Outcomes of Patients with Metastatic Castration-Resistant Prostate Cancer According to Somatic Damage DNA Repair Gene Alterations

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
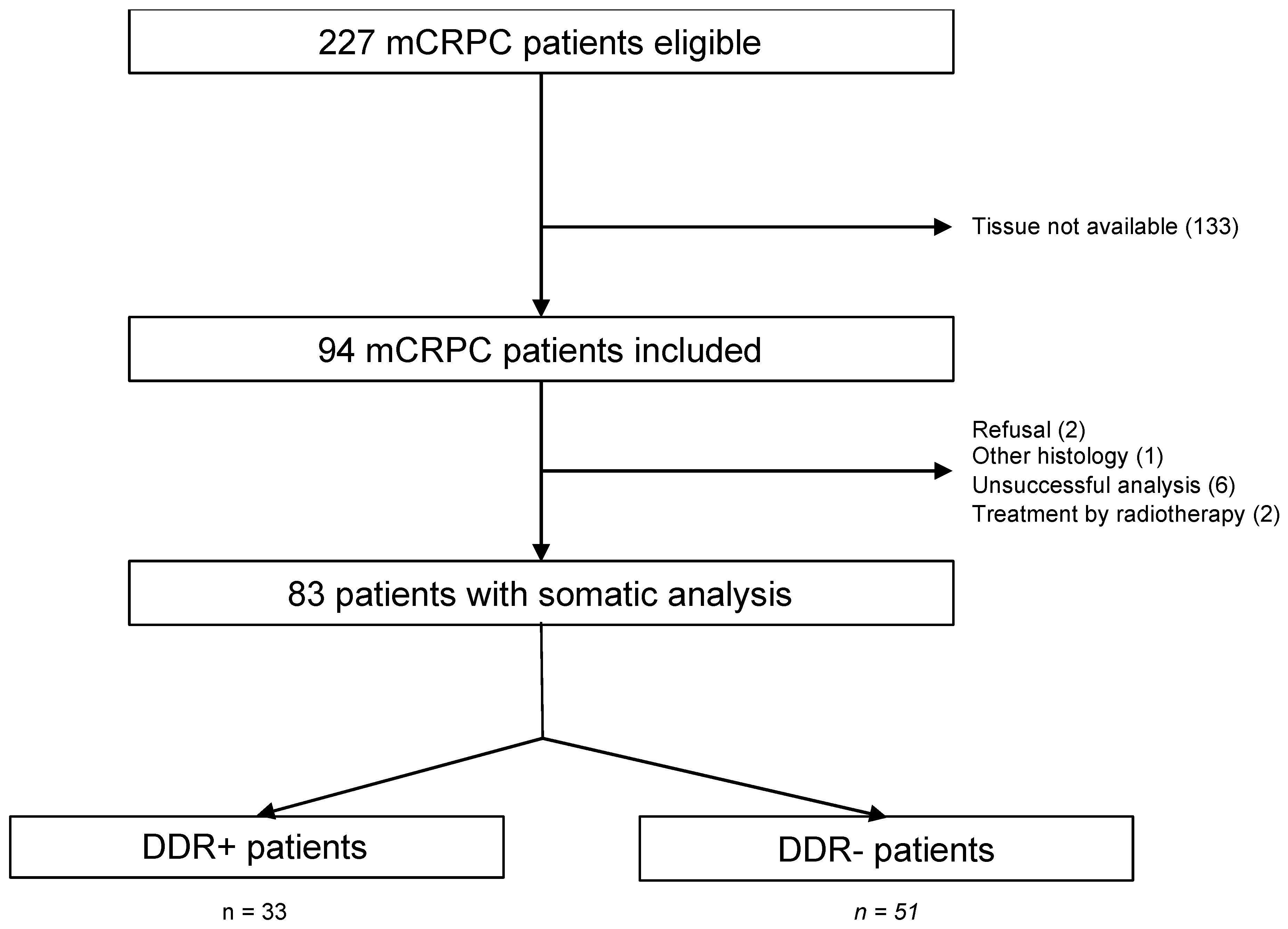
3.1. Patient Selection
3.2. Clinical Characteristics
