

Clinical Efficacy, Pharmacokinetics, and Safety of the Available Medical Options in the Treatment of Endometriosis-Related Pelvic Pain: A Scoping Review
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Results
3. Discussion
3.1. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
3.2. Combined Oral Contraceptives (COCs)
3.3. Progestins
3.4. Gonadotropin-Releasing Hormone Agonists
3.5. Gonadotropin-Releasing Hormone Antagonists
3.6. Aromatase Inhibitors
3.7. Selective Estrogen Receptor Modulators
3.8. Selective Progesterone Receptor Modulators
3.9. Levonorgestrel-Intrauterine Device
3.10. Unconventional Therapy Options
3.11. The Patients’ Pathway—From NSAIDs to Surgery
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giudice, L.C.; Kao, L.C. Endometriosis. Lancet 2004, 364, 1789–1799. [Google Scholar] [CrossRef] [PubMed]
- Chapron, C.; Marcellin, L.; Borghese, B.; Santulli, P. Rethinking Mechanisms, Diagnosis and Management of Endometriosis. Nat. Rev. Endocrinol. 2019, 15, 666–682. [Google Scholar] [CrossRef] [PubMed]
- Taylor, H.S.; Kotlyar, A.M.; Flores, V.A. Endometriosis Is a Chronic Systemic Disease: Clinical Challenges and Novel Innovations. Lancet 2021, 397, 839–852. [Google Scholar] [CrossRef] [PubMed]
- Mehedintu, C.; Plotogea, M.N.; Ionescu, S.; Antonovici, M. Endometriosis Still a Challenge. J. Med. Life 2014, 7, 349–357. [Google Scholar]
- Škegro, B.; Bjedov, S.; Mikuš, M.; Mustač, F.; Lešin, J.; Matijević, V.; Ćorić, M.; Elveđi Gašparović, V.; Medić, F.; Sokol Karadjole, V. Endometriosis, Pain and Mental Health. Psychiatr. Danub. 2021, 33, 632–636. [Google Scholar]
- Greene, A.D.; Lang, S.A.; Kendziorski, J.A.; Sroga-Rios, J.M.; Herzog, T.J.; Burns, K.A. Endometriosis: Where Are We and Where Are We Going? Reproduction 2016, 152, R63–R78. [Google Scholar] [CrossRef]
- Coric, M.; Barisic, D.; Pavicic, D.; Karadza, M.; Banovic, M. Electrocoagulation versus Suture after Laparoscopic Stripping of Ovarian Endometriomas Assessed by Antral Follicle Count: Preliminary Results of Randomized Clinical Trial. Arch. Gynecol. Obstet. 2011, 283, 373–378. [Google Scholar] [CrossRef]
- Leonardi, M.; Gibbons, T.; Armour, M.; Wang, R.; Glanville, E.; Hodgson, R.; Cave, A.E.; Ong, J.; Tong, Y.Y.F.; Jacobson, T.Z.; et al. When to Do Surgery and When Not to Do Surgery for Endometriosis: A Systematic Review and Meta-Analysis. J. Minim. Invasive Gynecol. 2020, 27, 390–407.e3. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.S.; Gude, K.; Perdeaux, E.; Gattrell, W.T.; Becker, C.M. Surgical Outcomes in Patients With Endometriosis: A Systematic Review. J. Obstet. Gynaecol. Can. 2020, 42, 881–888.e11. [Google Scholar] [CrossRef]
- Ferrero, S.; Evangelisti, G.; Barra, F. Current and Emerging Treatment Options for Endometriosis. Expert. Opin. Pharmacother. 2018, 19, 1109–1125. [Google Scholar] [CrossRef]
- Bindu, S.; Mazumder, S.; Bandyopadhyay, U. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) and Organ Damage: A Current Perspective. Biochem. Pharmacol. 2020, 180, 114147. [Google Scholar] [CrossRef] [PubMed]
- Lees, P.; Giraudel, J.; Landoni, M.F.; Toutain, P.L. PK-PD Integration and PK-PD Modelling of Nonsteroidal Anti-Inflammatory Drugs: Principles and Applications in Veterinary Pharmacology. J. Vet. Pharmacol. Ther. 2004, 27, 491–502. [Google Scholar] [CrossRef]
- Pilotto, A.; Seripa, D.; Franceschi, M.; Scarcelli, C.; Colaizzo, D.; Grandone, E.; Niro, V.; Andriulli, A.; Leandro, G.; Di Mario, F.; et al. Genetic Susceptibility to Nonsteroidal Anti-Inflammatory Drug-Related Gastroduodenal Bleeding: Role of Cytochrome P450 2C9 Polymorphisms. Gastroenterology 2007, 133, 465–471. [Google Scholar] [CrossRef]
- Wyatt, J.E.; Pettit, W.L.; Harirforoosh, S. Pharmacogenetics of Nonsteroidal Anti-Inflammatory Drugs. Pharmacogenom. J. 2012, 12, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.; Crawford, T.J.; Allen, C.; Hopewell, S.; Prentice, A. Nonsteroidal Anti-Inflammatory Drugs for Pain in Women with Endometriosis. Cochrane Database Syst. Rev. 2017, 1, CD004753. [Google Scholar] [CrossRef]
- Kauppila, A.; Rönnberg, L. Naproxen Sodium in Dysmenorrhea Secondary to Endometriosis. Obstet. Gynecol. 1985, 65, 379–383. [Google Scholar]
