Functional Outcomes and Shoulder Instability in Reconstruction of Proximal Humerus Metastases

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
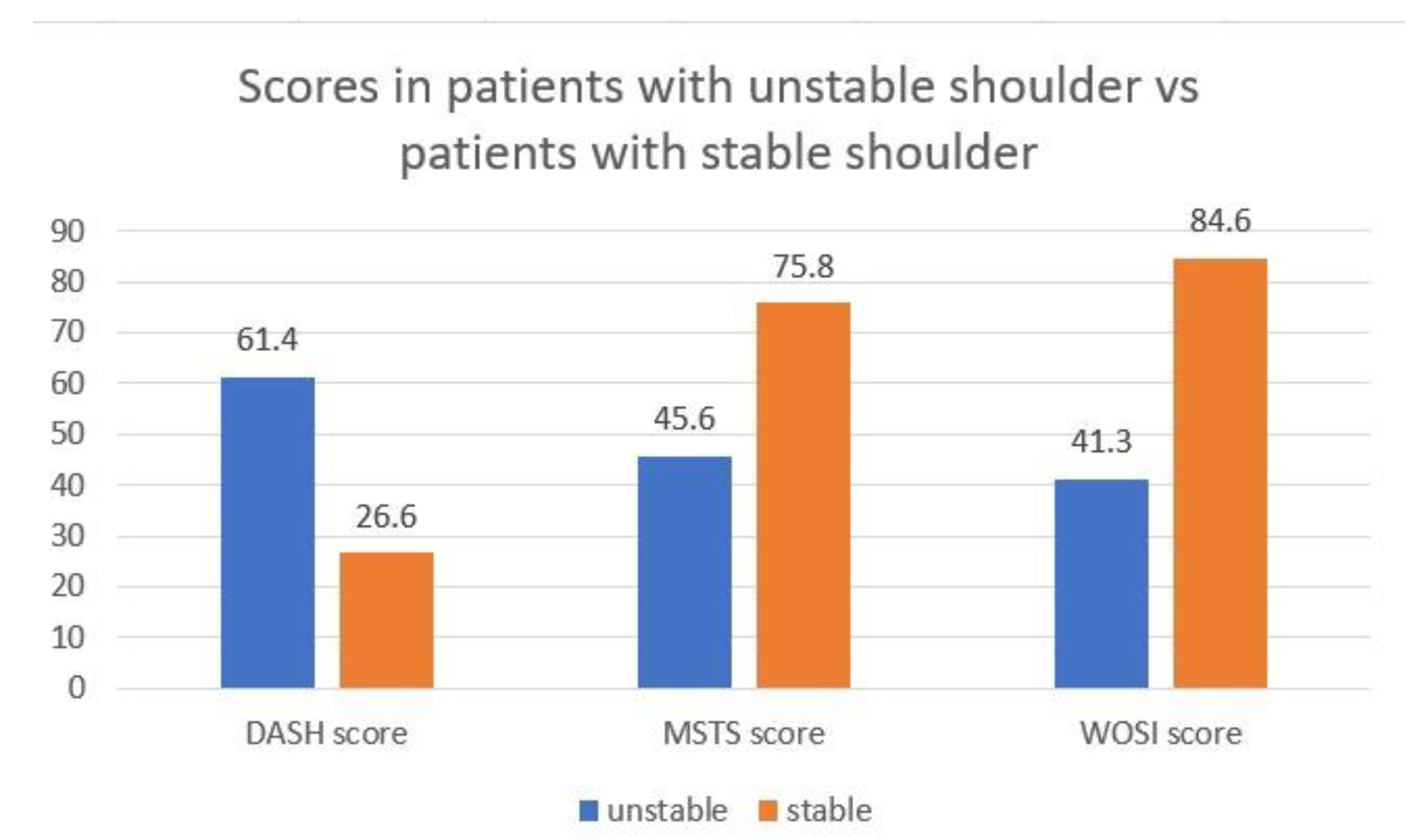
3.1. Shoulder’s Stability
3.2. Resection Surgery
3.3. Surgery Approach
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Ferlauto, H.R.; Wickman, J.R.; Lazarides, A.L.; Hendren, S.; Visgauss, J.D.; Brigman, B.E.; Anakwenze, O.A.; Klifto, C.S.; Eward, W.C. Reverse total shoulder arthroplasty for oncologic reconstruction of the proximal humerus: A systematic review. J. Shoulder Elbow Surg. 2021, 30, e647–e658. [Google Scholar] [CrossRef] [PubMed]
- Gebhart, M.; Dequanter, D.; Vandeweyer, E. Metastatic involvement of the humerus: A retrospective study of 51 cases. Acta. Orthop. Belg. 2001, 67, 456–463. [Google Scholar] [PubMed]
- Rovere, G.; Meschini, C.; Piazza, P.; Messina, F.; Caredda, M.; De Marco, D.; Noia, G.; Maccagnano, G.; Ziranu, A. Proximal humerus fractures treatment in adult patients with bone metastasis. Eur. Rev. Med. Pharmacol. Sci. 2022, 26 (Suppl. S1), 100–105. [Google Scholar] [PubMed]
- Vitiello, R.; Bellieni, A.; Oliva, M.S.; Di Capua, B.; Fusco, D.; Careri, S.; Colloca, G.F.; Perisano, C.; Maccauro, G.; Lillo, M. The importance of geriatric and surgical co-management of elderly in muscoloskeletal oncology: A literature review. Orthop. Rev. 2020, 12 (Suppl. 1), 8662. [Google Scholar] [CrossRef] [PubMed]
- Ayvaz, M.; Cetik, R.M.; Bakircioglu, S.; Tokgozoglu, A.M. Proximal Humerus Tumors: Higher-than-Expected Risk of Revision With Constrained Reverse Shoulder Arthroplasty. Clin. Orthop. Relat. Res. 2020, 478, 2585–2595. [Google Scholar] [CrossRef]
- D′Arienzo, A.; Ipponi, E.; Ruinato, A.D.; De Franco, S.; Colangeli, S.; Andreani, L.; Capanna, R. Proximal Humerus Reconstruction after Tumor Resection: An Overview of Surgical Management. Adv. Orthop. 2021, 2021, 5559377. [Google Scholar] [CrossRef] [PubMed]
- Vitiello, R.; Matrangolo, M.R.; El Motassime, A.; Perna, A.; Cianni, L.; Maccauro, G.; Ziranu, A. Three-Dimension-Printed Custom-Made Prosthetic Reconstructions in Bone Tumors: A Single Center Experience. Curr. Oncol. 2022, 29, 4566–4577. [Google Scholar] [CrossRef]
- Capanna, R.; Piccioli, A.; Di Martino, A.; Daolio, P.A.; Ippolito, V.; Maccauro, G.; Piana, R.; Ruggieri, P.; Gasbarrini, A.; Spinelli, M.S.; et al. Management of long bone metastases: Recommendations from the Italian Orthopaedic Society bone metastasis study group. Expert Rev. Anticancer. Ther. 2014, 14, 1127–1134. [Google Scholar] [CrossRef]
- Palumbo, B.T.; Henderson, E.R.; Groundland, J.S.; Cheong, D.; Pala, E.; Letson, G.D.; Ruggieri, P. Advances in segmental endoprosthetic reconstruction for extremity tumors: A review of contemporary designs and techniques. Cancer Control 2011, 18, 160–170. [Google Scholar] [CrossRef] [Green Version]
