
1-O-alkyl-glycerols from Squid Berryteuthis magister Reduce Inflammation and Modify Fatty Acid and Plasmalogen Metabolism in Asthma Associated with Obesity
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics of Clinical, Biochemical, and Immune Parameters of Obese Asthma Patients
2.2. 1-O-alkyl-glycerols Improve Lung Function in Obese Asthma Patients
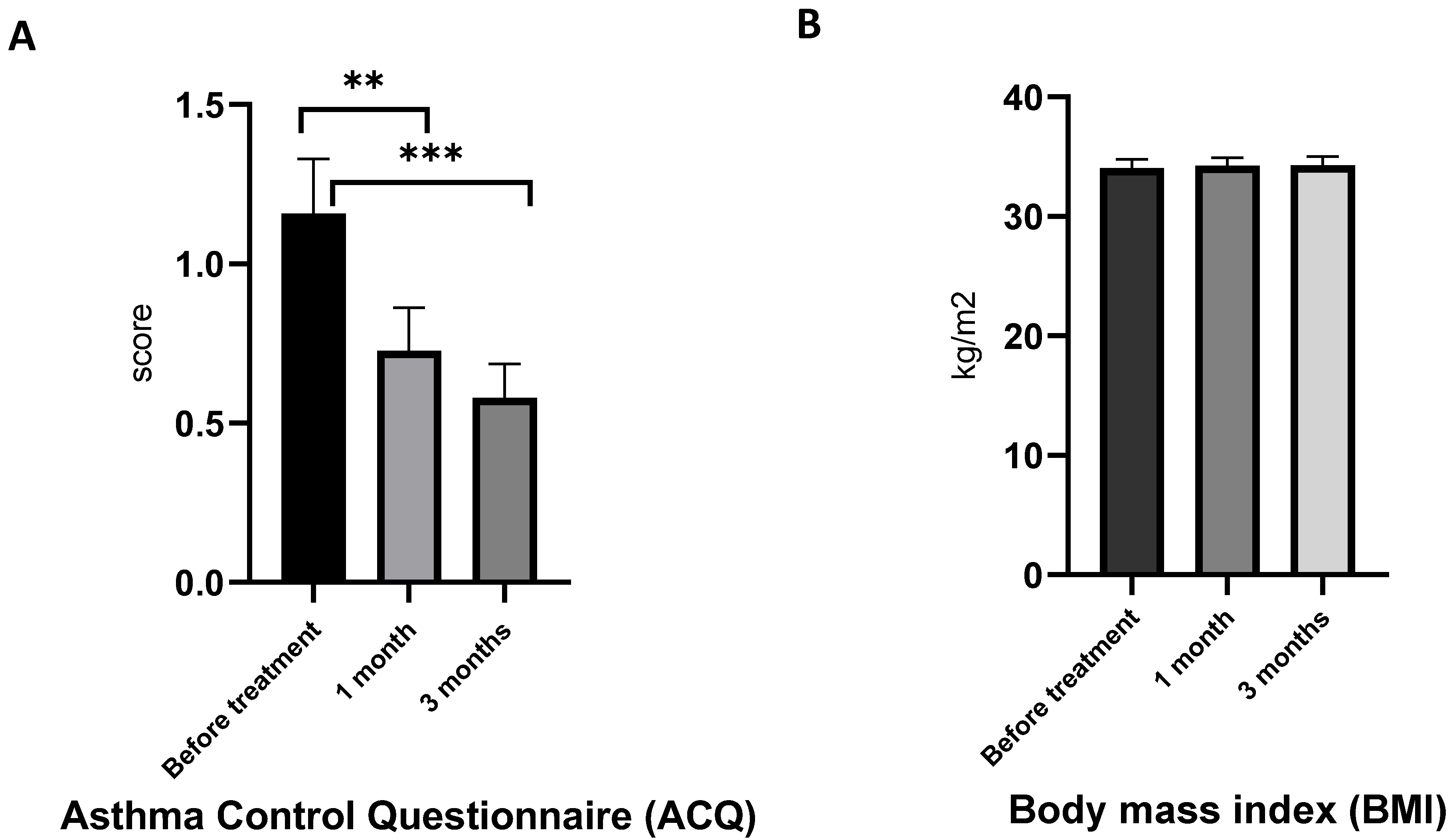
