

Medical Ozone: A Redox Regulator with Selectivity for Rheumatoid Arthritis Patients
 , ,
, ,
Abstract
:1. Introduction
2. Results
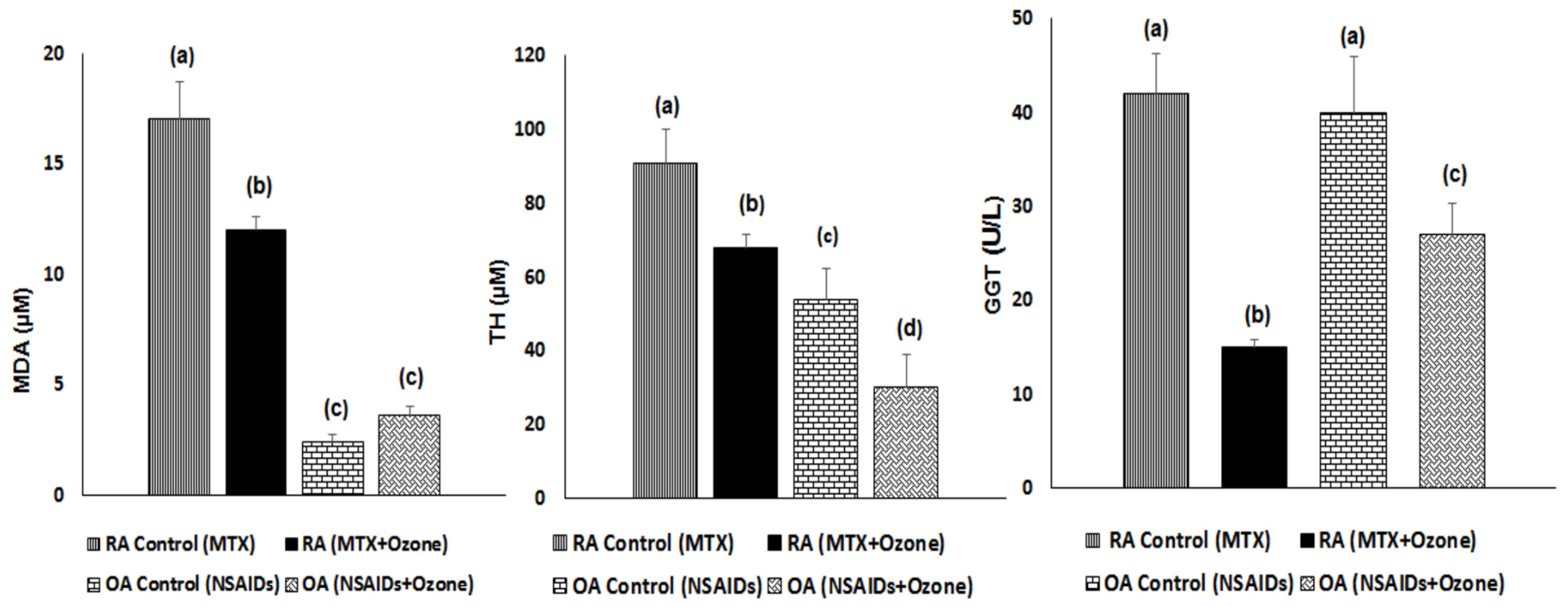
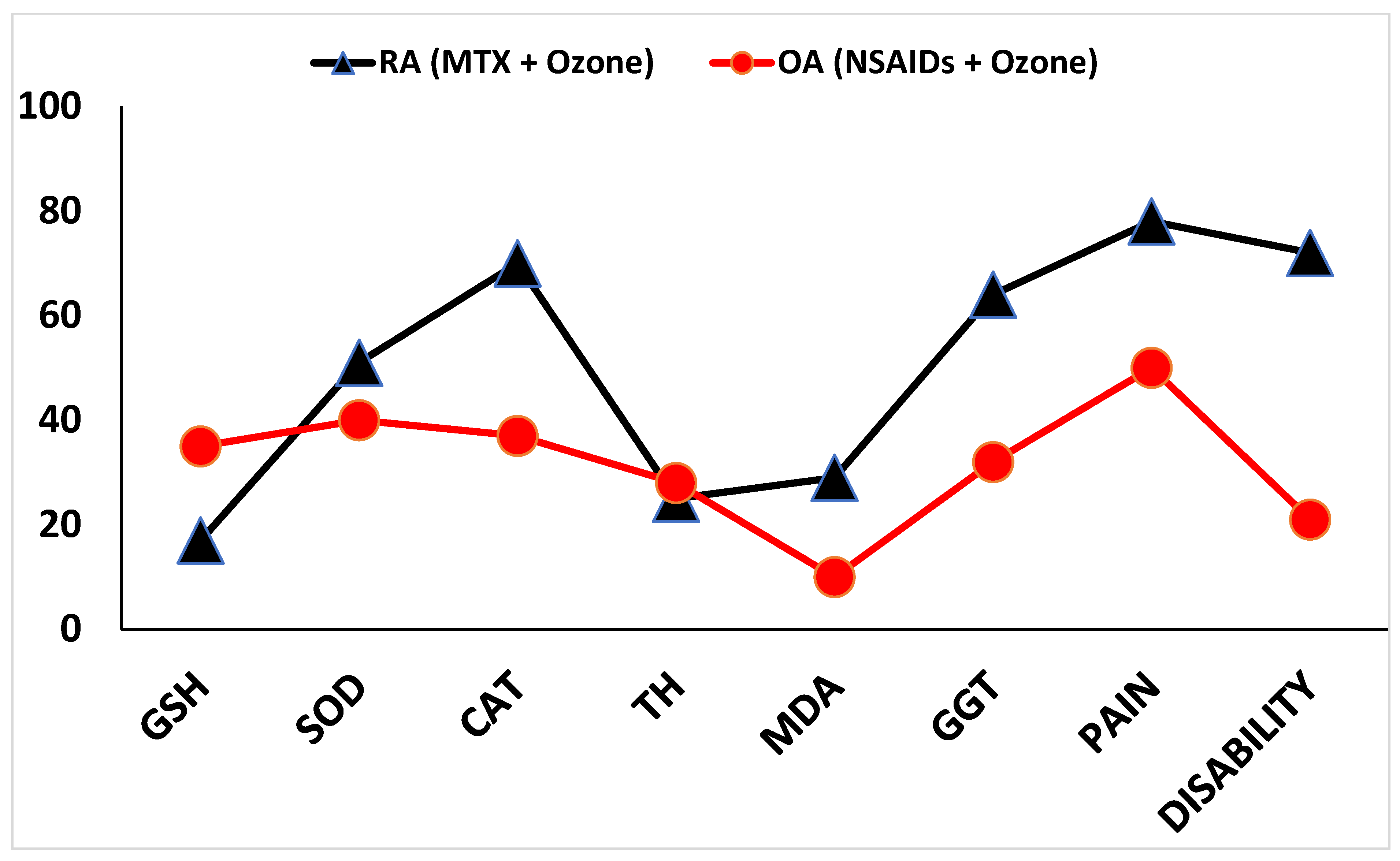
2.1. Antioxidant Defenses and Injury Biomarkers in RA and OA Patients
2.2. Pain, Disability, and Anti-Cylic Citrullinate Peptide Levels in RA and OA Patients
3. Discussion
4. Material and Methods
4.1. Study Design
4.2. Inclusion and Exclusion Criteria
4.2.1. For Rheumatoid Arthritis
4.2.2. For Osteoarthritis
4.2.3. Evaluation of Activity in Both Diseases
4.3. Biochemical Determinations
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ARs | Adenosine receptors |
| A2AR | Subtype 2A adenosine receptor |
| A2BR | Subtype 2B adenosine receptor |
| A3R | A3 Adenosine receptor |
| Ado | Adenosine |
| Anti-CCP | Anti-Cylic Citrullinate Peptides |
| CCPA | 8 cyclopentyl-1,3-dipropylxanthine |
| CAT | Catalase activity |
| ELISA | Enzyme-linked immunosorbent assay |
| DAS-28 | Disease Activity Score 28 |
| DMARDs | Disease-modifying antirheumatic drugs |
| DPCPX | 2-chloro-N6-cyclopentyladenosine |
| GSH | Reduced glutathione |
| GGT | γ glutamyl transferase |
| GSSG | Oxidized glutathione |
| HAQ-Di | Health Assessment Questionnaire-Disability Index |
| H2O2 | Hydrogen peroxide |
| MDA | Malondialdehyde |
| MTX | Methotrexate |
| Nox | NADPH oxidase subunit |
| NSAIDs | Non-steroidal anti-inflammatory drugs |
| NF-κB | Nuclear factor kappa B |
| Nrf2 | Erythroid 2-related factor 2 |
| OA | Osteoarthritis |
| ·OH | Hydroxyl radical |
| PTZ | Pentylenetetrazole |
| RA | Rheumatoid arthritis |
| ROS | Reactive Oxygen Species |
| SOD | Superoxide dismutase activity |
| TH | Total Hydroperoxide |
References
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the global burden of disease study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed]
- Myasoedova, E.; Crowson, C.S.; Turesson, C.; Gabriel, S.E.; Matteson, E.L. Incidence of extraarticular rheumatoid arthritis in Olmsted County, Minnesota, in 1995–2007 versus 1985–1994: A population-based study. J. Rheumatol. 2011, 38, 983–989. [Google Scholar] [CrossRef] [PubMed]
