1. Introduction
Chemotherapy-induced nausea and vomiting (CINV) is a frequent adverse event that affects up to 60–80% of cancer patients without antiemetic prophylaxis treatment [
1]. CINV significantly impairs cancer patients’ quality of life and affects the treatment outcome, including chemotherapy (CT) discontinuation, long-term response to anticancer treatment, and, ultimately, patient survival [
1,
2,
3,
4]. As nausea and vomiting are considered a certainty during the CT treatment, they represent a critical concern, being, thus, frequently anticipated by cancer patients [
2]. Notably, patient expectations regarding the consequences of the treatment are essential, considering that previous studies on nausea and vomiting suggest an association between the expectancy of CINV and its occurrence during treatment [
3]. Furthermore, it has been previously demonstrated that uncontrolled CINV is a pivotal factor for CINV repetition in subsequent cycles, increasing the probability of its occurrence by 6.5 and 14 times in cycles 2 and 3, respectively [
5,
6]. Therefore, it is crucial to address CINV from a preventive perspective so that patients remain engaged in their CT regimens, improving their compliance with anticancer treatments and their quality of life.
Previous studies described that current antiemetic treatments provide suboptimal CINV control, particularly during the delayed phase in patients receiving Highly Emetogenic Chemotherapy (HEC) or Moderate Emetogenic Chemotherapy (MEC) [
7]. Furthermore, a prospective observational study carried out in Portugal that analysed how health care professionals (HCP) perceive CINV compared to the effects directly reported by patients disclosed that HCP significantly underestimates the incidence and the negative impact of acute and delayed nausea in the daily life of patients, after HEC and MEC [
8].
Several international scientific societies, such as the Multinational Association for Supportive Care in Cancer (MASCC), the European Society for Medical Oncology (ESMO), and the National Comprehensive Cancer Network (NCCN), offer recommendations for antiemetic prophylaxis according to the emetogenicity grade of the oral antineoplastic agents. Globally, these guidelines share many fundamental similarities and focus on preventing acute and delayed nausea and vomiting induced by HEC and MEC. Notably, a recent update on MASCC/ESMO guidelines included two newly U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMA)-approved neurokinin-1 receptor antagonists (NK1-RAs), whose role in preventing acute and delayed nausea and vomiting is still under discussion [
9]. According to the recommendations of the Portuguese Oncology Nursing Association, the antiemetic agents used for the prevention of CINV are 5-HT3 receptor antagonists (dolasetron, granisetron, ondansetron, palonosetron); neurokinin-1 receptor antagonists (aprepitant, fosaprepitant, NEPA (nesupitant plus palonosetron)); corticosteroids (dexamethasone, methylprednisolone); dopamine receptor antagonists (metoclopramide, haloperidol), and benzodiazepines (lorazepam). Importantly, this working group also emphasises that an adequate regimen must be tailored to each situation [
10].
Although the international guidelines for the prevention and treatment of CINV are widespread, their application in a real-life context remains low [
7], and the adherence of HCP to those guidelines is considered a significant problem [
8].
Thus, the present study aims to raise awareness of supportive care for cancer patients, highlighting the need to improve CINV prophylactic treatment and the adoption of guidelines in Portuguese clinical practice. The primary objective of this study was to evaluate the achievement of a complete response to CINV prophylaxis during the first five days after CT in patients receiving HEC or MEC in Portugal. The secondary objectives were to address the impact of CINV on the quality of life in cancer patients receiving HEC or MEC and to describe all emetic episodes seven days after CT.
2. Methods
2.1. Study Design
This observational, non-interventional, prospective, multicenter study aimed to collect real-life data on CINV control with current antiemetic therapies in patients naïve and non-naïve to MEC or HEC in an outpatient cancer clinic in Portugal.