2.3. 1-O-alkyl-glycerols Reduce ACQ, but Do Not Affect BMI in Obese Asthma Patients
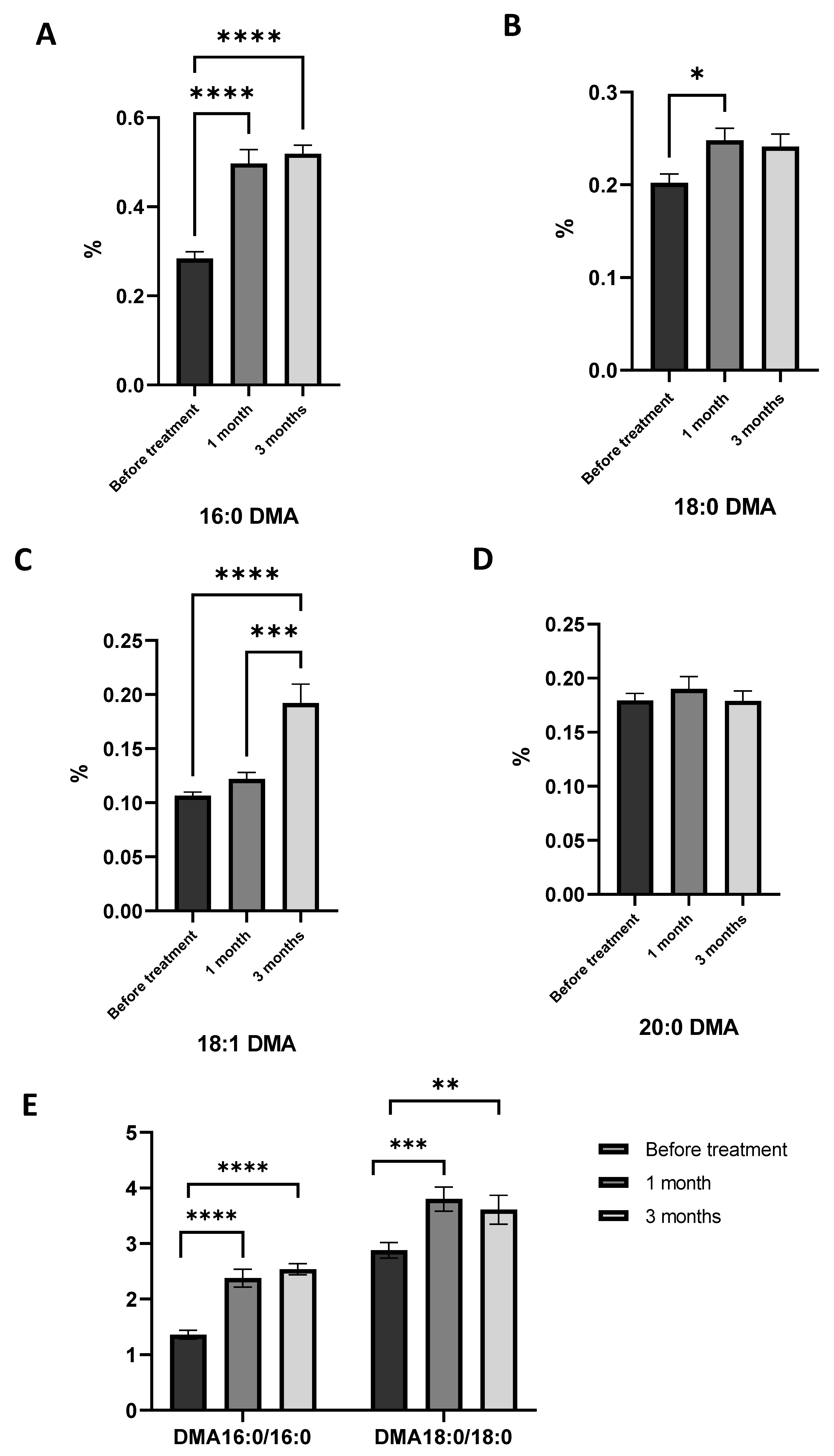
2.4. Effects of 1-O-alkyl-glycerol Supplementation on Plasmalogen Level in Obese Asthma Patients
2.5. Effects of 1-O-alkyl-glycerol Supplementation on Plasma Fatty Acid and Oxylipin Level in Obese Asthma Patients
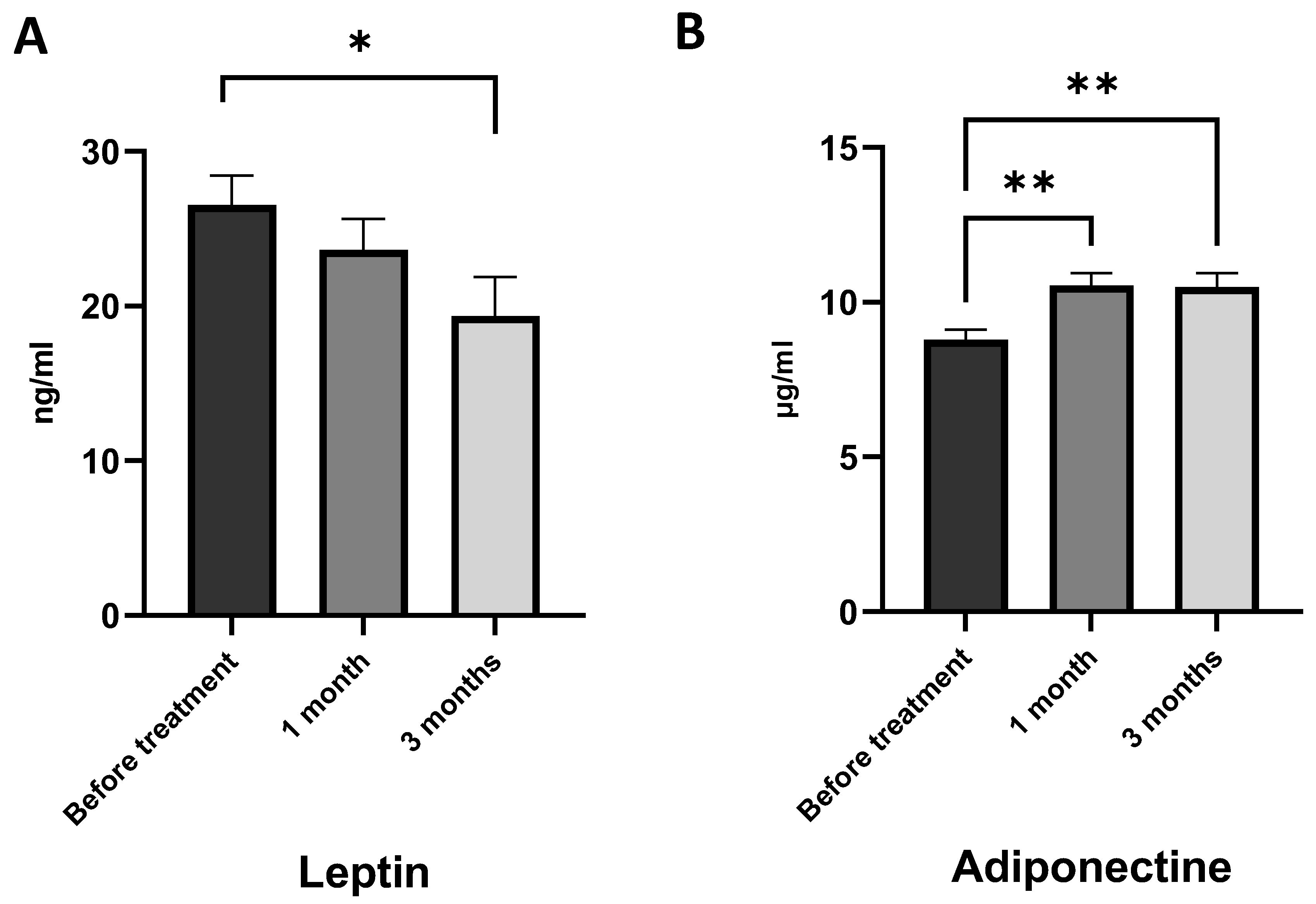
