, F.; Middleton, M.R. Long-term outcomes of immune checkpoint inhibition in metastatic melanoma. Am. J. Clin. Dermatol. 2022, 23, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Cowey, C.L.; Liu, F.X.; Boyd, M.; Aguilar, K.M.; Krepler, C. Real-world treatment patterns and clinical outcomes among patients with advanced melanoma: A retrospective, community oncology-based cohort study (A STROBE-compliant article). Medicine 2019, 98, e16328. [Google Scholar] [CrossRef]
- Atkinson, V.; Sandhu, S.; Hospers, G.; Long, G.V.; Aglietta, M.; Ferrucci, P.F.; Tulyte, S.; Cappellini, G.C.A.; Soriano, V.; Ali, S.; et al. Dabrafenib plus trametinib is effective in the treatment of BRAF V600-mutated metastatic melanoma patients: Analysis of patients from the dabrafenib plus trametinib Named Patient Program (DESCRIBE II). Melanoma Res. 2020, 30, 261–267. [Google Scholar] [CrossRef]
- Liu, F.X.; Ou, W.; Diede, S.J.; Whitman, E.D. Real-world experience with pembrolizumab in patients with advanced melanoma: A large retrospective observational study. Medicine 2019, 98, e16542. [Google Scholar] [CrossRef]
- Sassolas, B.; Leccia, M.T.; Godard, C.; Benmahamed, L.; Flinois, A.; Levy-Bachelot, L.; Bédane, C. Real-world treatment patterns and clinical outcomes in advanced cutaneous melanoma patients in France. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 587–594. [Google Scholar] [CrossRef]
- Suo, A.; Chan, Y.; Beaulieu, C.; Kong, S.; Cheung, W.Y.; Monzon, J.G.; Smylie, M.; Walker, J.; Morris, D.; Cheng, T. Anti-PD1-Induced Immune-Related Adverse Events and Survival Outcomes in Advanced Melanoma. Oncologist 2020, 25, 438–446. [Google Scholar] [CrossRef] [Green Version]
- Hanna, T.P.; Nguyen, P.; Baetz, T.; Booth, C.M.; Eisenhauer, E. A Population-based Study of Survival Impact of New Targeted and Immune-based Therapies for Metastatic or Unresectable Melanoma. Clin. Oncol. 2018, 30, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Rigo, R.; Doherty, J.; Koczka, K.; Kong, S.; Ding, P.Q.; Cheng, T.; Cheung, W.Y.; Monzon, J.G. Real World Outcomes in Patients with Advanced Melanoma Treated in Alberta, Canada: A Time-Era Based Analysis. Curr. Oncol. 2021, 28, 3978–3986. [Google Scholar] [CrossRef]
- Xu, Y.; Kong, S.; Cheung, W.Y.; Bouchard-Fortier, A.; Dort, J.C.; Quan, H.; Buie, E.M.; McKinnon, G.; Quan, M.L. Development and validation of case-finding algorithms for recurrence of breast cancer using routinely collected administrative data. BMC Cancer 2019, 19, 210. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]
- Normand, S.T.; Landrum, M.B.; Guadagnoli, E.; Ayanian, J.Z.; Ryan, T.J.; Cleary, P.D.; McNeil, B.J. Validating recommendations for coronary angiography following acute myocardial infarction in the elderly: A matched analysis using propensity scores. J. Clin. Epidemiol. 2001, 54, 387–398. [Google Scholar] [CrossRef]
- Nicholas, M.N.; Khoja, L.; Atenafu, E.G.; Hogg, D.; Quirt, I.; Butler, M.; Joshua, A.M. Prognostic factors for first-line therapy and overall survival of metastatic uveal melanoma: The Princess Margaret Cancer Centre experience. Melanoma Res. 2018, 28, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Hanna, T.P.; Chauvin, C.; Miao, Q.; Rizkalla, M.; Reid, K.; Peng, Y.; Nguyen, P.; Jalink, D.; Nanji, S. Clinical Outcomes After Pulmonary Metastasectomy for Melanoma: A Population-Based Study. Ann. Thorac. Surg. 2018, 106, 1675–1681. [Google Scholar] [CrossRef] [PubMed]