- Hootman, J.M.; Helmick, C.G. Projections of US prevalence of arthritis and associated activity limitations. Arthritis Rheum. 2006, 54, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.; Dai, C.; Wang, L.; Pan, X. Potential biomarkers that discriminate rheumatoid arthritis and osteoarthritis based on the analysis and validation of datasets. BMC Musculoskelet. Disord. 2022, 23, 319. [Google Scholar] [CrossRef]
- Kim, G.M.; Park, H.; Lee, S.Y. Roles of osteoclast-associated receptor in rheumatoid arthritis and osteoarthritis. Jt. Bone Spine 2022, 89, 105400. [Google Scholar] [CrossRef]
- Guo, Q.; Wang, Y.; Xu, D.; Nossent, J.; Pavlos, N.J.; Xu, J. Rheumatoid arthritis: Pathological mechanisms and modern pharmacologic therapies. Bone Res. 2018, 6, 15. [Google Scholar] [CrossRef]
- Saalfeld, W.; Mixon, A.M.; Zelie, J.; Lydon, E.J. Differentiating Psoriatic Arthritis from Osteoarthritis and Rheumatoid Arthritis: A Narrative Review and Guide for Advanced Practice Providers. Rheumatol. Ther. 2021, 8, 1493–1517. [Google Scholar] [CrossRef]
- Bullock, J.; Rizvi, S.A.; Saleh, A.M.; Ahmed, S.S.; Do, D.P.; Ansari, R.A.; Ahmed, J. Rheumatoid arthritis: A brief overview of the treatment. Med. Princ. Pract. 2018, 27, 501–507. [Google Scholar] [CrossRef]
- Katz, J.N.; Arant, K.R.; Loeser, R.F. Diagnosis and treatment of hip and knee osteoarthritis: A review. JAMA 2021, 325, 568–578. [Google Scholar] [CrossRef]
- Rodríguez-Vargas, G.-S.; Santos-Moreno, P.; Rubio-Rubio, J.-A.; Bautista-Niño, P.-K.; Echeverri, D.; Gutiérrez-Castañeda, L.-D.; Sierra-Matamoros, F.; Navarrete, S.; Aparicio, A.; Saenz, L.; et al. Vascular Age, Metabolic Panel, Cardiovascular Risk and Inflammaging in Patients with Rheumatoid Arthritis Compared with Patients with Osteoarthritis. Front. Cardiovasc. Med. 2022, 9, 894577. [Google Scholar] [CrossRef]
- Conti, V.; Corbi, G.; Costantino, M.; De Bellis, E.; Manzo, V.; Sellitto, C.; Stefanelli, B.; Colucci, F.; Filippelli, A. Biomarkers to Personalize the Treatment of Rheumatoid Arthritis: Focus on Autoantibodies and Pharmacogenetics. Biomolecules 2020, 10, 1672. [Google Scholar] [CrossRef] [PubMed]
- León, O.S.; Menéndez, S.; Merino, N.; Castillo, R.; Sam, S.; Pérez, L.; Cruz, E.; Bocci, V. Ozone oxidative preconditioning: A protection against cellular damage by free radicals. Mediat. Inflamm. 1998, 7, 289–294. [Google Scholar] [CrossRef] [PubMed]
