Prospective Randomized Phase II Study of Stereotactic Body Radiotherapy (SBRT) vs. Conventional Fractionated Radiotherapy (CFRT) for Chinese Patients with Early-Stage Localized Prostate Cancer †

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Demographic Characteristics
2.2. Treatments Received
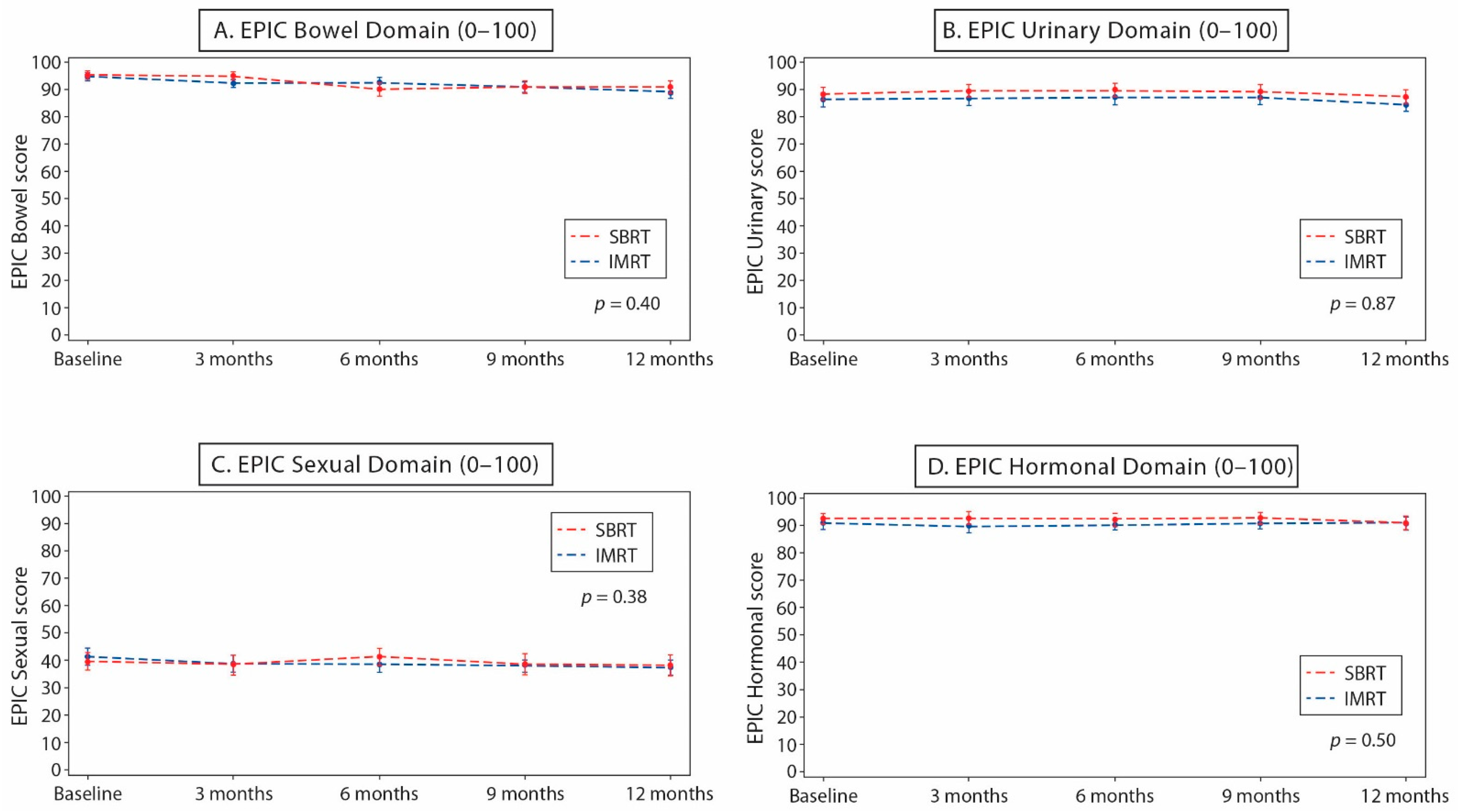
2.3. PRQOL
2.4. Acute and Late Toxicities
2.5. Disease Control
3. Discussion
4. Materials and Methods
4.1. Trial Design
4.2. Study Patients
4.3. Treatments
4.4. Patient Assessments
4.5. Study Endpoints
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Mason, M.; Metcalfe, C.; Holding, P.; Davis, M.; Peters, T.J.; Turner, E.L.; Martin, R.M.; et al. 10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer. N. Engl. J. Med. 2016, 375, 1415–1424. [Google Scholar] [CrossRef] [Green Version]
- Swisher-McClure, S.; Mitra, N.; Woo, K.; Smaldone, M.; Uzzo, R.; Bekelman, J.E. Increasing use of dose-escalated external beam radiation therapy for men with nonmetastatic prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 103–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, P.L.; Gu, X.; Lipsitz, S.R.; Choueiri, T.K.; Choi, W.W.; Lei, Y.; Hoffman, K.E.; Hu, J.C. Cost implications of the rapid adoption of newer technologies for treating prostate cancer. J. Clin. Oncol. 2011, 29, 1517–1524. [Google Scholar] [CrossRef] [Green Version]
- Barton, M.B.; Jacob, S.; Shafiq, J.; Wong, K.; Thompson, S.R.; Hanna, T.P.; Delaney, G.P. Estimating the demand for radiotherapy from the evidence: A review of changes from 2003 to 2012. Radiother Oncol. 2014, 112, 140–144. [Google Scholar] [CrossRef]
- Delaney, G.; Jacob, S.; Barton, M. Estimating the optimal external-beam radiotherapy utilization rate for genitourinary malignancies. Cancer 2005, 103, 462–473. [Google Scholar] [CrossRef]
- Gustavsen, G.; Gullet, L.; Cole, D.; Lewine, N.; Bishoff, J.T. Economic burden of illness associated with localized prostate cancer in the United States. Future Oncol. 2020, 16, 4265–4277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, M.; Gouveia, A.G.; Cury, F.L.; Moideen, N.; Bratti, V.F.; Patrocinio, H.; Berlin, A.; Mendez, L.C.; Moraes, F.Y. Practical considerations for prostate hypofractionation in the developing world. Nat. Rev. Urol. 2021, 18, 669–685. [Google Scholar] [CrossRef]
- McMahon, S.J. The linear quadratic model: Usage, interpretation and challenges. Phys. Med. Biol. 2018, 64, 01TR. [Google Scholar] [CrossRef]
- Miralbell, R.; Roberts, S.A.; Zubizarreta, E.; Hendry, J.H. Dose-fractionation sensitivity of prostate cancer deduced from radiotherapy outcomes of 5, 969 patients in seven international institutional datasets: Alpha/beta = 1.4 (0.9 − 2.2) Gy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e17–e24. [Google Scholar] [CrossRef] [PubMed]