- Bremner, S.; Lapierre, M.; Fraelic, A.; Stewart, D. Second-line drug regimens in metastatic melanoma patients based on BRAF mutation status: A Canadian real-world retrospective study. J. Clin. Oncol. 2016, 34, e21054. [Google Scholar] [CrossRef]
- Lapierre, M. Real-World Comparison of Metastatic Melanoma Treatments between Academic and Community Hospitals in Canada: A Retrospective Study. Value Health 2016, 19, A162. [Google Scholar] [CrossRef]
- McCarron, C.; Ernst, S.; Cao, J.Q.; Zaric, G.S. Population-based estimates of survival and cost for metastatic melanoma. Curr. Oncol. 2015, 22, 326–332. [Google Scholar] [CrossRef] [Green Version]
- Sam, D.; Gresham, G.; Abdel-Rahman, O.; Cheung, W.Y. Generalizability of clinical trials of advanced melanoma in the real-world, population-based setting. Med. Oncol. 2018, 35, 110. [Google Scholar] [CrossRef]
- Dai, W.F.; Beca, J.M.; Croxford, R.; Isaranawatchai, W.; Menjak, I.B.; Petrella, T.M.; Mittmann, N.; Earle, C.C.; Gavura, S.; Hanna, T.P.; et al. Real-world comparative effectiveness of second-line ipilimumab for metastatic melanoma: A population-based cohort study in Ontario, Canada. BMC Cancer 2020, 20, 304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoja, L.; Atenafu, E.G.; Ye, Q.; Gedye, C.; Chappell, M.; Hogg, D.; Butler, M.O.; Joshua, A.M. Real-world efficacy, toxicity and clinical management of ipilimumab treatment in metastatic melanoma. Oncol. Lett. 2016, 11, 1581–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitman, E.D.; Liu, F.X.; Cao, X.; Diede, S.J.; Haiderali, A.; Abernethy, A.P. Treatment patterns and outcomes for patients with advanced melanoma in US oncology clinical practices. Future Oncol. 2019, 15, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Moser, J.C.; Chen, D.; Hu-Lieskovan, S.; Grossmann, K.F.; Patel, S.; Colonna, S.V.; Ying, J.; Hyngstrom, J.R. Real-world survival of patients with advanced BRAF V600 mutated melanoma treated with front-line BRAF/MEK inhibitors, anti-PD-1 antibodies, or nivolumab/ipilimumab. Cancer Med. 2019, 8, 7637–7643. [Google Scholar] [CrossRef] [Green Version]
- Mohr, P.; Ascierto, P.; Arance, A.; McArthur, G.; Hernaez, A.; Kaskel, P.; Shinde, R.; Stevinson, K. Real-world treatment patterns and outcomes among metastatic cutaneous melanoma patients treated with ipilimumab. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 962–971. [Google Scholar] [CrossRef]
- Martin-Algarra, S.; Hinshelwood, R.; Mesnage, S.; Cebon, J.; Ferrucci, P.F.; Aglietta, M.; Neyns, B.; Chiarion-Sileni, V.; Lindsay, C.R.; Del Vecchio, M.; et al. Effectiveness of dabrafenib in the treatment of patients with BRAF V600-mutated metastatic melanoma in a Named Patient Program. Melanoma Res. 2019, 29, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Schachter, J.; Ribas, A.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus ipilimumab for advanced melanoma: Final overall survival results of a multicentre, randomised, open-label phase 3 study (KEYNOTE-006). Lancet 2017, 390, 1853–1862. [Google Scholar] [CrossRef]