- Arfè, A.; Scotti, L.; Varas-Lorenzo, C.; Nicotra, F.; Zambon, A.; Kollhorst, B.; Schink, T.; Garbe, E.; Herings, R.; Straatman, H.; et al. Non-Steroidal Anti-Inflammatory Drugs and Risk of Heart Failure in Four European Countries: Nested Case-Control Study. BMJ 2016, 354, i4857. [Google Scholar] [CrossRef]
- Kleinknecht, D. Interstitial Nephritis, the Nephrotic Syndrome, and Chronic Renal Failure Secondary to Nonsteroidal Anti-Inflammatory Drugs. Semin. Nephrol. 1995, 15, 228–235. [Google Scholar]
- Goldzieher, J.W.; Stanczyk, F.Z. Oral Contraceptives and Individual Variability of Circulating Levels of Ethinyl Estradiol and Progestins. Contraception 2008, 78, 4–9. [Google Scholar] [CrossRef]
- Simmons, K.B.; Edelman, A.B. Hormonal Contraception and Obesity. Fertil. Steril. 2016, 106, 1282–1288. [Google Scholar] [CrossRef]
- Edelman, A.B.; Cherala, G.; Stanczyk, F.Z. Metabolism and Pharmacokinetics of Contraceptive Steroids in Obese Women: A Review. Contraception 2010, 82, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Crawford, P. Interactions between Antiepileptic Drugs and Hormonal Contraception. CNS Drugs 2002, 16, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Simmons, K.B.; Haddad, L.B.; Nanda, K.; Curtis, K.M. Drug Interactions between Non-Rifamycin Antibiotics and Hormonal Contraception: A Systematic Review. Am. J. Obstet. Gynecol. 2018, 218, 88–97.e14. [Google Scholar] [CrossRef] [PubMed]
- Barbara, G.; Buggio, L.; Facchin, F.; Vercellini, P. Medical Treatment for Endometriosis: Tolerability, Quality of Life and Adherence. Front. Glob. Womens Health 2021, 2, 729601. [Google Scholar] [CrossRef] [PubMed]
- Sesti, F.; Pietropolli, A.; Capozzolo, T.; Broccoli, P.; Pierangeli, S.; Bollea, M.R.; Piccione, E. Hormonal Suppression Treatment or Dietary Therapy versus Placebo in the Control of Painful Symptoms after Conservative Surgery for Endometriosis Stage III-IV. A Randomized Comparative Trial. Fertil. Steril. 2007, 88, 1541–1547. [Google Scholar] [CrossRef] [PubMed]
- Guzick, D.S.; Huang, L.-S.; Broadman, B.A.; Nealon, M.; Hornstein, M.D. Randomized Trial of Leuprolide versus Continuous Oral Contraceptives in the Treatment of Endometriosis-Associated Pelvic Pain. Fertil. Steril. 2011, 95, 1568–1573. [Google Scholar] [CrossRef]
- Parazzini, F.; Di Cintio, E.; Chatenoud, L.; Moroni, S.; Ardovino, I.; Struzziero, E.; Falsetti, L.; Bianchi, A.; Bracco, G.; Pellegrini, A.; et al. Estroprogestin vs. Gonadotrophin Agonists plus Estroprogestin in the Treatment of Endometriosis-Related Pelvic Pain: A Randomized Trial. Gruppo Italiano per Lo Studio Dell’Endometriosi. Eur. J. Obstet. Gynecol. Reprod. Biol. 2000, 88, 11–14. [Google Scholar] [CrossRef]
- Vercellini, P.; Trespidi, L.; Colombo, A.; Vendola, N.; Marchini, M.; Crosignani, P.G. A Gonadotropin-Releasing Hormone Agonist versus a Low-Dose Oral Contraceptive for Pelvic Pain Associated with Endometriosis. Fertil. Steril. 1993, 60, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Leone Roberti Maggiore, U.; Remorgida, V.; Scala, C.; Tafi, E.; Venturini, P.L.; Ferrero, S. Desogestrel-Only Contraceptive Pill versus Sequential Contraceptive Vaginal Ring in the Treatment of Rectovaginal Endometriosis Infiltrating the Rectum: A Prospective Open-Label Comparative Study. Acta Obstet. Gynecol. Scand. 2014, 93, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Vercellini, P.; Barbara, G.; Somigliana, E.; Bianchi, S.; Abbiati, A.; Fedele, L. Comparison of Contraceptive Ring and Patch for the Treatment of Symptomatic Endometriosis. Fertil. Steril. 2010, 93, 2150–2161. [Google Scholar] [CrossRef]
- Bizzarri, N.; Remorgida, V.; Leone Roberti Maggiore, U.; Scala, C.; Tafi, E.; Ghirardi, V.; Salvatore, S.; Candiani, M.; Venturini, P.L.; Ferrero, S. Dienogest in the Treatment of Endometriosis. Expert. Opin. Pharmacother. 2014, 15, 1889–1902. [Google Scholar] [CrossRef] [PubMed]
- Vercellini, P.; Somigliana, E.; Consonni, D.; Frattaruolo, M.P.; De Giorgi, O.; Fedele, L. Surgical versus Medical Treatment for Endometriosis-Associated Severe Deep Dyspareunia: I. Effect on Pain during Intercourse and Patient Satisfaction. Hum. Reprod. 2012, 27, 3450–3459. [Google Scholar] [CrossRef] [PubMed]