- Vogelius, I.R.; Bentzen, S.M. Meta-analysis of the alpha/beta ratio for prostate cancer in the presence of an overall time factor: Bad news, good news, or no news? Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 89–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dearnaley, D.; Syndikus, I.; Mossop, H.; Khoo, V.; Birtle, A.; Bloomfield, D.; Graham, J.; Kirkbride, P.; Logue, J.; Malik, Z.; et al. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial. Lancet Oncol. 2016, 17, 1047–1060. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.R.; Dignam, J.J.; Amin, M.B.; Bruner, D.W.; Low, D.; Swanson, G.P.; Shah, A.B.; D’Souza, D.P.; Michalski, J.M.; Dayes, I.S.; et al. Randomized Phase III Noninferiority Study Comparing Two Radiotherapy Fractionation Schedules in Patients With Low-Risk Prostate Cancer. J. Clin. Oncol. 2016, 34, 2325–2332. [Google Scholar] [CrossRef] [PubMed]
- Catton, C.N.; Lukka, H.; Gu, C.S.; Martin, J.M.; Supiot, S.; Chung, P.W.M.; Bauman, G.S.; Bahary, J.P.; Ahmed, S.; Cheung, P.; et al. Randomized Trial of a Hypofractionated Radiation Regimen for the Treatment of Localized Prostate Cancer. J. Clin. Oncol. 2017, 35, 1884–1890. [Google Scholar] [CrossRef] [PubMed]
- Arcangeli, G.; Saracino, B.; Arcangeli, S.; Gomellini, S.; Petrongari, M.G.; Sanguineti, G.; Strigari, L. Moderate Hypofractionation in High-Risk, Organ-Confined Prostate Cancer: Final Results of a Phase III Randomized Trial. J. Clin. Oncol. 2017, 35, 1891–1897. [Google Scholar] [CrossRef] [PubMed]
- Morgan, S.C.; Hoffman, K.; Loblaw, D.A.; Buyyounouski, M.K.; Patton, C.; Barocas, D.; Bentzen, S.; Chang, M.; Efstathiou, J.; Greany, P.; et al. Hypofractionated Radiation Therapy for Localized Prostate Cancer: An ASTRO, ASCO, and AUA Evidence-Based Guideline. J. Clin. Oncol. 2018, 36, JCO1801097. [Google Scholar] [CrossRef]
- King, C.R.; Freeman, D.; Kaplan, I.; Fuller, D.; Bolzicco, G.; Collins, S.; Meier, R.; Wang, J.; Kupelian, P.; Steinberg, M.; et al. Stereotactic body radiotherapy for localized prostate cancer: Pooled analysis from a multi-institutional consortium of prospective phase II trials. Radiother Oncol. 2013, 109, 217–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, W.C.; Silva, J.; Hartman, H.E.; Dess, R.T.; Kishan, A.U.; Beeler, W.H.; Gharzai, L.A.; Jaworski, E.M.; Mehra, R.; Hearn, J.W.D.; et al. Stereotactic Body Radiation Therapy for Localized Prostate Cancer: A Systematic Review and Meta-Analysis of Over 6000 Patients Treated On Prospective Studies. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 778–789. [Google Scholar] [CrossRef] [Green Version]