2.2. Study Setting and Patient Population
The study included adult patients (≥18 years) CT-naïve or CT-non-naïve, both males and females, with any solid malignant tumours, with ECOG Scale of Performance Status between 0 and 2. Each patient was assessed once per cycle, not limited to only one cycle evaluation per CT regimen. The CT-non-naïve patients included those treated with single-day HEC or MEC or who had already received at least two CT cycles, considering the current CT regimen. The antiemetic and anticancer therapies were prescribed at the investigator’s discretion, meaning that patient assignment to a therapeutic strategy was not decided in advance by the study protocol but fell within current clinical practice. Patients had to be able to complete written questionnaires and complete patient diaries. Patients with nausea or vomiting not related to any CT cycle, other disorders or medications, or under chemoradiotherapy or CT with low or minimal emetic risk, or vomiting within 24 h (h) before the CT cycle or with unstable concomitant diseases or uncontrolled brain metastasis were excluded from the study. Pregnant or breastfeeding women and patients under chronic systemic corticosteroid treatment were also excluded.
2.3. Sample Size Determination
The study was designed to include ca. 120 patients with solid malignant tumours treated with single-day HEC or MEC who had already received at least two CT cycles. The sample size was determined based on the study’s primary objective, which aimed to evaluate the percentage of patients with a complete response for 120 h after CT, in patients receiving HEC or MEC and under CINV prophylaxis guidelines, in Portugal. The sampling calculation assumed a complete response (no vomiting, no rescue medication, and no more than mild nausea) in 55% of the CT cycles. Considering this hypothesis, and an error margin lower than 7%, for a 95% interval, it was necessary to evaluate 194 cycles.
2.4. Procedures and Assessments
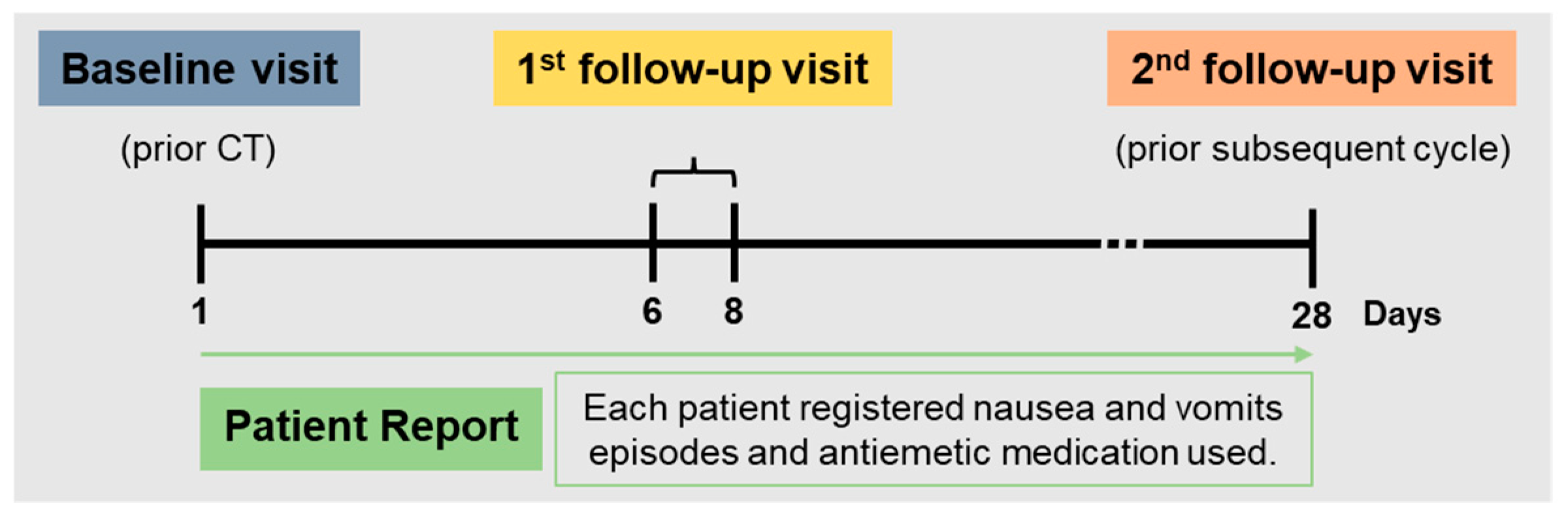
The antiemetic and anticancer therapies were prescribed according to current clinical practice. Specifically, the antiemetic agents used for the prevention of CINV were 5-HT3 receptor antagonists (dolasetron, granisetron, ondansetron, palonosetron); neurokinin-1 receptor antagonists (aprepitant, fosaprepitant, NEPA (nesupitant plus palonosetron)); corticosteroids (dexamethasone, methylprednisolone); dopamine receptor antagonists (metoclopramide, haloperidol), and benzodiazepines (lorazepam). No additional diagnostic or monitoring procedures were applied to the patients except if the investigator decided. CT regimens were categorised according to international guidelines (MASCC, ESMO, and NCCN) and based on the emetogenic potential of the agent. Each patient was evaluated three times during the study period: baseline, follow-up 1, and follow-up 2. Baseline visits occurred on day 1, before the administration of CT, and follow-up visits occurred following a clinical practice. The first follow-up visit occurred between days 6 and 8 of the CT cycle, and the second follow-up was on day 28, just before the subsequent CT cycle. During the study period, each patient filled out a diary to record nausea and vomits episodes and antiemetic medication use (
Figure 1).
