Incorporating Lymphovenous Anastomosis in Clinically Node-Positive Women Receiving Neoadjuvant Chemotherapy: A Shared Decision-Making Model and Nuanced Approached to the Axilla

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
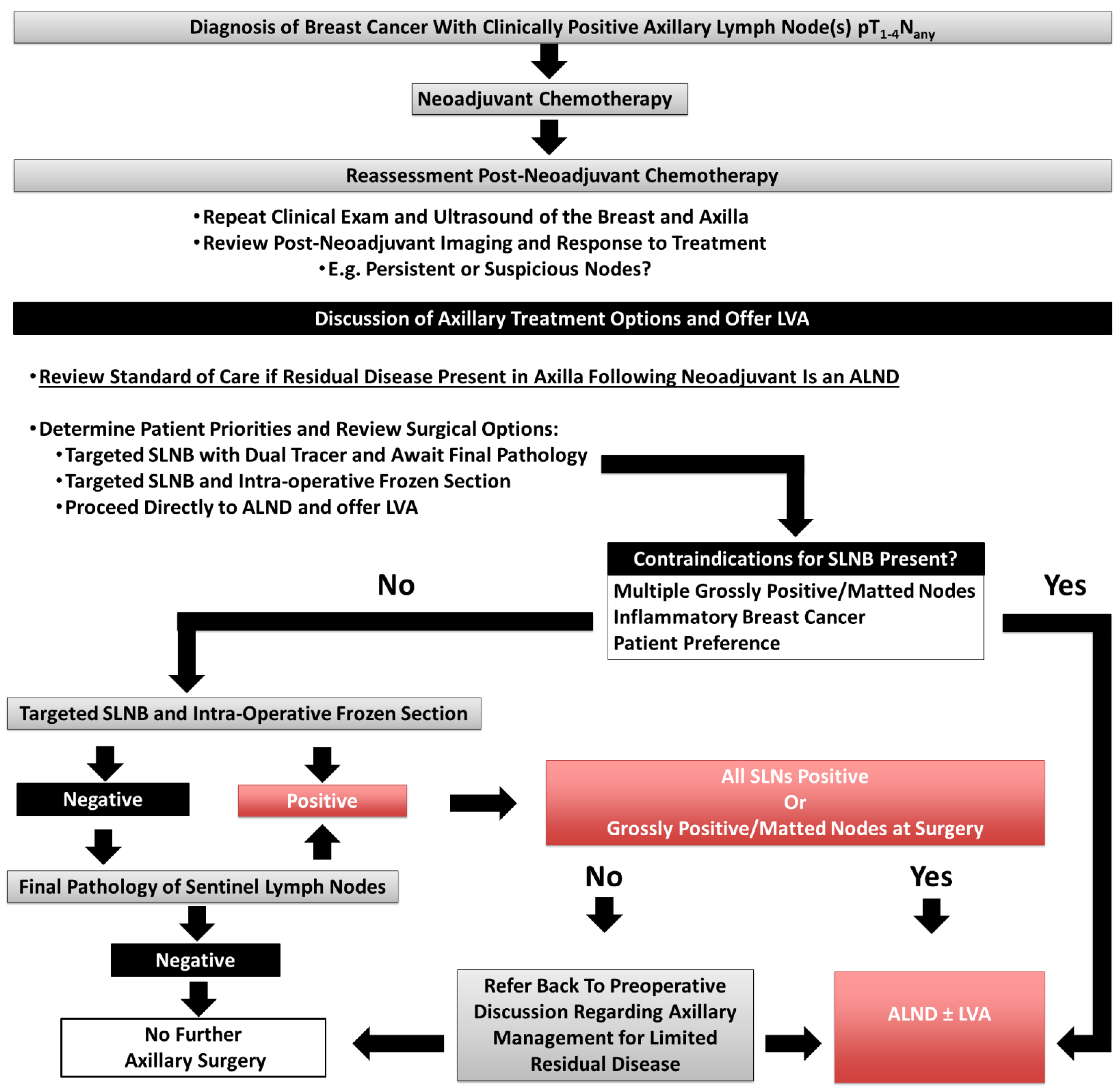
2.2. Patient Discussion Prior to Definitive Surgery
2.3. Lymphatic Reconstruction
2.4. Evaluation for Lymphedema
3. Results
3.1. Overview of Patient Demographics, Breast Cancer, and Initial Evaluation
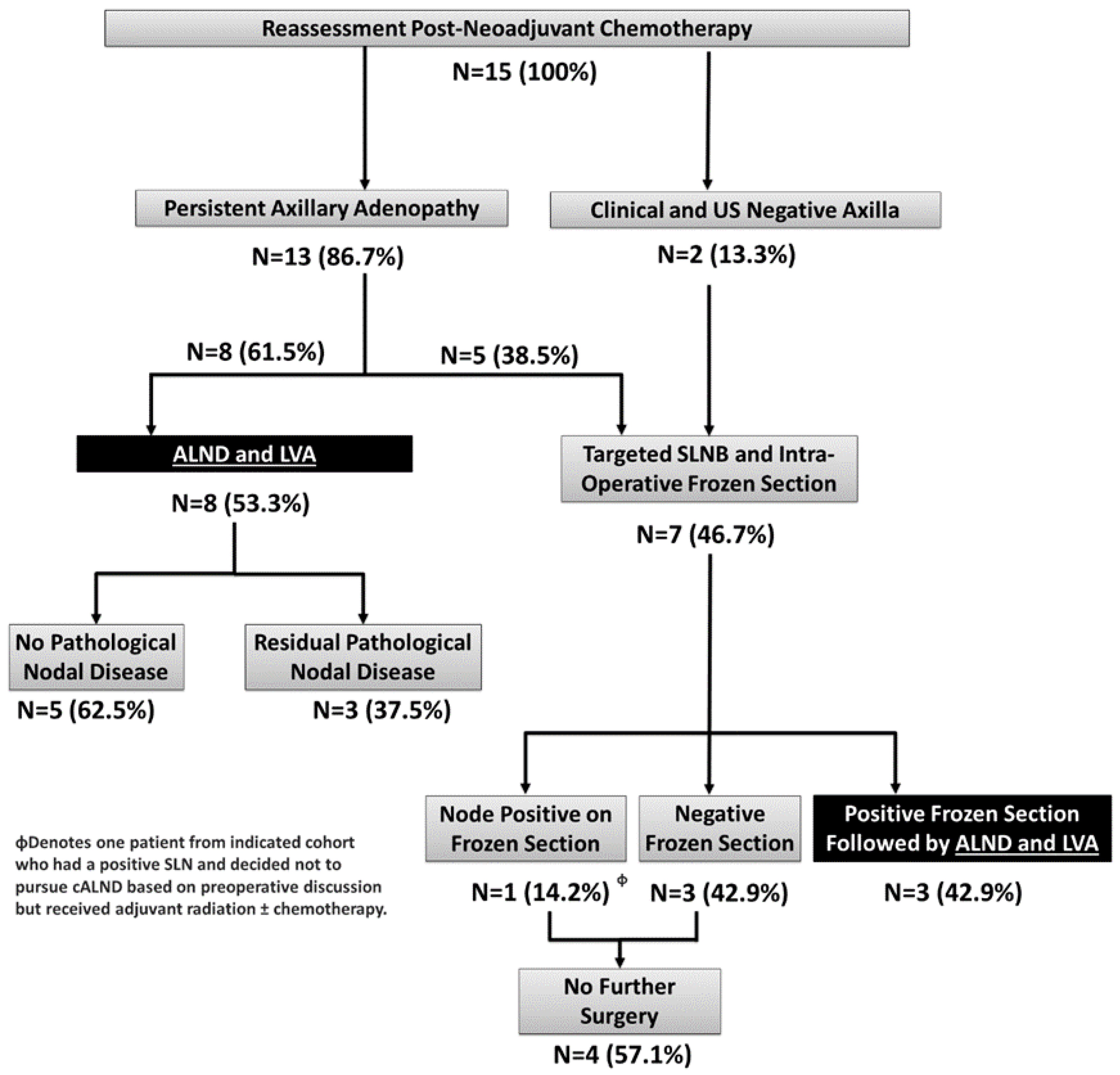
3.2. Reassessment Post-Neoadjuvant Chemotherapy and Definitive Surgery
3.3. Assessment of Pre-Operative US and Intraoperative Frozen Section for Predicting Positive Sentinel Lymph Nodes
3.4. Clinical Outcomes
3.5. Patient-Reported Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hill, W.K.F.; Deban, M.; Platt, A.; Rojas-Garcia, P.; Jost, E.; Temple-Oberle, C. Immediate lymphatic reconstruction during axillary node dissection for breast cancer: A systematic review and meta-analysis. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4291. [Google Scholar] [CrossRef] [PubMed]
- DiSipio, T.; Rye, S.; Newman, B.; Hayes, S. Incidence of unilateral arm lymphoedema after breast cancer: A systematic review and meta-analysis. Lancet Oncol. 2013, 14, 500–515. [Google Scholar] [CrossRef] [PubMed]
