Nuclear and Cytoplasmic hTERT, Tumor-Infiltrating Lymphocytes, and Telomere Elongation Leukocytes Are Independent Factors in the Response to Neoadjuvant Treatment in HER2-Enriched Breast Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Tumor Infiltrating Lymphocytes (TILs) Determination
2.3. hTERT Immunohistochemistry
2.4. Qualitative Evaluation of hTR/hTERT and Splice Variants in Breast Cancer Tissues and Leukocytes plus Investigation of Mutations in the hTERT Promoter Region
2.5. Leukocytes Telomere Length (LTL)
2.6. Statistical Analysis
3. Results
3.1. Clinical Data, pCR, and TILs
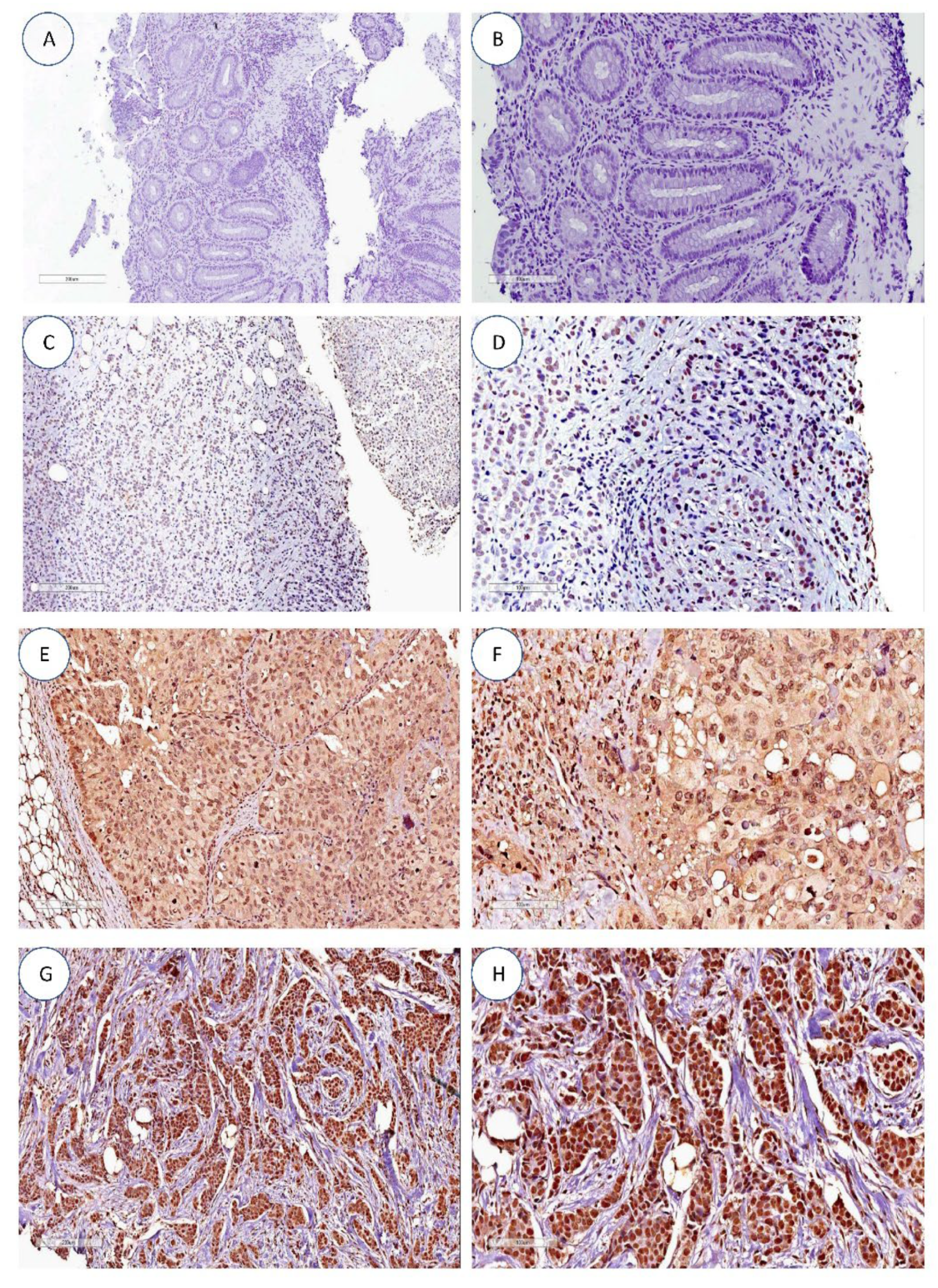
3.2. hTERT Expression by Immunochemistry
3.3. hTERT Expression by Immunochemistry and Correlation between the Clinical Variables
3.4. hTR/hTERT Transcripts Qualitative and hTERT Promoter Region Evaluation
3.5. Leukocyte Telomere Length
3.6. Leukocyte Telomere Length in HER2-E Breast Cancer and Correlation with Other Variables
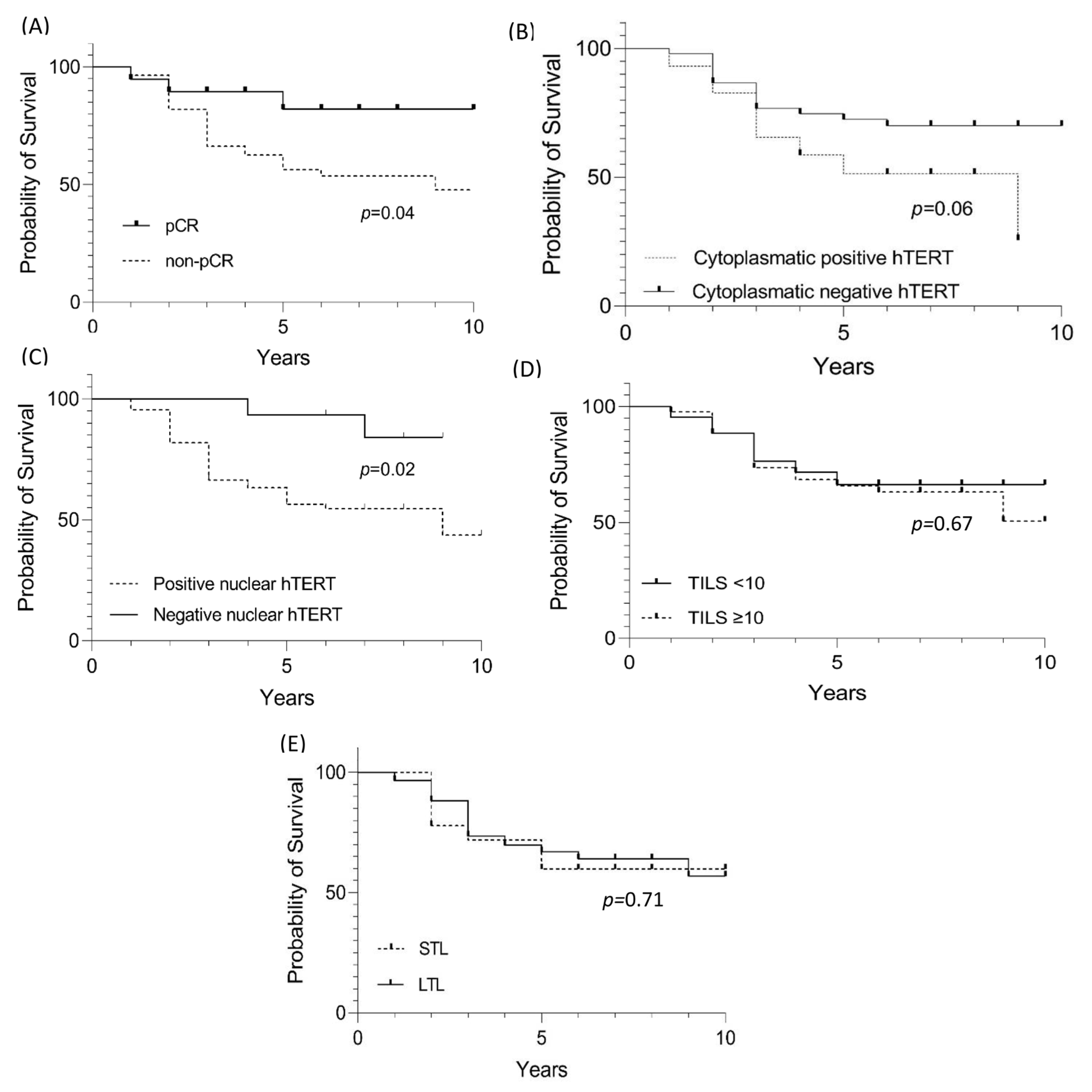
3.7. Survival Progression-Free Survival Assessment of HER2-E Cases
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schettini, F.; Buono, G.; Cardalesi, C.; Desideri, I.; De Placido, S.; Del Mastro, L. Hormone Receptor/Human Epidermal Growth Factor Receptor 2-positive breast cancer: Where we are now and where we are going. Cancer Treat. Rev. 2016, 46, 20–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swain, S.M.; Tang, G.; Lucas, P.C.; Robidoux, A.; Goerlitz, D.; Harris, B.T.; Bandos, H.; Geyer, C.E., Jr.; Rastogi, P.; Mamounas, E.P.; et al. Pathologic complete response and outcomes by intrinsic subtypes in NSABP B-41, a randomized neoadjuvant trial of chemotherapy with trastuzumab, lapatinib, or the combination. Breast Cancer Res. Treat. 2019, 178, 389–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gobbini, E.; Ezzalfani, M.; Dieras, V.; Bachelot, T.; Brain, E.; Debled, M.; Jacot, W.; Mouret-Reynier, M.A.; Goncalves, A.; Dalenc, F.; et al. Time trends of overall survival among metastatic breast cancer patients in the real-life ESME cohort. Eur. J. Cancer. 2018, 96, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Ruffell, B.; Au, A.; Rugo, H.S.; Esserman, L.J.; Hwang, E.S.; Coussens, L.M. Leukocyte composition of human breast cancer. Proc. Natl. Acad. Sci. USA 2012, 109, 2796–2801. [Google Scholar] [CrossRef] [Green Version]