- Kirkley, A.; Griffin, S.; McLintock, H.; Ng, L. The development and evaluation of a disease-specific quality of life measurement tool for shoulder instability. The western Ontario shoulder instability index (WOSI). Am. J. Sports Med. 1998, 26, 764–772. [Google Scholar] [CrossRef]
- Trovarelli, G.; Cappellari, A.; Angelini, A.; Pala, E.; Ruggieri, P. What Is the Survival and Function of Modular Reverse Total Shoulder Prostheses in Patients Undergoing Tumor Resections in Whom an Innervated Deltoid Muscle Can Be Preserved? Clin. Orthop. Relat. Res. 2019, 477, 2495–2507. [Google Scholar] [CrossRef] [PubMed]
- Schneider, K.N.; Bröking, J.N.; Gosheger, G.; Lübben, T.; Hardes, J.; Schorn, D.; Smolle, M.A.; Theil, C.; Andreou, D. What Is the Implant Survivorship and Functional Outcome After Total Humeral Replacement in Patients with Primary Bone Tumors? Clin. Orthop. Relat. Res. 2021, 479, 1754–1764. [Google Scholar] [CrossRef] [PubMed]
- Fiore, M.; Sambri, A.; Giannini, C.; Zucchini, R.; De Cristofaro, R.; De Paolis, R.M. Anatomical and reverse megaprosthesis in proximal humerus reconstructions after oncologic resections: A systematic review and meta—analysis. Arch. Orthop. Trauma Surg. 2022, 142, 2459–2469. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Guo, Z.; Li, J.; Li, X.; Sang, H. Functional outcomes and complications of reconstruction of the proximal humerus after intra-articular tumor resection. Orthop. Surg. 2010, 2, 19–26. [Google Scholar] [CrossRef]
- Ahrens, H.; Theil, C.; Gosheger, G.; Rödl, R.; Deventer, N.; Rickert, C.; Ackmann, T.; Schwarze, J.; Klingebiel, S.; Schneider, K.N. The Bateman-Type Soft Tissue Reconstruction around Proximal or Total Humeral Megaprostheses in Patients with Primary Malignant Bone Tumors—Functional Outcome and Endoprosthetic Complications. Cancers 2021, 13, 3971. [Google Scholar] [CrossRef]
- Jawad, M.U.; Scully, S.P. In brief: Classifications in brief: Mirels’ classification: Metastatic disease in long bones and impending pathologic fracture. Clin. Orthop. Relat. Res. 2010, 468, 2825–2827. [Google Scholar] [CrossRef] [Green Version]
- Enneking, W.F.; Spanier, S.S.; Goodman, M.A. A system for the surgical staging of musculoskeletal sarcoma. Clin. Orthop. Relat. Res. 1980, 153, 106–120. [Google Scholar] [CrossRef]
- Enneking, W.F.; Dunham, W.; Gebhardt, M.C.; Malawar, M.; Pritchard, D.J. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin. Orthop. Relat. Res. 1993, 286, 241–246. [Google Scholar] [CrossRef]
- Hudak, P.L.; Amadio, P.C.; Bombardier, C. Development of an upper extremity outcome measure: The DASH (Disabilities of the Arm, Shoulder and Hand). Am. J. Ind. Med. 1996, 29, 602–608. [Google Scholar] [CrossRef]