- Lehrer, E.J.; Kishan, A.U.; Yu, J.B.; Trifiletti, D.M.; Showalter, T.N.; Ellis, R.; Zaorsky, N.G. Ultrahypofractionated versus hypofractionated and conventionally fractionated radiation therapy for localized prostate cancer: A systematic review and meta-analysis of phase III randomized trials. Radiother Oncol. 2020, 148, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Widmark, A.; Gunnlaugsson, A.; Beckman, L.; Thellenberg-Karlsson, C.; Hoyer, M.; Lagerlund, M.; Kindblom, J.; Ginman, C.; Johansson, B.; Bjornlinger, K.; et al. Ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the HYPO-RT-PC randomised, non-inferiority, phase 3 trial. Lancet 2019, 394, 385–395. [Google Scholar] [CrossRef]
- Brand, D.H.; Tree, A.C.; Ostler, P.; van der Voet, H.; Loblaw, A.; Chu, W.; Ford, D.; Tolan, S.; Jain, S.; Martin, A.; et al. Intensity-modulated fractionated radiotherapy versus stereotactic body radiotherapy for prostate cancer (PACE-B): Acute toxicity findings from an international, randomised, open-label, phase 3, non-inferiority trial. Lancet Oncol. 2019, 20, 1531–1543. [Google Scholar] [CrossRef]
- Roach, M., 3rd; Hanks, G.; Thames, H., Jr.; Schellhammer, P.; Shipley, W.U.; Sokol, G.H.; Sandler, H. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 965–974. [Google Scholar] [CrossRef]
- Hodges, J.C.; Lotan, Y.; Boike, T.P.; Benton, R.; Barrier, A.; Timmerman, R.D. Cost-effectiveness analysis of stereotactic body radiation therapy versus intensity-modulated radiation therapy: An emerging initial radiation treatment option for organ-confined prostate cancer. J. Oncol. Pract. 2012, 8 (Suppl. 3), e31s–e37s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rammant, E.; Ost, P.; Swimberghe, M.; Vanderstraeten, B.; Lumen, N.; Decaestecker, K.; Bultijnck, R.; De Meerleer, G.; Sarrazyn, C.; Colman, R.; et al. Patient- versus physician-reported outcomes in prostate cancer patients receiving hypofractionated radiotherapy within a randomized controlled trial. Strahlenther Onkol. 2019, 195, 393–401. [Google Scholar] [CrossRef]
- Atkinson, T.M.; Wagner, J.S.; Basch, E. Trustworthiness of Patient-Reported Outcomes in Unblinded Cancer Clinical Trials. JAMA Oncol. 2017, 3, 738–739. [Google Scholar] [CrossRef] [Green Version]
- Roydhouse, J.K.; Fiero, M.H.; Kluetz, P.G. Investigating Potential Bias in Patient-Reported Outcomes in Open-label Cancer Trials. JAMA Oncol. 2019, 5, 457–458. [Google Scholar] [CrossRef]
- Lukka, H.R.; Pugh, S.L.; Bruner, D.W.; Bahary, J.P.; Lawton, C.A.F.; Efstathiou, J.A.; Kudchadker, R.J.; Ponsky, L.E.; Seaward, S.A.; Dayes, I.S.; et al. Patient Reported Outcomes in NRG Oncology RTOG 0938, Evaluating Two Ultrahypofractionated Regimens for Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 287–295. [Google Scholar] [CrossRef] [PubMed]