- Bick, A.J.; Louw-du Toit, R.; Skosana, S.B.; Africander, D.; Hapgood, J.P. Pharmacokinetics, Metabolism and Serum Concentrations of Progestins Used in Contraception. Pharmacol. Ther. 2021, 222, 107789. [Google Scholar] [CrossRef] [PubMed]
- Berman, J.R.; Almeida, F.G.; Jolin, J.; Raz, S.; Chaudhuri, G.; Gonzalez-Cadavid, N.F. Correlation of Androgen Receptors, Aromatase, and 5-Alpha Reductase in the Human Vagina with Menopausal Status. Fertil. Steril. 2003, 79, 925–931. [Google Scholar] [CrossRef]
- Konings, G.; Brentjens, L.; Delvoux, B.; Linnanen, T.; Cornel, K.; Koskimies, P.; Bongers, M.; Kruitwagen, R.; Xanthoulea, S.; Romano, A. Intracrine Regulation of Estrogen and Other Sex Steroid Levels in Endometrium and Non-Gynecological Tissues; Pathology, Physiology, and Drug Discovery. Front. Pharmacol. 2018, 9, 940. [Google Scholar] [CrossRef]
- Brown, J.; Kives, S.; Akhtar, M. Progestagens and Anti-Progestagens for Pain Associated with Endometriosis. Cochrane Database Syst. Rev. 2012, CD002122. [Google Scholar] [CrossRef]
- Ambacher, K.; Secter, M.; Sanders, A.P. The Use of Progestin Subdermal Implants in the Management of Endometriosis-Related Pain Symptoms and Quality of Life: A Systematic Review. Curr. Med. Res. Opin. 2022, 38, 479–486. [Google Scholar] [CrossRef]
- Ferrero, S.; Camerini, G.; Ragni, N.; Venturini, P.L.; Biscaldi, E.; Remorgida, V. Norethisterone Acetate in the Treatment of Colorectal Endometriosis: A Pilot Study. Hum. Reprod. 2010, 25, 94–100. [Google Scholar] [CrossRef]
- Angioni, S.; Nappi, L.; Pontis, A.; Sedda, F.; Luisi, S.; Mais, V.; Melis, G.B. Dienogest. A Possible Conservative Approach in Bladder Endometriosis. Results of a Pilot Study. Gynecol. Endocrinol. 2015, 31, 406–408. [Google Scholar] [CrossRef]
- de Andres, M.P.; Lopes, L.A.; Baracat, E.C.; Podgaec, S. Dienogest in the Treatment of Endometriosis: Systematic Review. Arch. Gynecol. Obstet. 2015, 292, 523–529. [Google Scholar] [CrossRef]
- Morotti, M.; Remorgida, V.; Venturini, P.L.; Ferrero, S. Progestogen-Only Contraceptive Pill Compared with Combined Oral Contraceptive in the Treatment of Pain Symptoms Caused by Endometriosis in Patients with Migraine without Aura. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 179, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Barra, F.; Scala, C.; Ferrero, S. Current Understanding on Pharmacokinetics, Clinical Efficacy and Safety of Progestins for Treating Pain Associated to Endometriosis. Expert. Opin. Drug Metab. Toxicol. 2018, 14, 399–415. [Google Scholar] [CrossRef] [PubMed]
- Tarlatzis, B.C.; Kolibianakis, E.M. GnRH Agonists vs Antagonists. Best. Pract. Res. Clin. Obstet. Gynaecol. 2007, 21, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.-M.; Wang, H.-S.; Huang, H.-Y.; Soong, Y.-K.; MacCalman, C.D.; Leung, P.C.K. GnRH Signaling in Intrauterine Tissues. Reproduction 2009, 137, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Tzoupis, H.; Nteli, A.; Androutsou, M.-E.; Tselios, T. Gonadotropin-Releasing Hormone and GnRH Receptor: Structure, Function and Drug Development. Curr. Med. Chem. 2020, 27, 6136–6158. [Google Scholar] [CrossRef] [PubMed]
- Stamatiades, G.A.; Kaiser, U.B. Gonadotropin Regulation by Pulsatile GnRH: Signaling and Gene Expression. Mol. Cell. Endocrinol. 2018, 463, 131–141. [Google Scholar] [CrossRef]
- Wilson, A.C.; Meethal, S.V.; Bowen, R.L.; Atwood, C.S. Leuprolide Acetate: A Drug of Diverse Clinical Applications. Expert. Opin. Investig. Drugs 2007, 16, 1851–1863. [Google Scholar] [CrossRef]
- Teutonico, D.; Montanari, S.; Ponchel, G. Leuprolide Acetate: Pharmaceutical Use and Delivery Potentials. Expert. Opin. Drug Deliv. 2012, 9, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Cox, M.C.; Scripture, C.D.; Figg, W.D. Leuprolide Acetate given by a Subcutaneous Extended-Release Injection: Less of a Pain? Expert Rev. Anticancer Ther. 2005, 5, 605–611. [Google Scholar] [CrossRef]