2.5. Statistical Analysis
The primary endpoint was the proportion of patients who achieved a complete response to CINV prophylaxis in the first five days (120 h) after CT and the respective 95% confidence interval.
The secondary endpoints were the percentage of change in the FLIE questionnaire score from baseline to day 7, the median and mean time to failure, defined as the time until the CINV control (occurrence of the first emetic episode or the first use of rescue medication), and the characterisation of nausea severity during the five days after CT measured by a Likert scale.
All variables were described using mean, median, standard deviation, interquartile range (IQR), maximum and minimum for continuous variables, and absolute (n) and relative frequencies (%) for categorical variables. Time to failure was estimated using Kaplan–Meier analysis and the response agreement between the physician’s assessment and the patient’s self-report through Cohen’s Kappa test. A 0.05 significance level was considered for all tests performed.
3. Results
A total of 115 patients were included from eight sites in Portugal. The baseline patients’ demographic and clinical characteristics are disclosed in
Table 1.
Most participants were female (61%), and the median age at baseline was 59.5 (IQR: 16; 51–67 CI 95%). The most frequent primary diagnosis was breast cancer (30%), followed by colon cancer (15%) and lung cancer (14%). Most of the participants in the study had an ECOG Performance Status of 0, and only a minority had a history of previous CT or radiation therapy (31% and 18%, respectively). The CT regimens and antiemetic prophylaxis performed among participants are shown in
Table 2 and
Table 3. The most common CT regimens were based on oxaliplatin or irinotecan, and the most used antiemetic agents were dexamethasone, metoclopramide, and ondansetron.
Regarding the primary endpoint, a complete response (no emetic episodes, no use of rescue antiemetic medication, and no more than mild nausea) was observed in 72% [95% CI 63.8–79.3] of the CT cycles during the 120 h (5 days) after CT. Between days 1 and 7 after CT, patients reported having experienced at least one emetic episode, one nausea episode, or used rescue antiemetic medication in 43% of the cycles. Significantly, this percentage dropped to 29% if considering only emetic episodes or using rescue medication.
The complete characterisation of nausea and emesis episodes and their severity classification are presented in
Table 4. The median time until the first emetic episode or first use of rescue antiemetic therapy was 15 h, varying from 8 to 148 h from the first CT administration. Approximately 25% of patients classified their emetic/nausea episodes as severe, 30% as mild [
1,
2], and the remaining as moderate.
Regarding the assessment of the patient’s quality of life, those without and with CINV have a mean FLIE Total Score of 46.2 at baseline and 46.4 at the first follow-up visit (
p = 0.502) and a mean FLIE Total Score of 56.1 at baseline and 60.9 at the first follow-up visit (
p-value = 0.149), respectively. Therefore, there was no difference in FLIE Total Score between baseline and the first follow-up visit (7 days after CT) in patients with and without CINV. FLIE Total Scores are reported in
Table 5.
Before the CT administration, the physicians expected that 40% of patients would experience nausea or emetic episodes between days 1 and 7 after the CT cycle. The severity of expected patients’ nausea and emesis episodes for seven days after CT was mainly graded from 1 to 3, according to physicians’ expectations.
