Epidemiology and Toxicology of Ciguatera Poisoning in the Colombian Caribbean


 ,
,
Abstract
:1. Introduction
1.1. Epidemiology in Colombia
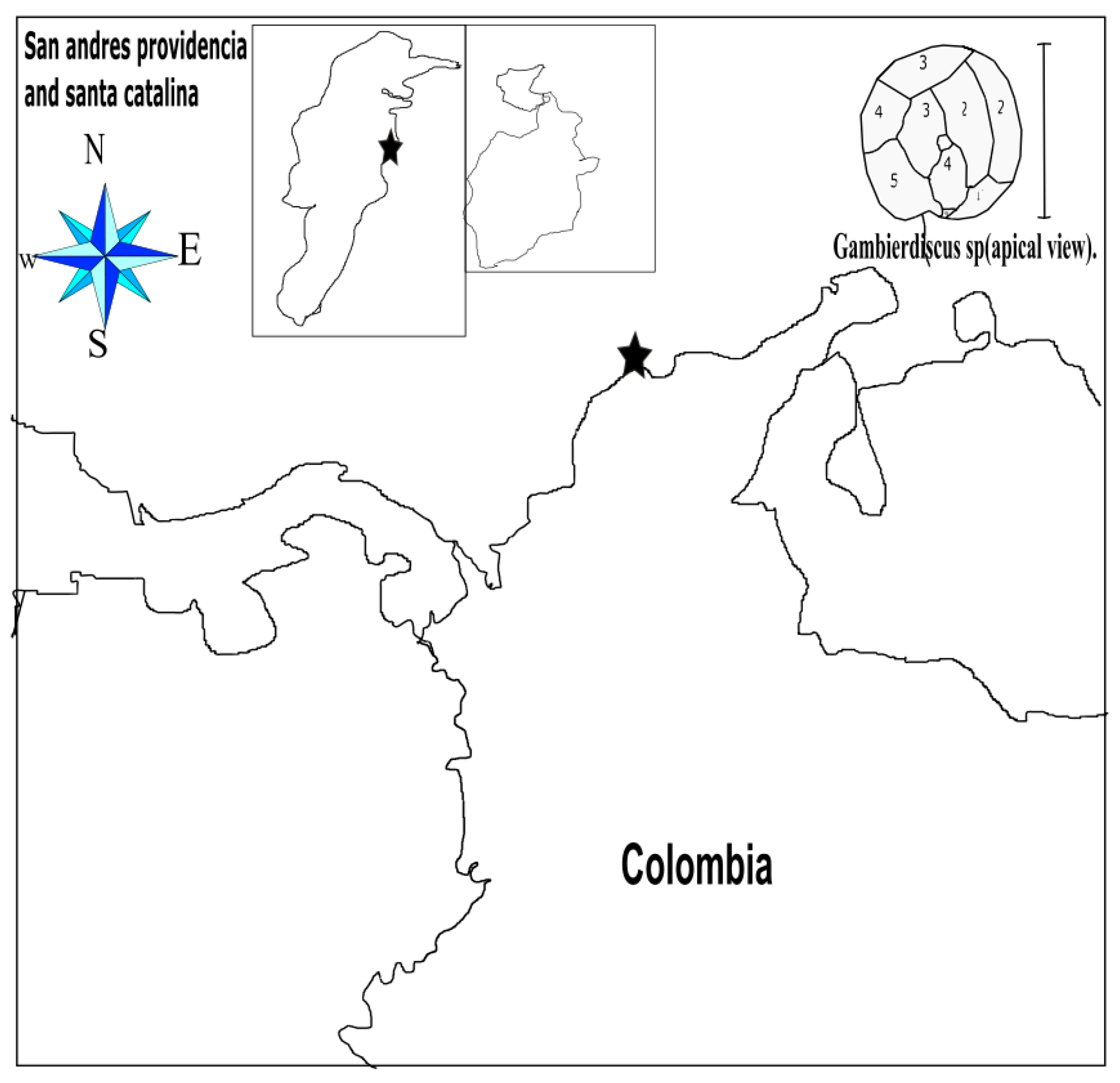
1.2. Distribution of Dinoflagellates Associated with Ciguatoxin in the Colombian Coasts
2. Pathophysiology
2.1. Clinical Manifestations
2.2. Diagnosis
2.3. Differential Diagnoses
3. Treatment
3.1. Acute Management
3.2. Chronic Management
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Friedman, M.A.; Fernández, M.; Backer, L.C.; Dickey, R.W.; Bernstein, J.; Schrank, K.; Kibler, S.; Stephan, W.; Gribble, M.O.; Bienfang, P.; et al. An Updated Review of Ciguatera Fish Poisoning: Clinical, Epidemiological, Environmental, and Public Health Management. Mar. Drugs 2017, 15, 72. [Google Scholar] [CrossRef]
- Van Dolah, F.M.; Morey, J.S.; Milne, S.; Ung, A.; Anderson, P.E.; Chinain, M. Transcriptomic analysis of polyketide synthases in a highly ciguatoxic dinoflagellate, Gambierdiscus polynesiensis and low toxicity Gambierdiscus pacificus, from French Polynesia. PLoS ONE 2020, 15, e0231400. [Google Scholar] [CrossRef] [Green Version]
- Gòmez, A.R.; Mancera-Pineda, J.E. Potentially Toxic Dinoflagellates Associated to Seagrass on Isla de Barú, Colombian Caribbean, During El Niño. Acta Biológica Colomb. 2019, 24, 109–117. [Google Scholar] [CrossRef]
- Scheuer, P.J.; Takahashi, W.; Tsutsumi, J.; Yoshida, T. Ciguatoxin: Isolation and Chemical Nature. Science 1967, 155, 1267–1268. [Google Scholar] [CrossRef]
- Murata, M.; Legrand, A.M.; Ishibashi, Y.; Yasumoto, T. Structures of ciguatoxin and its congener. J. Am. Chem. Soc. 1989, 111, 8929–8931. [Google Scholar] [CrossRef]
- Lewis, R.J.; Vernoux, J.-P.; Brereton, I.M. Structure of Caribbean Ciguatoxin Isolated from Caranx latus. J. Am. Chem. Soc. 1998, 120, 5914–5920. [Google Scholar] [CrossRef]
- Celis, J.S.; Pineda, J.E.M. Análisis Histórico de la Incidencia de Ciguatera en las Islas del Caribe Durante 31 Años: 1980–2010. Bull. Mar. Coast. Res. 2016, 44, 44. [Google Scholar] [CrossRef]
