

Shared Pathogenic and Therapeutic Characteristics of Endometriosis, Adenomyosis, and Endometrial Cancer: A Comprehensive Literature Review

 ,
,  , , and
, , and
Abstract
:1. Introduction
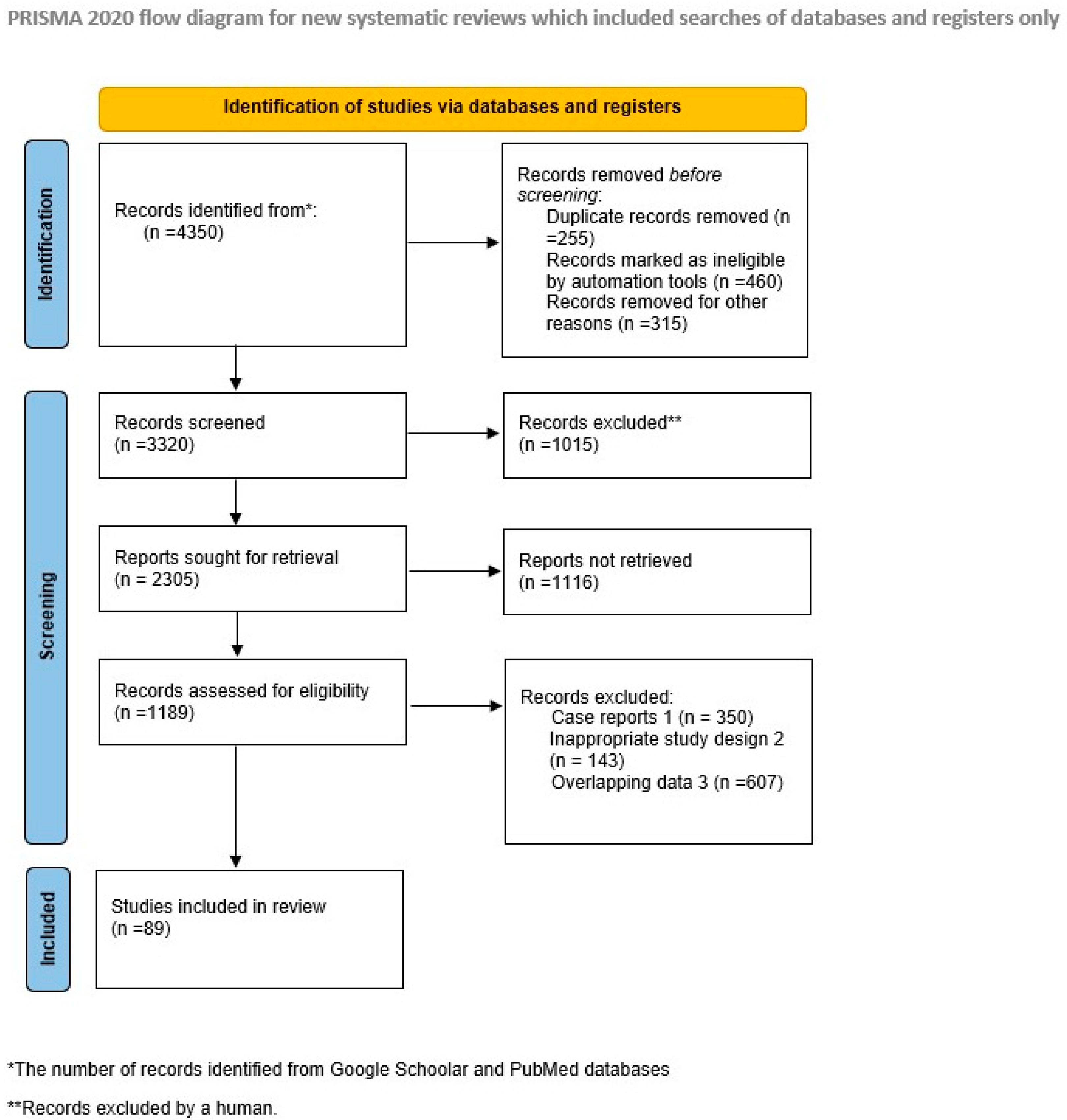
2. Materials and Methods
3. Results
3.1. Pathogenesis
3.2. Personalized Treatment for Endometriosis, Adenomyosis/Personalized Treatment studied for Endometrial Cancers with applicability in Endometriosis or Adenomyosis
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Králíčková, M.; Vetvicka, V. Endometriosis and ovarian cancer. World J. Clin. Oncol. 2014, 5, 800–805. [Google Scholar] [CrossRef]
- Vannuccini, S.; Luisi, S.; Tosti, C.; Sorbi, F.; Petraglia, F. Role of medical therapy in the management of uterine adenomyosis. Fertil. Steril. 2018, 109, 398–405. [Google Scholar] [CrossRef]
- MacLean, J.A., 2nd; Hayashi, K. Progesterone Actions and Resistance in Gynecological Disorders. Cells 2022, 11, 647. [Google Scholar] [CrossRef]
- Dai, Y.; Li, X.; Shi, J.; Leng, J. A review of the risk factors, genetics and treatment of endometriosis in Chinese women: A comparative update. Reprod. Health 2018, 15, 82. [Google Scholar] [CrossRef]
- Tosti, C.; Vannuccini, S.; Troìa, L.; Luisi, S.; Centini, G.; Lazzeri, L.; Petraglia, F. Long-Term Vaginal Danazol Treatment in Fertile Age Women with Adenomyosis. J. Endometr. Pelvic Pain Disord. 2017, 9, 39–43. [Google Scholar] [CrossRef]
- Markowska, A.; Chudecka-Głaz, A.; Pityński, K.; Baranowski, W.; Markowska, J.; Sawicki, W. Endometrial Cancer Management in Young Women. Cancers 2022, 14, 1922. [Google Scholar] [CrossRef] [PubMed]
- Brooks, R.A.; Fleming, G.F.; Lastra, R.R.; Lee, N.K.; Moroney, J.W.; Son, C.H.; Tatebe, K.; Veneris, J.L. Current recommendations and recent progress in endometrial cancer. CA Cancer J. Clin. 2019, 69, 258–279. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, A.; Bosse, T.; McAlpine, J.N. The emerging role of molecular pathology in directing the systemic treatment of endometrial cancer. Ther. Adv. Med. Oncol. 2021, 13, 17588359211035959. [Google Scholar] [CrossRef]
- Concin, N.; Creutzberg, C.L.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.A.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP Guidelines for the management of patients with endometrial carcinoma. Virchows Arch. 2021, 478, 153–190. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.W.; Groothuis, P.G. Is it time for a paradigm shift in drug research and development in endometriosis/adenomyosis? Hum. Reprod. Update 2018, 24, 577–598. [Google Scholar] [CrossRef]
- Donnez, J.; Dolmans, M.M. Endometriosis and Medical Therapy: From Progestogens to Progesterone Resistance to GnRH Antagonists: A Review. J. Clin. Med. 2021, 10, 1085. [Google Scholar] [CrossRef]
- Varma, R.; Rollason, T.; Gupta, J.K.; Maher, E.R. Endometriosis and the neoplastic process. Reproduction 2004, 127, 293–304. [Google Scholar] [CrossRef]
- Maheshwari, A.; Gurunath, S.; Fatima, F.; Bhattacharya, S. Adenomyosis and subfertility: A systematic review of prevalence, diagnosis, treatment and fertility outcomes. Hum. Reprod. Update 2012, 18, 374–392. [Google Scholar] [CrossRef]
- Dull, A.M.; Moga, M.A.; Dimienescu, O.G.; Sechel, G.; Burtea, V.; Anastasiu, C.V. Therapeutic Approaches of Resveratrol on Endometriosis via Anti-Inflammatory and Anti-Angiogenic Pathways. Molecules 2019, 24, 667. [Google Scholar] [CrossRef] [PubMed]