3.3. Molecular Characteristics of Tumors
3.4. PFS
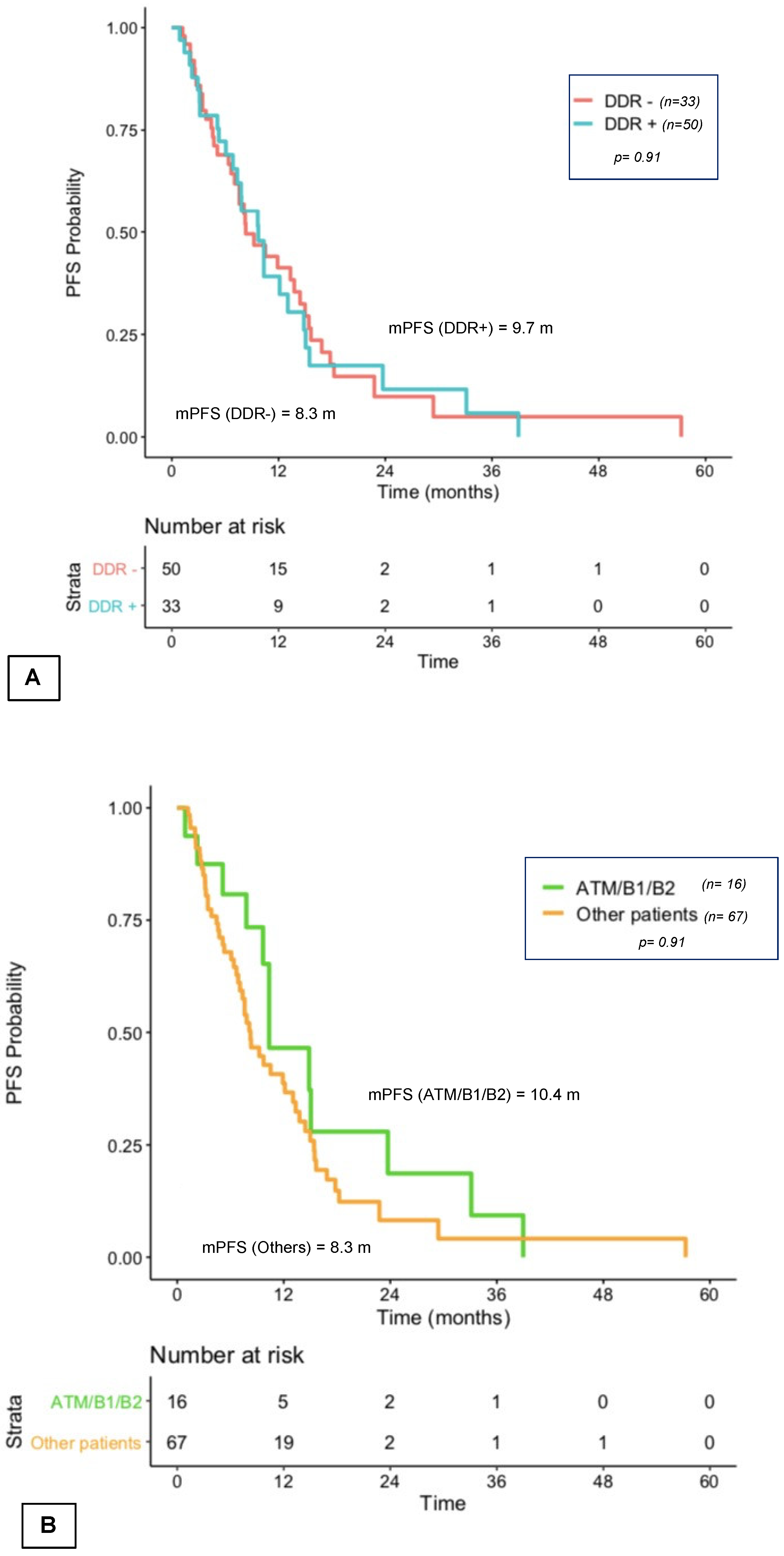
3.4.1. First-Line PFS
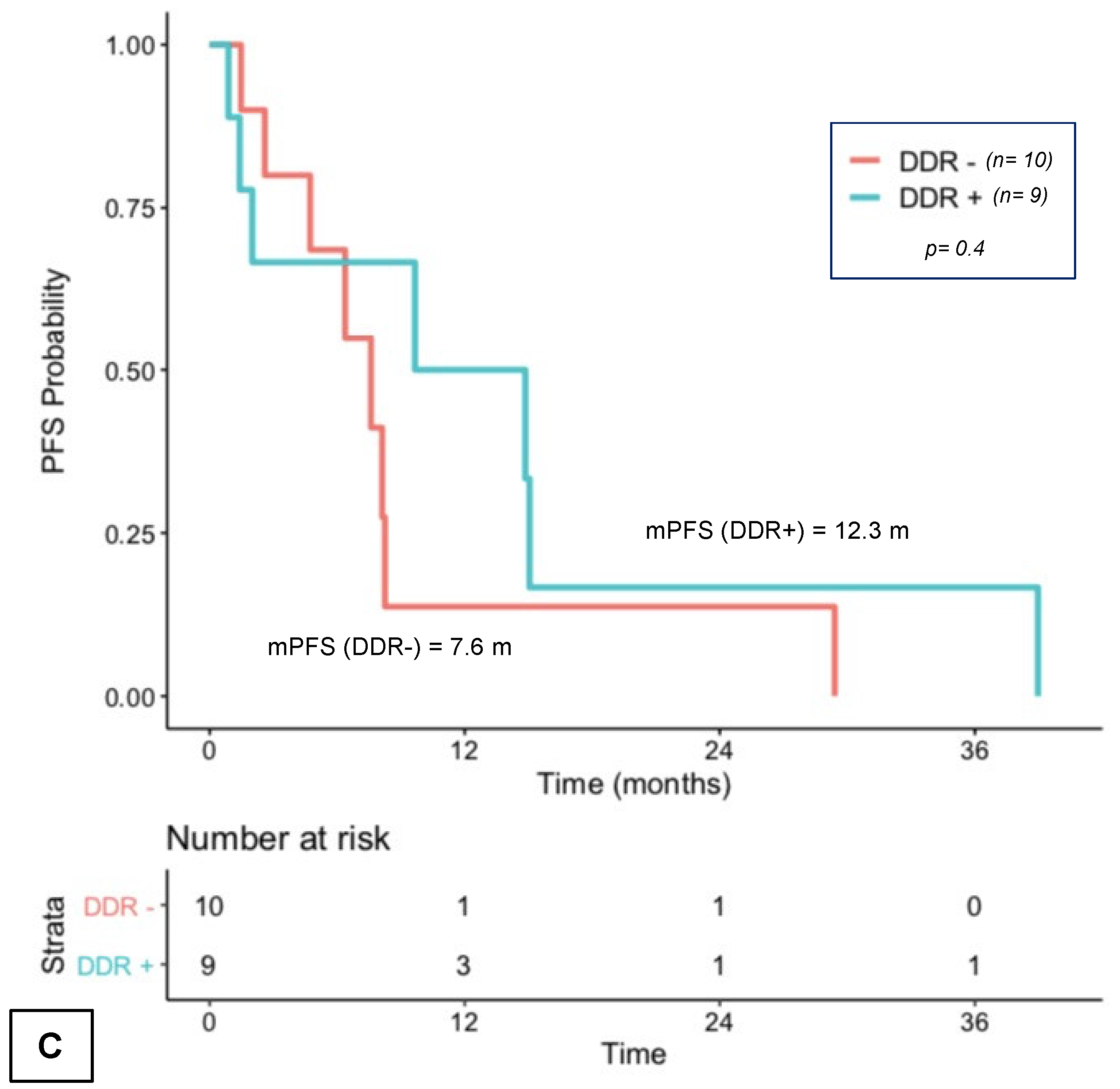
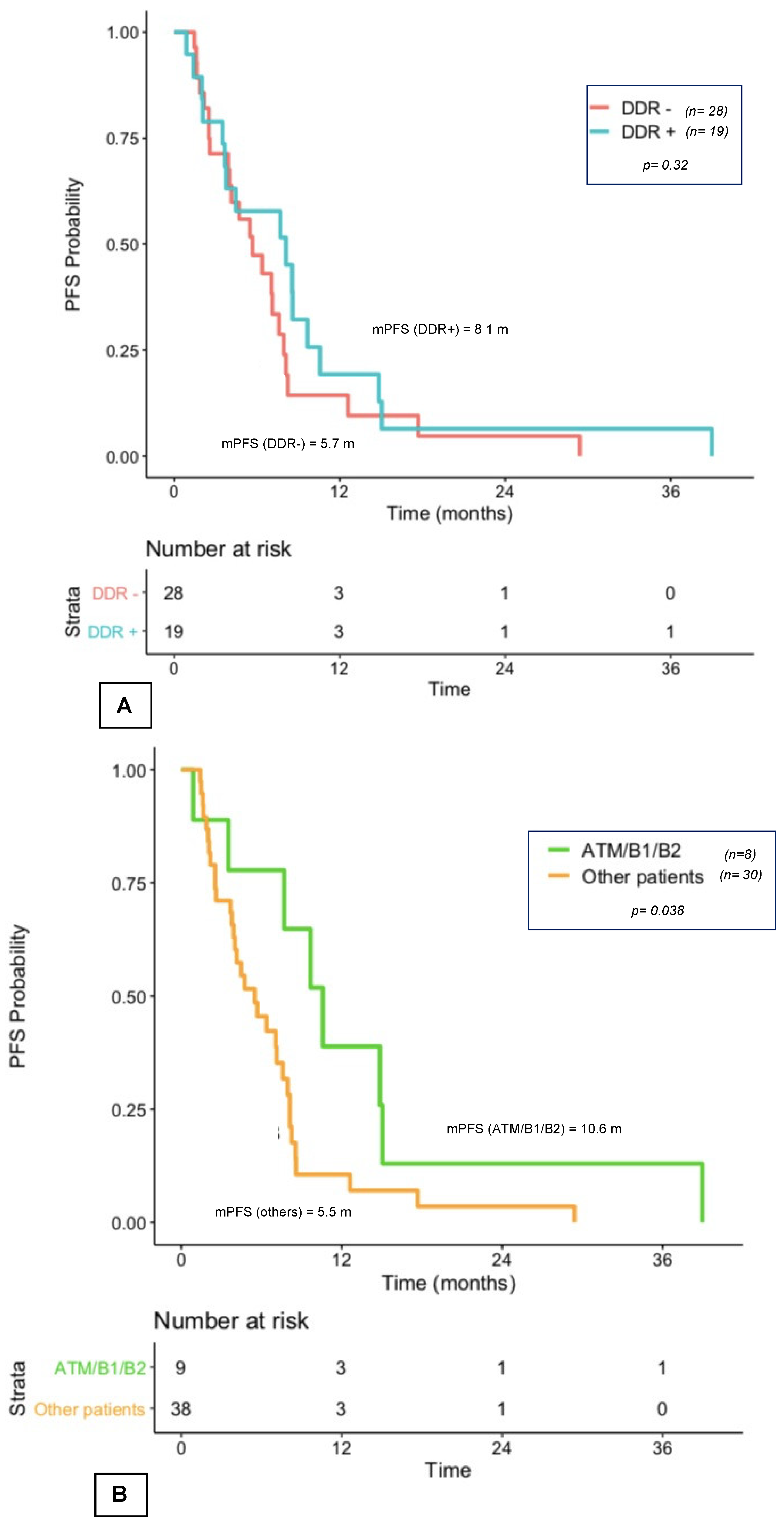
3.4.2. PFS with First Exposure to Taxanes and NHT
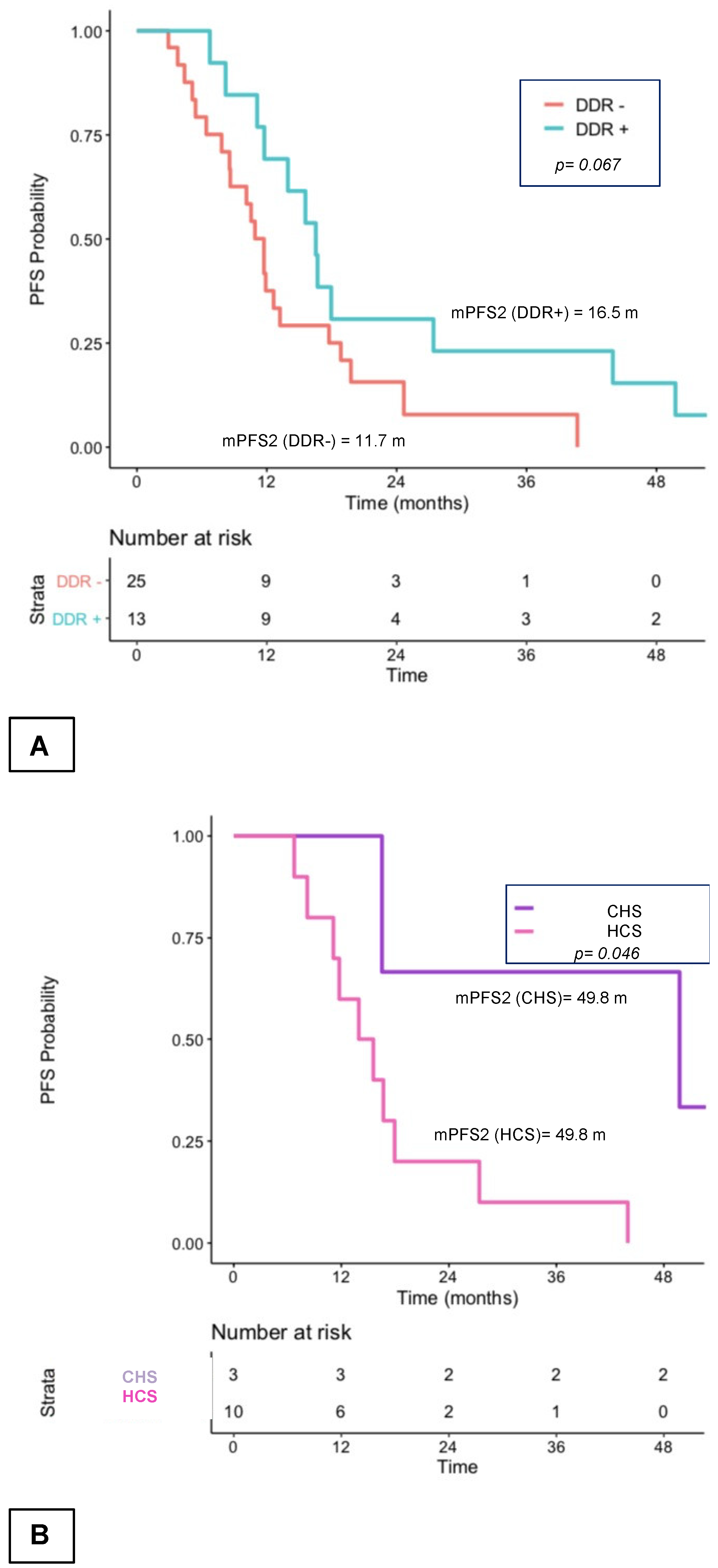
3.5. PFS2
3.6. Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robinson, D.; Van Allen, E.M.; Wu, Y.-M.; Schultz, N.; Lonigro, R.J.; Mosquera, J.-M.; Montgomery, B.; Taplin, M.-E.; Pritchard, C.C.; Attard, G.; et al. Integrative Clinical Genomics of Advanced Prostate Cancer. Cell 2015, 161, 1215–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- TCGA Identifies Subtypes of Prostate Cancer. The Cancer Genome Atlas—National Cancer Institute. Available online: https://cancergenome.nih.gov/newsevents/newsannouncements/PRAD_2015 (accessed on 6 March 2017).
