
Concurrent Imaging and Clinical Study of the Efficacy of Hyaluronic Acid Injection for Knee Osteoarthritis: A Synovial Membrane Investigation with Ultrasound Imaging

Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
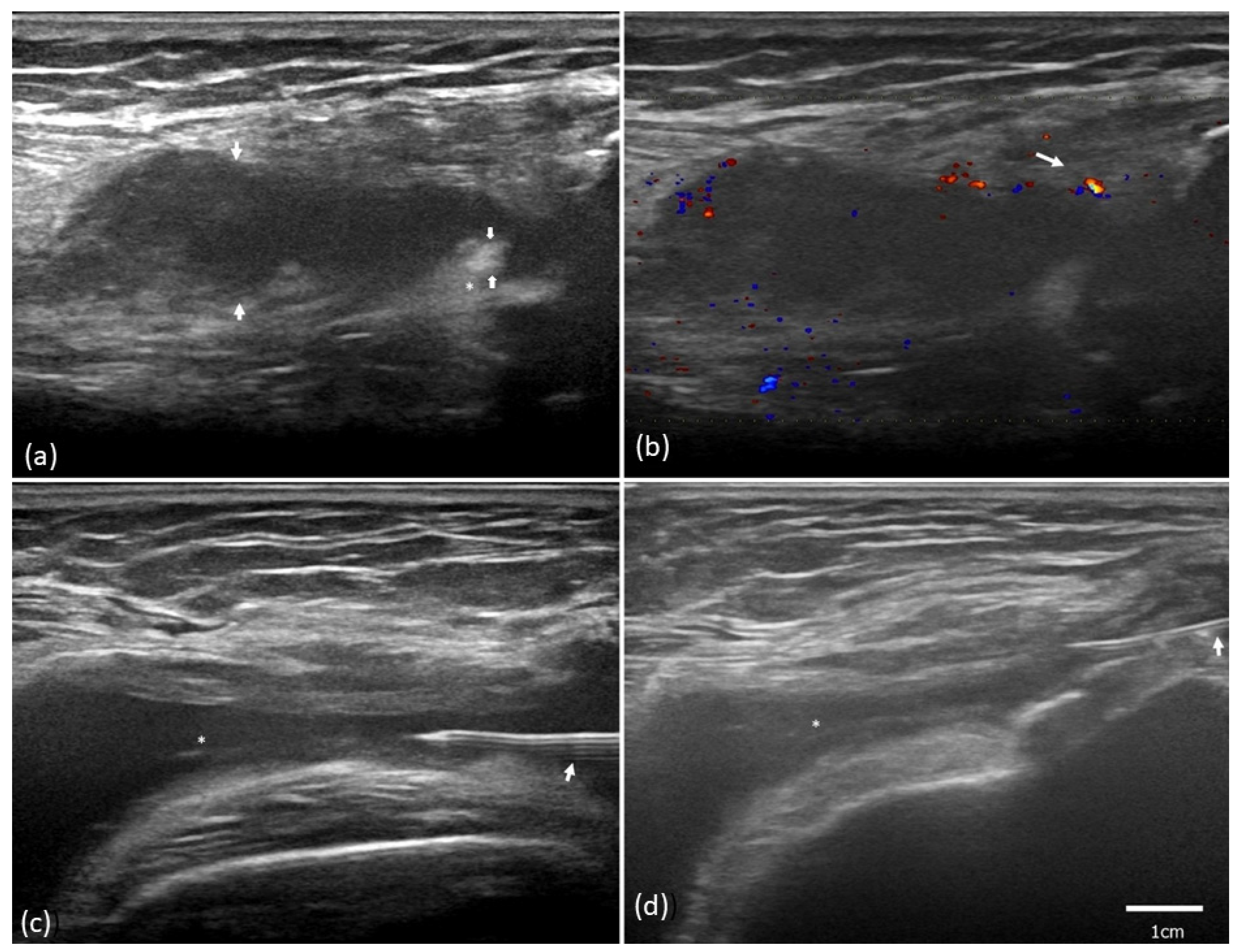
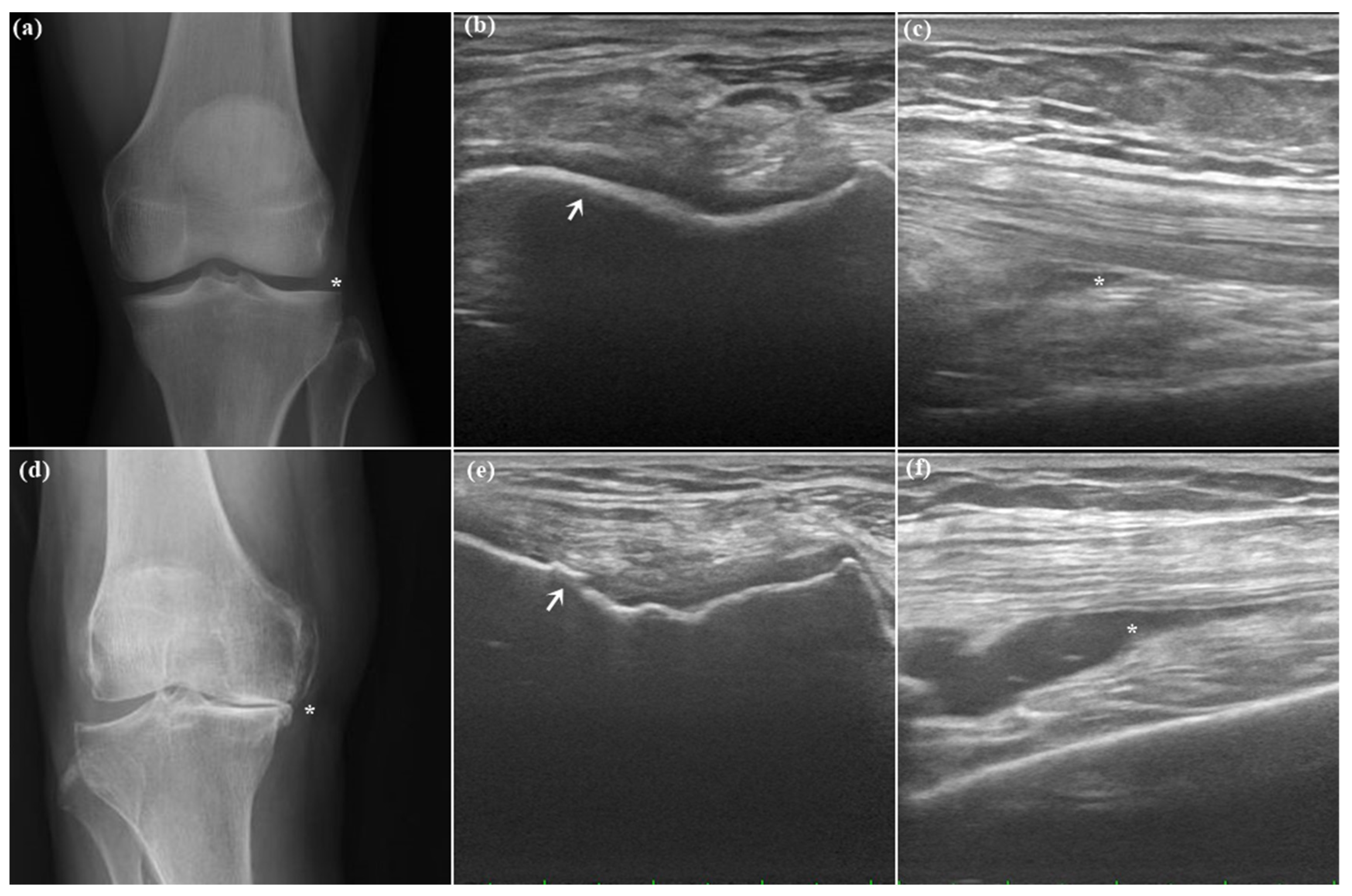
2.2. Ultrasound Synovial Outcome
2.3. Association between Ultrasound and Clinical Symptoms
3. Discussion
4. Materials and Methods
4.1. Participants
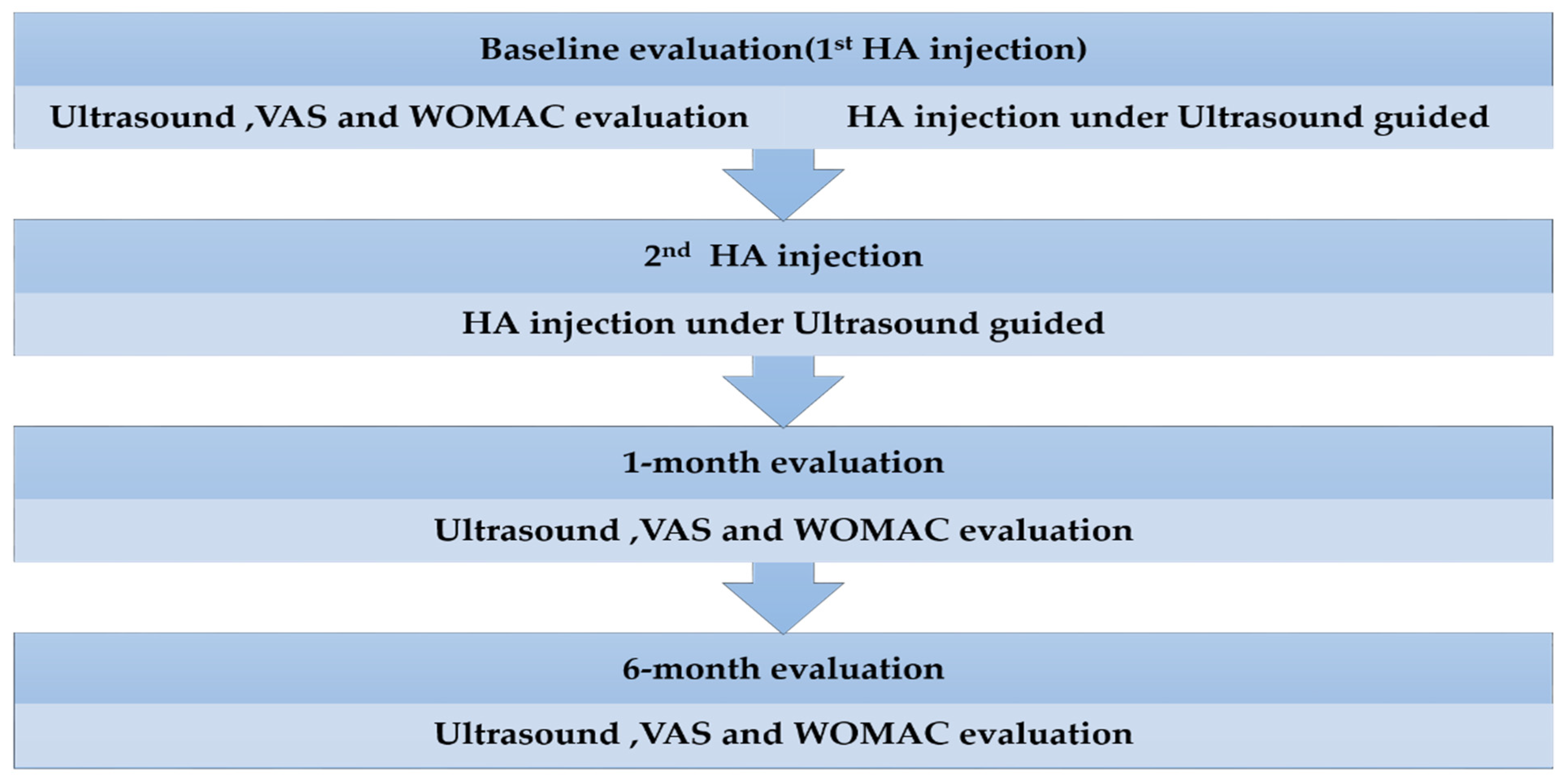
4.2. Drug Administration
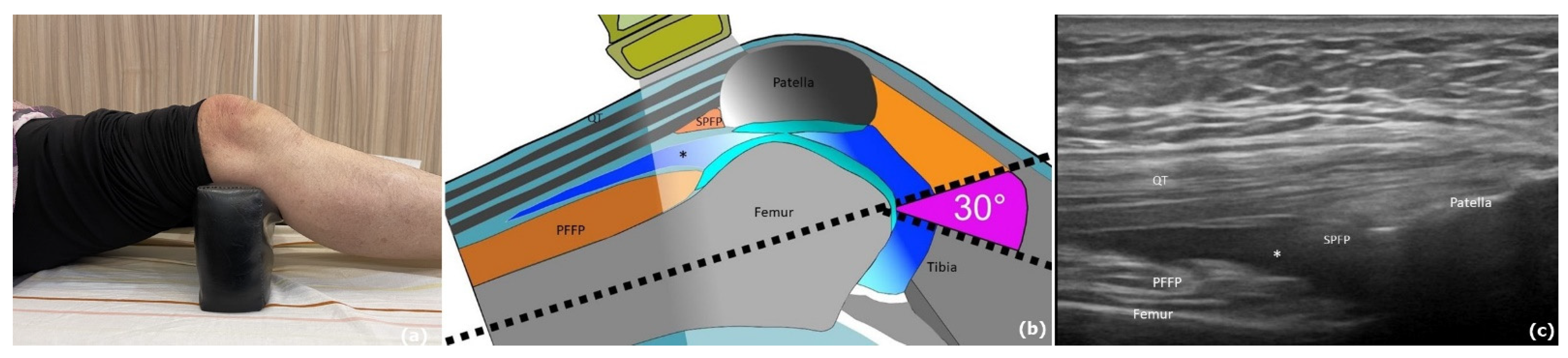
4.3. Ultrasound Evaluation
4.4. Clinical Outcome Measurement
4.5. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prieto-Alhambra, D.; Judge, A.; Javaid, M.K.; Cooper, C.; Diez-Perez, A.; Arden, N.K. Incidence