- Pasket, E.; Dean, J.; Oliveri, J.; Harrop, J. Cancer-related lymphedema risk factors, diagnosis, treatment, and impact. J. Clin. Oncol. 2012, 30, 3726–3733. [Google Scholar] [CrossRef] [PubMed]
- Boccardo, F.; Casabona, F.; DeCian, F.; Friedman, D.; Villa, G.; Bogliolo, S.; Ferrero, S.; Murelli, F.; Campisi, C. Lymphedema microsurgical preventive healing approach: A new technique for primary prevention of arm lymphedema after mastectomy. Ann. Surg. Oncol. 2009, 16, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Cakmakoglu, C.; Kwiecien, G.J.; Schwarz, G.S.; Gastman, B. Lymphaticovenous bypass for immediate lymphatic reconstruction in locoregional advanced melanoma patients. J. Reconstr. Microsurg. 2020, 36, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Boccardo, F.; Casabona, F.; DeCian, F.; Friedman, D.; Murelli, F.; Puglisi, M.; Campisi, C.C.; Molinari, L.; Spinaci, S.; Dessalvi, S.; et al. Lymphatic microsurgical preventing healing approach (LYMPHA) for primary surgical prevention of breast cancer–related lymphedema: Over 4 year follow up. Microsurgery 2014, 34, 421–424. [Google Scholar] [CrossRef] [PubMed]
- Boileau, J.F.; Poirier, B.; Basik, M.; Holloway, C.M.; Gaboury, L.; Sideris, L.; Meterissian, S.; Arnaout, A.; Brackstone, M.; McCready, D.R.; et al. Sentinel node biopsy after neoadjuvant chemotherapy in biopsy-proven node-positive breast cancer: The SN FNAC study. J. Clin. Oncol. 