- Jonsson, P.; Bandlamudi, C.; Cheng, M.L.; Srinivasan, P.; Chavan, S.S.; Friedman, N.D.; Rosen, E.Y.; Richards, A.L.; Bouvier, N.; Selcuklu, S.D.; et al. Tumour lineage shapes BRCA-mediated phenotypes. Nature 2019, 571, 576–579. [Google Scholar] [CrossRef] [PubMed]
- Castro, E.; Romero-Laorden, N.; Del Pozo, A.; Lozano, R.; Medina, A.; Puente, J.; Piulats, J.M.; Lorente, D.; Saez, M.I.; Morales-Barrera, R.; et al. PROREPAIR-B: A Prospective Cohort Study of the Impact of Germline DNA Repair Mutations on the Outcomes of Patients with Metastatic Castration-Resistant Prostate Cancer. J. Clin. Oncol. 2019, 37, 490–503. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, C.C.; Mateo, J.; Walsh, M.F.; De Sarkar, N.; Abida, W.; Beltran, H.; Garofalo, A.; Gulati, R.; Carreira, S.; Eeles, R.; et al. Inherited DNA-Repair Gene Mutations in Men with Metastatic Prostate Cancer. N. Engl. J. Med. 2016, 375, 443–453. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network. The Molecular Taxonomy of Primary Prostate Cancer. Cell 2015, 163, 1011–1025. [Google Scholar] [CrossRef] [Green Version]
- Mateo, J.; Carreira, S.; Sandhu, S.; Miranda, S.; Mossop, H.; Perez-Lopez, R.; Nava Rodrigues, D.; Robinson, D.; Omlin, A.; Tunariu, N.; et al. DNA-Repair Defects and Olaparib in Metastatic Prostate Cancer. N. Engl. J. Med. 2015, 373, 1697–1708. [Google Scholar] [CrossRef]
- Armenia, J.; Wankowicz, S.A.M.; Liu, D.; Gao, J.; Kundra, R.; Reznik, E.; Chatila, W.K.; Chakravarty, D.; Han, G.C.; Coleman, I.; et al. The long tail of oncogenic drivers in prostate cancer. Nat. Genet. 2018, 50, 645–651. [Google Scholar] [CrossRef]
- Annala, M.; Struss, W.J.; Warner, E.W.; Beja, K.; Vandekerkhove, G.; Wong, A.; Khalaf, D.; Seppälä, I.-L.; So, A.; Lo, G.; et al. Treatment Outcomes and Tumor Loss of Heterozygosity in Germline DNA Repair-deficient Prostate Cancer. Eur. Urol. 2017, 72, 34–42. [Google Scholar] [CrossRef]
- Grasso, C.S.; Wu, Y.-M.; Robinson, D.R.; Cao, X.; Dhanasekaran, S.M.; Khan, A.P.; Quist, M.J.; Jing, X.; Lonigro, R.J.; Brenner, J.C.; et al. The mutational landscape of lethal castration-resistant prostate cancer. Nature 2012, 487, 239–243. [Google Scholar] [CrossRef] [Green Version]
- Mateo, J.; Cheng, H.H.; Beltran, H.; Dolling, D.; Xu, W.; Pritchard, C.C.; Mossop, H.; Rescigno, P.; Perez-Lopez, R.; Sailer, V.; et al. Clinical Outcome of Prostate Cancer Patients with Germline DNA Repair Mutations: Retrospective Analysis from an International Study. Eur. Urol. 2018, 73, 687–693. [Google Scholar] [CrossRef] [Green Version]
- Wei, Y.; Wu, J.; Gu, W.; Qin, X.; Dai, B.; Lin, G.; Gan, H.; Freedland, S.J.; Zhu, Y.; Ye, D. Germline DNA Repair Gene Mutation Landscape in Chinese Prostate Cancer Patients. Eur. Urol. 2019, 76, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Castro, E.; Goh, C.; Olmos, D.; Saunders, E.; Leongamornlert, D.; Tymrakiewicz, M.; Mahmud, N.; Dadaev, T.; Govindasami, K.; Guy, M.; et al. Germline BRCA Mutations Are Associated with Higher Risk of Nodal Involvement, Distant Metastasis, and Poor Survival Outcomes in Prostate Cancer. J. Clin. Oncol. 2013, 31, 1748–1757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro, E.; Goh, C.; Leongamornlert, D.; Saunders, E.; Tymrakiewicz, M.; Dadaev, T.; Govindasami, K.; Guy, M.; Ellis, S.; Frost, D.; et al. Effect of BRCA Mutations on Metastatic Relapse and Cause-specific Survival After Radical Treatment for Localised Prostate Cancer. Eur. Urol. 2015, 68, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, D.J.; Gaudet, M.M.; Pal, P.; Kirchhoff, T.; Balistreri, L.; Vora, K.; Bhatia, J.; Stadler, Z.; Fine, S.W.; Reuter, V.; et al. Germline BRCA mutations denote a clinicopathologic subset of prostate cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2010, 16, 2115–2121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, D.J.; Cronin, A.M.; Milowsky, M.I.; Morris, M.J.; Bhatia, J.; Scardino, P.T.; Eastham, J.A.; Offit, K.; Robson, M.E. Germline BRCA mutation does not prevent response to taxane-based therapy for the treatment of castration-resistant prostate cancer. Br. J. Urol. 2011, 109, 713–719. [Google Scholar] [CrossRef] [Green Version]
- Hussain, M.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.D.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Phase III PROfound Study Evaluates Olaparib in Setting of mCRPC—The ASCO Post. 2019. Available online: https://oncologypro.esmo.org/meeting-resources/esmo-2019-congress/PROfound-Phase-3-study-of-olaparib-versus-enzalutamide-or-abiraterone-for-metastatic-castration-resistant-prostate-cancer-mCRPC-with-homologous-recombination-repair-HRR-gene-alterations (accessed on 11 March 2020).