- Gummesson, C.; Atroshi, I.; Ekdah, C. The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: Longitudinal construct validity and measuring self-rated health change after surgery. BMC Musculoskelet. Disord. 2003, 4, 11. [Google Scholar] [CrossRef] [Green Version]
- Salomonsson, B.; Ahlström, S.; Dalén, N.; Lillkrona, U. The Western Ontario Shoulder Instability Index (WOSI): Validity, reliability, and responsiveness retested with a Swedish translation. Acta. Orthop. 2009, 80, 233–238. [Google Scholar] [CrossRef]
- Gerber, C.; Nyffeler, R.W. Classification of glenohumeral joint instability. Clin. Orthop. Relat. Res. 2002, 400, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Manabe, J.; Kawaguchi, N.; Matsumoto, S.; Tanizawa, T. Surgical treatment of bone metastasis: Indications and outcomes. Int. J. Clin. Oncol. 2005, 10, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Pinnamaneni, S.; Damron, T.A. Proximal humerus reconstruction in orthopedic oncology. J. Cancer Metastasis Treat. 2021, 7, 7. [Google Scholar] [CrossRef]
- Ebeid, W.A.; Eldaw, S.; Badr, I.T.; Mesregah, M.K.; Hasan, B.Z. Outcomes of modular endoprosthesis reconstruction versus cement spacer reconstruction following resection of proximal humeral tumors. BMC Musculoskelet. Disord. 2022, 23, 484. [Google Scholar] [CrossRef] [PubMed]
- D’Adamio, S.; Cazzato, G.; Ziranu, A.; Sgambato, A.; Rosa, M.A.; Maccauro, G. Soft tissue adhesion patterns over Trevira tube on modular endoprosthesis for malignant bone tumours: An in vitro study. J. Biol. Regul. Homeost. Agents 2017, 31 (Suppl. S1), 37–42. [Google Scholar] [PubMed]
- Teunis, T.; Nota, S.P.; Hornicek, F.J.; Schwab, J.H.; Lozano-Calderón, S.A. Outcome after reconstruction of the proximal humerus for tumor resection: A systematic review. Clin. Orthop. Relat. Res. 2014, 472, 2245–2253. [Google Scholar] [CrossRef] [Green Version]
- Trikoupis, I.G.; Savvidou, O.D.; Tsantes, A.G.; Papadopoulos, D.V.; Goumenos, S.D.; Vottis, C.; Kaspiris, A.; Kontogeorgakos, V.; Papagelopoulos, P.J. Prosthetic Reconstruction of the Shoulder After Resection of Proximal Humerus Bone Tumor. Orthopedics 2022, 45, e335–e341. [Google Scholar] [CrossRef]
- Van Der Linde, J.A.; Van Kampen, D.A.; Van Beers, L.W.; Van Deurzen, D.F.; Saris, D.B.; Terwee, C.B. The Responsiveness and Minimal Important Change of the Western Ontario Shoulder Instability Index and Oxford Shoulder Instability Score. J. Orthop. Sports Phys. Ther. 2017, 6, 402–410. [Google Scholar] [CrossRef]
- Vitiello, R.; Perisano, C.; Greco, T.; Cianni, L.; Polichetti, C.; Comodo, R.M.; De Martino, I.; La Vergata, V.; Maccauro, G. Intramedullary nailing vs modular megaprosthesis in extracapsular metastases of proximal femur: Clinical outcomes and complication in a retrospective study. BMC Musculoskelet. Disord. 2022, 22 (Suppl. S2), 1069. [Google Scholar] [CrossRef]