- Donnez, J.; Stratopoulou, C.A.; Dolmans, M.M. Uterine Adenomyosis: From Disease Pathogenesis to a New Medical Approach Using GnRH Antagonists. Int. J. Environ. Res. Public Health 2021, 18, 9941. [Google Scholar] [CrossRef] [PubMed]
- Fatima, I.; Barman, S.; Rai, R.; Thiel, K.W.W.; Chandra, V. Targeting Wnt Signaling in Endometrial Cancer. Cancers 2021, 13, 2351. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Lang, X.; Lu, Z.; Wang, J.; Li, T.; Liao, Y.; Jia, C.; Zhao, W.; Fang, H. MiR-10b Directly Targets ZEB1 and PIK3CA to Curb Adenomyotic Epithelial Cell Invasiveness via Upregulation of E-Cadherin and Inhibition of Akt Phosphorylation. Cell Physiol. Biochem. 2015, 35, 2169–2180. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, V.; Farquhar, C.; Ponnampalam, A.P. Could DNA hydroxymethylation be crucial in influencing steroid hormone signaling in endometrial biology and endometriosis? Mol. Reprod. Dev. 2020, 87, 7–16. [Google Scholar] [CrossRef]
- Banz-Jansen, C.; Helweg, L.P.; Kaltschmidt, B. Endometrial Cancer Stem Cells: Where Do We Stand and Where Should We Go? Int. J. Mol. Sci. 2022, 23, 3412. [Google Scholar] [CrossRef] [PubMed]
- Gargett, C.E.; Hapangama, D. Endometrial Stem/Progenitor Cells: Prospects and Challenges. J. Pers. Med. 2022, 12, 1466. [Google Scholar] [CrossRef]
- Zhao, J.; Lin, X.; Yi, T.; Tong, A.; Pi, R.; Zheng, G.; Liao, S.; Zhao, X.; Bian, C.; Sun, G. Endometrial Mesenchymal Stem Cells and Their Role in the Origin and Treatment of Endometriosis. Clin. Exp. Obstet. Gynecol. 2022, 49, 263. [Google Scholar] [CrossRef]
- El Sabeh, M.; Afrin, S.; Singh, B.; Miyashita-Ishiwata, M.; Borahay, M. Uterine Stem Cells and Benign Gynecological Disorders: Role in Pathobiology and Therapeutic Implications. Stem Cell Rev. Rep. 2021, 17, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Dudley, A.C.; Griffioen, A.W. Pathological angiogenesis: Mechanisms and therapeutic strategies. Angiogenesis 2023, 26, 313–347. [Google Scholar] [CrossRef]
- Rousset-Rouviere, S.; Rochigneux, P.; Chrétien, A.-S.; Fattori, S.; Gorvel, L.; Provansal, M.; Lambaudie, E.; Olive, D.; Sabatier, R. Endometrial Carcinoma: Immune Microenvironment and Emerging Treatments in Immuno-Oncology. Biomedicines 2021, 9, 632. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Bauer, C.; Stewart, J.H., IV. Chasing Uterine Cancer with NK Cell-Based Immunotherapies. Future Pharmacol. 2022, 2, 642–659. [Google Scholar] [CrossRef]
- Cacciottola, L.; Donnez, J.; Dolmans, M.M. Can Endometriosis-Related Oxidative Stress Pave the Way for New Treatment Targets? Int. J. Mol. Sci. 2021, 22, 7138. [Google Scholar] [CrossRef]
- Amro, B.; Aristondo, M.E.R.; Alsuwaidi, S.; Almaamari, B.; Hakim, Z.; Tahlak, M.; Wattiez, A.; Koninckx, P.R. New Understanding of Diagnosis, Treatment and Prevention of Endometriosis. Int. J. Environ. Res. Public Health 2022, 19, 6725. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; He, F.; Lin, Z.; Liu, S.; Tang, L.; Huang, Y.; Hu, Z. Dysbiosis of the endometrial microbiota and its association with inflammatory cytokines in endometrial cancer. Int. J. Cancer 2021, 148, 1708–1716. [Google Scholar] [CrossRef]
- Koninckx, P.R.; Fernandes, R.; Ussia, A.; Schindler, L.; Wattiez, A.; Al-Suwaidi, S.; Amro, B.; Al-Maamari, B.; Hakim, Z.; Tahlak, M. Pathogenesis Based Diagnosis and Treatment of Endometriosis. Front. Endocrinol. 2021, 12, 745548. [Google Scholar] [CrossRef]