- Marshall, C.H.; Sokolova, A.O.; McNatty, A.L.; Cheng, H.H.; Eisenberger, M.A.; Bryce, A.H.; Schweizer, M.T.; Antonarakis, E.S. Differential Response to Olaparib Treatment Among Men with Metastatic Castration-resistant Prostate Cancer Harboring BRCA1 or BRCA2 Versus ATM Mutations. Eur. Urol. 2019, 76, 452–458. [Google Scholar] [CrossRef] [Green Version]
- TRITON2: An International, Multicenter, Open-Label, Phase II Study of the Parp Inhibitor Rucaparib in Patients with Metastatic Castration-Resistant Prostate Cancer (mCRPC) Associated with Homologous Recombination Deficiency (HRD). J. Clin. Oncol. 2018, 36.
- Clarke, N.; Wiechno, P.; Alekseev, B.; Sala, N.; Jones, R.; Kocak, I.; Chiuri, V.E.; Jassem, J.; Flechon, A.; Redferm, C.; et al. Olaparib combined with abiraterone in patients with metastatic castration-resistant prostate cancer: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 2018, 19, 975–986. [Google Scholar] [CrossRef]
- Mateo, J.; Porta, N.; Bianchini, D.; McGovern, U.; Elliott, T.; Jones, R.; Syndikus, I.; Ralph, C.; Jain, S.; Varughese, M.; et al. Olaparib in patients with metastatic castration-resistant prostate cancer with DNA repair gene aberrations (TOPARP-B): A multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2020, 21, 162–174. [Google Scholar] [CrossRef]
- Antonarakis, E.S.; Lu, C.; Luber, B.; Liang, C.; Wang, H.; Chen, Y.; Silberstein, J.L.; Piana, D.; Lai, Z.; Chen, Y.; et al. Germline DNA-repair Gene Mutations and Outcomes in Men with Metastatic Castration-resistant Prostate Cancer Receiving First-line Abiraterone and Enzalutamide. Eur. Urol. 2018, 74, 218–225. [Google Scholar] [CrossRef]
- Annala, M.; Vandekerkhove, G.; Khalaf, D.; Taavitsainen, S.; Beja, K.; Warner, E.W.; Sunderland, K.; Kollmannsberger, C.; Eigl, B.J.; Finch, D.; et al. Circulating Tumor DNA Genomics Correlate with Resistance to Abiraterone and Enzalutamide in Prostate Cancer. Cancer Discov. 2018, 8, 444–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nientiedt, C.; Heller, M.; Endris, V.; Volckmar, A.-L.; Zschäbitz, S.; Tapia-Laliena, M.A.; Duensing, A.; Jäger, D.; Schirmacher, P.; Sültmann, H.; et al. Mutations in BRCA2 and taxane resistance in prostate cancer. Sci. Rep. 2017, 7, 4574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, M.; Daignault-Newton, S.; Twardowski, P.W.; Albany, C.; Stein, M.N.; Kunju, L.P.; Siddiqui, J.; Wu, Y.-M.; Robinson, D.; Lonigro, R.J.; et al. Targeting Androgen Receptor and DNA Repair in Metastatic Castration-Resistant Prostate Cancer: Results From NCI 9012. J. Clin. Oncol. 2018, 36, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Pennington, K.P.; Walsh, T.; Harrell, M.I.; Lee, M.K.; Pennil, C.C.; Rendi, M.H.; Thornton, A.; Norquist, B.M.; Casadei, S.; Nord, A.S.; et al. Germline and Somatic Mutations in Homologous Recombination Genes Predict Platinum Response and Survival in Ovarian, Fallopian Tube, and Peritoneal Carcinomas. Clin. Cancer Res. 2014, 20, 764–775. [Google Scholar] [CrossRef] [Green Version]