- Alvarez, R. Primer caso de ciguatera en el caribe colombiano por Seriola zonata (Mitchill, 181 5) (Pisces: Carangidae). Biomédica 1997, 17, 67. [Google Scholar] [CrossRef]
- Yasumoto, T.; Igarashi, T.; Legrand, A.-M.; Cruchet, P.; Chinain, M.; Fujita, T.; Naoki, H. Structural Elucidation of Ciguatoxin Congeners by Fast-Atom Bombardment Tandem Mass Spectroscopy. J. Am. Chem. Soc. 2000, 122, 4988–4989. [Google Scholar] [CrossRef]
- Mancera-Pineda, J.E.; Montalvo-Talaigua, M.; Gavio, B. Dinoflagelados potencialmente tóxicos asociados a material orgánico flotante (drift) en San Andrés Isla, Reserva Internacional de la Biosfera-Seaflower: Potentially toxic dinoflagellates associated to drift in San Andrés Island, International Biosphere Reservation-Seaflower. Caldasia 2014, 36, 139–156. [Google Scholar]
- Rodriguez, E.A.; Mancera-Pineda, J.E.; Gavio, B. Survey of Benthic dinoflagellatesassociated to beds of Thalassia testudinumin san andrés island, seaflower biosphere reserve, Caribbean Colombia. Acta Biológica Colomb. 2010, 15, 229–246. [Google Scholar]
- Espitia, J.D.G. Ictiotoxismo por consumo de barracuda (Sphyraena barracuda) y morena manchada (Gymnothorax moringa) en la comunidad de pescadores artesanales de Tasajera, Caribe colombiano. Duazary 2007, 4, 160–167. [Google Scholar] [CrossRef]
- Ramos, B.; Edith, M. Asociación entre la Temperatura Ambiental y Temperatura Superficial del Mar sobre la Aparición de Casos de Ciguatera en el Departamento de San Andrés y Providencia. Master’s Thesis, Francisco José de Caldas District University, Bogotá, Colombia, 2015. [Google Scholar]
- Kibler, S.R.; Davenport, E.D.; Tester, P.A.; Hardison, D.R.; Holland, W.C.; Litaker, R.W. Gambierdiscus and Fukuyoa species in the greater Caribbean: Regional growth projections for ciguatera-associated dinoflagellates. Ecol. Model. 2017, 360, 204–218. [Google Scholar] [CrossRef]
- Uribe, A.G.; Martínez, M.L.O.; Quijada, H.; Durán, M.E.M. Perfil epidemiológico de las intoxicaciones por sustancias químicas en Colombia. Inf. Quinc. Epidemiológico Nac. 2013, 22, 24. [Google Scholar]