- Shore, N.D.; Guerrero, S.; Sanahuja, R.M.; Gambús, G.; Parente, A. A New Sustained-Release, 3-Month Leuprolide Acetate Formulation Achieves and Maintains Castrate Concentrations of Testosterone in Patients with Prostate Cancer. Clin. Ther. 2019, 41, 412–425. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, N.M.; Hosmane, B.; Larsen, L.M.; Chwalisz, K.; Chiu, Y.-L.; Pradhan, R.S. Pharmacokinetic and Exposure-Response Analyses of Leuprolide Following Administration of Leuprolide Acetate 3-Month Depot Formulations to Children with Central Precocious Puberty. Clin. Drug Investig. 2014, 34, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.; Pan, A.; Hart, R.J. Gonadotrophin-Releasing Hormone Analogues for Pain Associated with Endometriosis. Cochrane Database Syst. Rev. 2010, CD008475. [Google Scholar] [CrossRef]
- Fedele, L.; Bianchi, S.; Bocciolone, L.; Di Nola, G.; Franchi, D. Buserelin Acetate in the Treatment of Pelvic Pain Associated with Minimal and Mild Endometriosis: A Controlled Study. Fertil. Steril. 1993, 59, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Bergqvist, A.; Bergh, T.; Hogström, L.; Mattsson, S.; Nordenskjöld, F.; Rasmussen, C. Effects of Triptorelin versus Placebo on the Symptoms of Endometriosis. Fertil. Steril. 1998, 69, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Dlugi, A.M.; Miller, J.D.; Knittle, J. Lupron Depot (Leuprolide Acetate for Depot Suspension) in the Treatment of Endometriosis: A Randomized, Placebo-Controlled, Double-Blind Study. Lupron Study Group. Fertil. Steril. 1990, 54, 419–427. [Google Scholar] [CrossRef]
- Miller, J.D. Leuprolide Acetate for the Treatment of Endometriosis. Prog. Clin. Biol. Res. 1990, 323, 337–341. [Google Scholar]
- Harada, T.; Momoeda, M.; Taketani, Y.; Aso, T.; Fukunaga, M.; Hagino, H.; Terakawa, N. Dienogest Is as Effective as Intranasal Buserelin Acetate for the Relief of Pain Symptoms Associated with Endometriosis—A Randomized, Double-Blind, Multicenter, Controlled Trial. Fertil. Steril. 2009, 91, 675–681. [Google Scholar] [CrossRef]
- Strowitzki, T.; Marr, J.; Gerlinger, C.; Faustmann, T.; Seitz, C. Dienogest Is as Effective as Leuprolide Acetate in Treating the Painful Symptoms of Endometriosis: A 24-Week, Randomized, Multicentre, Open-Label Trial. Hum. Reprod. 2010, 25, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Lemay, A.; Maheux, R.; Huot, C.; Blanchet, J.; Faure, N. Efficacy of Intranasal or Subcutaneous Luteinizing Hormone-Releasing Hormone Agonist Inhibition of Ovarian Function in the Treatment of Endometriosis. Am. J. Obstet. Gynecol. 1988, 158, 233–236. [Google Scholar] [CrossRef]
- Dmowski, W.P.; Radwanska, E.; Binor, Z.; Tummon, I.; Pepping, P. Ovarian Suppression Induced with Buserelin or Danazol in the Management of Endometriosis: A Randomized, Comparative Study. Fertil. Steril. 1989, 51, 395–400. [Google Scholar] [CrossRef]
- Agarwal, S.K.; Hamrang, C.; Henzl, M.R.; Judd, H.L. Nafarelin vs. Leuprolide Acetate Depot for Endometriosis. Changes in Bone Mineral Density and Vasomotor Symptoms. Nafarelin Study Group. J. Reprod. Med. 1997, 42, 413–423. [Google Scholar] [PubMed]
- Zheng, Q.; Mao, H.; Xu, Y.; Zhao, J.; Wei, X.; Liu, P. Can Postoperative GnRH Agonist Treatment Prevent Endometriosis Recurrence? A Meta-Analysis. Arch. Gynecol. Obstet. 2016, 294, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Huirne, J.A.; Lambalk, C.B. Gonadotropin-Releasing-Hormone-Receptor Antagonists. Lancet 2001, 358, 1793–1803. [Google Scholar] [CrossRef] [PubMed]
- Rocca, M.L.; Palumbo, A.R.; Lico, D.; Fiorenza, A.; Bitonti, G.; D’Agostino, S.; Gallo, C.; Di Carlo, C.; Zullo, F.; Venturella, R. Relugolix for the Treatment of Uterine Fibroids. Expert. Opin. Pharmacother. 2020, 21, 1667–1674. [Google Scholar] [CrossRef]
- Barra, F.; Seca, M.; Della Corte, L.; Giampaolino, P.; Ferrero, S. Relugolix for the Treatment of Uterine Fibroids. Drugs Today 2019, 55, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Tan, O.; Bukulmez, O. Biochemistry, Molecular Biology and Cell Biology of Gonadotropin-Releasing Hormone Antagonists. Curr. Opin. Obstet. Gynecol. 2011, 23, 238–244. [Google Scholar] [CrossRef]
- Donnez, J.; Taylor, H.S.; Taylor, R.N.; Akin, M.D.; Tatarchuk, T.F.; Wilk, K.; Gotteland, J.-P.; Lecomte, V.; Bestel, E. Treatment of Endometriosis-Associated Pain with Linzagolix, an Oral Gonadotropin-Releasing Hormone-Antagonist: A Randomized Clinical Trial. Fertil. Steril. 2020, 114, 44–55. [Google Scholar] [CrossRef]