- Abida, W.; Campbell, D.; Patnaik, A.; Shapiro, J.D.; Sautois, B.; Vogelzang, N.J.; Voog, E.G.; Bryce, A.H.; McDermott, R.; Ricci, F.; et al. Non-BRCA DNA Damage Repair Gene Alterations and Response to the PARP Inhibitor Rucaparib in Metastatic Castration-Resistant Prostate Cancer: Analysis From the Phase II TRITON2 Study. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2020, 26, 2487–2496. [Google Scholar] [CrossRef] [Green Version]
- Horwich, A.; Hugosson, J.; de Reijke, T.; Wiegel, T.; Fizazi, K.; Kataja, V.; Parker, C.; Bellmunt, J.; Berthold, D.; Bill-Axelson, A.; et al. Prostate cancer: ESMO Consensus Conference Guidelines 2012. Ann. Oncol. 2013, 24, 1141–1162. [Google Scholar] [CrossRef]
- Rozet, F.; Hennequin, C.; Beauval, J.-B.; Beuzeboc, P.; Cormier, L.; Fromont-Hankard, G.; Mongiat-Artus, P.; Ploussard, G.; Mathieu, R.; Brureau, L.; et al. French ccAFU guidelines—Update 2018-2020: Prostate cancer. Progres. En. Urol. J. Assoc. Fr. Urol. Soc. Fr. Urol. 2018, 28 (Suppl. S1), R81–R132. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | DDR+ | DDR− | p | ||||
|---|---|---|---|---|---|---|---|
| Age(years) | 69.5 | (23–82) | 70 | (65–76) | 69.5 | (55–82) | 0.43 |
| ECOG | 0.21 | ||||||
| 0 | 34 | (44%) | 15 | (48%) | 19 | (41%) | |
| 1 | 38 | (49%) | 12 | (39%) | 26 | (55%) | NA |
| 2 | 6 | (8%) | 4 | (13%) | 2 | (4%) | NA |
| BMI | 27.5 | (23–38) | 27.5 | (25–31) | 27.5 | (23–36) | 0.71 |
| Previous Treatments | |||||||
| Surgery | 22 | (27%) | 10 | (30%) | 12 | (24%) | 0.74 |
| Chemotherapy | 14 | (17%) | 6 | (18%) | 8 | (16%) | 1 |
| Radiotherapy | 45 | (54%) | 19 | (58%) | 26 | (52%) | 0.8 |
| First-line Treatment | 0.61 | ||||||
| NHT | 64 | (77%) | 14 | (73%) | 40 | (80%) | |
| Taxanes | 19 | (23%) | 9 | (27%) | 10 | (20%) | NA |
| Gleason | 0.47 | ||||||
| 5 to 7 | 35 | (43%) | 12 | (36%) | 23 | (47%) | |
| 8 to 10 | 47 | (57%) | 21 | (67%) | 26 | (53%) | NA |
| TNM | 0.85 | ||||||
| T1/2 | 42 | (51%) | 7 | (21%) | 14 | (28%) | |
| T3/4 | 41 | (49%) | 22 | (67%) | 30 | (60%) | NA |
| Tx | 10 | (12%) | 4 | (12%) | 6 | (12%) | |
| N1+ | 25 | (30%) | 8 | (24%) | 17 | (34%) | 0.55 |
| N0 | 16 | (19%) | 6 | (18%) | 10 | (20%) | NA |
| Nx | 42 | (51%) | 19 | (58%) | 23 | (46%) | NA |
| M1 | 43 | (52%) | 15 | (46%) | 28 | (56%) | 0.47 |
| M0/Mx | 40 | (48%) | 18 | (54%) | 22 | (44%) | NA |
| Initial Pas | 28.8 | (1–5500) | 28.8 | (9.7–60) | 27.6 | (10–232) | 0.32 |
| Diagnostic Modes | 0.73 | ||||||
| Symptoms | 49 | (62%) | 18 | (58%) | 31 | (65%) | |
| Individual screening | 30 | (38%) | 13 | (42%) | 17 | (35%) | NA |
| Durtion of Hormonosensitivity (years) | 2.07 | (0.4–18.1) | 2.14 | (0.5–18.1) | 1.92 | (0.4–13.9) | 0.5 |
| Time Before Metastasis (years) | 0.04 | (0–13.8) | 0.92 | (0–13.8) | 0.02 | (0–12.1) | 0.07 |
| Patient | Gene | Alteration | Protein | Function | Types |
|---|---|---|---|---|---|
| 1 | ATM | 5188C > T | ARG1730* | stop | Pathogenic |
| 2 | CDK12 | 2068DEL | ALA690GLNFS*63 | frameshift | Pathogenic |
| 2 | CDK12 | 3046C > T | GLN1016* | stop | Pathogenic |
| 8 | ATM | 4403T > A | VAL1468ASP | missense | Pathogenic |
| 9 | firefox | 1100DEL | THR307METFS*15 | frameshift | Pathogenic |
| 14 | BRCA1 | 3741DEL | ALA1248LEUFS*16 | frameshift | Pathogenic |
| 15 | MRE11A | 571C > T | ARG191* | stop | Pathogenic |
| 16 | ATM | 5712DUP | SER1905ILEFS*25 | frameshift | Pathogenic |