- Rhodes, L.L.; Smith, K.F.; Murray, J.S.; Nishimura, T.; Finch, S.C. Ciguatera Fish Poisoning: The Risk from an Aotearoa/New Zealand Perspective. Toxins 2020, 12, 50. [Google Scholar] [CrossRef] [Green Version]
- Yan, M.; Mak, M.Y.L.; Cheng, J.; Li, J.; Gu, J.R.; Leung, P.T.Y.; Lam, P.K.S. Effects of dietary exposure to ciguatoxin P-CTX-1 on the reproductive performance in marine medaka (Oryzias melastigma). Mar. Pollut. Bull. 2020, 152, 110837. [Google Scholar] [CrossRef]
- Soliño, L.; Costa, P.R. Global impact of ciguatoxins and ciguatera fish poisoning on fish, fisheries and consumers. Environ. Res. 2020, 182, 109111. [Google Scholar] [CrossRef]
- Sanchez-Henao, J.A.; García-Álvarez, N.; Fernández, A.; Saavedra, P.; Silva Sergent, F.; Padilla, D.; Acosta-Hernández, B.; Martel Suárez, M.; Diogène, J.; Real, F. Predictive score and probability of CTX-like toxicity in fish samples from the official control of ciguatera in the Canary Islands. Sci. Total Environ. 2019, 673, 576–584. [Google Scholar] [CrossRef]
- Meyer, L.; Capper, A.; Carter, S.; Simpfendorfer, C. An investigation into ciguatoxin bioaccumulation in sharks. Toxicon Off. J. Int. Soc. Toxinol. 2016, 119, 234–243. [Google Scholar] [CrossRef]
- Magalhães, V.F.; Marinho, M.M.; Domingos, P.; Oliveira, A.C.; Costa, S.M.; Azevedo, L.O.; Azevedo, S.M.F.O. Microcystins (cyanobacteria hepatotoxins) bioaccumulation in fish and crustaceans from Sepetiba Bay (Brasil, RJ). Toxicon 2003, 42, 289–295. [Google Scholar] [CrossRef]
- Alavarado, D.A.; Vera, J.M.R. Dynamics of the bioaccumulation of ciguatoxins in a food chain. Rev. Cuba. Investig. Biomed. 2013, 32, 271–283. [Google Scholar]
- Palafox, N.A.; Buenconsejo-Lum, L.E. Ciguatera Fish Poisoning: Review of Clinical Manifestations. J. Toxicol. Toxin Rev. 2001, 20, 141–160. [Google Scholar] [CrossRef]
- Clinical Observations on 3,009 Cases of Ciguatera (Fish Poisoning) in the South Pacific—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/574366/ (accessed on 15 June 2020).
