Active Pharmacovigilance Study: A Follow-Up Model of Oral Anti-Cancer Drugs under Additional Monitoring

 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
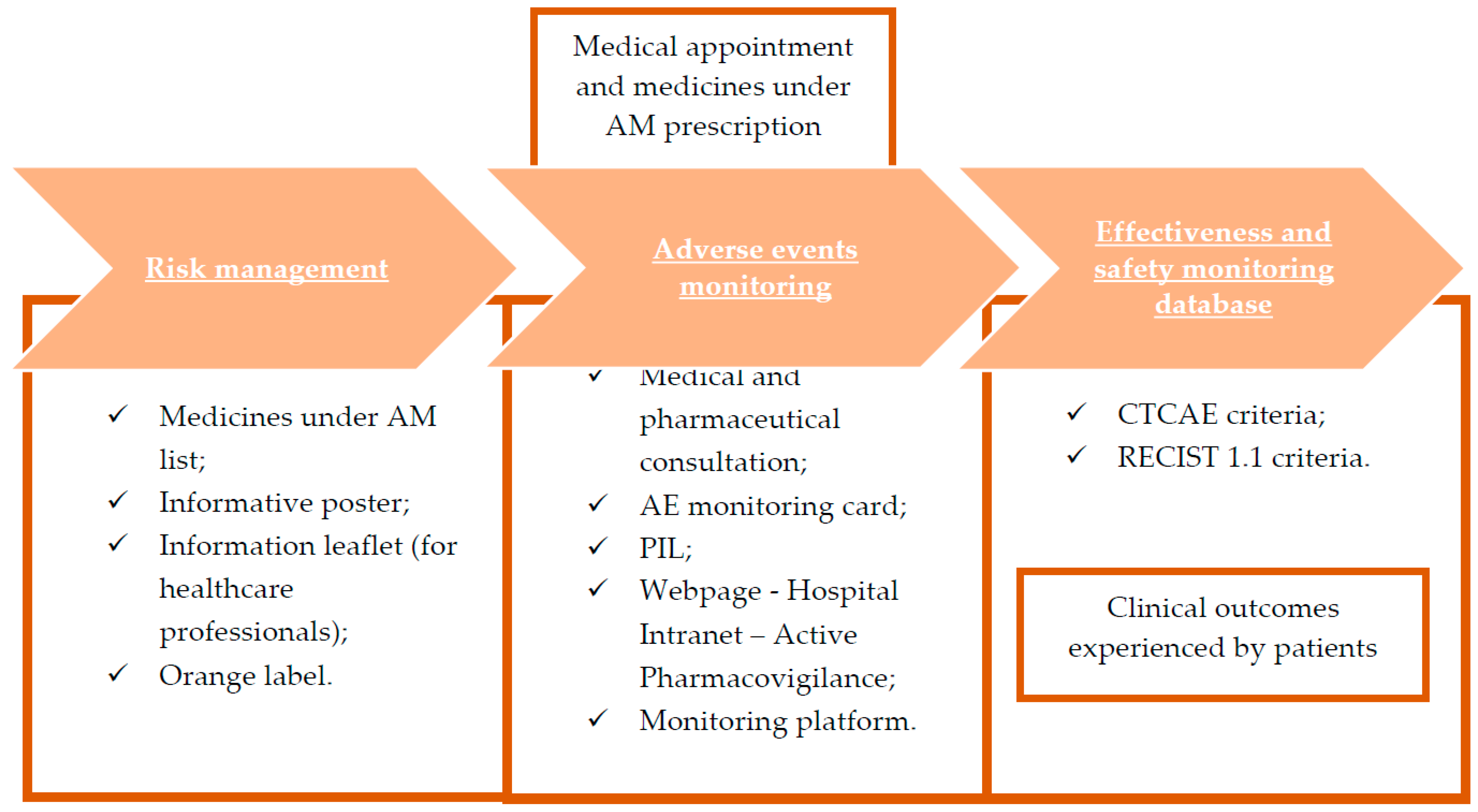
2.1. Study Design
2.2. Risk Minimization Measures
2.3. Adverse Events Monitoring
2.4. Effectiveness and Safety Monitoring Database
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Strengthening Pharmacovigilance to Reduce Adverse Effects of Medicines. 2008. Available online: https://ec.europa.eu/commission/presscorner/detail/en/MEMO_08_782 (accessed on 2 February 2023).