2015, 33, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, T.; Bauerfeind, I.; Fehm, T.; Fleige, B.; Hausschild, M.; Helms, G.; Lebeau, A.; Liedtke, C.; von Minckwitz, G.; Nekjudova, V.; et al. Sentinel-lymph-node biopsy in patients with breast cancer before and after neoadjuvant chemotherapy (SENTINA): A prospective, multicentre cohort study. Lancet Oncol. 2013, 14, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Boughey, J.C.; Suman, V.J.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Leitch, A.M.; Kuerer, H.M.; Bowling, M.; Flippo-Morton, T.S.; et al. Alliance for Clinical Trials in Oncology. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: The ACOSOG Z1071 (Alliance) clinical trial. JAMA 2013, 310, 1455–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brackstone, M.; Baldassarre, F.G.; Perera, F.E.; Cil, T.; Chavez Mac Gregor, M.; Dayes, I.S.; Engel, J.; Horton, J.K.; King, T.A.; Kornecki, A.; et al. Management of the Axilla in Early-Stage Breast Cancer: Ontario Health (Cancer Care Ontario) and ASCO Guideline. J. Clin. Oncol. 2021, 39, 3056–3082. [Google Scholar] [CrossRef] [PubMed]
- Boughey, J. Comparison of Axillary Lymph Node Dissection with Axillary Radiation for Patients with Node-Positive Breast Cancer Treated with Chemotherapy. Available online: https://clinicaltrials.gov/ct2/show/NCT01901094 (accessed on 17 July 2013).