- Diamond, M.P.; Carr, B.; Dmowski, W.P.; Koltun, W.; O’Brien, C.; Jiang, P.; Burke, J.; Jimenez, R.; Garner, E.; Chwalisz, K. Elagolix Treatment for Endometriosis-Associated Pain: Results from a Phase 2, Randomized, Double-Blind, Placebo-Controlled Study. Reprod. Sci. 2014, 21, 363–371. [Google Scholar] [CrossRef]
- Taylor, H.S.; Giudice, L.C.; Lessey, B.A.; Abrao, M.S.; Kotarski, J.; Archer, D.F.; Diamond, M.P.; Surrey, E.; Johnson, N.P.; Watts, N.B.; et al. Treatment of Endometriosis-Associated Pain with Elagolix, an Oral GnRH Antagonist. N. Engl. J. Med. 2017, 377, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Giudice, L.C.; As-Sanie, S.; Arjona Ferreira, J.C.; Becker, C.M.; Abrao, M.S.; Lessey, B.A.; Brown, E.; Dynowski, K.; Wilk, K.; Li, Y.; et al. Once daily oral relugolix combination therapy versus placebo in patients with endometriosis-associated pain: Two replicate phase 3, randomised, double-blind, studies (spirit 1 and 2). Lancet 2022, 399, 2267–2279. [Google Scholar] [CrossRef]
- Garzon, S.; Laganà, A.S.; Barra, F.; Casarin, J.; Cromi, A.; Raffaelli, R.; Uccella, S.; Franchi, M.; Ghezzi, F.; Ferrero, S. Novel Drug Delivery Methods for Improving Efficacy of Endometriosis Treatments. Expert. Opin. Drug Deliv. 2021, 18, 355–367. [Google Scholar] [CrossRef]
- Lønning, P.; Pfister, C.; Martoni, A.; Zamagni, C. Pharmacokinetics of Third-Generation Aromatase Inhibitors. Semin. Oncol. 2003, 30, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Lønning, P. Clinical Pharmacokinetics of Aromatase Inhibitors and Inactivators. Clin. Pharmacokinet. 2003, 42, 619–631. [Google Scholar] [CrossRef] [PubMed]
- Remorgida, V.; Abbamonte, L.H.; Ragni, N.; Fulcheri, E.; Ferrero, S. Letrozole and Desogestrel-Only Contraceptive Pill for the Treatment of Stage IV Endometriosis. Aust. N. Z. J. Obstet. Gynaecol. 2007, 47, 222–225. [Google Scholar] [CrossRef]
- Ferrero, S.; Venturini, P.L.; Gillott, D.J.; Remorgida, V. Letrozole and Norethisterone Acetate versus Letrozole and Triptorelin in the Treatment of Endometriosis Related Pain Symptoms: A Randomized Controlled Trial. Reprod. Biol. Endocrinol. 2011, 9, 88. [Google Scholar] [CrossRef]
- Hefler, L.A.; Grimm, C.; van Trotsenburg, M.; Nagele, F. Role of the Vaginally Administered Aromatase Inhibitor Anastrozole in Women with Rectovaginal Endometriosis: A Pilot Study. Fertil. Steril. 2005, 84, 1033–1036. [Google Scholar] [CrossRef]
- Amsterdam, L.L.; Gentry, W.; Jobanputra, S.; Wolf, M.; Rubin, S.D.; Bulun, S.E. Anastrazole and Oral Contraceptives: A Novel Treatment for Endometriosis. Fertil. Steril. 2005, 84, 300–304. [Google Scholar] [CrossRef]
- Soysal, S.; Soysal, M.E.; Ozer, S.; Gul, N.; Gezgin, T. The Effects of Post-Surgical Administration of Goserelin plus Anastrozole Compared to Goserelin Alone in Patients with Severe Endometriosis: A Prospective Randomized Trial. Hum. Reprod. 2004, 19, 160–167. [Google Scholar] [CrossRef]
- Garzon, S.; Laganà, A.S.; Barra, F.; Casarin, J.; Cromi, A.; Raffaelli, R.; Uccella, S.; Franchi, M.; Ghezzi, F.; Ferrero, S. Aromatase Inhibitors for the Treatment of Endometriosis: A Systematic Review about Efficacy, Safety and Early Clinical Development. Expert. Opin. Investig. Drugs 2020, 29, 1377–1388. [Google Scholar] [CrossRef]
- Schultze-Mosgau, M.-H.; Waellnitz, K.; Nave, R.; Klein, S.; Kraetzschmar, J.; Rautenberg, T.; Schmitz, H.; Rohde, B. Pharmacokinetics, Pharmacodynamics, Safety and Tolerability of an Intravaginal Ring Releasing Anastrozole and Levonorgestrel in Healthy Premenopausal Women: A Phase 1 Randomized Controlled Trial. Hum. Reprod. 2016, 31, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Dutertre, M.; Smith, C.L. Molecular Mechanisms of Selective Estrogen Receptor Modulator (SERM) Action. J. Pharmacol. Exp. Ther. 2000, 295, 431–437. [Google Scholar]
- Morello, K.C.; Wurz, G.T.; De Gregorio, M.W. Pharmacokinetics of Selective Estrogen Receptor Modulators. Clin. Pharmacokinet. 2003, 42, 361–372. [Google Scholar] [CrossRef] [PubMed]