2.6. 1-O-alkyl-glycerols Regulate Adipocyte Adiponectin and Leptin Generation in Obese Asthma Patients
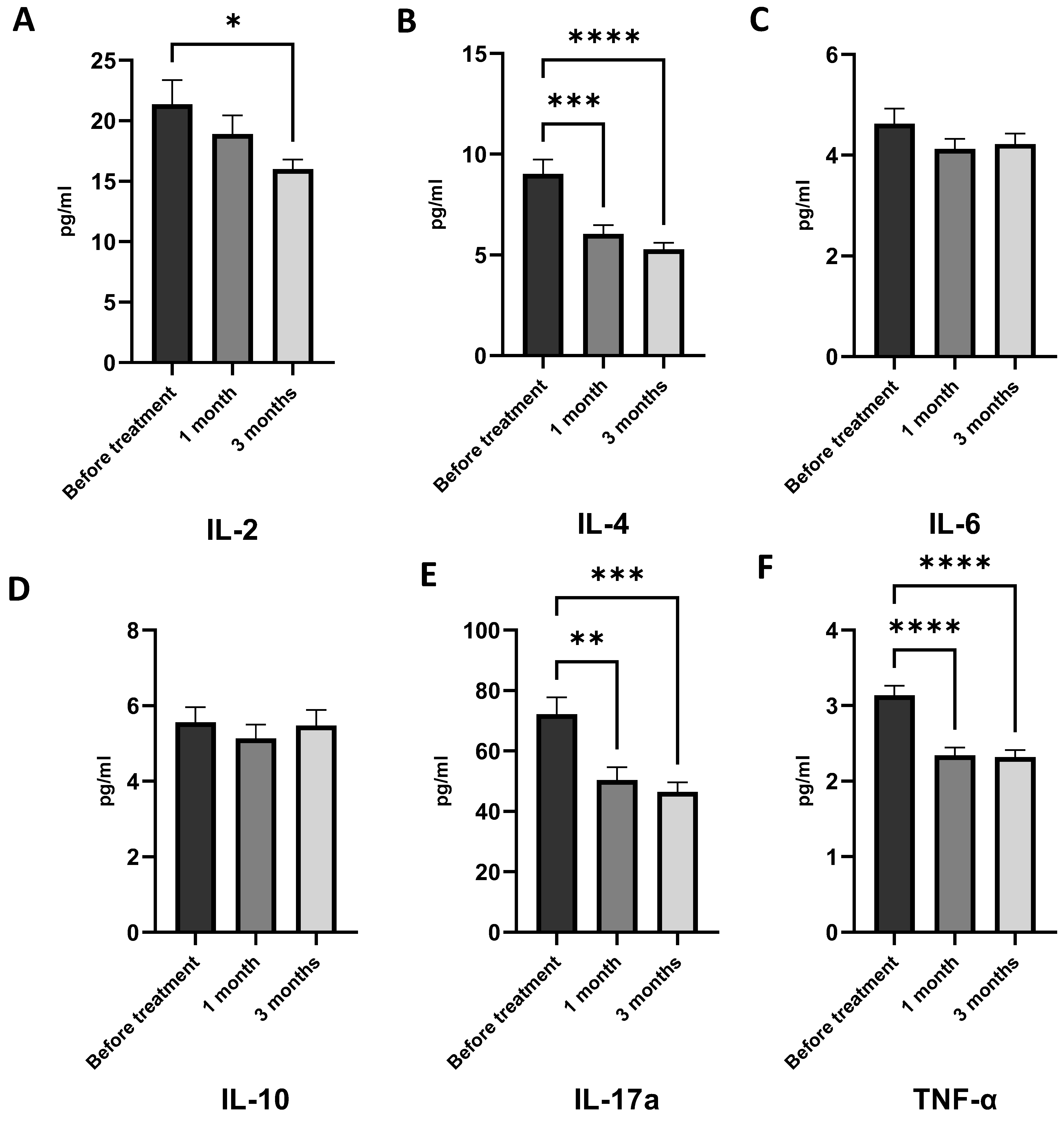
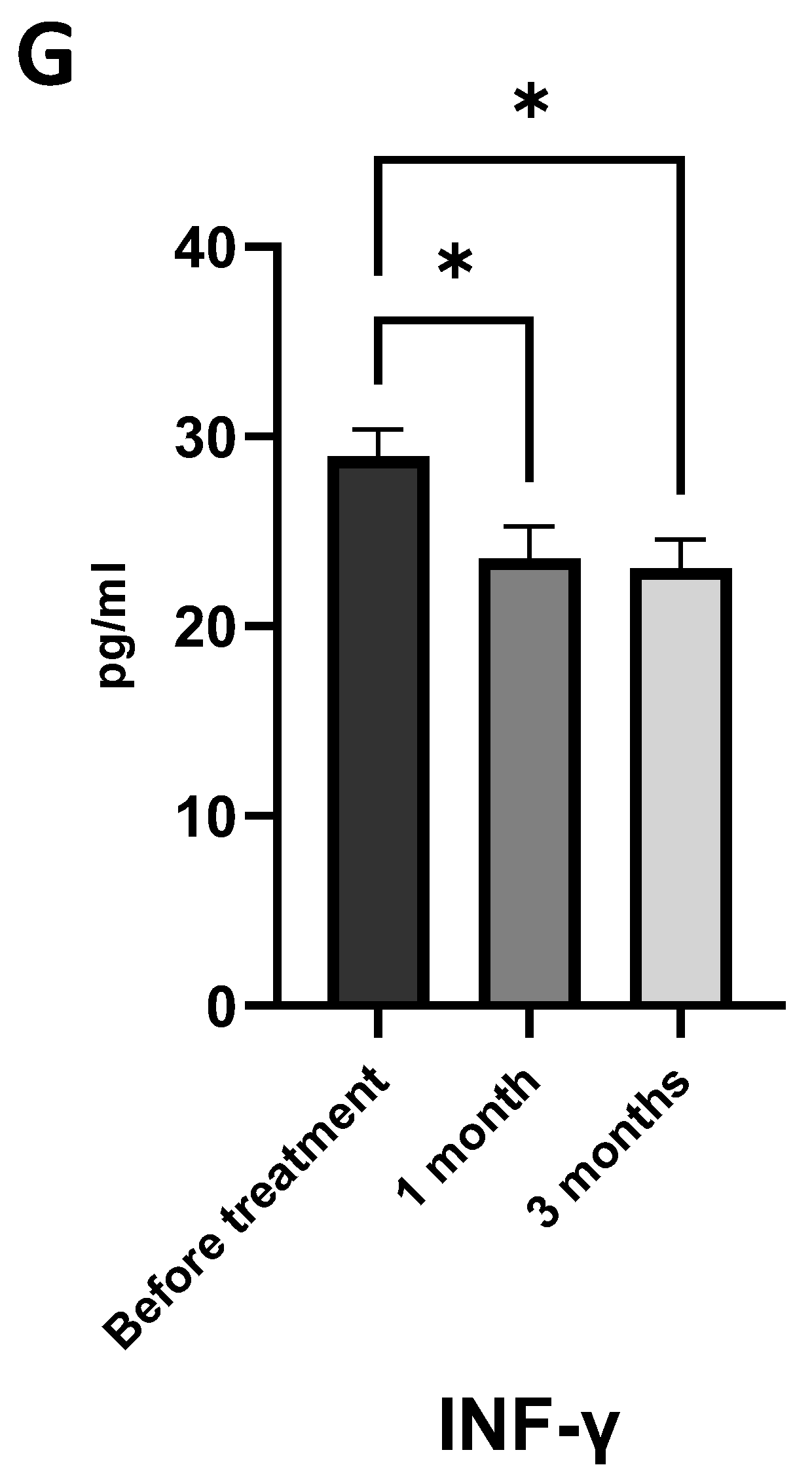
2.7. 1-O-alkyl-glycerols Modulate Immune System Function and Reduce Chronic Inflammation
3. Discussion
4. Materials and Methods
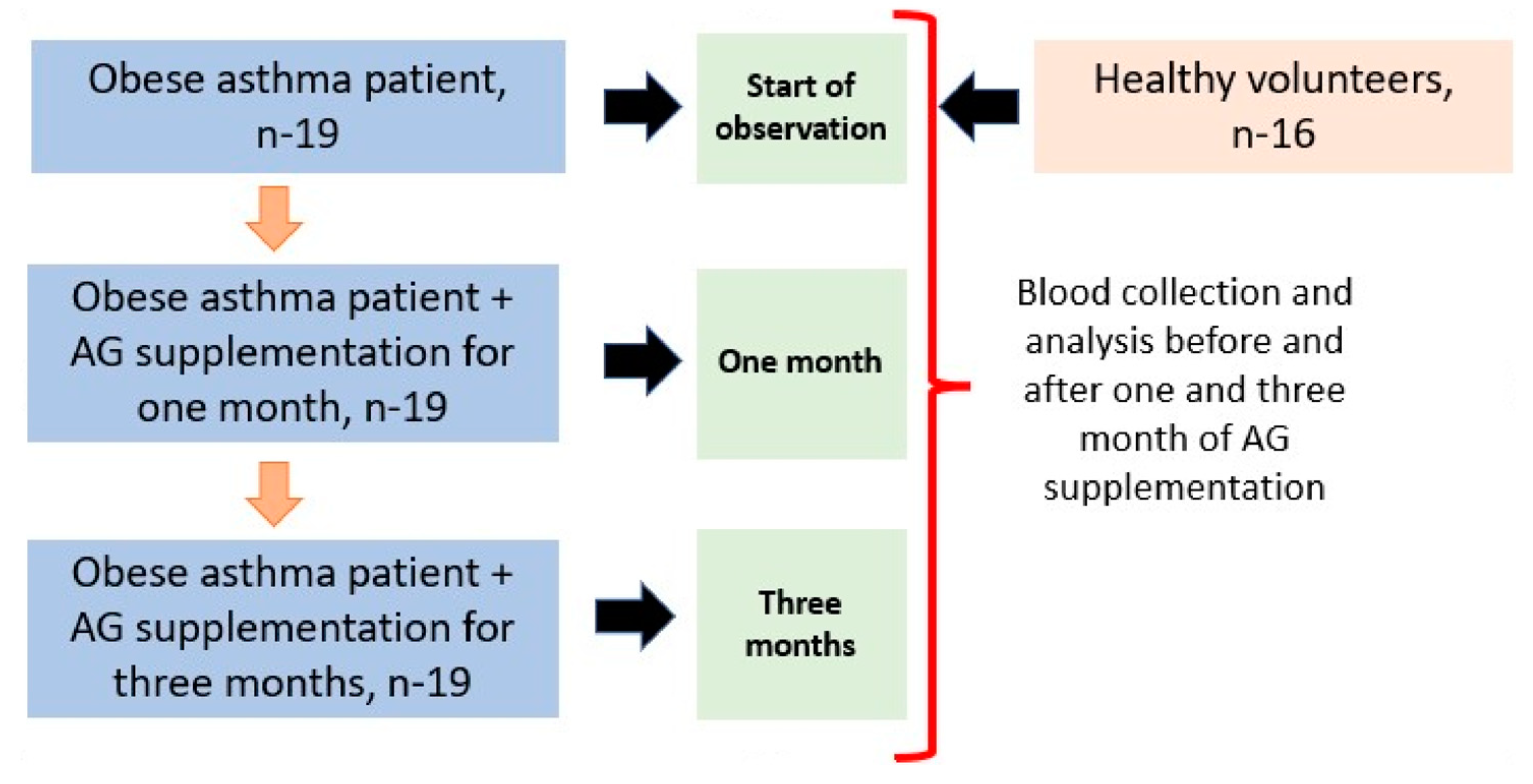
4.1. Study Population and Sample Selection
4.2. Treatment and Supplementation
4.3. Analysis of Total Fatty Acids and Dimethyl Acetals in Plasma
4.4. Analysis of Eicosanoid Concentrations
4.5. Cytokine and Adipokine Level Analysis
4.6. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Papi, A.; Brightling, C.; Pedersen, S.; Reddel, H. Asthma. Lancet 2018, 391, 783–800. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention. Available online: https://ginasthma.org (accessed on 2 April 2023).