- Sobstyl, M.; Brecht, P.; Sobstyl, A.; Mertowska, P.; Grywalska, E. The Role of Microbiota in the Immunopathogenesis of Endometrial Cancer. Int. J. Mol. Sci. 2022, 23, 5756. [Google Scholar] [CrossRef]
- Chen, L.H.; Lo, W.C.; Huang, H.Y.; Wu, H.M. A Lifelong Impact on Endometriosis: Pathophysiology and Pharmacological Treatment. Int. J. Mol. Sci. 2023, 24, 7503. [Google Scholar] [CrossRef]
- Di Paolo, A.; Vignini, A.; Alia, S.; Membrino, V.; Carpini, G.D.; Giannella, L.; Ciavattini, A. Pathogenic Role of the Sphingosine 1-Phosphate (S1P) Pathway in Common Gynecologic Disorders (GDs): A Possible Novel Therapeutic Target. Int. J. Mol. Sci. 2022, 23, 13538. [Google Scholar] [CrossRef] [PubMed]
- Falcone, T.; Flyckt, R. Clinical Management of Endometriosis. Obstet. Gynecol. 2018, 131, 557–571. [Google Scholar] [CrossRef] [PubMed]
- Nezhat, C.R.; Stevens, A.; Balassiano, E.; Soliemannjad, R. Robotic-assisted laparoscopy vs. conventional laparoscopy for the treatment of advanced stage endometriosis. J. Minim. Invasive Gynecol. 2015, 22, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Tskhay, V.; Schindler, A.E.; Mikailly, G. Operation, hormone therapy and recovery of the patients with severe forms of adenomyosis. Gynecol. Endocrinol. 2018, 34, 647–650. [Google Scholar] [CrossRef] [PubMed]
- Ferrero, S.; Evangelisti, G.; Barra, F. Current and emerging treatment options for endometriosis. Expert Opin. Pharmacother. 2018, 19, 1109–1125. [Google Scholar] [CrossRef] [PubMed]
- Parasar, P.; Ozcan, P.; Terry, K.L. Endometriosis: Epidemiology, Diagnosis and Clinical Management. Curr. Obstet. Gynecol. Rep. 2017, 6, 34–41. [Google Scholar] [CrossRef]
- Maggiore, U.L.R.; Khamisy-Farah, R.; Bragazzi, N.L.; Bogani, G.; Martinelli, F.; Lopez, S.; Chiappa, V.; Signorelli, M.; Ditto, A.; Raspagliesi, F. Fertility-Sparing Treatment of Patients with Endometrial Cancer: A Review of the Literature. J. Clin. Med. 2021, 10, 4784. [Google Scholar] [CrossRef]
- Murji, A.; Biberoğlu, K.; Leng, J.; Mueller, M.D.; Römer, T.; Vignali, M.; Yarmolinskaya, M. Use of dienogest in endometriosis: A narrative literature review and expert commentary. Curr. Med. Res. Opin. 2020, 36, 895–907. [Google Scholar] [CrossRef]
- Streuli, I.; Dubuisson, J.; Santulli, P.; de Ziegler, D.; Batteux, F.; Chapron, C. An update on the pharmacological management of adenomyosis. Expert Opin. Pharmacother. 2014, 15, 2347–2360. [Google Scholar] [CrossRef]
- Banno, K.; Kisu, I.; Yanokura, M.; Tsuji, K.; Masuda, K.; Ueki, A.; Kobayashi, Y.; Yamagami, W.; Nomura, H.; Susumu, N.; et al. Progestin therapy for endometrial cancer: The potential of fourth-generation progestin (review). Int. J. Oncol. 2012, 40, 1755–1762. [Google Scholar] [CrossRef]
- Rütten, H.; Verhoef, C.; van Weelden, W.J.; Smits, A.; Dhanis, J.; Ottevanger, N.; Pijnenborg, J.M.A. Recurrent Endometrial Cancer: Local and Systemic Treatment Options. Cancers 2021, 13, 6275. [Google Scholar] [CrossRef] [PubMed]
- Cheung, T.K.; Lo, K.W.; Lam, C.W.; Lau, W.; Lam, P.K. A crossover study of triptorelin and leuprorelin acetate. Fertil. Steril. 2000, 74, 299–305, Erratum in Fertil. Steril. 2000, 74, 1060.. [Google Scholar] [CrossRef]
- Emons, G.; Gründker, C. The Role of Gonadotropin-Releasing Hormone (GnRH) in Endometrial Cancer. Cells 2021, 10, 292. [Google Scholar] [CrossRef] [PubMed]
- Hung, S.W.; Zhang, R.; Tan, Z.; Chung, J.P.W.; Zhang, T.; Wang, C.C. Pharmaceuticals targeting signaling pathways of endometriosis as potential new medical treatment: A review. Med. Res. Rev. 2021, 41, 2489–2564. [Google Scholar] [CrossRef]