- Simsa, P.; Mihalyi, A.; Kyama, C.M.; Mwenda, J.M.; Fülöp, V.; D’Hooghe, T.M. Selective Estrogen-Receptor Modulators and Aromatase Inhibitors: Promising New Medical Therapies for Endometriosis? Women’s Health 2007, 3, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Bedaiwy, M.A.; Alfaraj, S.; Yong, P.; Casper, R. New Developments in the Medical Treatment of Endometriosis. Fertil. Steril. 2017, 107, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Le Bouëdec, G.; Kauffmann, P.; Pingeon, J.M.; de Latour, M.; Lemesle, P.; Dauplat, J. Post-menopausal endometriosis developed during tamoxifen treatment. Rev. Fr. Gynecol. Obstet. 1991, 86, 407–410. [Google Scholar]
- Nath, A.; Sitruk-Ware, R. Pharmacology and Clinical Applications of Selective Estrogen Receptor Modulators. Climacteric 2009, 12, 188–205. [Google Scholar] [CrossRef]
- Altintas, D.; Kokcu, A.; Kandemir, B.; Tosun, M.; Cetinkaya, M.B. Comparison of the Effects of Raloxifene and Anastrozole on Experimental Endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2010, 150, 84–87. [Google Scholar] [CrossRef]
- Yao, Z.; Shen, X.; Capodanno, I.; Donnelly, M.; Fenyk-Melody, J.; Hausamann, J.; Nunes, C.; Strauss, J.; Vakerich, K. Validation of Rat Endometriosis Model by Using Raloxifene as a Positive Control for the Evaluation of Novel SERM Compounds. J. Investig. Surg. 2005, 18, 177–183. [Google Scholar] [CrossRef]
- Stratton, P.; Sinaii, N.; Segars, J.; Koziol, D.; Wesley, R.; Zimmer, C.; Winkel, C.; Nieman, L.K. Return of Chronic Pelvic Pain From Endometriosis After Raloxifene Treatment: A Randomized Controlled Trial. Obstet. Gynecol. 2008, 111, 88–96. [Google Scholar] [CrossRef]
- Kulak, J.; Fischer, C.; Komm, B.; Taylor, H.S. Treatment with Bazedoxifene, a Selective Estrogen Receptor Modulator, Causes Regression of Endometriosis in a Mouse Model. Endocrinology 2011, 152, 3226–3232. [Google Scholar] [CrossRef]
- Lusher, S.J.; Raaijmakers, H.C.A.; Vu-Pham, D.; Dechering, K.; Lam, T.W.; Brown, A.R.; Hamilton, N.M.; Nimz, O.; Bosch, R.; McGuire, R.; et al. Structural Basis for Agonism and Antagonism for a Set of Chemically Related Progesterone Receptor Modulators. J. Biol. Chem. 2011, 286, 35079–35086. [Google Scholar] [CrossRef]
- Mutter, G.L.; Bergeron, C.; Deligdisch, L.; Ferenczy, A.; Glant, M.; Merino, M.; Williams, A.R.W.; Blithe, D.L. The Spectrum of Endometrial Pathology Induced by Progesterone Receptor Modulators. Mod. Pathol. 2008, 21, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.R.W.; Bergeron, C.; Barlow, D.H.; Ferenczy, A. Endometrial Morphology after Treatment of Uterine Fibroids with the Selective Progesterone Receptor Modulator, Ulipristal Acetate. Int. J. Gynecol. Pathol. 2012, 31, 556–569. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, L.H.R.; Murray, A.A.; Matthews, R.; Shaw, G.; Williams, A.R.W.; Saunders, P.T.K.; Critchley, H.O.D. Selective Progesterone Receptor Modulator (SPRM) Ulipristal Acetate (UPA) and Its Effects on the Human Endometrium. Hum. Reprod. 2017, 32, 531–543. [Google Scholar] [CrossRef] [PubMed]
- De Milliano, I.; Van Hattum, D.; Ket, J.C.F.; Huirne, J.A.F.; Hehenkamp, W.J.K. Endometrial Changes during Ulipristal Acetate Use: A Systematic Review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 214, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Kettel, L.M.; Murphy, A.A.; Morales, A.J.; Ulmann, A.; Baulieu, E.E.; Yen, S.S. Treatment of Endometriosis with the Antiprogesterone Mifepristone (RU486). Fertil. Steril. 1996, 65, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Song, H.; Zhou, M.; Zhu, H.; Wang, Y.; Chen, H.; Huang, W. Progesterone Receptor Modulators for Endometriosis. Cochrane Database Syst. Rev. 2017, 7, CD009881. [Google Scholar] [CrossRef] [PubMed]
- DeManno, D.; Elger, W.; Garg, R.; Lee, R.; Schneider, B.; Hess-Stumpp, H.; Schubert, G.; Chwalisz, K. Asoprisnil (J867): A Selective Progesterone Receptor Modulator for Gynecological Therapy. Steroids 2003, 68, 1019–1032. [Google Scholar] [CrossRef]
- Chwalisz, K.; Perez, M.C.; DeManno, D.; Winkel, C.; Schubert, G.; Elger, W. Selective Progesterone Receptor Modulator Development and Use in the Treatment of Leiomyomata and Endometriosis. Endocr. Rev. 2005, 26, 423–438. [Google Scholar] [CrossRef]