- Bouvy, J.C.; De Bruin, M.L.; Koopmanschap, M.A. Epidemiology of adverse drug reactions in Europe: A review of recent observational studies. Drug Saf. 2015, 38, 437–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, K.J.; Kedia, M.S.; Bajpai, D.; Mehta, S.S.; Kshirsagar, N.A.; Gogtay, N.J. Evaluation of the prevalence and economic burden of adverse drug reactions presenting to the medical emergency department of a tertiary referral centre: A prospective study. BMC Clin. Pharmacol. 2007, 7, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adedapo, A.D.A.; Adedeji, W.A.; Adedapo, I.A.; Adedapo, K.S. Cohort study on adverse drug reactions in adults admitted to the medical wards of a tertiary hospital in Nigeria: Prevalence, incidence, risk factors and fatality. Br. J. Clin. Pharmacol. 2021, 87, 1878–1889. [Google Scholar] [CrossRef] [PubMed]
- Formica, D.; Sultana, J.; Cutroneo, P.M.; Lucchesi, S.; Angelica, R.; Crisafulli, S.; Ingrasciotta, Y.; Salvo, F.; Spina, E.; Trifirò, G. The economic burden of preventable adverse drug reactions: A systematic review of observational studies. Expert Opin. Drug Saf. 2018, 17, 681–695. [Google Scholar] [CrossRef]
- Singh, S.; Dhasmana, D.C.; Bisht, M.; Singh, P.K. Pattern of Adverse Drug Reactions to Anticancer Drugs: A Quantitative and Qualitative Analysis. Indian J. Med. Paediatr. Oncol. 2017, 38, 140–145. [Google Scholar]
- Guo, H.J.; Ren, F.; Zhang, D.; Ji, M. Monitoring report on 341 cases of adverse reactions caused by antitumor drugs. Afr. J. Microbiol. Res. 2012, 6, 3774–3777. [Google Scholar]
- Vijayalakshmi, M.K.; Palatty, P.L.; Bhat, P.; Dinesh, M. A comparative assessment of the ADR profile in various anti-cancer regimens excluding gastro-intestinal and haematological toxicity at a tertiary care centre. J. Clin. Diagn. Res. 2011, 5, 1209–1213. [Google Scholar]
- Baldo, P.; Fornasier, G.; Ciolfi, L.; Sartor, I.; Francescon, S. Pharmacovigilance in oncology. Int. J. Clin. Pharm. 2018, 40, 832–841. [Google Scholar] [CrossRef] [Green Version]
- Legal Framework: Pharmacovigilance. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/pharmacovigilance/legal-framework-pharmacovigilance (accessed on 2 February 2023).
- Medicines under Additional Monitoring. Available online: https://www.ema.europa.eu/en/human-regulatory/post-authorisation/pharmacovigilance/medicines-under-additional-monitoring (accessed on 2 February 2023).
- Guideline on Good Pharmacovigilance Practices Module X—Additional Monitoring. 2013. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-good-pharmacovigilance-practices-module-x-additional-monitoring_en.pdf (accessed on 2 February 2023).
- Regulation (EC) No 726/2004 of the European Parliament and of the Council of 31 March 2004 laying down Community Procedures for the Authorisation and Supervision of Medicinal Products for Human and Veterinary Use and Establishing a European Medicines Agency. Official Journal of the European Union, L–136, pp. 1–33. 2004. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2004:136:0001:0033:en:PDF (accessed on 3 February 2023).