- Loi, S.; Sirtaine, N.; Piette, F.; Salgado, R.; Viale, G.; Van Eenoo, F.; Rouas, G.; Francis, P.; Crown, J.P.; Hitre, E.; et al. Prognostic and predictive value of tumor-infiltrating lymphocytes in a phase III randomized adjuvant breast cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin with doxorubicin-based chemotherapy: BIG 02-98. J. Clin. Oncol. 2013, 31, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Hiam-Galvez, K.J.; Allen, B.M.; Spitzer, M.H. Systemic immunity in cancer. Nat. Rev. Cancer 2021, 21, 345–359. [Google Scholar] [CrossRef]
- Demaria, S.; Volm, M.D.; Shapiro, R.L.; Yee, H.T.; Oratz, R.; Formenti, S.C.; Muggia, F.; Symmans, W.F. Development of tumor-infiltrating lymphocytes in breast cancer after neoadjuvant paclitaxel chemotherapy. Clin. Cancer Res. 2001, 7, 3025–3030. [Google Scholar]
- Loi, S.; Michiels, S.; Salgado, R.; Sirtaine, N.; Jose, V.; Fumagalli, D.; Kellokumpu-Lehtinen, P.L.; Bono, P.; Kataja, V.; Desmedt, C.; et al. Tumor-infiltrating lymphocytes are prognostic in triple negative breast cancer and predictive for trastuzumab benefit in early breast cancer: Results from the FinHER trial. Ann. Oncol. 2014, 25, 1544–1550. [Google Scholar] [CrossRef]
- Denkert, C.; von Minckwitz, G.; Brase, J.C.; Sinn, B.V.; Gade, S.; Kronenwett, R.; Pfitzner, B.M.; Salat, C.; Loi, S.; Schmitt, W.D.; et al. Tumor-infiltrating lymphocytes and response to neoadjuvant chemotherapy with or without carboplatin in human epidermal growth factor receptor 2-positive and triple-negative primary breast cancers. J. Clin. Oncol. 2015, 33, 983–991. [Google Scholar] [CrossRef]
- Zhou, J.; Shen, X.; Huang, J.; Hodes, R.J.; Rosenberg, S.A.; Robbins, P.F. Telomere length of transferred lymphocytes correlates with in vivo persistence and tumor regression in melanoma patients receiving cell transfer therapy. J. Immunol. 2005, 175, 7046–7052. [Google Scholar] [CrossRef] [Green Version]
- Quintela-Fandino, M.; Soberon, N.; Lluch, A.; Manso, L.; Calvo, I.; Cortes, J.; Moreno-Antón, F.; Gil-Gil, M.; Martinez-Jánez, N.; Gonzalez-Martin, A.; et al. Critically short telomeres and toxicity of chemotherapy in early breast cancer. Oncotarget 2017, 28, 21472–21482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blackburn, E.H. Structure and function of telomeres. Nature 1991, 350, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Heaphy, C.M.; Subhawong, A.P.; Gross, A.L.; Konishi, Y.; Kouprina, N.; Argani, P.; Visvanathan, K.; Meeker, A.K. Shorter telomeres in luminal B, HER-2 and triple-negative breast cancer subtypes. Mod. Pathol. 2011, 24, 194–200. [Google Scholar] [CrossRef] [Green Version]
- Robinson, N.J.; Schiemann, W.P. Telomerase in cancer: Function, regulation, and clinical translation. Cancers 2022, 14, 808. [Google Scholar] [CrossRef] [PubMed]