- Mu, N.; Xu, T.; Gao, M.; Dong, M.; Tang, Q.; Hao, L.; Wang, G.; Li, Z.; Wang, W.; Yang, Y.; et al. Therapeutic effect of metformin in the treatment of endometrial cancer. Oncol. Lett. 2020, 20, 156. [Google Scholar] [CrossRef]
- Brichant, G.; Laraki, I.; Henry, L.; Munaut, C.; Nisolle, M. New Therapeutics in Endometriosis: A Review of Hormonal, Non-Hormonal, and Non-Coding RNA Treatments. Int. J. Mol. Sci. 2021, 22, 10498. [Google Scholar] [CrossRef] [PubMed]
- Kimber-Trojnar, Ż.; Dłuski, D.F.; Wierzchowska-Opoka, M.; Ruszała, M.; Leszczyńska-Gorzelak, B. Metformin as a Potential Treatment Option for Endometriosis. Cancers 2022, 14, 577. [Google Scholar] [CrossRef]
- Maksym, R.B.; Hoffmann-Młodzianowska, M.; Skibińska, M.; Rabijewski, M.; Mackiewicz, A.; Kieda, C. Immunology and Immunotherapy of Endometriosis. J. Clin. Med. 2021, 10, 5879. [Google Scholar] [CrossRef]
- Mamatha, J.; Simon, P.; Thilakchand, K.R.; Vijendra, R.; Rao, S.; Baliga, M.S.; Palatty, P.L. Cancer Pain and Analgesics: A Brief Review. Int. J. Med. Lab. Res. 2021, 6, 35–44. [Google Scholar] [CrossRef]
- Donnez, O.; Donnez, J. Gonadotropin-releasing hormone antagonist (linzagolix): A new therapy for uterine adenomyosis. Fertil. Steril. 2020, 114, 640–645. [Google Scholar] [CrossRef]
- Donnez, J.; Donnez, O.; Tourniaire, J.; Brethous, M.; Bestel, E.; Garner, E.; Charpentier, S.; Humberstone, A.; Loumaye, E. Uterine Adenomyosis Treated by Linzagolix, an Oral Gonadotropin-Releasing Hormone Receptor Antagonist: A Pilot Study with a New ‘Hit Hard First and then Maintain’ Regimen of Administration. J. Clin. Med. 2021, 10, 5794. [Google Scholar] [CrossRef]
- Grundker, C.; Schlotawa, L.; Viereck, V.; Eicke, N.; Horst, A.; Kairies, B.; Emons, G. Antiproliferative effects of the GnRH antagonist cetrorelix and of GnRH-II on human endometrial and ovarian cancer cells are not mediated through the GnRH type I receptor. Eur. J. Endocrinol. 2004, 151, 141–149. [Google Scholar] [CrossRef]
- Lambertini, M.; Peccatori, F.A.; Demeestere, I.; Amant, F.; Wyns, C.; Stukenborg, J.B.; Paluch-Shimon, S.; Halaska, M.J.; Uzan, C.; Meissner, J.; et al. Fertility preservation and post-treatment pregnancies in post-pubertal cancer patients: ESMO Clinical Practice Guidelines†. Ann. Oncol. 2020, 31, 1664–1678. [Google Scholar] [CrossRef] [PubMed]
- Hackenberg, R.; Schulz, K.D. Androgen receptor mediated growth control of breast cancer and endometrial cancer modulated by antiandrogen- and androgen-like steroids. J. Steroid Biochem. Mol. Biol. 1996, 56, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Słopień, R.; Męczekalski, B. Aromatase inhibitors in the treatment of endometriosis. Prz. Menopauzalny 2016, 15, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Peitsidis, P.; Tsikouras, P.; Laganà, A.S.; Laios, A.; Gkegkes, I.D.; Iavazzo, C. A Systematic Review of Systematic Reviews on the Use of Aromatase Inhibitors for the Treatment of Endometriosis: The Evidence to Date. Drug Des. Devel. Ther. 2023, 17, 1329–1346. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Zhou, L.; Shangguan, A.J.; Bulun, S.E. Aromatase expression and regulation in breast and endometrial cancer. J. Mol. Endocrinol. 2016, 57, R19–R33. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Cao, L.; Xu, Z.; Ma, Y.; Liang, X. Anti-Angiogenic Alternative and Complementary Medicines for the Treatment of Endometriosis: A Review of Potential Molecular Mechanisms. Evid. Based Complement. Alternat. Med. 2018, 2018, 4128984. [Google Scholar] [CrossRef] [PubMed]