- Bantulà, M.; Roca-Ferrer, J.; Ebymar, A.; Picado, C. Asthma and Obesity: Two Diseases on the Rise and Bridged by Inflammation. J. Clin. Med. 2021, 10, 169. [Google Scholar] [CrossRef] [PubMed]
- Tooba, R.; Wu, T. Obesity and asthma: A focused review. Respir. Med. 2022, 204, 107012. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, S.C.; Panettieri, R.A.; Rastogi, D. Mechanistic Links Between Obesity and Airway Pathobiology Inform Therapies for Obesity-Related Asthma. Paediatr. Drugs 2023, 25, 283–299. [Google Scholar] [CrossRef] [PubMed]
- Scott, H.A.; Wood, L.G.; Gibson, P.G. Role of Obesity in Asthma: Mechanisms and Management Strategies. Curr. Allergy Asthma Rep. 2017, 17, 53. [Google Scholar] [CrossRef]
- Zhang, X.; Zheng, J.; Zhang, L.; Liu, Y.; Chen, G.P.; Zhang, H.P.; Wang, L.; Kang, D.Y.; Wood, L.G.; Wang, G. Systemic Inflammation Mediates the Detrimental Effects of Obesity on Asthma Control. Allergy Asthma Proc. 2018, 39, 43–50. [Google Scholar] [CrossRef]
- Vezir, E.; Civelek, E.; Dibek Misirlioglu, E.; Toyran, M.; Capanoglu, M.; Karakus, E.; Kahraman, T.; Ozguner, M.; Demirel, F.; Gursel, I. Effects of Obesity on Airway and Systemic Inflammation in Asthmatic Children. Int. Arch. Allergy Immunol. 2021, 182, 679–689. [Google Scholar] [CrossRef]
- Cartier, A.; Lemieux, I.; Alméras, N.; Tremblay, A.; Bergeron, J.; Després, J.P. Visceral Obesity and Plasma Glucose-Insulin Homeostasis: Contributions of Interleukin-6 and Tumor Necrosis Factor-α in Men. J. Clin. Endocrinol. Metab. 2008, 93, 1931–1938. [Google Scholar] [CrossRef]
- Bantulà, M.; Tubita, V.; Roca-Ferrer, J.; Mullol, J.; Valero, A.; Bobolea, I.; Pascal, M.; de Hollanda, A.; Vidal, J.; Picado, C.; et al. Differences in Inflammatory Cytokine Profile in Obesity-Associated Asthma: Effects of Weight Loss. J. Clin. Med. 2022, 11, 3782. [Google Scholar] [CrossRef]
- Landecho, M.F.; Tuero, C.; Valentí, V.; Bilbao, I.; de la Higuera, M.; Frühbeck, G. Relevance of Leptin and Other Adipokines in Obesity-Associated Cardiovascular Risk. Nutrients 2019, 11, 2664. [Google Scholar] [CrossRef] [Green Version]
- Leiria, L.O.; Martins, M.A.; Saad, M.J.A. Obesity and asthma: Beyond TH2 inflammation. Metabolism 2015, 64, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Marijsse, G.S.; Seys, S.F.; Schelpe, A.S.; Dilissen, E.; Goeminne, P.; Dupont, L.J.; Ceuppens, J.L.; Bullens, D.M. Obese individuals with asthma preferentially have a high IL-5/IL-17A/IL-25 sputum inflammatory pattern. Am. J. Respir. Crit. Care Med. 2014, 189, 1281–1284. [Google Scholar] [CrossRef] [PubMed]
- Diaz, J.; Farzan, S. Clinical implications of the obese-asthma phenotypes. Immunol. Allergy Clin. N. Am. 2014, 34, 739–751. [Google Scholar] [CrossRef] [PubMed]
- Farzan, S.; Coyle, T.; Coscia, G.; Rebaza, A.; Santiago, M. Clinical Characteristics and Management Strategies for Adult Obese Asthma Patients. J. Asthma Allergy 2022, 15, 673–689. [Google Scholar] [CrossRef]
- Honsho, M.; Fujiki, Y. Plasmalogen homeostasis—Segulation of plasmalogen biosynthesis and its physiological consequence in mammals. FEBS 2017, 591, 2720–2729. [Google Scholar] [CrossRef] [Green Version]
- Nagan, N.; Zoellerb, R.A. Plasmalogens: Biosynthesis and functions. Prog. Lipid Res. 2001, 40, 199–229. [Google Scholar] [CrossRef]
- Braverman, N.E.; Moser, A.B. Functions of plasmalogen lipids in health and disease. Biochim. Biophys. Acta 2012, 1822, 1442–1452. [Google Scholar] [CrossRef] [Green Version]
- Sordillo, J.E.; Lutz, S.M.; Kelly, R.S.; McGeachie, M.J.; Dahlin, A.; Tantisira, K.; Clish, C.; Lasky-Su, J.; Wu, A.C. Plasmalogens Mediate the Effect of Age on Bronchodilator Response in Individuals with Asthma. Front. Med. 2020, 7, 38. [Google Scholar] [CrossRef] [Green Version]
- Zhuo, R.; Rong, P.; Wang, J.; Parvin, R.; Deng, Y. The Potential Role of Bioactive Plasmalogens in Lung Surfactant. Front. Cell Dev. Biol. 2021, 9, 618102. [Google Scholar] [CrossRef]
- Rüdiger, M.; von Baehr, A.; Haupt, R.; Wauer, R.R.; Rüstow, B. Preterm infants with high polyunsaturated fatty acid and plasmalogen content in tracheal aspirates develop bronchopulmonary dysplasia less often. Crit. Care Med. 2000, 28, 1572–1577. [Google Scholar] [CrossRef]
- Senanayake, V.; Goodenowe, D.B. Plasmalogen deficiency and neuropathology in Alzheimer’s disease: Causation or coincidence? Alzheimers Dement. 2019, 5, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, S.; Kanno, S.; Nakagawa, K.; Kinoshitaa, M.; Miyazawa, T. Extrinsic plasmalogens suppress neuronal apoptosis in mouse neuroblastoma Neuro-2A cells: Importance of plasmalogen molecular species. RSC Adv. 2015, 75, 61012–61020. [Google Scholar] [CrossRef]