- León, O.S. Ozone Therapy. Oxidative Condition. Basis for Its Clinical Effectiveness, 1st ed.; ODREI: Freudenstadt, Germany, 2014; pp. 1–202. [Google Scholar]
- Fernández, O.S.L.; Viebahn-Haensler, R.; Cabreja, G.L.; Espinosa, I.S.; Matos, Y.H.; Roche, L.D.; Santos, B.T.; Oru, G.T.; Vega, J.C.P. Medical ozone increases methotrexate clinical response and improves cellular redox balance in patients with rheumatoid arthritis. Eur. J. Pharmacol. 2016, 789, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, I.N.; Pratt, C.; Gorelik, A.; Liew, D. Projected Burden of Osteoarthritis and Rheumatoid Arthritis in Australia: A Population-Level Analysis. Arthritis Care Res. 2018, 70, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Eldjoudi, D.A.; Barreal, A.C.; Gonzalez-Rodríguez, M.; Ruiz-Fernández, C.; Farrag, Y.; Farrag, M.; Lago, F.; Capuozzo, M.; Gonzalez-Gay, M.A.; Varela, A.M.; et al. Leptin in Osteoarthritis and Rheumatoid Arthritis: Player or Bystander? Int. J. Mol. Sci. 2022, 23, 2859. [Google Scholar] [CrossRef] [PubMed]
- Pulik, Ł.; Łęgosz, P.; Motyl, G. Matrix metalloproteinases in rheumatoid arthritis and osteoarthritis: A state of the art review. Rheumatology 2023, 61, 191–201. [Google Scholar] [CrossRef]
- Sohn, R.; Junker, M.; Meurer, A.; Zaucke, F.; Straub, R.H.; Jenei-Lanzl, Z. Anti-Inflammatory Effects of Endogenously Released Adenosine in Synovial Cells of Osteoarthritis and Rheumatoid Arthritis Patients. Int. J. Mol. Sci. 2021, 22, 8956. [Google Scholar] [CrossRef]
- Thiele, G.M.; Duryee, M.J.; Hunter, C.D.; England, B.R.; Fletcher, B.S.; Daubach, E.C.; Pospisil, T.P.; Klassen, L.W.; Mikuls, T.R. Immunogenic and Inflammatory Responses to Citrullinated Proteins Are Enhanced Following Modification with Malondialdehyde-Acetaldehyde Adducts. Int. Immunopharmacol. 2020, 83, 106433. [Google Scholar] [CrossRef]
- Ndrepepa, G.; Kastrati, A. Gamma-glutamyl transferase and cardiovascular disease. Ann. Transl. Med. 2016, 4, 481. [Google Scholar] [CrossRef]
- Ballatori, N.; Krance, S.M.; Notenboom, S.; Shi, S.; Tieu, K.; Hammond, C.L. Glutathione dysregulation and the etiology and progression of human diseases. Biol. Chem. 2009, 390, 191–214. [Google Scholar] [CrossRef]
- Pasquini, S.; Contri, C.; Borea, P.A.; Vincenzi, F.; Varani, K. Adenosine and Inflammation: Here, There and Everywhere. Int. J. Mol. Sci. 2021, 22, 7685. [Google Scholar] [CrossRef] [PubMed]