- Gay-Bellile, M.; Romero, P.; Cayre, A.; Véronèse, L.; Privat, M.; Singh, S.; Combes, P.; Kwiatkowski, F.; Abrial, C.; Bignon, Y.J.; et al. ERCC1 and telomere status in breast tumours treated with neoadjuvant chemotherapy and their association with patient prognosis. J. Pathol. Clin. Res. 2016, 2, 234–246. [Google Scholar] [CrossRef]
- Ceja-Rangel, H.A.; Sánchez-Suárez, P.; Castellanos-Juárez, E.; Peñaroja-Flores, R.; Arenas-Aranda, D.J.; Gariglio, P.; Benítez-Bribiesca, L. Shorter telomeres and high telomerase activity correlate with a highly aggressive phenotype in breast cancer cell lines. Tumour Biol. 2016, 37, 11917–11926. [Google Scholar] [CrossRef]
- Cong, Y.S.; Wen, J.; Bacchetti, S. The human telomerase catalytic subunit hTERT: Organization of the gene and characterization of the promoter. Hum. Mol. Genet. 1999, 8, 137–142. [Google Scholar] [CrossRef] [Green Version]
- Wick, M.; Zubov, D.; Hagen, G. Genomic organization and promoter characterization of the gene encoding the human telomerase reverse transcriptase (hTERT). Gene 1999, 17, 97–106. [Google Scholar] [CrossRef]
- Takakura, M.; Kyo, S.; Kanaya, T.; Hirano, H.; Takeda, J.; Yutsudo, M.; Inoue, M. Cloning of human telomerase catalytic subunit (hTERT) gene promoter and identification of proximal core promoter sequences essential for transcriptional activation in immortalized and cancer cells. Cancer Res. 1999, 1, 551–557. [Google Scholar]
- Zehir, A.; Benayed, R.; Shah, R.H.; Syed, A.; Middha, S.; Kim, H.R.; Srinivasan, P.; Gao, J.; Chakravarty, D.; Devlin, S.M.; et al. Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat. Med. 2017, 23, 703–713, Erratum in: Nat. Med. 2017, 23, 1004. [Google Scholar] [CrossRef]
- Piscuoglio, S.; Ng, C.K.; Murray, M.; Burke, K.A.; Edelweiss, M.; Geyer, F.C.; Macedo, G.S.; Inagaki, A.; Papanastasiou, A.D.; Martelotto, L.G.; et al. Massively parallel sequencing of phyllodes tumours of the breast reveals actionable mutations, and TERT promoter hotspot mutations and TERT gene amplification as likely drivers of progression. J. Pathol. 2016, 238, 508–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Silva, E.M.; Selenica, P.; Vahdatinia, M.; Pareja, F.; Da Cruz Paula, A.; Ferrando, L.; Gazzo, A.M.; Dopeso, H.; Ross, D.S.; Bakhteri, A.; et al. TERT promoter hotspot mutations and gene amplification in metaplastic breast cancer. NPJ Breast Cancer 2021, 7, 43. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, S.R.; Ellis, I.O.; Schnitt, S.J.; Tan, P.H.; van de Vijver, M.J. WHO Classification of Tumours of the Breast, 4th ed.; IARC Press: Lyon, France, 2012. [Google Scholar]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef]