- Dai, W.F.; Beca, J.; Croxford, R.; Isaranawatchai, W.; Menjak, I.B.; Petrella, T.M.; Mittmann, N.; Earle, C.C.; Gavura, S.; Mercer, R.E.; et al. Real-world, population-based cohort study of toxicity and resource utilization of second-line ipilimumab for metastatic melanoma in Ontario, Canada. Int. J. Cancer 2021, 148, 1910–1918. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | De Novo (n = 110) |
| Demographics | |
| Age, years (median (IQR)) | 65.96 (57.31, 76.31) |
| <65 years (%) | 53 (48.2) |
| ≥65 years (%) | 57 (51.8) |
| Male (%) | 77 (70.0) |
| Socioeconomic Status | |
| Urban Residence (%) | 91 (82.7) |
| Neighborhood Annual Household Income (median (IQR)) | 37,344.46 (31,721.02, 45,489.21) |
| Quintile Neighborhood Annual Household Income (%) | |
| Q1 (poorest) | 15 (13.6) |
| Q2 | 16 (14.5) |
| Q3 | 22 (20.0) |
| Q4 | 25 (22.7) |
| Q5 (richest) | 32 (29.1) |
| Proportion of Neighborhood Residents who achieved a Highschool Education or Greater (median (IQR)) | 0.80 (0.73, 0.84) |
| Quintile of Neighborhood Education (%) | |
| Q1 (lowest) | 13 (11.8) |
| Q2 | 19 (17.3) |
| Q3 | 18 (16.4) |
| Q4 | 42 (38.2) |
| Q5 (highest) | 18 (16.4) |
| Comorbidity | |
| Charlson Comorbidity Index (%) | |
| 0 | 82 (74.5) |
| 1 | 16 (14.5) |
| ≥2 | 12 (10.9) |
| Cardiovascular Disease (%) | 11 (10.0) |
| Diabetes (%) | 11 (10.0) |
| Metastatic Sites | |
| Number of Metastatic Sites at Diagnosis | |
| 1 | 46 (41.8) |
| 2 | 28 (25.5) |
| 3 | 12 (10.9) |
| ≥4 | 24 (21.8) |
| Sites of Metastasis at Diagnosis 1 | |
| Pulmonary/Pleura | 59 (53.6) |
| Lymph Nodes | 46 (41.8) |
| Brain | 31 (28.2) |
| Hepatic | 27 (24.5) |
| Osseous | 23 (20.9) |
| Variable | Mutant (n = 22) | Wild Type (n = 32) | p-Value | SMD |
|---|---|---|---|---|
| Age, years (mean [SD]) | 61.88 (13.34) | 69.34 (13.20) | 0.063 | 0.562 |
| Male (%) | <10 1 | 21 (65.6) | - | - |
| Neighborhood Household Income (mean [SD]) | 39,155.33 (12,149.72) | 40,333.23 (16,408.30) | 0.776 | 0.082 |
| Proportion who achieved a Highschool Education or Greater (mean [SD]) | 0.76 (0.11) | 0.76 (0.10) | 0.842 | 0.055 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Sullivan, D.E.; Boyne, D.J.; Gogna, P.; Brenner, D.R.; Cheung, W.Y. Understanding Real-World Treatment Patterns and Clinical Outcomes among Metastatic Melanoma Patients in Alberta, Canada. Curr. Oncol. 2023, 30, 4166-4176. https://doi.org/10.3390/curroncol30040317
O’Sullivan DE, Boyne DJ, Gogna P, Brenner DR, Cheung WY. Understanding Real-World Treatment Patterns and Clinical Outcomes among Metastatic Melanoma Patients in Alberta, Canada. Current Oncology. 2023; 30(4):4166-4176. https://doi.org/10.3390/curroncol30040317
Chicago/Turabian StyleO’Sullivan, Dylan E., Devon J. Boyne, Priyanka Gogna, Darren R. Brenner, and Winson Y. Cheung. 2023. "Understanding Real-World Treatment Patterns and Clinical Outcomes among Metastatic Melanoma Patients in Alberta, Canada" Current Oncology 30, no. 4: 4166-4176. https://doi.org/10.3390/curroncol30040317