- Williams, A.R.W.; Critchley, H.O.D.; Osei, J.; Ingamells, S.; Cameron, I.T.; Han, C.; Chwalisz, K. The Effects of the Selective Progesterone Receptor Modulator Asoprisnil on the Morphology of Uterine Tissues after 3 Months Treatment in Patients with Symptomatic Uterine Leiomyomata. Hum. Reprod. 2007, 22, 1696–1704. [Google Scholar] [CrossRef]
- Critchley, H.O.D.; Chodankar, R.R. 90 YEARS OF PROGESTERONE: Selective Progesterone Receptor Modulators in Gynaecological Therapies. J. Mol. Endocrinol. 2020, 65, T15–T33. [Google Scholar] [CrossRef]
- Middelkoop, M.; Bet, P.M.; Drenth, J.P.H.; Huirne, J.A.F.; Hehenkamp, W.J.K. Risk–Efficacy Balance of Ulipristal Acetate Compared to Surgical Alternatives. Br. J. Clin. Pharmacol. 2021, 87, 2685–2697. [Google Scholar] [CrossRef] [PubMed]
- Donnez, J. Liver Injury and Ulipristal Acetate: An Overstated Tragedy? Fertil. Steril. 2018, 110, 593–595. [Google Scholar] [CrossRef]
- Huniadi, C.A.; Pop, O.L.; Antal, T.A.; Stamatian, F. The Effects of Ulipristal on Bax/Bcl-2, Cytochrome c, Ki-67 and Cyclooxygenase-2 Expression in a Rat Model with Surgically Induced Endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 169, 360–365. [Google Scholar] [CrossRef]
- Department of Obstetrics and Gynecology; Bressler, L.H. Treatment of Endometriosis-Related Chronic Pelvic Pain with Ulipristal Acetate and Associated Endometrial Changes. HSOA J. Reprod. Med. Gynaecol. Obstet. 2017, 2, 8. [Google Scholar] [CrossRef]
- Donnez, J.; Dolmans, M.-M. Uterine Fibroid Management: From the Present to the Future. Hum. Reprod. Update 2016, 22, 665–686. [Google Scholar] [CrossRef]
- Wagenfeld, A.; Bone, W.; Schwede, W.; Fritsch, M.; Fischer, O.M.; Moeller, C. BAY 1002670: A Novel, Highly Potent and Selective Progesterone Receptor Modulator for Gynaecological Therapies. Hum. Reprod. 2013, 28, 2253–2264. [Google Scholar] [CrossRef] [PubMed]
- Schultze-Mosgau, M.-H.; Höchel, J.; Prien, O.; Zimmermann, T.; Brooks, A.; Bush, J.; Rottmann, A. Characterization of the Pharmacokinetics of Vilaprisan: Bioavailability, Excretion, Biotransformation, and Drug–Drug Interaction Potential. Clin. Pharmacokinet. 2018, 57, 1001–1015. [Google Scholar] [CrossRef] [PubMed]
- Wagenfeld, A.; Saunders, P.T.K.; Whitaker, L.; Critchley, H.O.D. Selective Progesterone Receptor Modulators (SPRMs): Progesterone Receptor Action, Mode of Action on the Endometrium and Treatment Options in Gynecological Therapies. Expert. Opin. Ther. Targets 2016, 20, 1045–1054. [Google Scholar] [CrossRef]
- Grandi, G.; Farulla, A.; Sileo, F.G.; Facchinetti, F. Levonorgestrel-Releasing Intra-Uterine Systems as Female Contraceptives. Expert. Opin. Pharmacother. 2018, 19, 677–686. [Google Scholar] [CrossRef]
- Schwartz, B.I.; Alexander, M.; Breech, L.L. Levonorgestrel Intrauterine Device Use for Medical Indications in Nulliparous Adolescents and Young Adults. J. Adolesc. Health 2021, 68, 357–363. [Google Scholar] [CrossRef]
- Zhu, S.-Y.; Wu, Y.-S.; Gu, Z.-Y.; Zhang, J.; Jia, S.-Z.; Shi, J.-H.; Dai, Y.; Leng, J.-H.; Li, X.-Y. Preventive Therapeutic Options for Postoperative Recurrence of Ovarian Endometrioma: Gonadotropin-Releasing Hormone Agonist with or without Levonorgestrel Intrauterine System Insertion. Arch. Gynecol. Obstet. 2021, 303, 533–539. [Google Scholar] [CrossRef]
- Gomes, M.K.O.; Rosa-e-Silva, J.C.; Garcia, S.B.; de Sá Rosa-e-Silva, A.C.J.; Turatti, A.; Vieira, C.S.; Ferriani, R.A. Effects of the Levonorgestrel-Releasing Intrauterine System on Cell Proliferation, Fas Expression and Steroid Receptors in Endometriosis Lesions and Normal Endometrium. Hum. Reprod. 2009, 24, 2736–2745. [Google Scholar] [CrossRef]
- Dunselman, G.A.J.; Vermeulen, N.; Becker, C.; Calhaz-Jorge, C.; D’Hooghe, T.; De Bie, B.; Heikinheimo, O.; Horne, A.W.; Kiesel, L.; Nap, A.; et al. ESHRE Guideline: Management of Women with Endometriosis. Hum. Reprod. 2014, 29, 400–412. [Google Scholar] [CrossRef]
- Vercellini, P.; Frontino, G.; De Giorgi, O.; Aimi, G.; Zaina, B.; Crosignani, P.G. Comparison of a Levonorgestrel-Releasing Intrauterine Device versus Expectant Management after Conservative Surgery for Symptomatic Endometriosis: A Pilot Study. Fertil. Steril. 2003, 80, 305–309. [Google Scholar] [CrossRef]