- D’Adamio, S.; Ziranu, A.; Cazzato, G.; Sanguinetti, M.; Manicone, P.F.; Rosa, M.A.; Maccauro, G. Antifungal properties of silver coating on tumour endoprostheses: An in vitro study. Eur. Rev. Med. Pharmacol. Sci. 2019, 23 (Suppl. S2), 252–257. [Google Scholar] [PubMed]
- Vitiello, R.; Bocchi, M.B.; Gessi, M.; Greco, T.; Cianni, L.; de Maio, F.; Pesce, V.; Maccauro, G.; Perisano, C. Induced membrane by silver-coated knee megaprosthesis: Keep or toss? J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. S1), 101–106. [Google Scholar] [PubMed]
- Donati, F.; Di Giacomo, G.; Ziranu, A.; Spinelli, S.; Perisano, C.; Rosa, M.A.; Maccauro, G. Silver coated prosthesis in oncological limb salvage surgery reduce the infection rate. J. Biol. Regul. Homeost. Agents 2015, 29 (Suppl. S4), 149–155. [Google Scholar] [PubMed]
- El Ezzo, O.; Oliva, M.S.; Cauteruccio, M.; Saracco, M.; Vitiello, R.; Maccauro, G.; Perisano, C. Innovations in prevention of infections in oncological megaprostheses: A narrative review. J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. S3), 275–278. [Google Scholar]



{kind=link}
{kind=link}
| Individual-Level Variables | N | Percent | Mean | SD |
|---|---|---|---|---|
| Age | 61.3 | 13.26 | ||
| 40–50 | 4 | 20% | ||
| 51–60 | 4 | 20% | ||
| 61–70 | 8 | 40% | ||
| 71–80 | 2 | 10% | ||
| 81–90 | 2 | 10% | ||
| Gender | ||||
| Male | 12 | 60% | ||
| Female | 8 | 40% | ||
| Comorbidities | ||||
| Diabetes | 11 | 55% | ||
| Thyroid pathologies | 2 | 10% | ||
| Primary tumor | ||||
| Kidney | 8 | 40% | ||
| Breast | 4 | 20% | ||
| Lung | 2 | 10% | ||
| Brain | 2 | 10% | ||
| Lymphoma | 2 | 10% | ||
| Uterus | 2 | 10% | ||
| Total | 20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Motassime, A.; Meschini, C.; Di Costa, D.; Rovere, G.; Matrangolo, M.R.; De Maio, F.; Farsetti, P.; Ziranu, A.; Maccauro, G.; Vitiello, R. Functional Outcomes and Shoulder Instability in Reconstruction of Proximal Humerus Metastases. Curr. Oncol. 2023, 30, 3571-3579. https://doi.org/10.3390/curroncol30040272
El Motassime A, Meschini C, Di Costa D, Rovere G, Matrangolo MR, De Maio F, Farsetti P, Ziranu A, Maccauro G, Vitiello R. Functional Outcomes and Shoulder Instability in Reconstruction of Proximal Humerus Metastases. Current Oncology. 2023; 30(4):3571-3579. https://doi.org/10.3390/curroncol30040272
Chicago/Turabian StyleEl Motassime, Alessandro, Cesare Meschini, Doriana Di Costa, Giuseppe Rovere, Maria Rosaria Matrangolo, Fernando De Maio, Pasquale Farsetti, Antonio Ziranu, Giulio Maccauro, and Raffaele Vitiello. 2023. "Functional Outcomes and Shoulder Instability in Reconstruction of Proximal Humerus Metastases" Current Oncology 30, no. 4: 3571-3579. https://doi.org/10.3390/curroncol30040272