- Harada, T.; Ohta, I.; Endo, Y.; Sunada, H.; Noma, H.; Taniguchi, F. SR-16234, a Novel Selective Estrogen Receptor Modulator for Pain Symptoms with Endometriosis: An Open-label Clinical Trial. Yonago Acta Med. 2018, 60, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Pinkerton, J.V.; Conner, E.A. Beyond estrogen: Advances in tissue selective estrogen complexes and selective estrogen receptor modulators. Climacteric 2019, 22, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Savelieva, G.M. A new strategy in selection of hormone therapy for endometrial proliferative process in postmenopausal patients. Bull. Russ. State Med. Univ. 2022, 42–50. [Google Scholar] [CrossRef]
- Che, X.; Wang, J.; He, J.; Yu, Q.; Sun, W.; Chen, S.; Zou, G.; Li, T.; Guo, X.; Zhang, X. A new trick for an old dog: The application of mifepristone in the treatment of adenomyosis. J. Cell. Mol. Med. 2020, 24, 1724–1737. [Google Scholar] [CrossRef] [PubMed]
- Che, X.; Wang, J.; He, J.; Guo, X.; Li, T.; Zhang, X. The new application of mifepristone in the relief of adenomyosis-caused dysmenorrhea. Int. J. Med. Sci. 2020, 17, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Conway, F.; Morosetti, G.; Camilli, S.; Martire, F.G.; Sorrenti, G.; Piccione, E.; Zupi, E.; Exacoustos, C. Ulipristal acetate therapy increases ultrasound features of adenomyosis: A good treatment given in an erroneous diagnosis of uterine fibroids. Gynecol. Endocrinol. 2019, 35, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Rolla, E. Endometriosis: Advances and controversies in classification, pathogenesis, diagnosis, and treatment. F1000Res 2019, 8, 529. [Google Scholar] [CrossRef]
- Kanda, R.; Miyagawa, Y.; Wada-Hiraike, O.; Hiraike, H.; Nagasaka, K.; Ryo, E.; Fujii, T.; Osuga, Y.; Ayabe, T. Ulipristal acetate simultaneously provokes antiproliferative and proinflammatory responses in endometrial cancer cells. Heliyon 2021, 8, e08696. [Google Scholar] [CrossRef]
- Gibson, D.A.; Simitsidellis, I.; Collins, F.; Saunders, P.T.K. Androgens, oestrogens and endometrium: A fine balance between perfection and pathology. J. Endocrinol. 2020, 246, R75–R93. [Google Scholar] [CrossRef]
- Lu, H.; Hu, H.; Yang, Y.; Li, S. The inhibition of reactive oxygen species (ROS) by antioxidants inhibits the release of an autophagy marker in ectopic endometrial cells. Taiwan J. Obstet. Gynecol. 2020, 59, 256–261. [Google Scholar] [CrossRef]
- Ilhan, M.; Gürağaç Dereli, F.T.; Akkol, E.K. Novel Drug Targets with Traditional Herbal Medicines for Overcoming Endometriosis. Curr. Drug Deliv. 2019, 16, 386–399. [Google Scholar] [CrossRef]
- Mehnert, J.M.; Panda, A.; Zhong, H.; Hirshfield, K.; Damare, S.; Lane, K.; Sokol, L.; Stein, M.N.; Rodriguez-Rodriquez, L.; Kaufman, H.L.; et al. Immune activation and response to pembrolizumab in POLE-mutant endometrial cancer. J. Clin. Investig. 2016, 126, 2334–2340. [Google Scholar] [CrossRef]
- Besharat, A.R.; Giannini, A.; Caserta, D. Pathogenesis and Treatments of Endometrial Carcinoma. Clin. Exp. Obstet. Gynecol. 2023, 50, 229. [Google Scholar] [CrossRef]
- Wang, X.; Wei, Z.; Tang, Z.; Xue, C.; Yu, H.; Zhang, D.; Li, Y.; Liu, X.; Shi, Y.; Zhang, L.; et al. IL-37bΔ1-45 suppresses the migration and invasion of endometrial cancer cells by targeting the Rac1/NF-κB/MMP2 signal pathway. Lab Investig. 2021, 101, 760–774. [Google Scholar] [CrossRef] [PubMed]