- Ulaner, G.A.; Hu, J.F.; Vu, T.H.; Giudice, L.C.; Hoffman, A.R. Telomerase activity in human development is regulated by human telomerase reverse transcriptase (hTERT) transcription and by alternate splicing of hTERT transcripts. Cancer Res. 1998, 58, 4168–4172. [Google Scholar]
- Lincz, L.F.; Mudge, L.M.; Scorgie, F.E.; Sakoff, J.A.; Hamilton, C.S.; Seldon, M. Quantification of hTERT splice variants in melanoma by SYBR green real-time polymerase chain reaction indicates a negative regulatory role for the beta deletion variant. Neoplasia 2008, 10, 1131–1137. [Google Scholar] [CrossRef] [Green Version]
- Trung, N.T.; Hoan, N.X.; Trung, P.Q.; Binh, M.T.; Van Tong, H.; Toan, N.L.; Bang, M.H.; Song, L.H. Clinical significance of combined circulating TERT promoter mutations and miR-122 expression for screening HBV-related hepatocellular carcinoma. Sci Rep. 2020, 10, 8181. [Google Scholar] [CrossRef]
- Delmonico, L.; Costa, M.A.S.M.; Fournier, M.V.; Romano, S.O.; Nascimento, C.M.D.; Barbosa, A.S.; Moreira, A.D.S.; Scherrer, L.R.; Ornellas, M.H.F.; Alves, G. Mutation profiling in the PIK3CA, TP53, and CDKN2A genes in circulating free DNA and impalpable breast lesions. Ann. Diagn. Pathol. 2019, 39, 30–35. [Google Scholar] [CrossRef]
- Cawthon, R.M. Telomere measurement by quantitative PCR. Nucleic Acids Res. 2002, 30, e47. [Google Scholar] [CrossRef] [Green Version]
- Joglekar, M.V.; Satoor, S.N.; Wong, W.K.M.; Cheng, F.; Ma, R.C.W.; Hardikar, A.A. An Optimised Step-by-Step protocol for measuring relative telomere length. Methods Protoc. 2020, 3, 27. [Google Scholar] [CrossRef] [Green Version]
- Liu, K.; Schoonmaker, M.M.; Levine, B.L.; June, C.H.; Hodes, R.J.; Weng, N.P. Constitutive and regulated expression of telomerase reverse transcriptase (hTERT) in human lymphocytes. Proc. Natl. Acad. Sci. USA 1999, 96, 5147–5152. [Google Scholar] [CrossRef] [Green Version]
- Hamy, A.S.; Bonsang-Kitzis, H.; De Croze, D.; Laas, E.; Darrigues, L.; Topciu, L.; Menet, E.; Vincent-Salomon, A.; Lerebours, F.; Pierga, J.Y.; et al. Interaction between molecular subtypes and stromal immune infiltration before and after treatment in breast cancer patients treated with neoadjuvant chemotherapy. Clin. Cancer Res. 2019, 25, 6731–6741. [Google Scholar] [CrossRef] [Green Version]
- Denkert, C.; von Minckwitz, G.; Darb-Esfahani, S.; Lederer, B.; Heppner, B.I.; Weber, K.E.; Budczies, J.; Huober, J.; Klauschen, F.; Furlanetto, J.; et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: A pooled analysis of 3771, patients treated with neoadjuvant therapy. Lancet Oncol. 2018, 19, 40–50. [Google Scholar] [CrossRef]