According to physicians’ assessment of patients’ diaries analysis, CINV occurred in 37% of patients between days 1 and 7 after the CT cycle. Patients’ nausea and emesis episodes for seven days after CT were mainly classified as a severity grade of 3 or 4. Accordingly to the physicians’ assessment, CINV occurred in 27% of patients between days 8 and 28 after CT and was also classified mainly as grade 3 or 4. In fact, 42% of the patients reported having experienced nausea or emetic episodes in the first week after CT.
The response agreement between physician assessment and patient reports was assessed using Cohen’s Kappa and disclosed 92.7% (p < 0.001).
4. Discussion
Despite substantial advances in supportive care of cancer patients over the last decades, through developing recommendations to improve antiemetic strategies [
9,
11,
12], CINV remains one of cancer treatments’ most distressing and debilitating adverse effects [
13]. Accordingly, this study confirms the high prevalence of CINV as in 43% of all the CT cycles, patients reported having experienced at least one emetic episode, one nausea episode, or used rescue antiemetic medication during the first week after CT.
Though the data herein collected shows that the prophylaxis treatments were overall effective in the prevention of emesis in 72% of the cycles (patients have a complete response, meaning no emetic episodes, no use of rescue antiemetic medication, and no mild nausea for five days after CT), there is still space for improvement. These results disclose that the doublet regimen (specifically, dexamethasone and a 5-HT3) is insufficient to prevent CINV episodes in MEC and HEC patients. Based on this, it is fundamental to discuss new therapeutic strategies comprising the use of NK1-RAs medication and the adoption of more effective international antiemetic guidelines in the Portuguese clinical practice to improve CINV supportive care for cancer patients.
Nevertheless, a complete emetic response is not an appropriate endpoint to characterise the treatment effect on nausea [
14], and control of nausea still represents the most critical challenge in CINV. Although nausea and vomiting have always been treated as unified symptoms, they represent different phenomena. Notably, nausea has a higher incidence and is more challenging to evaluate, quantify and control with medication [
15,
16]. Additionally, our data corroborate that nausea has also been described to affect patients’ quality of life [
15,
17,
18]. Nausea episodes are frequently described during the first week after CT compared to emesis episodes. As already described, the optimal control of CINV is particularly relevant concerning nausea, and its adequate prevention, rather than just vomiting, remains an unmet need in patients submitted to CT [
16,
19,
20].
No significant differences in the patient’s quality of life were detected. Specifically, the variation in the score of the FLIE questionnaire between baseline and the first follow-up visit after seven days upon CT was not significant, which might result from the “ceiling effect” caused by high baseline and follow-up scores that usually lead to modest alterations.
Noteworthy, our study disclosed a high response agreement between patients’ reports and physicians’ assessments concerning nausea or emetic episodes. This finding differs from previous studies on this topic, where HCP significantly underestimate the incidence of acute and delayed nausea after HEC and MEC compared to patients’ reports [
7,
21]. This may indicate that, in the last decades, physicians are becoming increasingly aware of CINV, suggesting the achievement of an important milestone in implementing CINV prophylaxis strategies [
22,
23].
5. Conclusions
In conclusion, this study discloses that a significant proportion of complete response has been achieved, suggesting that a therapeutic effort is being made to minimise this unagreeable side effect of anticancer regimens and improve cancer patients’ quality of life. Nonetheless, despite the several improvements in clinical practice and the discovery of new treatments, CINV still represents a pertinent question in cancer patients submitted to HEC or MEC in Portugal, pointing out the need to implement more effective strategies and adopt antiemetic guideline directives.