- Buza, N.; Roque, D.M.; Santin, A.D. HER2/neu in Endometrial Cancer: A Promising Therapeutic Target with Diagnostic Challenges. Arch. Pathol. Lab. Med. 2014, 138, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Premium: Mammalian target of rapamycin (mTOR) inhibitors in solid tumours. Pharm. J. 2016, 8, 439–454. [CrossRef]
- Nuñez-Olvera, S.I.; Gallardo-Rincón, D.; Puente-Rivera, J.; Salinas-Vera, Y.M.; Marchat, L.A.; Morales-Villegas, R.; López-Camarillo, C. Autophagy Machinery as a Promising Therapeutic Target in Endometrial Cancer. Front. Oncol. 2019, 9, 1326. [Google Scholar] [CrossRef]
- Yen, T.-T.; Miyamoto, T.; Asaka, S.; Chui, M.H.; Wang, Y.; Lin, S.-F.; Stone, R.L.; Fader, A.N.; Asaka, R.; Kashima, H.; et al. Loss of ARID1A expression in endometrial samplings is associated with the risk of endometrial carcinoma. Gynecol. Oncol. 2018, 150, 426–431. [Google Scholar] [CrossRef]
- Shen, J.; Peng, Y.; Wei, L.; Zhang, W.; Yang, L.; Lan, L.; Kapoor, P.; Ju, Z.; Mo, Q.; Shih, I.-M.; et al. ARID1A Deficiency Impairs the DNA Damage Checkpoint and Sensitizes Cells to PARP Inhibitors. Cancer Discov. 2015, 5, 752–767. [Google Scholar] [CrossRef]
- Rižner, T.L. The Important Roles of Steroid Sulfatase and Sulfotransferases in Gynecological Diseases. Front. Pharmacol. 2016, 7, 30. [Google Scholar] [CrossRef]
- Androutsopoulos, G.; Decavalas, G. Standard and Novel Therapies in Endometrial Cancer. J. Gynecol. Women’s Health 2016, 1, 555–564. [Google Scholar] [CrossRef]
- Vanhie, A.; Tomassetti, C.; Peeraer, K.; Meuleman, C.; D’Hooghe, T. Challenges in the development of novel therapeutic strategies for treatment of endometriosis. Expert Opin. Ther. Targets 2016, 20, 593–600. [Google Scholar] [CrossRef]
- Berlanda, N.; Somigliana, E.; Viganò, P.; Vercellini, P. Safety of medical treatments for endometriosis. Expert Opin. Drug Saf. 2016, 15, 21–30. [Google Scholar] [CrossRef]
- Matsushima, T.; Akira, S.; Fukami, T.; Yoneyama, K.; Takeshita, T. Efficacy of Hormonal Therapies for Decreasing Uterine Volume in Patients with Adenomyosis. Gynecol. Minim. Invasive Ther. 2018, 7, 119–123. [Google Scholar] [CrossRef]
- Wang, X.; Shi, Y.; Xu, L.; Wang, Z.; Wang, Y.; Shi, W.; Ma, K. Traditional Chinese medicine prescription Guizhi Fuling Pills in the treatment of endometriosis. Int. J. Med. Sci. 2021, 18, 2401–2408. [Google Scholar] [CrossRef]
- Zhang, Z.; Yang, B.; Zhang, W.; Gao, X.; Zhao, C.; Zhang, X.; Wang, L.; Zhang, Y.; Zhang, F.; Zhang, H.; et al. Clinicopathological characteristics and survival outcomes of patients with coexistence of adenomyosis and endometrial carcinoma. Int. J. Clin. Exp. Pathol. 2018, 11, 956–962. [Google Scholar] [PubMed]
- Aydin, H.A.; Toptas, T.; Bozkurt, S.; Pestereli, E.; Simsek, T. Impact of coexistent adenomyosis on outcomes of patients with endometrioid endometrial cancer: A propensity score-matched analysis. Tumori 2018, 104, 60–65. [Google Scholar] [CrossRef]
- Pluchino, N.; Freschi, L.; Wenger, J.M.; Streuli, I. Innovations in classical hormonal targets for endometriosis. Expert Rev. Clin. Pharmacol. 2016, 9, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Guerriero, S.; Condous, G.; van den Bosch, T.; Valentin, L.; Leone, F.P.; Van Schoubroeck, D.; Exacoustos, C.; Installé, A.J.; Martins, W.P.; Abrao, M.S.; et al. Systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis, including terms, definitions and measurements: A consensus opinion from the International Deep Endometriosis Analysis (IDEA) group. Ultrasound Obs. Gynecol 2016, 48, 318–332. [Google Scholar] [CrossRef]