| 17 | BRCA2 | - | - | - | Pathogenic |
| 18 | CDK12 | 3566_3575DEL | LEU1189GLNFS*23 | frameshift | Pathogenic |
| 19 | PALB2 | 658_659DEL | SER220CYSFS*14 | frameshift | Pathogenic |
| 25 | BRCA2 | 5909C > A | SER1970* | stop | Pathogenic |
| 27 | CHEK2 | 1100DEL | THR367METFS*15 | frameshift | Pathogenic |
| 28 | MDC1 | 907DEL | VAL303TRPFS*45 | frameshift | Pathogenic |
| 30 | ATM | 9022C > T | ARG3008CYS | missense | Pathogenic |
| 30 | ATM | 8096C > T | PRO2699LEU | missense | Pathogenic |
| 34 | ATM | 5293_5302DEL | GLN1765GLUFS*8 | frameshift | Pathogenic |
| 38 | ATM | 8759_8772DEL | ILE2920ARGFS18* | frameshift | Pathogenic |
| 39 | BLM | 1701G > A | TRP567* | stop | Pathogenic |
| 40 | CHEK2 | - | TYR370CYS | missense | Pathogenic |
| 51 | CHEK1 | 783DEL | ASP262ILEFS*42 | frameshift | Pathogenic |
| 53 | FANCM | 1827T > G | TYR609* | stop | Pathogenic |
| 53 | CDK12 | 467_470DEL | GLU156GLYFS*10 | frameshift | Pathogenic |
| 54 | FANCG | 1183_1192DEL | GLU375TRPFS* | frameshift | Pathogenic |
| 56 | FANCF | 1087C > T | GLN363* | stop | Pathogenic |
| 59 | ATM | 5818G > T | GLU1940* | stop | Pathogenic |
| 60 | BRCA2 | 1597DEL | THR533LEUFS*25 | frameshift | Pathogenic |
| 62 | MRE11A | 1331_1332DEL | VAL444ALAFS*2 | frameshift | Pathogenic |
| 63 | BRCA2 | C.1813DEL | ILE605TYRFS*9 | frameshift | Pathogenic |
| 68 | FANCG | 572T > G | LEU191* | stop | Pathogenic |
| 75 | ATM | 7306A > G | ARG2436GLY | missense | Pathogenic |
| 76 | BRCA2 | 5073DUP | TRP1692METFS*3 | frameshift | Pathogenic |
| 76 | FANCI | 3184C > T | GLN1082* | stop | Pathogenic |
| 76 | FANCG | 1143G > C | ARG381SER | missense | Likely pathogenic |
| 76 | BRCA2 | 7307DEL | ASN2436THRFS*33 | frameshift | Pathogenic |
| 78 | ATM | 901G > A | GLY301SER | faux sens | Pathogenic |
| 81 | ATM | 7031G > A | TRP2344* | stop | Likely pathogenic |
| 81 | SMARCA2 | 4369C > T | ARG1457CYS | missense | Pathogenic |
| 82 | PALB2 | 2850DEL | SER951LEUFS*11 | frameshift | Pathogenic |
| 83 | CHEK2 | 1116_1117DEINSTG | LYS373GLU | missense | Pathogenic |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neviere, Z.; Coquan, E.; Brachet, P.-E.; Meriaux, E.; Bonnet, I.; Krieger, S.; Castéra, L.; Vaur, D.; Boulouard, F.; Leconte, A.; et al. Outcomes of Patients with Metastatic Castration-Resistant Prostate Cancer According to Somatic Damage DNA Repair Gene Alterations. Curr. Oncol. 2022, 29, 2776-2791. https://doi.org/10.3390/curroncol29040226
Neviere Z, Coquan E, Brachet P-E, Meriaux E, Bonnet I, Krieger S, Castéra L, Vaur D, Boulouard F, Leconte A, et al. Outcomes of Patients with Metastatic Castration-Resistant Prostate Cancer According to Somatic Damage DNA Repair Gene Alterations. Current Oncology. 2022; 29(4):2776-2791. https://doi.org/10.3390/curroncol29040226
Chicago/Turabian StyleNeviere, Zoé, Elodie Coquan, Pierre-Emmanuel Brachet, Emeline Meriaux, Isabelle Bonnet, Sophie Krieger, Laurent Castéra, Dominique Vaur, Flavie Boulouard, Alexandra Leconte, and et al. 2022. "Outcomes of Patients with Metastatic Castration-Resistant Prostate Cancer According to Somatic Damage DNA Repair Gene Alterations" Current Oncology 29, no. 4: 2776-2791. https://doi.org/10.3390/curroncol29040226