- Lively, A.; Minard, L.V.; Scott, S.; Deal, H.; Lambourne, T.; Giffin, J. Exploring the perspectives of healthcare professionals in delivering optimal oncology medication education. PLoS ONE 2020, 15, e0228571. [Google Scholar] [CrossRef] [Green Version]
- Reumerman, M.; Tichelaar, J.; Piersma, B.; Richir, M.C.; van Agtmael, M.A. Urgent need to modernize pharmacovigilance education in healthcare curricula: Review of the literature. Eur. J. Clin. Pharmacol. 2018, 74, 1235–1248. [Google Scholar] [CrossRef] [Green Version]
- Guideline on Good Pharmacovigilance Practices (GVP). Module XVI—Risk Minimisation Measures: Selection of Tools and Effectiveness Indicators (Rev 2). European Medicines Agency. 2017. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-good-pharmacovigilance-practices-module-xvi-risk-minimisation-measures-selection-tools_en-3.pdf (accessed on 3 February 2023).
- Guideline on Good Pharmacovigilance Practices (GVP). Module V—Risk Management Systems (Rev 2). European Medicines Agency. 2017. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-good-pharmacovigilance-practices-module-v-risk-management-systems-rev-2_en.pdf (accessed on 3 February 2023).
- Guideline on Good Pharmacovigilance Practices (GVP): Module VI—Collection, Management and Submission of Reports of Suspected Adverse Reactions to Medicinal Products (Rev 2). European Medicines Agency. 2017. Available online: https://www.ema.europa.eu/en/documents/regulatory-procedural-guideline/guideline-good-pharmacovigilance-practices-gvp-module-vi-collection-management-submission-reports_en.pdf (accessed on 25 March 2023).
- Pan American Health Organization. Good Pharmacovigilance Practices for the Americas. PANDRH Technical Document Nº 5 Washington D.C. 2011. Available online: https://www.paho.org/hq/dmdocuments/2011/Series-Red-PARF---5-Eng.pdf (accessed on 25 March 2023).
- Common Terminology Criteria for Adverse Events (CTCAE). Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm (accessed on 3 February 2023).
- RECIST 1.1 Guidelines. Available online: https://recist.eortc.org/recist-1-1-2/ (accessed on 3 February 2023).
- Peters, S.; Camidge, D.R.; Shaw, A.T.; Gadgeel, S.; Ahn, J.S.; Kim, D.W.; Ou, S.I.; Pérol, M.; Dziadziuszko, R.; Rosell, R.; et al. Alectinib versus Crizotinib in Untreated ALK-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 829–838. [Google Scholar] [CrossRef]
- Mayer, R.J.; Van Cutsem, E.; Falcone, A.; Yoshino, T.; Garcia-Carbonero, R.; Mizunuma, N.; Yamazaki, K.; Shimada, Y.; Tabernero, J.; Komatsu, Y.; et al. Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N. Engl. J. Med. 2015, 372, 1909–1919. [Google Scholar] [CrossRef] [Green Version]
- Bahri, P.; Pariente, A. Systematising Pharmacovigilance Engagement of Patients, Healthcare Professionals and Regulators: A Practical Decision Guide Derived from the International Risk Governance Framework for Engagement Events and Discourse. Drug Saf. 2021, 44, 1193–1208. [Google Scholar] [CrossRef]
- O’Callaghan, J.; Griffin, B.T.; Morris, J.M.; Bermingham, M. Knowledge of adverse drug reaction reporting and the Pharmacovigilance of biological medicines: A survey of healthcare professionals in Ireland. BioDrugs 2018, 32, 267–280. [Google Scholar] [CrossRef] [Green Version]
- Summary of Product Characteristics LONSURF®. 2016. Available online: https://www.ema.europa.eu/en/documents/product-information/lonsurf-epar-product-information_en.pdf (accessed on 4 February 2023).
- Summary of Product Characteristics NINLARO®. 2016. Available online: https://www.ema.europa.eu/en/documents/product-information/ninlaro-epar-product-information_en.pdf (accessed on 4 February 2023).
- Summary of Product Characteristics REVLIMID®. 2007. Available online: https://www.ema.europa.eu/en/documents/product-information/revlimid-epar-product-information_en.pdf (accessed on 4 February 2023).