Author Contributions
A.A.: Investigation, Conceptualization, Supervision, Writing—Original Draft, Writing—Review and Editing. N.T.: Investigation. A.L.F.: Investigation. R.G.: Investigation. J.C.M.: Investigation. B.P.: Investigation. A.C.: Investigation. F.B.: Investigation. A.M.: Conceptualisation, Methodology, Formal analysis, Writing–Original Draft. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by VIFOR Pharma.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board/Ethics Committee of the centres involved in this study (Centro Hospitalar Universitário do Porto, Centro Hospitalar Universitário de São João, Centro Hospitalar de Entre-o-Douro e Vouga, Centro Hospitalar de Trás-os-Montes e Alto Douro, Hospital da Senhora da Oliveira, Hospital CUF Porto, Centro Hospitalar de Vila Nova de Gaia/Espinho, Centro Hospitalar Universitário de Coimbra.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to thank Evidenze Portugal for their support in medical writing.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bloechl-Daum, B.; Deuson, R.R.; Mavros, P.; Hansen, M.; Herrstedt, J. Delayed nausea and vomiting continue to reduce patients’ quality of life after highly and moderately emetogenic chemotherapy despite antiemetic treatment. J. Clin. Oncol. 2006, 24, 4472–4478. [Google Scholar] [CrossRef] [PubMed]
- Sommariva, S.; Pongiglione, B.; Tarricone, R. Impact of chemotherapy-induced nausea and vomiting on health-related quality of life and resource utilization: A systematic review. Crit. Rev. Oncol. Hematol. 2016, 99, 13–36. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.; Morrow, G.R.; Roscoe, J.A.; Hickok, J.T.; Mustian, K.M.; Moore, D.F.; Wade, J.L.; Fitch, T.R. Cancer patients’ expectations of experiencing treatment-related side effects: A University of Rochester Cancer Center--Community Clinical Oncology Program study of 938 patients from community practices. Cancer 2004, 101, 851–857. [Google Scholar] [CrossRef]
- Neymark, N.; Crott, R. Impact of emesis on clinical and economic outcomes of cancer therapy with highly emetogenic chemotherapy regimens: A retrospective analysis of three clinical trials. Support Care Cancer 2005, 13, 812–818. [Google Scholar] [CrossRef] [PubMed]
- Aapro, M.; Molassiotis, A.; Dicato, M.; Pelaez, I.; Rodriguez-Lescure, A.; Pastorelli, D.; Ma, L.; Burke, T.; Gu, A.; Gascon, P.; et al. The effect of guideline-consistent antiemetic therapy on chemotherapy-induced nausea and vomiting (CINV): The Pan European Emesis Registry (PEER). Ann. Oncol. 2012, 23, 1986–1992. [Google Scholar] [CrossRef] [PubMed]
- From the American Association of Neurological Surgeons (AANS); American Society of Neuroradiology (ASNR); Cardiovascular and Interventional Radiology Society of Europe (CIRSE); Canadian Interventional Radiology Association (CIRA); Congress of Neurological Surgeons (CNS); European Society of Minimally Invasive Neurological Therapy (ESMINT); European Society of Neuroradiology (ESNR); European Stroke Organization (ESO); Society for Cardiovascular Angiography and Interventions (SCAI); Society of Interventional Radiology (SIR); et al. Multisociety Consensus Quality Improvement Revised Consensus Statement for Endovascular Therapy of Acute Ischemic Stroke. Int. J. Stroke 2018, 13, 612–632. [Google Scholar] [CrossRef]
- Dinis, J.; Wisniewski, T.; Moreira, A.; Raposo, J.; Ma, L.; Burke, T. Chemotherapy-induced nausea and vomiting in Portugal: Incidence versus healthcare provider estimations and effect on quality of life. Therapy 2009, 6, 595–602. [Google Scholar] [CrossRef]
- Lindley, C.M.; Hirsch, J.D.; O’Neill, C.V.; Transau, M.C.; Gilbert, C.S.; Osterhaus, J.T. Quality of life consequences of chemotherapy-induced emesis. Qual Life Res. 1992, 1, 331–340. [Google Scholar] [CrossRef]