- Brigelius-Flohé, R.; Flohé, L. Basic Principles and Emerging Concepts in the Redox Control of Transcription Factors. Antioxid. Redox Signal. 2011, 15, 2335–2381. [Google Scholar] [CrossRef]
- León Fernández, O.S.; Ajamieh, H.H.; Berlanga, J.; Menendez, S.; Viebahn-Hánsler, R.; Re, L.; Carmona, A.M. Ozone oxidative preconditioning is mediated by A1 adenosine receptors in a rat model of liver ischemia/ reperfusion. Tansplantation 2008, 21, 39–48. [Google Scholar]
- Galiè, M.; Covi, V.; Tabaracci, G.; Malatesta, M. The Role of Nrf2 in the Antioxidant Cellular Response to Medical Ozone Exposure. Int. J. Mol. Sci. 2019, 20, 4009. [Google Scholar] [CrossRef]
- Vaillant, J.D.; Fraga, A.; Díaz, M.T.; Mallok, A.; Viebahn-Hänsler, R.; Fahmy, Z.; Barberá, A.; Delgado, L.; Menéndez, S.; Fernández, O.S.L. Ozone oxidative postconditioning ameliorates joint damage and decreases pro-inflammatory cytokine levels and oxidative stress in PG/PS-induced arthritis in rats. Eur. J. Pharmacol. 2013, 714, 318–324. [Google Scholar] [CrossRef]
- Hao, W.T.; Huang, L.; Pan, W.; Le Ren, Y. Antioxidant glutathione inhibits inflammation in synovial fibroblasts via PTEN/PI3K/AKT pathway: An in vitro study. Arch. Rheumatol. 2022, 37, 212–222. [Google Scholar] [CrossRef]
- Viebahn-Haensler, R.; Fernández, O.S.L. Ozone in Medicine. The Low-Dose Ozone Concept and Its Basic Biochemical Mechanisms of Action in Chronic Inflammatory Diseases. Int. J. Mol. Sci. 2021, 22, 7890. [Google Scholar] [CrossRef]
- Oru, G.T.; Viebhan-Haensler, R.; Cabreja, G.L.; Espinosa, I.S.; Santos, B.T.; Vega, J.C.P.; Cintas, S.S.; Fernández, O.S.L. Medical Ozone Reduces the Risk of γ-Glutamyl Transferase and Alkaline Phosphatase Abnormalities and Oxidative Stress in Rheumatoid Arthritis Patients Treated with Methotrexate. SM J. Arthritis Res. 2017, 1, 1004. [Google Scholar] [CrossRef]
- Fernandez, O.S.L.; Oru, G.T.; Vega, J.C.P.; Fernandez, E.G.; Viebahn-Hänsler, R.; Torres-Carballeira, R.; Cabreja, G.L.; Mendez, R.M. Ozone + Arthroscopy: Improved Redox Status, Function and Surgical Outcome in Knee Osteoarthritis Patients. Int. J. Innov. Surg. 2020, 3, 1011. [Google Scholar]