- Keeley, V.; Crooks, S.; Locke, J.; Veigas, D.; Riches, K.; Hilliam, R. A quality of life measure for limb lymphedema (LYMQOL). J. Lymphoedema 2012, 5, 26–37. [Google Scholar]
- Karges, J.R.; Mark, B.E.; Stikeleather, S.J.; Worrell, T.W. Concurrent validity of upper-extremity volume estimates: Comparison of calculated volume derived from girth measurements and water displacement volume. Phys. Ther. 2003, 83, 134–145. [Google Scholar] [CrossRef] [PubMed]
- McMurtry, V.; Poretta, J.M.; Factor, R.E. After neoadjuvant therapy, axillary sentinel lymph node frozen sections from breast cancer patients are accurately diagnosed using telepathology. J. Pathol. Inform. 2022, 13, 100092. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, A.; Nigri, G.; Maggi, S.; Stanzani, G.; Vitale, V.; Vecchione, A.; Nania, A.; Amanti, C. Role of frozen section in sentinel lymph node biopsy for breast cancer in the era of the ACOSOG Z0011 and IBCSG 23-10 trials. Surgeon 2018, 16, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Rutgers, E.J.; Donker, M.; Poncet, C.; Straver, M.E.; Meijnen, P.; Velde, C.J.; Mansel, R.E.; Blanken, C.; Przalesi, L.; Klinkenbijl, J.H.; et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer patients: 10 year follow up results of the EORTC AMAROS trial (EORTC 10981/22023). Cancer Res. 2019, 79, GS4. [Google Scholar] [CrossRef]
- McDuff, S.G.R.; Mina, A.I.; Brunelle, C.L.; Salama, L.; Warren, L.E.G.; Abouegylah, M.; Swaroop, M.; Skolny, M.N.; Asdourian, M.; Gillespie, T.; et al. Timing of lymphedema after treatment for breast cancer: When are patients most At risk? Int. J. Radiat. Oncol. 2019, 103, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.R.; Asban, A.; Granoff, M.D.; Kang, C.O.; Lee, B.T.; Chatteriee, A.; Singhal, D. Is immediate lymphatic reconstruction cost-effective. Ann. Surg. 2021, 274, e581–e588. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographics | (N, %) |
|---|---|
| Age (mean, range) | 49.9 (32–75) |
| Menopausal Status | |
| Pre-Menopause | 11 (73.3%) |
| Post-Menopause | 4 (26.7%) |
| BMI (kg/m2) | |
| Non-Obese (BMI < 30) | 11 (73.3%) |
| Obese (BMI > 30) | 4 (26.7%) |
| Tumour Characteristics | |
| Histological Subtype | |
| Ductal | 12 (80.0%) |
| Lobular | 1 (6.7%) |
| Not Specified | 2 (13.3%) |
| Receptor Subtype | |
| ER/PR Positive HER-2 Negative | 4 (26.7%) |
| HER-2 Positive | 5 (33.3%) |
| Triple Negative | 6 (40.0%) |
| TNM Staging | |
| Tumour (T) Stage | |
| T0 | 1 (6.7%) |
| T1 | 0 (0%) |
| T2 | 10 (66.7%) |
| T3 | 4 (20.0%) |
| T4 | 1 (6.7%) |
| Nodal (N) Stage | |
| N1 | 11 (73.3%) |
| N2 | 4 (26.7%) |
| N3 | 0 (0%) |
| Clinical Stage | |
| I | 0 (0%) |
| II | 8 (53.3%) |
| III | 7 (46.7%) |
| IV | 0 (0%) |
| Metric | All Patients N = 15 | cALND and LVA N = 11 | SLNB Only N = 4 | Patients without Lymphedema N = 14 | Patient with Lymphedema N = 1 |
|---|---|---|---|---|---|
| Function | 1.1 ± 0.2 | 1.2 ± 0.2 | 1.1 ± 0.1 | 1.1 ± 0.2 | 1.5 |
| Appearance | 1.1 ± 0.3 | 1.2 ± 0.3 | 1.0 ± 0.0 | 1.1 ± 0.3 | 1 |
| Symptoms | 1.4 ± 0.4 | 1.4 ± 0.4 | 1.5 ± 0.5 | 1.4 ± 0.3 | 2.3 |
| Mood | 1.2 ± 0.4 | 1.1 ± 0.2 | 1.1 ± 0.2 | 1.2 ± 0.4 | 1.2 |
| Overall Quality of Life | 8.1 ± 0.9 | 8.1 ± 0.6 | 8.1 ± 0.6 | 8.1 ± 0.9 | 8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lustig, D.B.; Temple-Oberle, C.; Bouchard-Fortier, A.; Quan, M.L. Incorporating Lymphovenous Anastomosis in Clinically Node-Positive Women Receiving Neoadjuvant Chemotherapy: A Shared Decision-Making Model and Nuanced Approached to the Axilla. Curr. Oncol. 2023, 30, 4041-4051. https://doi.org/10.3390/curroncol30040306
Lustig DB, Temple-Oberle C, Bouchard-Fortier A, Quan ML. Incorporating Lymphovenous Anastomosis in Clinically Node-Positive Women Receiving Neoadjuvant Chemotherapy: A Shared Decision-Making Model and Nuanced Approached to the Axilla. Current Oncology. 2023; 30(4):4041-4051. https://doi.org/10.3390/curroncol30040306
Chicago/Turabian StyleLustig, Daniel Ben, Claire Temple-Oberle, Antoine Bouchard-Fortier, and May Lynn Quan. 2023. "Incorporating Lymphovenous Anastomosis in Clinically Node-Positive Women Receiving Neoadjuvant Chemotherapy: A Shared Decision-Making Model and Nuanced Approached to the Axilla" Current Oncology 30, no. 4: 4041-4051. https://doi.org/10.3390/curroncol30040306