- Skinner, M.P.; Brewer, T.D.; Johnstone, R.; Fleming, L.E.; Lewis, R.J. Ciguatera Fish Poisoning in the Pacific Islands (1998 to 2008). PLoS Negl. Trop. Dis. 2011, 5. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, D.N. Ciguatera Fish Poisoning in Miami. JAMA J. Am. Med. Assoc. 1980, 244, 254. [Google Scholar] [CrossRef]
- Sims, J.K. A theoretical discourse on the pharmacology of toxic marine ingestions. Ann. Emerg. Med. 1987, 16, 1006–1015. [Google Scholar] [CrossRef]
- Edwards, A.; Zammit, A.; Farrell, H. Four recent ciguatera fish poisoning incidents in New South Wales, Australia linked to imported fish. Commun. Dis. Intell. 2019, 43. [Google Scholar] [CrossRef]
- Friedemann, M. Ciguatera fish poisoning outbreaks from 2012 to 2017 in Germany caused by snappers from India, Indonesia, and Vietnam. J. Consum. Prot. Food Saf. 2019, 14, 71–80. [Google Scholar] [CrossRef]
- Neves Junior, C.K.; Goldani, L.Z.; Neves Junior, C.K.; Goldani, L.Z. Ciguatera fish poisoning in Brazilian traveler to Caribbean. Braz. J. Infect. Dis. 2019, 23, 200–202. [Google Scholar] [CrossRef]
- Ortega Chavarría, M.J.; Alcocer Delgado, D.; Diaz Greene, E.J.; Rodríguez Weber, F.L. Ciguatera poisoning: Infectious cause neuropathy. Acta Médica Grupo Ángeles 2019, 17, 268–271. [Google Scholar]
- Raman, R.; Coppes, S.; Hellingman, T.; Laclé, C. Junctional bradycardia caused by ciguatera intoxication. BMJ Case Rep. 2019, 12, e229354. [Google Scholar] [CrossRef]
- Chinain, M.; Gatti, C.M.; Roué, M.; Darius, H.T. Ciguatera poisoning in French Polynesia: Insights into the novel trends of an ancient disease. New Microbes New Infect. 2019, 31. [Google Scholar] [CrossRef] [PubMed]
- Asaeda, G. The transport of ciguatoxin: A case report11Selected Topics: Toxicology is coordinated by Kenneth Kulig, MD, of Denver, Colorado. J. Emerg. Med. 2001, 20, 263–265. [Google Scholar] [CrossRef]
- Farrell, H.; Zammit, A.; Manning, J.; Shadbolt, C.; Szabo, L.; Harwood, D.T.; McNabb, P.; Turahui, J.A.; van den Berg, D.J. Clinical diagnosis and chemical confirmation of ciguatera fish poisoning in New South Wales, Australia. Commun. Dis. Intell. Q. Rep. 2016, 40, E1–E6. [Google Scholar]
- Milaciu, M.V.; Ciumărnean, L.; Orășan, O.H.; Para, I.; Alexescu, T.; Negrean, V. Semiology of food poisoning. HVM Bioflux 2016, 8, 108–113. [Google Scholar]
- Caillaud, A.; de la Iglesia, P.; Darius, H.T.; Pauillac, S.; Aligizaki, K.; Fraga, S.; Chinain, M.; Diogène, J. Update on Methodologies Available for Ciguatoxin Determination: Perspectives to Confront the Onset of Ciguatera Fish Poisoning in Europe. Mar. Drugs 2010, 8, 1838–1907. [Google Scholar] [CrossRef]
- Satake, M.; Fukui, M.; Legrand, A.-M.; Cruchet, P.; Yasumoto, T. Isolation and structures of new ciguatoxin analogs, 2,3-dihydroxyCTX3C and 51-hydroxyCTX3C, accumulated in tropical reef fish. Tetrahedron Lett. 1998, 39, 1197–1198. [Google Scholar] [CrossRef]
- Tsumuraya, T.; Hirama, M. Rationally Designed Synthetic Haptens to Generate Anti-Ciguatoxin Monoclonal Antibodies, and Development of a Practical Sandwich ELISA to Detect Ciguatoxins. Toxins 2019, 11, 533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodero, M.; Gerssen, A.; Portier, L.; Klijnstra, M.D.; Hoogenboom, R.L.A.P.; Guzmán, L.; Hendriksen, P.J.M.; Bovee, T.F.H. A Strategy to Replace the Mouse Bioassay for Detecting and Identifying Lipophilic Marine Biotoxins by Combining the Neuro-2a Bioassay and LC-MS/MS Analysis. Mar. Drugs 2018, 16, 501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humpage, A.; Magalhaes, V.; Froscio, S. Comparison of analytical tools and biological assays for detection of paralytic shellfish poisoning toxins. Anal. Bioanal. Chem. 2010, 397, 1655–1671. [Google Scholar] [CrossRef] [PubMed]