- Zhang, H.; Liu, H.; Iles, K.E.; Liu, R.-M.; Postlethwait, E.M.; Laperche, Y.; Forman, H.J. 4-Hydroxynonenal Induces Rat γ-Glutamyl Transpeptidase through Mitogen-Activated Protein Kinase–Mediated Electrophile Response Element/Nuclear Factor Erythroid 2–Related Factor 2 Signaling. Am. J. Respir. Cell Mol. Biol. 2006, 34, 174–181. [Google Scholar] [CrossRef]
- Liao, W.; Yang, Y.; Yang, H.; Qu, Y.; Song, H.; Li, Q. Circulating gamma-glutamyl transpeptidase and risk of pancreatic cancer: A prospective cohort study in the UK Biobank. Cancer Med. 2023, 12, 7877–7887. [Google Scholar] [CrossRef]
- Lee, Y.; Seo, J.H. Potential Causal Association between Elevated Gamma-Glutamyl Transferase Level and Stroke: A Two-Sample Mendelian Randomization Study. Biomolecules 2023, 13, 1592. [Google Scholar] [CrossRef]
- Kim, D.; Kim, J.H.; Lee, H.; Hong, I.; Chang, Y.; Song, T.-J. Association of gamma-glutamyl transferase variability with risk of osteoporotic fractures: A nationwide cohort study. PLoS ONE 2023, 18, e0277452. [Google Scholar] [CrossRef]
- Margis, R.; Dunand, C.; Teixeira, F.K.; Margis-Pinheiro, M. Glutathione peroxidase family—An evolutionary overview. FEBS J. 2008, 275, 3959–3970. [Google Scholar] [CrossRef]
- Kondo, N.; Kanai, T.; Okada, M. Rheumatoid Arthritis and Reactive Oxygen Species: A Review. Curr. Issues Mol. Biol. 2023, 45, 3000–3015. [Google Scholar] [CrossRef]
- Mishra, R.; Singh, A.; Chandra, V.; Negi, M.P.S.; Tripathy, B.C.; Prakash, J.; Gupta, V. A comparative analysis of serological parameters and oxidative stress in osteoarthritis and rheumatoid arthritis. Rheumatol. Int. 2012, 32, 2377–2382. [Google Scholar] [CrossRef] [PubMed]
- Peralta, C.; Xaus, C.; Bartrons, R.; Leon, O.; Gelpi, E.; Roselló-Catafau, J. Effect of ozone treatment on reactive oxygen species and adenosine production during hepatic ischemia-reperfusion. Free. Radic. Res. 2000, 33, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Effendi, W.I.; Nagano, T.; Kobayashi, K.; Nishimura, Y. Focusing on Adenosine Receptors as a Potential Targeted Therapy in Human Diseases. Cells 2020, 9, 785. [Google Scholar] [CrossRef] [PubMed]
- Ajamieh, H.H.; Berlanga, J.; Merino, N.; Sanchez, G.M.; Carmona, A.M.; Cepero, S.M.; Giuliani, A.; Re, L.; Leon, O.S. Role of protein synthesis in the protection conferred by ozone-oxidative-preconditioning in hepatic ischaemia/reperfusion. Transpl. Int. 2005, 18, 604–612. [Google Scholar] [CrossRef]