- Paul, S.; Lancaster, G.I.; Meikle, P.J. Plasmalogens: A potential therapeutic target for neurodegenerative and cardiometabolic disease. Prog. Lipid Res. 2019, 74, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Mello, V.D.; Selander, T.; Lindström, J.; Tuomilehto, J.; Uusitupa, M.; Kaarniranta, K. Serum Levels of Plasmalogens and Fatty Acid Metabolites Associate with Retinal Microangiopathy in Participants from the Finnish Diabetes Prevention Study. Nutrients 2021, 13, 4452. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.E.; Park, H.S.; Yoo, H.J.; Baek, I.-J.; Yoon, J.E.; Ko, M.S.; Kim, A.R.; Kim, R.S.; Park, H.-S.; Lee, S.E. Protective role of endogenous plasmalogens against hepatic steatosis and steatohepatitis. Hepatology 2017, 66, 416–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodenowe, D.B.; Haroon, J.; Kling, M.A.; Zielinski, M.; Mahdavi, K.; Habelhah, B.; Shtilkind, L.; Jordan, S. Targeted Plasmalogen Supplementation: Effects on Blood Plasmalogens, Oxidative Stress Biomarkers, Cognition, and Mobility in Cognitively Impaired Persons. Front. Cell. Dev. Biol. 2022, 10, 864842. [Google Scholar] [CrossRef]
- Astudillo, A.M.; Balboa, M.A.; Balsinde, J. Compartmentalized regulation of lipid signaling in oxidative stress and inflammation: Plasmalogens, oxidized lipids and ferroptosis as new paradigms of bioactive lipid research Affiliations expand. Rev. Prog. Lipid Res. 2022, 89, 101207. [Google Scholar] [CrossRef]
- Ifuku, M.; Katafuchi, T.; Mawatari, S.; Noda, M.; Miake, K.; Sugiyama, M.; Fujino, T. Anti-inflammatory/anti-amyloidogenic effects of plasmalogens in lipopolysaccharide-induced neuroinflammation in adult mice. J. Neuroinflamm. 2012, 9, 197. [Google Scholar] [CrossRef] [Green Version]
- Bozelli, J.C.; Azher, S.; Epand, R. Plasmalogens and Chronic Inflammatory Diseases. Front. Physiol. 2021, 12, 730829. [Google Scholar] [CrossRef]
- Sultanov, R.; Ermolenko, E.; Poleshchuk, T.; Kasyanov, S. Alkyl Glycerol Ethers as Adaptogens. Mar. Drugs 2023, 21, 4. [Google Scholar] [CrossRef]
- Deniau, A.L.; Mosset, P.; Pédrono, F.; Mitre, R.; Le Bot, D.; Legrand, A.B. Multiple beneficial health effects of natural alkylglycerols from shark liver oil. Mar. Drugs 2010, 8, 2175–2184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ermolenko, E.; Latyshev, N.; Sultanov, R.; Kasyanov, S. Technological approach of 1-O-alkyl-sn-glycerols separation from Berryteuthis magister squid liver oil. J. Food Sci. Technol. 2016, 53, 1722–1726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brites, P.; Ferreira, A.S.; Ferreira da Silva, T.; Sousa, V.F.; Malheiro, A.R.; Duran, M. Alkyl-Glycerol Rescues Plasmalogen Levels and Pathology of Ether-Phospholipid Deficient Mice. PLoS ONE 2011, 6, e28539. [Google Scholar] [CrossRef] [Green Version]
- Ali, F.; Hossain, M.S.; Sejimo, S. Plasmalogens Inhibit Endocytosis of Toll-like Receptor 4 to Attenuate the Inflammatory Signal in Microglial Cells. Mol. Neurobiol. 2019, 56, 3404–3419. [Google Scholar] [CrossRef] [PubMed]
- Sultanov, R.; Ermolenko, E.; Poleschuk, T.; Denisenko, Y.; Kasyanov, S. Action of alkyl glycerol ethers and n-3 polyunsaturated fatty acids diet on hematological parameters of blood and liver plasmalogen level in aged rats. J. Food Sci. 2021, 86, 2727–2735. [Google Scholar] [CrossRef] [PubMed]
- Latyshev, N.A.; Ermakova, S.P.; Ermolenko, E.V.; Imbs, A.B.; Kasyanov, S.P.; Sultanov, R.M. 1-O-alkylglycerols from the hepatopancreas of the crab Paralithodes camtschaticus, liver of the squid Berryteuthis magister, and liver of the skate Bathyraja parmifera, and their anticancer activity on human melanoma cells. J. Food Biochem. 2019, 43, e12828. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.; Smith, A.A.T.; Culham, K.; Gunawan, K.A.; Weir, J.M.; Cinel, M.A.; Jayawardana, K.S.; Mellett, N.A.; Lee, M.K.S.; Murphy, A.J.; et al. Shark liver oil supplementation enriches endogenous plasmalogens and reduces markers of dyslipidemia and inflammation. J. Lipid Res. 2021, 62, 100092. [Google Scholar] [CrossRef]
- Hamadate, N.; Matsumoto, Y.; Seto, K.; Yamamoto, T.; Yamaguchi, H.; Nakagawa, T.; Yamamoto, E.; Fukagawa, M.; Yazawa, K. Vascular effects and safety of supplementation with shark liver oil in middle-aged and elderly males. Exp. Ther. Med. 2015, 10, 641–646. [Google Scholar] [CrossRef] [Green Version]
- Parri, A.; Fitó, M.; Torres, C.F. Alkylglycerols reduce serum complement and plasma vascular endothelial growth factor in obese individuals. Inflammopharmacoly 2016, 24, 127–131. [Google Scholar] [CrossRef] [Green Version]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.; Coates, A.; van der Grinten, C.P.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir J. 2005, 26, 948–968. [Google Scholar] [CrossRef] [Green Version]
- Denisenko, Y.K.; Kytikova, O.Y.; Novgorodtseva, T.P.; Antonyuk, M.V.; Gvozdenko, T.A.; Kantur, T.A. Lipid-Induced Mechanisms of Metabolic Syndrome. J. Obes. 2020, 26, 5762395. [Google Scholar] [CrossRef] [PubMed]
- Fruhbeck, G.; Catalan, V.; Rodriguez, A.; Gomez-Ambrosi, J. Adiponectin-Leptin Ratio: A Promising Index to Estimate Adipose Tissue Dysfunction. Relation with Obesity-Associated Cardiometabolic Risk. Adipocyte 2018, 7, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Aljafary, M.A.; Al-Suhaimi, E.A. Adiponectin System (Rescue Hormone): The Missing Link between Metabolic and Cardiovascular Diseases. Pharmaceutics 2022, 14, 1430. [Google Scholar] [CrossRef]