- Summary of Product Characteristics CABOMETYX®. 2016. Available online: https://www.ema.europa.eu/en/documents/product-information/cabometyx-epar-product-information_en.pdf (accessed on 4 February 2023).
- Summary of Product Characteristics CAPRELSA®. 2012. Available online: https://www.ema.europa.eu/en/documents/product-information/caprelsa-epar-product-information_en.pdf (accessed on 4 February 2023).
- Summary of Product Characteristics IBRANCE®. 2016. Available online: https://www.ema.europa.eu/en/documents/product-information/ibrance-epar-product-information_en.pdf (accessed on 4 February 2023).
- Summary of Product Characteristics KISQALI®. 2017. Available online: https://www.ema.europa.eu/en/documents/product-information/kisqali-epar-product-information_en.pdf (accessed on 4 February 2023).
- Braal, C.L.; Jongbloed, E.M.; Wilting, S.M.; Mathijssen, R.H.J.; Koolen, S.L.W.; Jager, A. Inhibiting CDK4/6 in Breast Cancer with Palbociclib, Ribociclib, and Abemaciclib: Similarities and Differences. Drugs 2021, 81, 317–331. [Google Scholar] [CrossRef]
- Masuda, N.; Ohe, Y.; Gemma, A.; Kusumoto, M.; Yamada, I.; Ishii, T.; Yamamoto, N. Safety and effectiveness of alectinib in a real-world surveillance study in patients with ALK-positive non-small-cell lung cancer in Japan. Cancer Sci. 2019, 110, 1401–1407. [Google Scholar] [CrossRef] [Green Version]
- Summary of Product Characteristics ALESCENSA®. 2017. Available online: https://www.ema.europa.eu/en/documents/product-information/alecensa-epar-product-information_en.pdf (accessed on 4 February 2023).
- Camidge, D.R.; Dziadziuszko, R.; Peters, S.; Mok, T.; Noe, J.; Nowicka, M.; Gadgeel, S.M.; Cheema, P.; Pavlakis, N.; de Marinis, F.; et al. Updated efficacy and safety data and impact of the EML4-ALK fusion variant on the efficacy of alectinib in untreated ALK-Positive advanced non-small cell lung cancer in the global phase III ALEX study. J. Thorac. Oncol. 2019, 14, 1233–1243. [Google Scholar] [CrossRef]
- Makimoto, G.; Kawakado, K.; Nakanishi, M.; Tamura, T.; Kuyama, S. Successful Treatment with Lorlatinib after the Development of Alectinib-Induced Liver Damage in ALK-Positive Non-Small-Cell Lung Cancer: A Case Report. Case Rep. Oncol. 2021, 14, 197–201. [Google Scholar] [CrossRef]
- Anderson, S.; Kiernan, M.; Ho, P.J. Lenalidomide-related progressive multifocal leukoencephalopathy: A Case Report and review of drug-related cases in multiple myeloma. Clin. Lymphoma Myeloma Leuk. 2019, 19, e169–e171. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Halabi, S.; Sanford, B.L.; Hahn, O.; Michaelson, M.D.; Walsh, M.K.; Feldman, D.R.; Olencki, T.; Picus, J.; Small, E.J.; et al. Cabozantinib Versus Sunitinib as Initial Targeted Therapy for Patients With Metastatic Renal Cell Carcinoma of Poor or Intermediate Risk: The Alliance A031203 CABOSUN Trial. J. Clin. Oncol. 2017, 35, 591–597. [Google Scholar] [CrossRef]