- Belkacem, O.; Bacha, D.; Rahoui, N.; Zran, M.D.; Lahmar, A.; Slama, S.B. Prognostic value of tumor-infiltrating lymphocytes (TILS) and their association with clinicopathological features in breast cancer: A retrospective study involving 53 cases. Rev. Senol. Patol. Mamar. 2022, 35, 160–166. [Google Scholar] [CrossRef]
- Takada, K.; Kashiwagi, S.; Asano, Y.; Goto, W.; Morisaki, T.; Shibutani, M.; Tanaka, H.; Hirakawa, K.; Ohira, M. Differences in tumor-infiltrating lymphocyte density and prognostic factors for breast cancer by patient age. World J. Surg. Oncol. 2022, 17, 38. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: Meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 2018, 19, 27–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarotti, C.; Papassotiropoulos, B.; Elfgen, C.; Dedes, K.; Vorburger, D.; Pestalozzi, B.; Trojan, A.; Varga, Z. Biomarker dynamics and prognosis in breast cancer after neoadjuvant chemotherapy. Sci. Rep. 2022, 12, 91. [Google Scholar] [CrossRef]
- Shen, J.; Gammon, M.D.; Terry, M.B.; Bradshaw, P.T.; Wang, Q.; Teitelbaum, S.L.; Neugut, A.I.; Santella, R.M. Genetic polymorphisms in telomere pathway genes, telomere length, and breast cancer survival. Breast Cancer Res. Treat. 2012, 134, 393–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uno, Y.; Tanaka, H.; Miyakawa, K.; Akiyama, N.; Kamikokura, Y.; Yuzawa, S.; Kitada, M.; Takei, H.; Tanino, M. Subcellular localization of hTERT in breast cancer: Insights into its tumorigenesis and drug resistance mechanisms in HER2-immunopositive breast cancer. Hum. Pathol. 2023, 134, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Gomatou, G.; Masaoutis, C.; Vamvakaris, I.; Kotteas, E.; Bouros, E.; Tzilas, V.; Bouros, D. Differential immunohistochemical expression of hTERT in lung cancer patients with and without idiopathic pulmonary fibrosis. Pulmonology, 2022; ahead of print. [Google Scholar] [CrossRef]
- Nishi, Y.; Aoki, T.; Shimizu, T.; Sato, S.; Matsumoto, T.; Shiraki, T.; Sakuraoka, Y.; Mori, S.; Iso, Y.; Ishizuka, M.; et al. Significance of cytoplasmic expression of telomerase reverse transcriptase in patients with hepatocellular carcinoma undergoing liver resection. Mol. Clin. Oncol. 2021, 15, 244. [Google Scholar] [CrossRef]
- Shimoi, T.; Yoshida, M.; Kitamura, Y.; Yoshino, T.; Kawachi, A.; Shimomura, A.; Noguchi, E.; Yunokawa, M.; Yonemori, K.; Shimizu, C.; et al. TERT promoter hotspot mutations in breast cancer. Breast Cancer 2018, 25, 292–296. [Google Scholar] [CrossRef] [Green Version]