- Razvi, Y.; Chan, S.; McFarlane, T.; McKenzie, E.; Zaki, P.; DeAngelis, C.; Pidduck, W.; Bushehri, A.; Chow, E.; Jerzak, K.J. ASCO, NCCN, MASCC/ESMO: A comparison of antiemetic guidelines for the treatment of chemotherapy-induced nausea and vomiting in adult patients. Support Care Cancer 2019, 27, 87–95. [Google Scholar] [CrossRef]
- Basch, E.; Hesketh, P.J.; Kris, M.G.; Prestrud, A.A.; Temin, S.; Lyman, G.H. Antiemetics: American society of clinical oncology clinical practice guideline update. J. Oncol. Pract. 2011, 7, 395–398. [Google Scholar] [CrossRef]
- Berger, M.J.; Ettinger, D.S.; Aston, J.; Barbour, S.; Bergsbaken, J.; Bierman, P.J.; Brandt, D.; Dolan, D.E.; Ellis, G.; Kim, E.J.; et al. NCCN Guidelines Insights: Antiemesis, Version 2.2017. J. Natl. Compr. Cancer Netw. 2017, 15, 883–893. [Google Scholar] [CrossRef] [PubMed]
- Hesketh, P.J.; Kris, M.G.; Basch, E.; Bohlke, K.; Barbour, S.Y.; Clark-Snow, R.A.; Danso, M.A.; Dennis, K.; Dupuis, L.L.; Dusetzina, S.B.; et al. Antiemetics: ASCO Guideline Update. J. Clin. Oncol. 2020, 38, 2782–2797. [Google Scholar] [CrossRef]
- Natale, J.J. Overview of the prevention and management of CINV. Am. J. Manag. Care 2018, 24 (Suppl. S18), S391–S397. [Google Scholar] [PubMed]
- Roila, F.; Warr, D.; Hesketh, P.J.; Gralla, R.; Herrstedt, J.; Jordan, K.; Aapro, M.; Ballatori, E.; Rapoport, B. 2016 updated MASCC/ESMO consensus recommendations: Prevention of nausea and vomiting following moderately emetogenic chemotherapy. Support Care Cancer 2017, 25, 289–294. [Google Scholar] [CrossRef]
- Navari, R.M.; Aapro, M. Antiemetic Prophylaxis for Chemotherapy-Induced Nausea and Vomiting. N. Engl. J. Med. 2016, 374, 1356–1367. [Google Scholar] [CrossRef]
- Aapro, M. CINV: Still troubling patients after all these years. Support Care Cancer 2018, 26 (Suppl. S1), 5–9. [Google Scholar] [CrossRef] [Green Version]
- Foubert, J.; Vaessen, G. Nausea: The neglected symptom? Eur. J. Oncol. Nurs. 2005, 9, 21–32. [Google Scholar] [CrossRef]
- Ballatori, E.; Roila, F. Impact of nausea and vomiting on quality of life in cancer patients during chemotherapy. Health Qual. Life Outcomes 2003, 1, 46. [Google Scholar] [CrossRef] [Green Version]
- Ng, T.L.; Hutton, B.; Clemons, M. Chemotherapy-Induced Nausea and Vomiting: Time for More Emphasis on Nausea? Oncologist 2015, 20, 576–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Einhorn, L.H.; Rapoport, B.; Navari, R.M.; Herrstedt, J.; Brames, M.J. 2016 updated MASCC/ESMO consensus recommendations: Prevention of nausea and vomiting following multiple-day chemotherapy, high-dose chemotherapy, and breakthrough nausea and vomiting. Support Care Cancer 2017, 25, 303–308. [Google Scholar] [CrossRef]
- Escobar, Y.; Cajaraville, G.; Virizuela, J.A.; Alvarez, R.; Munoz, A.; Olariaga, O.; Tames, M.J.; Muros, B.; Lecumberri, M.J.; Feliu, J.; et al. Incidence of chemotherapy-induced nausea and vomiting with moderately emetogenic chemotherapy: ADVICE (Actual Data of Vomiting Incidence by Chemotherapy Evaluation) study. Support Care Cancer 2015, 23, 2833–2840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aapro, M.; Ruffo, P.; Panteri, R.; Costa, S.; Piovesana, V. Oncologist perspectives on chemotherapy-induced nausea and vomiting (CINV) management and outcomes: A quantitative market research-based survey. Cancer Rep. (Hoboken) 2018, 1, e1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dielenseger, P.; Borjeson, S.; Vidall, C.; Young, A.; Jahn, P. Evaluation of antiemetic practices for prevention of chemotherapy-induced nausea and vomiting (CINV): Results of a European oncology nurse survey. Support Care Cancer 2019, 27, 4099–4106. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 

{kind=link}