- Brigo, F.; Pagani, E.; Tezzon, F.; Masi, E.; Nardone, R. Lenalidomide-associated progressive multifocal leukoencephalopathy. Leuk. Lymphoma 2017, 58, 2514–2515. [Google Scholar] [CrossRef]
- Ruiz-Heredia, Y.; Sanchez-Vega, B.; Barrio, S.; Linares, M.; Rapado, I.; Braggio, E.; Stewart, K.; Folgueira, M.D.; Ramos, A.; Collado, L.; et al. Concurrent progressive multifocal leukoencephalopathy and central nervous system infiltration by multiple myeloma: A case report. J. Oncol. Pharm. Pract. 2019, 25, 998–1002. [Google Scholar] [CrossRef] [PubMed]
- Bauer, T.M.; Felip, E.; Solomon, B.J.; Thurm, H.; Peltz, G.; Chioda, M.D.; Shaw, A.T. Clinical Management of Adverse Events Associated with Lorlatinib. Oncologist 2019, 24, 1103–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, V.W.; Lin, Y.T.; Kim, D.W.; Loong, H.H.; Nagasaka, M.; To, H.; Ang, Y.L.; Ock, C.Y.; Tchekmedyian, N.; Ou, S.I.; et al. An International Real-World Analysis of the Efficacy and Safety of Lorlatinib Through Early or Expanded Access Programs in Patients With Tyrosine Kinase Inhibitor-Refractory ALK-Positive or ROS1-Positive NSCLC. J. Thorac. Oncol. 2020, 15, 1484–1496. [Google Scholar] [CrossRef] [PubMed]
- Summary of Product Characteristics LORVIQUA®. 2019. Available online: https://www.ema.europa.eu/en/documents/product-information/lorviqua-epar-product-information_en.pdf (accessed on 4 February 2023).


{kind=link}
| Medicines under AM | Base Pathology | Number of Patients |
|---|---|---|
| Alectinib | Lung adenocarcinoma | 4 |
| Lung squamous cell carcinoma | 2 | |
| Cabozantinib | Hepatocellular carcinoma | 1 |
| Entrectinib | Lung adenocarcinoma | 1 |
| Ixazomib | Multiple myeloma | 3 |
| Lenalidomide | Multiple myeloma | 5 |
| Lorlatinib | Lung adenocarcinoma | 2 |
| Niraparib | High-grade serous ovarian carcinoma | 2 |
| Osimertinib | Lung adenocarcinoma | 7 |
| Palbociclib | Breast cancer | 3 |
| Ribociclib | Breast cancer | 4 |
| Trametinib + Dabrafenib | Lung adenocarcinoma | 1 |
| Vandetanib | Medullary thyroid carcinoma | 1 |
| Venetoclax | Chronic lymphocytic leukemia | 7 |
| Trifluridine + Tipiracil | Colon adenocarcinoma | 5 |
| Rectal adenocarninoma | 2 | |
| Gastric adenocarcinoma | 2 | |
| N Total | 52 |
| Number of Patients | Gender | ||
|---|---|---|---|
| Medicines under AM | F | M | N Total |
| Alectinib | 3 | 3 | 6 |
| Cabozantinib | 1 | 1 | |
| Entrectinib | 1 | 1 | |
| Ixazomib | 2 | 1 | 3 |
| Lenalidomide | 4 | 1 | 5 |
| Lorlatinib | 2 | 2 | |
| Niraparib | 2 | 2 | |
| Osimertinib | 5 | 2 | 7 |
| Palbociclib | 3 | 3 | |
| Ribociclib | 4 | 4 | |
| Trametinib + Dabrafenib | 1 | 1 | |
| Vandetanib | 1 | 1 | |
| Venetoclax | 3 | 4 | 7 |
| Trifluridine + Tipiracil | 2 | 7 | 9 |
| N total | 31 | 21 | 52 |
| Number of Patients | Gender | ||
|---|---|---|---|
| Age Group (Years) | F | M | N Total |
| 40–50 | 2 | 2 | |
| 50–60 | 9 | 3 | 12 |
| 60–70 | 9 | 6 | 15 |
| 70–80 | 8 | 7 | 15 |
| 80–90 | 3 | 5 | 8 |
| N total | 31 | 21 | 52 |
| Medicines under AM | Type of the 1st Suspected Toxicity | Grade of the 1st Suspected Toxicity | Type of the 2nd Suspected Toxicity | Grade of the 2nd Suspected Toxicity | Number of Patients |