- Ennour-Idrissi, K.; Maunsell, E.; Diorio, C. Telomere length and breast cancer prognosis: A systematic review. Cancer Epidemiol. Biomark. Prev. 2017, 26, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Samavat, H.; Luu, H.N.; Beckman, K.B.; Jin, A.; Wang, R.; Koh, W.P.; Yuan, J.M. Leukocyte telomere length, cancer incidence and all-cause mortality among Chinese adults: Singapore Chinese Health Study. Int. J. Cancer 2021, 148, 352–362. [Google Scholar] [CrossRef]
- Arbeev, K.G.; Verhulst, S.; Steenstrup, T.; Kark, J.D.; Bagley, O.; Kooperberg, C.; Reiner, A.P.; Hwang, S.J.; Levy, D.; Fitzpatrick, A.L.; et al. Association of leukocyte telomere length with mortality among adult participants in 3 longitudinal studies. JAMA Netw. Open 2020, 3, e200023. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patients N = 103 (%) | |
|---|---|
| Characteristic | |
| Age, years | |
| Mean | 50.3 |
| SD | 10.1 |
| Cases ≤ 50 | 55 (53%) |
| Cases > 50 years | 48 (47%) |
| Race * | |
| Brazilian White | 34 (33%) |
| Brazilian Black/Brown * | 53 (51%) |
| NI | 16 (16%) |
| Menarche | |
| <12 | 22 (21%) |
| ≥12 | 65 (63%) |
| NI | 16 (16%) |
| Alcoholism Intake * | |
| Yes | 9 (9%) |
| No | 78 (76%) |
| NI | 16 (15%) |
| Tobacco use * | |
| Yes | 17 (17%) |
| No | 60 (58%) |
| Ex-tagagist | 10 (10%) |
| NI | 16 (15%) |
| Familial history | |
| Yes ** | 33 (32%) |
| Second Cancer | 2 (2%) |
| No | 52 (50%) |
| NI | 16 (15%) |
| Histopathologic Classification | |
| ILC | 1 (1%) |
| IDC | 102 (99%) |
| Stage Classification | |
| IIB | 25 (24%) |
| IIIA | 38 (37%) |
| IIIB | 36 (35%) |
| IIIC | 4 (4%) |
| Pathologic complete response | |
| Yes | 19 (18%) |
| No | 84 (82%) |
| TILs | |
| <10 | 43 (42%) |
| ≥10 | 44 (43%) |
| NI | 16 (15%) |
| Nuclear hTERT | Patients (N = 103) |
|---|---|
| Yes | 65 (63%) |
| No | 16 (16%) |
| NI | 22 (21%) |
| Citoplasmatic hTERT | |
| 0, 1 | 53 (52%) |
| 2, 3 | 28 (27%) |
| NI | 22 (21%) |
| Nuclear and Cytoplasmatic hTERT | |||||
|---|---|---|---|---|---|
| Patients (N = 81) (%) | pCR N = 15 (%) | Relapse (N = 14) (%) | TILs < 10 (N = 7) (%) | TILs ≥ 10 (N = 7) (%) | |
| Nucleus and cytoplasm | 39 (48%) | 5 (33%) | 5 (36%) | 3 (43%) | 2 (27%) |
| Nucleus | 26 (32%) | 3 (20%) | 5 (36%) | 3 (43%) | 2 (27%) |
| Cytoplasm | 5 (6%) | 0 | 0 | 0 | 0 |
| No expression | 11 (13%) | 7 (47%) | 4 (28%) | 1 (14%) | 3 (43%) |
| Total | 81 | 15 | 14 | 7 | 7 |
| Nuclear hTERT | Age | p-Value | ||
| <50 (N = 51) | ≥50 (N = 52) | |||
| Negative (N = 16) | 10 (20%) | 6 (12%) | 0.27 | |
| Positive (N = 65) | 30 (59%) | 35 (67%) | ||