- Tosti, C.; Biscione, A.; Morgante, G.; Bifulco, G.; Luisi, S.; Petraglia, F. Hormonal Therapy for Endometriosis: From Molecular Research to Bedside. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 209, 61–66. [Google Scholar] [CrossRef]
- Chen, X.; Man, G.C.; Hung, S.W.; Zhang, T.; Fung, L.W.; Cheung, C.W.; Chung, J.P.; Li, T.C.; Wang, C.C. Therapeutic effects of green tea on endometriosis. Crit. Rev. Food Sci. Nutr. 2021, 63, 3222–3235. [Google Scholar] [CrossRef]
- Vallée, A.; Lecarpentier, Y. Curcumin and endometriosis. Int. J. Mol. Sci. 2020, 21, 2440. [Google Scholar] [CrossRef]
- D’Alterio, M.N.; Saponara, S.; Agus, M.; Laganà, A.S.; Noventa, M.; Loi, E.S.; Feki, A.; Angioni, S. Medical and surgical interventions to improve the quality of life for endometriosis patients: A systematic review. Gynecol. Surg. 2021, 18, 13. [Google Scholar] [CrossRef]
- Rafique, S.; Decherney, A.H. Medical Management of endometriosis. Clin. Obstet. Gynecol. 2017, 60, 485–496. [Google Scholar] [CrossRef]
- Brichant, G.; Laraki, I.; Henry, L.; Munaut, C.; Nisolle, M. New Therapeutics in Endometriosis: A Review of Hormonal, Non-Hormonal, and Non-Coding RNA Treatments. Int. J. Mol. Sci. 2021, 22, 10498. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Drug Category | Drugs | Mechanism of Action (in Endometriosis) | Adverse Effects/Toxicity | Molecule Structure of Representative Drug |
|---|---|---|---|---|
| NSAIDs | Ibuprofen, naproxen | Reversibly inhibits COX-1 and COX-2 → decreased prostaglandin formation | Gastrointestinal ulcers, edema, and renal impairment |  |
| Combined estrogen–progestin contraceptives | Ethynil-estradiol combined with norethindrone, norgestrel, levonorgestrel, and desogestrel | Inhibits FSH and LH; decreases cell proliferation and enhances endometrial apoptosis | Nausea, vomiting, breast tenderness, weight gain, acne, depression, fatigue, breakthrough bleeding, thromboembolism, and increased risk of developing estrogen-dependent cancers |  |
| Progestin-only preparations | Norethindrone, medroxyprogesterone, and levonorgestrel | Inhibits FSH and LH and stimulates atrophy/regression of endometrial lesions | Weight gain, acne, breast tenderness, depression, hirsutism, nausea, and peripheral edema |  |
| GnRH agonists | Leuprolide, goserelin | Inhibits steroidogenesis due to reduced FSH and LH levels | Hot flashes, vaginal atrophy, bone loss, and venous thromboembolism |  |
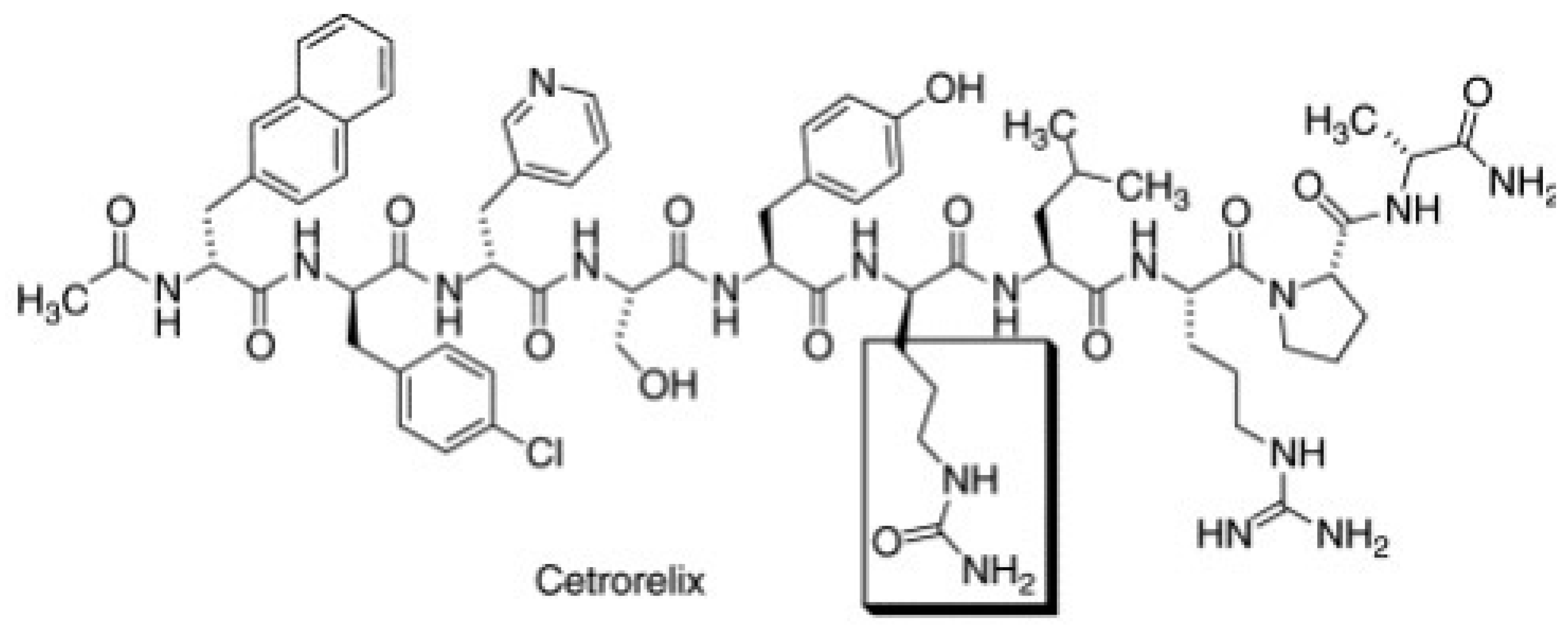
| GnRH antagonists | Elagolix, relugolix, and linzagolix | Suppression of LH secretion, competitive action on GnRH receptors in endometrial cells → inhibition of growth and proliferation of endometrial tissue | Hot flashes, fatigue, weight gain, and decreased libido |  |
| SPRMs | Ulipristal acetate, mifepristone, and asoprisnil | PR modulator-associated endometrial changes (PAEC) → endometrial antiproliferative effect | Nausea, vomiting, fatigue, diarrhea, headache, hot flushes, and loss of libido |  |
| Aromatase inhibitors | Letrozole, anastrozole | Blocks conversion of androgens to estrogen → decreased endometrial proliferation | Arthralgia, myalgia, and decreased bone mineral density (BMD) |  |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mikuš, M.; Šprem Goldštajn, M.; Laganà, A.S.; Vukorepa, F.; Ćorić, M. Clinical Efficacy, Pharmacokinetics, and Safety of the Available Medical Options in the Treatment of Endometriosis-Related Pelvic Pain: A Scoping Review. Pharmaceuticals 2023, 16, 1315. https://doi.org/10.3390/ph16091315
Mikuš M, Šprem Goldštajn M, Laganà AS, Vukorepa F, Ćorić M. Clinical Efficacy, Pharmacokinetics, and Safety of the Available Medical Options in the Treatment of Endometriosis-Related Pelvic Pain: A Scoping Review. Pharmaceuticals. 2023; 16(9):1315. https://doi.org/10.3390/ph16091315
Chicago/Turabian StyleMikuš, Mislav, Marina Šprem Goldštajn, Antonio Simone Laganà, Franka Vukorepa, and Mario Ćorić. 2023. "Clinical Efficacy, Pharmacokinetics, and Safety of the Available Medical Options in the Treatment of Endometriosis-Related Pelvic Pain: A Scoping Review" Pharmaceuticals 16, no. 9: 1315. https://doi.org/10.3390/ph16091315