- Harmsen, M.J.; Van den Bosch, T.; de Leeuw, R.A.; Dueholm, M.; Exacoustos, C.; Valentin, L.; Hehenkamp, W.J.K.; Groenman, F.; De Bruyn, C.; Rasmussen, C.; et al. Consensus on revised definitions of Morphological Uterus Sonographic Assessment (MUSA) features of adenomyosis: Results of modified Delphi procedure. Ultrasound Obs. Gynecol 2022, 60, 118–131. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Therapeutic Options | Pathologies | Symptoms | Mechanism | Side Effects |
|---|---|---|---|---|
| Estroprogestins [4,10,33,35,36,37] | Endometriosis Adenomyosis | Pain Control of menstrual cycle | Ovulation inhibitor Decidualization Endometrial atrophy | Vaginal bleeding Breast pain Headaches |
| Progestins [4,8,10,11,33,35,36,37,40,41,42,70] | Endometriosis Adenomyosis Endometrial cancer | Pain Decreased uterine volume Reduced need for surgery Fertility-sparing management Lesion recurrence prevention Improved quality of life | Suppress ovarian steroidogenesis Decidualization Anti-inflammatory effects Anti-angiogenesis Reduced cell proliferation, migration, apoptosis, and infiltration in EC | Breast pain Weight gain Fluid retention Bleeding Acne Headaches Mood changes Liver enzyme increase |
| GnRh analogs [2,4,10,11,33,35,36,37,40,43,44] | Endometriosis Adenomyosis Endometrial cancer | Pain Preventing the recurrence of pain and lesions | Suppress ovarian estrogen production Inhibit cell proliferation and migration | Depression Hot flashes Headaches Vaginal atrophy Bone density decrease Alteration of lipid profile Induce apoptosis |
| Anti-inflammatory drugs: NSAIDs [2,4,35,36,37,40] Metformin, Heparin [10,45,46] Anti-TNF [47,48] Botulinum toxin Melatonin [45] Naltrexone [49] | Endometriosis Adenomyosis Endometrial cancer | Pain | Under study for their anti-inflammatory effects (insufficient data) | Gastro-intestinal ulcers Hypertension Renal failure |
| GnRh antagonists [2,4,10,11,13,15,33,36,40,51,52,53] | Endometriosis Adenomyosis Endometrial cancer | Pain | Some are under study Downregulation of estrogen Anti-proliferative effects | Vaginal bleeding Nausea Headaches Anxiety Mild hot flashes Lipid modification |
| Androgenic steroids (Danazol) [2,5,10,13,33,40,45,54,55] | Endometriosis Adenomyosis Endometrial cancer | Pain Good compliance | Inhibition of pituitary gonadotropin-releasing hormone Inhibition of estrogen secretion Local growth factor inhibitor Decrease in proliferation | Hair loss Acne Hirsutism Weight gain Vaginal bleeding |
| Aromatase inhibitor [2,10,33,35,36,40,56,57,58] | Endometriosis Endometrial cancer | Pain | Blocks estrogen synthesis from androgens | Hot flashes Headaches Bone density decrease Weight gain Fatigue Depression Insomnia Spotting Decreased libido |
| Anti-angiogenic treatment [10,23,25,36,40,45,47,59] | Endometriosis Adenomyosis Endometrial cancer | Beneficial in early-stage disease Prevents recurrence | Ischemia and tumor necrosis Procoagulant Proapoptotic effect Antibody delivers toxic agents against tumor endothelium | No obvious adverse effects |
| SERMs [10,35,36,61] | Endometriosis Adenomyosis Endometrial cancer | Various beneficial effects Pain Reduce lesion size | Target estrogen receptors | Enhance hyperalgesia Sometimes exhibits estrogenic effects |