- Oru, G.T.; Viebhan-Haensler, R.; Matos, Y.H.; Díaz, D.; Rodríguez, M.C.O.; Fernández, O.S.L. Medical ozone prevents inflammatory effects from carrageenan-induced knee joint synovitis in rats through A1 adenosine receptor, as well as lipid and protein oxidative damages. J. Sci. Res. Stud. 2018, 5, 65–72. [Google Scholar]
- Mallok, A.; Vaillant, J.D.; Soto, M.T.D.; Viebahn-Hänsler, R.; Viart, M.d.L.A.B.; Pérez, A.F.; Cedeño, R.I.D.; Fernández, O.S.L. Ozone protective effects against PTZ-induced generalized seizures are mediated by reestablishment of cellular redox balance and A1adenosine receptors. Neurol. Res. 2015, 3, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Macedo-Júnior, S.J.; Nascimento, F.P.; Luiz-Cerutti, M.; Santos, A.R.S. The role of peripheral adenosine receptors in glutamate-induced pain nociceptive behavior. Purinergic Signal. 2021, 17, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Vincenzi, F.; Pasquini, S.; Borea, P.A.; Varani, K. Targeting Adenosine Receptors: A Potential Pharmacological Avenue for Acute and Chronic Pain. Int. J. Mol. Sci. 2020, 21, 871. [Google Scholar] [CrossRef] [PubMed]
- Declaration of Helsinki, 2013, 7th Revisión. Available online: http://jama.md/H1WvEO (accessed on 20 September 2005).
- Wichmann, B.A.; Hill, I.D. Algorithm AS 183: An effcient and portable pseudo-random number generator. Appl. Stat. 1982, 31, 188–190. [Google Scholar] [CrossRef]
- McLeod, A.I. Remark AS R58: A Remark on algorithm AS 183. An efficient and portable pseudo-random number generator. J. Appl. Stat. 1985, 34, 198. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Cardiel, M.H.; Abello-Banfi, M.; Ruiz-Mercado, R.; Alarcon-Segovia, D. How to measure health status in rheumatoid arthritis in non-English speaking patients: Validation of a Spanish version of the Health Assessment Questionnaire Disability Index (Spanish HAQ-DI). Clin. Exp. Reum. 1993, 11, 117–121. [Google Scholar]
- Merino, R.J. Utilidad diagnóstica de la velocidad de sedimentación globular. Med. Integral 2002, 39, 325–329. [Google Scholar]
- Boehringer_Mannheim Biochemica Information. A Revised Biochemical Reference Source. Enzymes for Routine, 1st ed.; Boehringer Mannheim: Berlin, Germany, 1987; pp. 80–81.