- Raikhlin-Eisenkraft, B.; Bentur, Y. Rabbitfish (“aras”): An unusual source of ciguatera poisoning. Isr. Med. Assoc. J. Imaj. 2002, 4, 28–30. [Google Scholar]
- Saraya, A.; Sintunawa, C.; Wacharapluesadee, S.; Swangpun, K.; Dumrongchua, S.; Wilde, H.; Hemachudha, T. Marine Fish Toxins in Thailand: Report of 6 Suspected Ciguatera Cases. Case Rep. Clin. Med. 2014, 2014. [Google Scholar] [CrossRef] [Green Version]
- Álvarez Rivero, V.; Cervantes Zorrilla, R.; Lorea Cárdenas-Hernández, M.; González-Chávez, M.A. Scombroidosis. Acta Médica Grupo Ángeles 2018, 16, 63–65. [Google Scholar]
- Gillespie, N.C.; Lewis, R.J.; Holmes, M.J.; Bourke, J.B.; Pearn, J.H.; Bourke, A.T.C.; Shields, W.J. Ciguatera in Australia: Occurrence, clinical features, pathophysiology and management. Med. J. Aust. 1986, 145, 584–590. [Google Scholar] [CrossRef]
- Friedman, M.A.; Fleming, L.E.; Fernandez, M.; Bienfang, P.; Schrank, K.; Dickey, R.; Bottein, M.-Y.; Backer, L.; Ayyar, R.; Weisman, R.; et al. Ciguatera Fish Poisoning: Treatment, Prevention and Management. Mar. Drugs 2008, 6, 456–479. [Google Scholar] [CrossRef]
- Palafox, N.A.; Jain, L.G.; Pinano, A.Z.; Gulick, T.M.; Williams, R.K.; Schatz, I.J. Successful Treatment of Ciguatera Fish Poisoning With Intravenous Mannitol. JAMA 1988, 259, 2740–2742. [Google Scholar] [CrossRef]
- Pearn, J.H.; Lewis, R.J.; Ruff, T.; Tait, M.; Quinn, J.; Murtha, W.; King, G.; Mallett, A.; Gillespie, N.C. Ciguatera and Mannitol: Experience with a New Treatment Regimen. Available online: https://pubmed.ncbi.nlm.nih.gov/2500582/ (accessed on 18 September 2020).
- Bourdy, G.; Cabalion, P.; Amade, P.; Laurent, D. Traditional remedies used in the Western Pacific for the treatment of ciguatera poisoning. J. Ethnopharmacol. 1992, 36, 163–174. [Google Scholar] [CrossRef] [Green Version]
- Chan, T.Y.K. Severe bradycardia and prolonged hypotension in ciguatera. Singap. Med. J. 2013, 54, e120–e122. [Google Scholar] [CrossRef] [Green Version]
- Chateau-Degat, M.-L.; Huin-Blondey, M.-O.; Chinain, M.; Darius, T.; Legrand, A.-M.; Nguyen, N.L.; Laudon, F.; Chansin, R.; Dewailly, E. Prevalence of Chronic Symptoms of Ciguatera Disease in French Polynesian Adults. Am. J. Trop. Med. Hyg. 2007, 77, 842–846. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Year | Number of Shoots | Number of Cases Associated with Outbreaks | Number of Isolated Cases | Total |
|---|---|---|---|---|
| 1968 | 1 | 28 | 0 | 28 |
| 1984 | 1 | 15 | 0 | 15 |
| 1994 | 1 | 7 | 0 | 7 |
| 1997 | 2 | 25 | 0 | 25 |
| 2005 | 1 | 7 | 0 | 7 |
| 2007 | 2 | 25 | 0 | 25 |
| 2010 | 5 | 28 | 0 | 28 |
| 2011 | 1 | 9 | 0 | 9 |
| 2012 | 3 | 12 | 2 | 14 |
| 2013 | 9 | 30 | 3 | 33 |
| 2014 | 3 | 8 | 9 | 17 |
| 2015 | 1 | 30 | 0 | 30 |
| Total | 30 | 224 | 14 | 238 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro Quiroz, R.; Herrera-Usuga, J.C.; Osorio-Ospina, L.M.; Garcia-Pertuz, K.M.; Navarro Quiroz, E. Epidemiology and Toxicology of Ciguatera Poisoning in the Colombian Caribbean. Mar. Drugs 2020, 18, 504. https://doi.org/10.3390/md18100504
Navarro Quiroz R, Herrera-Usuga JC, Osorio-Ospina LM, Garcia-Pertuz KM, Navarro Quiroz E. Epidemiology and Toxicology of Ciguatera Poisoning in the Colombian Caribbean. Marine Drugs. 2020; 18(10):504. https://doi.org/10.3390/md18100504
Chicago/Turabian StyleNavarro Quiroz, Roberto, Juan Carlos Herrera-Usuga, Laura Maria Osorio-Ospina, Katia Margarita Garcia-Pertuz, and Elkin Navarro Quiroz. 2020. "Epidemiology and Toxicology of Ciguatera Poisoning in the Colombian Caribbean" Marine Drugs 18, no. 10: 504. https://doi.org/10.3390/md18100504