|---|---|---|---|---|---|
| Alectinib | Gastrointestinal disorders | 2 | 1 | ||
| Liver disorders | 2 | 1 | |||
| Lung disorders | 2 | 1 | |||
| Kidney disorders | 2 | Liver disorders | 3 | 1 | |
| Cabozantinib | Mucositis | 3 | Hypertension | 4 | 1 |
| Entrectinib | Hypotension | 2 | Vomiting | 2 | 1 |
| Ixazomib | Hematological disorders | 3 | 1 | ||
| Lenalidomide | Anorexia | 2 | 1 | ||
| Hematological disorders | 1 | 1 | |||
| Neurological disorders | 2 | 1 | |||
| Lorlatinib | Dyslipidemia | 2 | 1 | ||
| Osimertinib | Mucositis | 3 | 1 | ||
| Paronychia | 2 | 1 | |||
| 3 | 1 | ||||
| Palbociclib | Hematological disorders | 2 | 2 | ||
| 3 | 1 | ||||
| Ribociclib | Hematological disorders | 3 | 3 | ||
| Trametinib + Dabrafenib | Fever | 1 | 1 | ||
| Vandetanib | QT prolongation | 1 | Skin disorders | 2 | 1 |
| Venetoclax | Hematological disorders | 1 | 1 | ||
| Trifluridine + tipiracil | Gastrointestinal disorders | 3 | 1 | ||
| Hematological disorders | 1 | 1 | |||
| 2 | 3 | ||||
| Proteinuria | 2 | 1 | |||
| N total | 29 |
| Causes of Drug Discontinuation | Medicines under AM | Number of Patients |
|---|---|---|
| Complete therapeutic scheme | Ixazomib | 1 |
| Lenalidomide | 2 | |
| Hyperbilirubinemia | Lorlatinib | 1 |
| Disease progression | Trifluridine + tipiracil | 5 |
| Alectinib | 3 | |
| Entrectinib | 1 | |
| Osimertinib | 4 | |
| Trifluridine + tipiracil | 2 | |
| Trifluridine + tipiracil | 2 | |
| Palbociclib | 1 | |
| Ribociclib | 1 | |
| Alectinib | 1 | |
| Niraparib | 1 | |
| Cabozantinib | 1 | |
| Ixazomib | 2 | |
| Lenalidomide | 2 | |
| Toxicity | Alectinib | 1 |
| Vandetanib | 1 | |
| Lenalidomide | 1 | |
| N total | 33 |
| DP | Type of Response | 3 M Evaluation Number of Patients | 12 M Evaluation Number of Patients |
|---|---|---|---|
| No DP | CR | 3 (7.9%) | 4 (25.0%) |
| PR | 19 (50.0%) | 3 (18.8%) | |
| SD | 12 (31.6%) | 2 (12.5%) | |
| DP | 4 (10.5%) | 7 (43.75%) | |
| N total | 38 | 16 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carvalho da Silva, S.P.; Jesus, M.; Roque, F.; Herdeiro, M.T.; Costa e Sousa, R.; Duarte, A.P.; Morgado, M. Active Pharmacovigilance Study: A Follow-Up Model of Oral Anti-Cancer Drugs under Additional Monitoring. Curr. Oncol. 2023, 30, 4139-4152. https://doi.org/10.3390/curroncol30040315
Carvalho da Silva SP, Jesus M, Roque F, Herdeiro MT, Costa e Sousa R, Duarte AP, Morgado M. Active Pharmacovigilance Study: A Follow-Up Model of Oral Anti-Cancer Drugs under Additional Monitoring. Current Oncology. 2023; 30(4):4139-4152. https://doi.org/10.3390/curroncol30040315
Chicago/Turabian StyleCarvalho da Silva, Sofia Pinto, Mafalda Jesus, Fátima Roque, Maria Teresa Herdeiro, Rita Costa e Sousa, Ana Paula Duarte, and Manuel Morgado. 2023. "Active Pharmacovigilance Study: A Follow-Up Model of Oral Anti-Cancer Drugs under Additional Monitoring" Current Oncology 30, no. 4: 4139-4152. https://doi.org/10.3390/curroncol30040315