| NA (N = 22) | 11 (21%) | 11 (21%) | ||
| Total | 51 | 52 | ||
| Cytoplasmatic hTERT | Age | p-value | ||
| <50 (N = 50) | ≥50 (N = 53) | |||
| Grade 0, 1 (N = 53) | 24 (48%) | 29 (55%) | 0.49 | |
| Grade 2, 3 (N = 28) | 15 (30%) | 13 (24%) | ||
| NA (N = 22) | 11 (22%) | 11 (21%) | ||
| Total | 50 | 53 | ||
| pCR | Age | p-value | ||
| <50 (N = 50) | ≥50 (N = 53) | |||
| pCR (N = 19) | 7 (14%) | 12 (23%) | 0.31 | |
| nonpCR (N = 84) | 43 (86%) | 41 (77%) | ||
| Total | 50 | 53 | ||
| TILs | Age | p-value | ||
| <50 (N = 59) | ≥50 (N = 54) | |||
| <10 (N = 43) | 26 (44%) | 17 (31%) | 0.31 | |
| ≥10 (N = 44) | 15 (25%) | 29 (54%) | ||
| NA (N = 16) | 8 (31%) | 8 (15%) | ||
| Total | 49 | 54 | ||
| Nuclear hTERT | pCR | p-value | ||
| pCR (N = 19) | nonPCR (N = 84) | |||
| Negative | 7 (37%) | 9 (11%) | 0.008 | |
| Positive | 8 (42%) | 57 (68%) | ||
| NA | 4 (21%) | 18 (21%) | ||
| Total | 19 | 84 | ||
| Cytoplasmatic hTERT | pCR | p-value | ||
| pCR (N = 19) | nonPCR (N = 84) | |||
| Grade 0, 1 (N = 53) | 13 (68%) | 40 (48%) | 0.07 | |
| Grade 2, 3 (N = 28) | 2 (10%) | 26 (31%) | ||
| NA (N = 22) | 4 (22%) | 18 (21%) | ||
| Total | 19 | 84 | ||
| TILs | pCR | p-value | ||
| pCR (N = 19) | nonPCR (N = 84) | |||
| <10 (N = 43) | 7 (37%) | 36 (43%) | 0.59 | |
| ≥10 (N = 44) | 10 (53%) | 34 (40%) | ||
| NA (N = 16) | 2 (10%) | 14 (17%) | ||
| Total | 19 | 84 | ||
| TILs | Nuclear hTERT | NA (N = 22) | p-value | |
| Negative (N = 16) | Positive (N = 65) | |||
| <10 (N = 36) | 8 (50%) | 28 (43%) | 7 (32%) | 0.76 |
| ≥10 (N = 34) | 6 (37%) | 28 (43%) | 10 (45%) | |
| NA (N = 11) | 2 (13%) | 9 (14%) | 5 (23%) | |
| Total | 16 | 65 | 22 | |
| TILs | Cytoplasmatic hTERT | NA (N = 22) | p-value | |
| Grade 0, 1 (N = 53) | Grade 2, 3 (N = 28) | |||
| <10 | 21 (40%) | 14 (50%) | 7 (32%) | 0.45 |
| ≥10 | 25 (47%) | 10 (36%) | 10 (45%) | |
| NA | 7 (13%) | 4 (14%) | 5 (23%) | |
| Total | 53 | 28 | 22 | |
| TL (HER2-E) (N = 103) | Age | p-Value | ||
| <50 (N = 47) | ≥50 (N = 56) | |||
| LT (N = 84) | 37 (79%) | 47 (84%) | 0.61 | |
| ST (N = 19) | 10 (21%) | 9 (16%) | ||
| Total | 47 | 56 | ||
| TL (HR+) (N = 35) | Age | p-value | ||
| <50 (N = 29) | ≥50 (N = 6) | |||
| LT (N = 25) | 21 (72%) | 4 (66%) | >0.99 | |
| ST (N = 10) | 8 (28%) | 2 (34%) | ||
| Total | 29 | 6 | ||
| TL (Controls) (N = 89) | Age | p-value | ||
| <50 (N = 36) | ≥50 (N = 53) | |||
| LT (N = 33) | 20 (55%) | 13 (25%) | 0.003 | |
| ST (N = 56) | 16 (45%) | 40 (75%) | ||
| Total | 36 | 53 | ||
| TL | Nuclear hTERT | p-value | ||
| Negative (N = 16) | Positive (N = 65) | NA (N = 22) | ||