- King, C.R.; Collins, S.; Fuller, D.; Wang, P.C.; Kupelian, P.; Steinberg, M.; Katz, A. Health-related quality of life after stereotactic body radiation therapy for localized prostate cancer: Results from a multi-institutional consortium of prospective trials. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 939–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, A.T.; Schreiber, D.; Agarwal, M.; Polubarov, A.; Schwartz, D. Impact of the use of an endorectal balloon on rectal dosimetry during stereotactic body radiation therapy for localized prostate cancer. Pract. Radiat. Oncol. 2016, 6, 262–267. [Google Scholar] [CrossRef]
- Wei, J.T.; Dunn, R.L.; Sandler, H.M.; McLaughlin, P.W.; Montie, J.E.; Litwin, M.S.; Nyquist, L.; Sanda, M.G. Comprehensive comparison of health-related quality of life after contemporary therapies for localized prostate cancer. J. Clin. Oncol. 2002, 20, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Payne, H.; Cornford, P. Prostate-specific antigen: An evolving role in diagnosis, monitoring, and treatment evaluation in prostate cancer. Urol. Oncol. 2011, 29, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.K.; Poon, D.M.C.; Ng, A.C.F.; Ho, T.; Singh-Carlson, S.; Joffres, M.; Oshan, G.; Kohli, J.; Kwan, W. Cultural adaptation and validation of the Chinese version of the expanded prostate cancer index composite. Asia Pac. J. Clin. Oncol. 2018, 14 (Suppl. 1), 10–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, G.R.; Sloan, J.A.; Wyrwich, K.W. Interpretation of changes in health-related quality of life: The remarkable universality of half a standard deviation. Med. Care 2003, 41, 582–592. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Characteristics | SBRT (n = 31) | CFRT (n = 33) |
|---|---|---|
| Age | ||
| Mean (SD) | 69.4 (6.0) | 69.0 (6.8) |
| Median (range) | 68 (53–78) | 70 (55–81) |
| Zubrod Performance | ||
| 0 | 30 (96%) | 30 (90%) |
| 1 | 1 (3%) | 3 (10%) |
| Clinical T Stage | ||
| 1a | 1 (3%) | 0 |
| 1c | 16 (51%) | 15 (45%) |
| 2a | 7 (22%) | 10 (30%) |
| 2b | 5 (16%) | 3 (9%) |
| 2c | 2 (6%) | 5 (15%) |
| Gleason Score | ||
| 5 | 3 (9%) | 0 |
| 6 | 16 (51%) | 22 (66%) |
| 7 | 12 (38%) | 11 (33%) |
| PSA | ||
| Mean (SD) | 9.2 (5.0) | 8.6 (5.4) |
| Median (Q1–Q3) | 8.8 (6.0–11.8) | 7.6 (5.8–10.3) |
| NCCN Risk Group | ||
| Low | 16 (51%) | 16 (48%) |
| Intermediate | 15 (48%) | 17 (51%) |
| Domain | SBRT | p-Value | CFRT | p-Value |
|---|---|---|---|---|
| Bowel | ||||
| Patients, no. | 30 | 32 | ||
| Mean (SD) | −4.2 (12.5) | 0.40 ** | −5.8 (9.9) | |
| Median | 0.0 | −1.8 | ||
| >5-point reduction, no (%) † | 12 (40%) | 0.28 * | 15 (46.9%) | 0.08 * |