- Sedlak, J.; Lindsay, R.H. Estimation of total protein-bound and nonprotein sulfhydryl groups in tissue with Ellman’s reagent. Anal. Biochem. 1968, 25, 192–205. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Data/Patient Histories | Rheumatoid Arthritis (RA) | Osteoarthritis (OA) | |||
|---|---|---|---|---|---|
| Groups | Control (MTX) (n = 20) | MTX + Ozone (n = 20) | Control (NSAIDs) (n = 20) | NSAIDs + Ozone (n = 20) | |
| Women (n/%) | 13/65 | 14/70 | 15/75 | 17/88 | |
| Men (n/%) | 7/35 | 6/30 | 5/25 | 3/12 | |
| Age (years) | 53 ± 8 (a) | 57 ± 7 (a) | 60 ± 8 (a) | 57 ± 9 (a) | |
| Osteoarthritis grading (*) | |||||
| III | - | - | 46% | 27% | |
| III–IV | - | - | 54% | 63% | |
| IV | - | - | - | 10% | |
| Previous therapy | |||||
| Methotrexate (n/%) | 20/100 | 20/100 | - | - | |
| NSAIDs | 20/100 | 20/100 | 20/100 | 20/100 | |
| Folic acid | 20/100 | 20/100 | - | - | |
| Evolution time of the | |||||
| disease (years) | 7 ± 2 (a) | 11 ± 3 (a) | 4 ± 2 (a) | 4 ± 9 (a) | |
| Ethnic origin | |||||
| Caucasian | 7/35% | 9/45% | 15/75% | 14/70% | |
| Non-Caucasian | 13/65% | 11/55% | 5/25% | 6/30% | |
| Groups | Control (MTX) | MTX + Ozone | Control (NSAIDs) | NSAIDs + Ozone | |
|---|---|---|---|---|---|
| Markers | |||||
| Pain | 5 ± 0.2 (a) | 1 ± 0.8 (b) | 6.6 ± 0.4 (c) | 3.3 ± 0.2 (d) | |
| HAQ-DI (*) | 0.6 ± 0.1 (a) | 0.16 ± 0.05 (b) | - | - | |
| Lysholm Scale (**) | - | - | 64 ± 9 (e) | 79 ± 9 (f) | |
| Anti-CCP (***) | 110 ± 9 (a) | 89 ± 8 (b) | . | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
León Fernández, O.S.; Oru, G.T.; Viebahn-Haensler, R.; López Cabreja, G.; Serrano Espinosa, I.; Corrales Vázquez, M.E. Medical Ozone: A Redox Regulator with Selectivity for Rheumatoid Arthritis Patients. Pharmaceuticals 2024, 17, 391. https://doi.org/10.3390/ph17030391
León Fernández OS, Oru GT, Viebahn-Haensler R, López Cabreja G, Serrano Espinosa I, Corrales Vázquez ME. Medical Ozone: A Redox Regulator with Selectivity for Rheumatoid Arthritis Patients. Pharmaceuticals. 2024; 17(3):391. https://doi.org/10.3390/ph17030391
Chicago/Turabian StyleLeón Fernández, Olga Sonia, Gabriel Takon Oru, Renate Viebahn-Haensler, Gilberto López Cabreja, Irainis Serrano Espinosa, and María Elena Corrales Vázquez. 2024. "Medical Ozone: A Redox Regulator with Selectivity for Rheumatoid Arthritis Patients" Pharmaceuticals 17, no. 3: 391. https://doi.org/10.3390/ph17030391