| LT (n = 84) | 15 (94%) | 50 (77%) | 19 (86%) | >0.99 |
| ST (n = 19) | 1 (6%) | 15 (23%) | 3 (14%) | |
| Total | 16 | 65 | 22 | |
| TL | Cytoplasmatic hTERT | p-value | ||
| Grade 0, 1 (N = 53) | Grade 2, 3 (N = 28) | NA (N = 22) | ||
| LT (n = 84) | 42 (79%) | 23 (82%) | 19 (86%) | >0.99 |
| ST (n = 19) | 11 (21%) | 5 (18%) | 3 (14%) | |
| Total | 53 | 28 | 22 | |
| TL | TILs | p-value | ||
| <10 (N = 42) | ≥10 (N = 44) | NA (N = 17) | ||
| LT (n = 84) | 36 (86%) | 35 (80%) | 13 (76%) | 0.57 |
| ST (n = 19) | 6 (14%) | 9 (20%) | 4 (24%) | |
| Total | 42 | 44 | 17 | |
| TL | pCR | p-value | ||
| pCR (N = 19) | nonPCR (N = 84) | |||
| LT (n = 84) | 16 (84%) | 68 (81%) | >0.99 | |
| ST (n = 19) | 3 (16%) | 16 (19%) | ||
| Total | 19 | 84 | ||
| Variable | Hazard Ratio/Estimate | |Z| | p Value | 95% CI (Profile Likelihood) |
|---|---|---|---|---|
| pCR [No] | 2.34 | 1.50 | 0.133 | 0.8557 to 8.296 |
| Nuclear hTERT [Yes] | 0.67 | 0.89 | 0.376 | 0.2870 to 1.755 |
| Cytoplasmatic hTERT [Yes] | 1.51 | 1.02 | 0.307 | 0.6676 to 3.275 |
| LTL [Short] | 3.39 | 1.98 | 0.048 | 1.172 to 14.33 |
| TILs [<10] | 0.55 | 1.55 | 0.121 | 0.2560 to 1.168 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delmonico, L.; Bines, J.; Nascimento, C.M.d.; Fernandes, P.V.; Barbosa, I.d.S.; Ribeiro, G.B.; de Paula, B.H.R.; Silvestre, R.T.; Ornellas, M.H.F.; Alves, G.; et al. Nuclear and Cytoplasmic hTERT, Tumor-Infiltrating Lymphocytes, and Telomere Elongation Leukocytes Are Independent Factors in the Response to Neoadjuvant Treatment in HER2-Enriched Breast Cancer. Curr. Oncol. 2023, 30, 4094-4109. https://doi.org/10.3390/curroncol30040311
Delmonico L, Bines J, Nascimento CMd, Fernandes PV, Barbosa IdS, Ribeiro GB, de Paula BHR, Silvestre RT, Ornellas MHF, Alves G, et al. Nuclear and Cytoplasmic hTERT, Tumor-Infiltrating Lymphocytes, and Telomere Elongation Leukocytes Are Independent Factors in the Response to Neoadjuvant Treatment in HER2-Enriched Breast Cancer. Current Oncology. 2023; 30(4):4094-4109. https://doi.org/10.3390/curroncol30040311
Chicago/Turabian StyleDelmonico, Lucas, José Bines, Cristina Moreira do Nascimento, Priscila Valverde Fernandes, Isabel de Souza Barbosa, Gabriel Brito Ribeiro, Bruno Henrique Rala de Paula, Rafaele Tavares Silvestre, Maria Helena Faria Ornellas, Gilda Alves, and et al. 2023. "Nuclear and Cytoplasmic hTERT, Tumor-Infiltrating Lymphocytes, and Telomere Elongation Leukocytes Are Independent Factors in the Response to Neoadjuvant Treatment in HER2-Enriched Breast Cancer" Current Oncology 30, no. 4: 4094-4109. https://doi.org/10.3390/curroncol30040311