| SPRMs [2,5,10,33,36,40,62,63,64,65,66,67] | Endometriosis Adenomyosis Endometrial cancer (under study) | Pain Decrease in uterine volume Antitumoral effects | Cell apoptosis Inhibition of ovulation Suppress EMT Inhibits migration | Can induce endometrial cancer Liver failure Mood change Headaches Pelvic pain Nausea Vaginal bleeding |
| SARMs [10,55,68] | Endometriosis Adenomyosis Endometrial cancer (under study) | Pain Muscle loss Urinary stress incontinence | Anti-proliferative effects Modulate androgen-like steroid receptors | Unknown |
| Antioxidants [4,10,25,36,45,69,70] | Endometriosis Adenomyosis Endometrial cancer (under study) | Pain Reduce lesions | Anti-inflammatory effects Anti-proliferative Anti-adherent Anti-angiogenic Affect apoptosis and autophagy | Still under investigation |
| Immunotherapy [10,24,36,37,49,71,72] | Endometriosis Adenomyosis Endometrial cancer (under study) | Reduces the size and number of lesions, but controversial results | Anti-inflammatory effects Reduces ROS | Still under investigation |
| Epigenetic agents (valproic acid and anti-platelet agents) [2,10,35,36,40] | Endometriosis Adenomyosis Endometrial cancer (under study) | Reduce lesion size Reduce pain and fibrosis | Anti-inflammatory effects Effects on EMT | Unknown |
| Stem cells [10,19,21,22,47] | Endometriosis Adenomyosis Endometrial cancer (under study) | Pain Reduce lesion sizes | Induce cell differentiation Reduce stemness | Unknown |
| Therapeutic Research Targeting New Pathways | Pathologies | Outcome | Disadvantage |
|---|---|---|---|
| HER2/Neu [Natalia Buza et al., 2014] [74] | Endometrial cancer | Improved free survival | Must be combined with classical chemotherapy |
| Targeting PI3K-AKT-mTor pathway (temsirolimus, ridaforolimus, and everolimus; at least five clinical trials are being conducted) [7,75] | Endometrial cancer | Only everolimus showed a good response | High toxicity |
| ARID1A and EZH2 inhibitors [77,78] | Endometrial cancer | Disappointing efficacy as monotherapy | Must be combined with other drugs |
| Sulfatase and sulfotransferase [68,79] | Endometriosis Endometrial cancer | No convincing clinical outcomes | Limited effects |
| PARP, PD-1, and PD-L1 [24,49,74,78] | Endometriosis Endometrial cancer | Partial response | PARP inhibitors associated with hematologic disorders |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitranovici, M.-I.; Chiorean, D.M.; Moraru, L.; Moraru, R.; Caravia, L.; Tiron, A.T.; Cotoi, T.C.; Toru, H.S.; Cotoi, O.S. Shared Pathogenic and Therapeutic Characteristics of Endometriosis, Adenomyosis, and Endometrial Cancer: A Comprehensive Literature Review. Pharmaceuticals 2024, 17, 311. https://doi.org/10.3390/ph17030311
Mitranovici M-I, Chiorean DM, Moraru L, Moraru R, Caravia L, Tiron AT, Cotoi TC, Toru HS, Cotoi OS. Shared Pathogenic and Therapeutic Characteristics of Endometriosis, Adenomyosis, and Endometrial Cancer: A Comprehensive Literature Review. Pharmaceuticals. 2024; 17(3):311. https://doi.org/10.3390/ph17030311
Chicago/Turabian StyleMitranovici, Melinda-Ildiko, Diana Maria Chiorean, Liviu Moraru, Raluca Moraru, Laura Caravia, Andreea Taisia Tiron, Titiana Cornelia Cotoi, Havva Serap Toru, and Ovidiu Simion Cotoi. 2024. "Shared Pathogenic and Therapeutic Characteristics of Endometriosis, Adenomyosis, and Endometrial Cancer: A Comprehensive Literature Review" Pharmaceuticals 17, no. 3: 311. https://doi.org/10.3390/ph17030311