- Telenga, E.D.; Tideman, S.W.; Kerstjens, H.A.M.; Hacken, N.H.T.T.; Timens, W.; Postma, D.S.; Berge, M.V.D. Obesity in asthma: More neutrophilic inflammation as a possible explanation for a reduced treatment response. Allergy 2012, 67, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- Debouzy, J.C.; Crouzier, D.; Lefebvre, B.; Dabouis, V. Study of alkylglycerol containing shark liver oil: A physic chemical support for biological effects. Drug Target Insights 2008, 3, 125–135. [Google Scholar] [CrossRef] [Green Version]
- Hichami, A.; Duroudier, V.; Leblais, V.; Vernhet, L.; Le Goffic, F.; Ninio, E.; Legrand, A. Modulation of platelet-activating-factor production by incorporation of naturally occurring 1-O-alkylglycerols in phospholipids of human leukemic monocyte-like cells THP-1. Eur. J. Biochem. 1997, 250, 242–248. [Google Scholar] [CrossRef]
- Pédrono, F.; Khan, N.A.; Legrand, A.B. Regulation of calcium signalling by 1-O-alkylglycerols in human Jurkat T cells. Life Sci. 2004, 74, 2793–2801. [Google Scholar] [CrossRef]
- Hossain, M.S.; Mawatari, S.; Fujino, T. Plasmalogens, the Vinyl Ether-Linked Glycerophospholipids, Enhance Learning and Memory by Regulating Brain-Derived Neurotrophic Factor. Front. Cell Dev. Biol. 2022, 9, 828282. [Google Scholar] [CrossRef]
- Arismendi, E.; Bantulà, M.; Perpiñá, M.; Picado, C. Effects of Obesity and Asthma on Lung Function and Airway Dysanapsis in Adults and Children. J. Clin. Med. 2020, 9, 3762. [Google Scholar] [CrossRef]
- Dias-Júnior, S.A.; Reis, M.; de Carvalho-Pinto, R.M.; Stelmach, R.; Halpern, A.; Cukier, A. Effects of weight loss on asthma control in obese patients with severe asthma. Eur. Respir. J. 2014, 43, 1368–1377. [Google Scholar] [CrossRef] [Green Version]
- Wynalda, K.M.; Murphy, R.C. Low-concentration ozone reacts with plasmalogen glycerophosphoethanolamine lipids in lung surfactant. Chem. Res. Toxicol. 2010, 23, 108–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engelmann, B. Plasmalogens: Targets for oxidants and major lipophilic antioxidants. Biochem. Soc. Trans. 2004, 32, 147–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, C.; Zhou, J.; Yang, S.; Li, H.; Wang, C.; Fang, X.; Fan, Y.; Zhang, J.; Han, X.; Wen, C. Oxidative stress leads to reduction of plasmalogen serving as a novel biomarker for systemic lupus erythematosus. Free Radic. Biol. Med. 2016, 101, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Dorninger, F.; Forss-Petter, S.; Wimmerb, I.; Berger, J. Plasmalogens, platelet-activating factor and beyond—Ether lipids in signaling and neurodegeneration. Neurobiol. Dis. 2020, 145, 105061. [Google Scholar] [CrossRef]
- Kleiboeker, B.; Lodhi, I.J. Peroxisomal regulation of energy homeostasis: Effect on obesity and related metabolic disorders. Mol. Metab. 2022, 65, 101577. [Google Scholar] [CrossRef]
- Kytikova, O.; Novgorodtseva, T.; Denisenko, Y.; Antonyuk, M.; Gvozdenko, T. Pro-Resolving Lipid Mediators in the Pathophysiology of Asthma. Medicina 2019, 55, 284. [Google Scholar] [CrossRef] [Green Version]
- Youssef, M.; Ibrahim, A.; Akashi, K.; Hossain, M.S. PUFA-Plasmalogens Attenuate the LPS-Induced Nitric Oxide Production by Inhibiting the NF-kB, p38 MAPK and JNK Pathways in Microglial Cells. Neuroscience 2019, 397, 18–30. [Google Scholar] [CrossRef]
- Kim, H.Y.; Lee, H.J.; Chang, Y.-J.; Pichavant, M.; Shore, S.A.; Fitzgerald, K.A.; Iwakura, Y.; Israel, E.; Bolger, K.; Faul, J. Interleukin-17–producing innate lymphoid cells and the NLRP3 inflammasome facilitate obesity-associated airway hyperreactivity. Nat. Med. 2014, 20, 54–61. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 2 April 2023).
- Brauer, P.; Gorber, S.C.; Shaw, E.; Singh, H.; Bell, N.; Shane, A.R.; Jaramillo, A.; Tonelli, M. Canadian Task Force on Preventive Health Care. Recommendations for prevention of weight gain and use of behavioural and pharmacologic interventions to manage overweight and obesity in adults in primary care. Can. Med. Assoc. J. 2015, 187, 184–195. [Google Scholar] [CrossRef] [Green Version]
- Bligh, E.G.; Dyer, W.J. A rapid method of total lipid extraction and purification. Can. J. Biochem. Physiol. 1959, 37, 911–917. [Google Scholar] [CrossRef]
- Carreau, J.P.; Dubacq, J.P. Adaptation of a macro-scale method to the micro-scale for fatty acid methyl transesterification of biological lipid extracts. J. Chromatogr. 1978, 151, 384–390. [Google Scholar] [CrossRef]
- Christie, W.W. Equivalent chain-lengths of methyl ester derivatives of fatty acids on gas chromatography A reappraisal. J. Chromatogr. 1988, 447, 305–314. [Google Scholar] [CrossRef]