| Urinary | ||||
| Patients, no. | 30 | 32 | ||
| Mean (SD) | −1.3 (12.9) | 0.87 ** | −2.3 (12.7) | |
| Median | −2.1 | 0.0 | ||
| >2-point reduction, no (%) ‡ | 16 (53.3%) | 0.07 * | 15 (46.9%) | 0.21 * |
| Sexual | ||||
| Patients, no. | 30 | 32 | ||
| Mean (SD) | −1.9 (15.3) | 0.38 ** | −3.8 (18.3) | |
| Median | 0.3 | −1.8 | ||
| >11-point reduction, no (%) § | 9 (30%) | 0.28 * | 8 (25%) | 0.12 * |
| Hormonal | ||||
| Patients, no. | 30 | 32 | ||
| Mean (SD) | −1.3 (13.8) | 0.50 ** | 0.2 (13.6) | |
| Median | 0.0 | 0.0 | ||
| >3-point reduction, no (%) ¶ | 13 (43%) | 0.27 * | 8 (25%) | 0.06 * |
| Adverse Event (Maximum Grade) | SBRT (n = 31) | CFRT (n = 33) | p-Value |
|---|---|---|---|
| Acute GI Toxicity | |||
| None reported | 20 (64%) | 4 (12%) | p < 0.0001 † |
| 1 | 9 (29%) | 22 (66%) | |
| 2 | 2 (6%) | 7 (21%) | |
| ≥3 | 0 | 0 | |
| ≥1 (Total) | 11 (35%) | 29 (87%) | |
| Acute GU Toxicity | |||
| None reported | 3 (9%) | 0 | p = 0.0426 ‡ |
| 1 | 26 (83%) | 25 (75%) | |
| 2 | 1 (3%) | 8 (24%) | |
| ≥3 | 0 | 0 | |
| ≥1 (Total) | 27 (87%) | 33 (100%) | |
| 1-Year Late GI Toxicity | |||
| None reported | 11 (35%) | 5 (15%) | p = 0.033 † |
| 1 | 16 (51%) | 22 (66%) | |
| 2 | 4 (12%) | 6 (18%) | |
| ≥3 | 0 | 0 | |
| ≥1 (Total) | 20 (64%) | 28 (84%) | |
| 1-Year Late GU Toxicity | |||
| None reported | 2 (6%) | 0 | p = 0.2307 † |
| 1 | 23 (74%) | 25 (75%) | |
| 2 | 5 (16%) | 7 (21%) | |
| ≥3 | 1 (3%) | 1 (3%) | |
| ≥1 (Total) | 29 (93%) | 33 (100%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poon, D.M.C.; Lam, D.; Wong, K.C.W.; Chu, C.-M.; Cheung, M.; Mo, F.; Suen, J.; Ng, C.-F.; Chan, A.T.C. Prospective Randomized Phase II Study of Stereotactic Body Radiotherapy (SBRT) vs. Conventional Fractionated Radiotherapy (CFRT) for Chinese Patients with Early-Stage Localized Prostate Cancer. Curr. Oncol. 2022, 29, 27-37. https://doi.org/10.3390/curroncol29010003
Poon DMC, Lam D, Wong KCW, Chu C-M, Cheung M, Mo F, Suen J, Ng C-F, Chan ATC. Prospective Randomized Phase II Study of Stereotactic Body Radiotherapy (SBRT) vs. Conventional Fractionated Radiotherapy (CFRT) for Chinese Patients with Early-Stage Localized Prostate Cancer. Current Oncology. 2022; 29(1):27-37. https://doi.org/10.3390/curroncol29010003
Chicago/Turabian StylePoon, Darren M. C., Daisy Lam, Kenneth C. W. Wong, Cheuk-Man Chu, Michael Cheung, Frankie Mo, Joyce Suen, Chi-Fai Ng, and Anthony T. C. Chan. 2022. "Prospective Randomized Phase II Study of Stereotactic Body Radiotherapy (SBRT) vs. Conventional Fractionated Radiotherapy (CFRT) for Chinese Patients with Early-Stage Localized Prostate Cancer" Current Oncology 29, no. 1: 27-37. https://doi.org/10.3390/curroncol29010003