- Bjorkhem, I.; Sisfontes, L.; Bostrom, B.; Kase, B.F.; Blomstrand, R. Simple diagnosis of the Zellweger syndrome by gas-liquid chromatography of dimethyl acetals. J. Lipid Res. 1986, 27, 786–791. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Healthy | Asthma with Obesity |
|---|---|---|
| Age | 45.88 ± 8.54 | 58.31 ± 7.01 |
| Body mass index (BMI), kg/m2 | 23.50 ± 0.72 | 34.06 ± 0.72 *** |
| Asthma Control Questionnaire (ACQ) | - | 1.08 ± 0.15 |
| Adiponectin, mg/mL | 11.94 ± 0.60 | 9.32 ± 0.38 **** |
| Leptin, ng/mL | 2.03 ± 0.21 | 26.53 ± 1.89 **** |
| Interleukin-2 (IL-2), pg/mL | 13.30 ± 0.73 | 21.36 ± 2.00 ** |
| Interleukin-4 (IL-4), pg/mL | 3.39 ± 0.19 | 9.02 ± 0.70 *** |
| Interleukin-6 (IL-6), pg/mL | 4.49 ± 0.28 | 4.62 ± 0.30 |
| Interleukin-10 (IL-10), pg/mL | 5.29 ± 0.19 | 5.56 ± 0.40 |
| Tumor necrosis factor-α (TNF-α), pg/mL | 2.31 ± 0.09 | 3.13 ± 0.13 *** |
| Interferon gamma (IFN-γ), pg/mL | 28.79 ± 2.57 | 28.93 ± 1.43 |
| Interleukin-17a (IL-17a), pg/mL | 36.05 ± 1.29 | 72.10 ± 5.62 *** |
| Thromboxane B2 (TXB2), pg/mL | 63.18 ± 2.50 | 91.56 ± 1.75 **** |
| Leukotriene B4 (LTB4), pg/mL | 12.06 ± 0.61 | 25.81 ± 1.02 **** |
| Fatty Acids, % | Healthy | Asthma with Obesity |
|---|---|---|
| 14:0 | 0.51 ± 0.02 | 1.04 ± 0. 05 *** |
| 15:0 | 0.18 ± 0.01 | 0.19 ± 0.008 |
| 16:0 | 20.27 ± 0.37 | 21.76 ± 0.33 |
| 16:1n−9 | 0.39 ± 0.009 | 0.47 ± 0.01 *** |
| 16:1n−7 | 1.46 ± 0.07 | 2.02 ± 0.09 *** |
| 18:0 | 6.32 ± 0.13 | 7.05 ± 0.11 *** |
| 18:1n−9 | 15.80 ± 0.41 | 16.71 ± 0.25 |
| 18:1n−7 | 1.52 ± 0.05 | 1.55 ± 0.02 |
| 18:2n−6 | 37.17 ± 0.76 | 36.01 ± 0.59 |
| 18:3n−6 | 0.32 ± 0.02 | 0.36 ± 0.02 |
| 18:3n−3 | 0.53 ± 0.01 | 0.47 ± 0.01 * |
| 20:3n−6 | 1.16 ± 0.06 | 1.17 ± 0.04 |
| 20:4n−6 | 5.14 ± 0.12 | 5.47 ± 0.17 * |
| 20:5n−3 | 0.88 ± 0.07 | 0.78 ± 0.09 * |
| 22:4n−6 | 0.18 ± 0.01 | 0.12 ± 0.004 *** |
| 22:5n−3 | 0.46 ± 0.03 | 0.41 ± 0.029 |
| 22:6n−3 | 2.32 ± 0.15 | 1.50 ± 0.04 *** |
| 16:0DMA | 0.41 ± 0.02 | 0,28 ± 0.01 ** |
| 18:0DMA | 0.27 ± 0.01 | 0.20 ± 0.00 ** |
| 18:1DMA | 0.14 ± 0.006 | 0.10 ± 0.00 |
| 20:0DMA | 0.16 ± 0.007 | 0.17 ± 0.00 |
| DMA16:0/16:0FAME | 1.97 ± 0.14 | 1.31 ± 0.07 *** |
| DMA18:0/18:0FAME | 4.14 ± 0.25 | 2.87 ± 0.14 *** |
| Lung Function Parameters, % | Before Treatment | One Month | Three Months |
|---|---|---|---|
| VC | 108.7 (98.1;118.8) | 110.2 (102.3;118.8) | 110.9 (105.3;119.4) |
| FVC | 107.2 (98.2;116.0) | 109.78 (101.7;116.0) | 109.5 (101.2;117.8) |
| FEV1 | 105.2 (99.7; 112.4) | 108.6 (102.8;113.3) p < 0.001 | 109.0 (102.9;114.1) p < 0.001 |
| FEV1/VC | 87.0 (76.2;98.3) | 90.2 (77.9;101.3) p < 0.05 | 91.0 (78.3;102.5) p < 0.05 |
| FEV1/FVC | 83.1 (71.5; 91.3) | 86.7 (80.6;91.3) | 86.9 (80.8;92.2) |
| Asthma with Obesity | |||
|---|---|---|---|
| Fatty Acids, % | Before Treatment | One Month | Three Months |
| 14:0 | 1.04 ± 0.05 | 0.94 ± 0.06 | 0.89 ± 0.04 |
| 15:0 | 0.19 ± 0.008 | 0.19 ± 0.007 | 0.18 ± 0.00 |
| 16:0 | 21.76 ± 0.33 | 20.97 ± 0.38 | 20.57 ± 0.34 |
| 16:1n−9 | 0.47 ± 0.01 | 0.41 ± 0.01 * | 0.42 ± 0.01 |
| 16:1n−7 | 2.02 ± 0.09 | 2.00 ± 0.09 | 2.36 ± 0.13 |
| 18:0 | 7.05 ± 0.11 | 6.63 ± 0.15 * | 6.81 ± 0.14 |
| 18:1n−9 | 16.71 ± 0.25 | 16.32 ± 0.24 | 16.48 ± 0.3 |
| 18:1n−7 | 1.55 ± 0.02 | 1.53 ± 0.03 | 1.54 ± 0.03 |
| 18:2n−6 | 36.01 ± 0.59 | 34.54 ± 1.00 | 36.78 ± 0.74 |
| 18:3n−6 | 0.36 ± 0.02 | 0.33 ± 0.02 | 0.34 ± 0.02 |
| 18:3n−3 | 0.47 ± 0.01 | 0.51 ± 0.03 ** | 0.52 ± 0.03 ** |
| 20:3n−6 | 1.17 ± 0.04 | 1.23 ± 0.03 | 1.25 ± 0.03 |
| 20:4n−6 | 5.47 ± 0.17 | 5.04 ± 0.18 | 4.91 ± 0.2 * |
| 20:5n−3 | 0.78 ± 0.09 | 1.01 ± 0.11 ** | 0.91 ± 0.06 ** |
| 22:4n−6 | 0.12 ± 0.004 | 0.13 ± 0.006 | 0.13 ± 0.00 |
| 22:5n−3 | 0.41 ± 0.029 | 0.46 ± 0.025 | 0.45 ± 0.02 |
| 22:6n−3 | 1.50 ± 0.04 | 2.16 ± 0.13 *** | 2.08 ± 0.08 *** |
| Alkyl Chain a | Content, % b | Trivial Name |
|---|---|---|
| 14:0 | 1.55 ± 0.20 | |
| 16:0 | 91.07 ± 0.21 | chimyl alcohol |
| 18:0 | 7.38 ± 0.57 | batyl alcohol |
| Ʃsat | 100 ± 0.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Denisenko, Y.; Novgorodtseva, T.; Antonyuk, M.; Yurenko, A.; Gvozdenko, T.; Kasyanov, S.; Ermolenko, E.; Sultanov, R. 1-O-alkyl-glycerols from Squid Berryteuthis magister Reduce Inflammation and Modify Fatty Acid and Plasmalogen Metabolism in Asthma Associated with Obesity. Mar. Drugs 2023, 21, 351. https://doi.org/10.3390/md21060351
Denisenko Y, Novgorodtseva T, Antonyuk M, Yurenko A, Gvozdenko T, Kasyanov S, Ermolenko E, Sultanov R. 1-O-alkyl-glycerols from Squid Berryteuthis magister Reduce Inflammation and Modify Fatty Acid and Plasmalogen Metabolism in Asthma Associated with Obesity. Marine Drugs. 2023; 21(6):351. https://doi.org/10.3390/md21060351
Chicago/Turabian StyleDenisenko, Yulia, Tatyana Novgorodtseva, Marina Antonyuk, Alla Yurenko, Tatyana Gvozdenko, Sergey Kasyanov, Ekaterina Ermolenko, and Ruslan Sultanov. 2023. "1-O-alkyl-glycerols from Squid Berryteuthis magister Reduce Inflammation and Modify Fatty Acid and Plasmalogen Metabolism in Asthma Associated with Obesity" Marine Drugs 21, no. 6: 351. https://doi.org/10.3390/md21060351