and risk factors for clinically diagnosed knee, hip and hand osteoarthritis: Influences of age, gender and osteoarthritis affecting other joints. Ann. Rheum. Dis. 2014, 73, 1659–1664. [Google Scholar] [CrossRef] [PubMed]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29–30, 100587. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Schofield, D.; Callander, E. The individual and socioeconomic impact of osteoarthritis. Nat. Rev. Rheumatol. 2014, 10, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Malanga, G.; Niazi, F.; Kidd, V.D.; Lau, E.; Kurtz, S.M.; Ong, K.L.; Concoff, A.L. Knee Osteoarthritis Treatment Costs in the Medicare Patient Population. Am. Health Drug Benefits 2020, 13, 144–153. [Google Scholar]
- Macchi, V.; Stocco, E.; Stecco, C.; Belluzzi, E.; Favero, M.; Porzionato, A.; De Caro, R. The infrapatellar fat pad and the synovial membrane: An anatomo-functional unit. J. Anat. 2018, 233, 146–154. [Google Scholar] [CrossRef]
- Robinson, W.H.; Lepus, C.M.; Wang, Q.; Raghu, H.; Mao, R.; Lindstrom, T.M.; Sokolove, J. Low-grade inflammation as a key mediator of the pathogenesis of osteoarthritis. Nat. Rev. Rheumatol. 2016, 12, 580–592. [Google Scholar] [CrossRef]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Bacon, K.; LaValley, M.P.; Jafarzadeh, S.R.; Felson, D. Does cartilage loss cause pain in osteoarthritis and if so, how much? Ann. Rheum. Dis. 2020, 79, 1105–1110. [Google Scholar] [CrossRef]
- Wallace, G.; Cro, S.; Doré, C.; King, L.; Kluzek, S.; Price, A.; Roemer, F.; Guermazi, A.; Keen, R.; Arden, N. Associations Between Clinical Evidence of Inflammation and Synovitis in Symptomatic Knee Osteoarthritis: A Cross-Sectional Substudy. Arthritis Care Res. 2017, 69, 1340–1348. [Google Scholar] [CrossRef]
- Veronese, N.; Cooper, C.; Reginster, J.Y.; Hochberg, M.; Branco, J.; Bruyère, O.; Chapurlat, R.; Al-Daghri, N.; Dennison, E.; Herrero-Beaumont, G.; et al. Type 2 diabetes mellitus and osteoarthritis. Semin. Arthritis Rheum. 2019, 49, 9–19. [Google Scholar] [CrossRef]
- Courties, A.; Sellam, J. Osteoarthritis and type 2 diabetes mellitus: What are the links? Diabetes Res. Clin. Pract. 2016, 122, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Roman-Blas, J.A.; Castañeda, S.; Sánchez-Pernaute, O.; Largo, R.; Herrero-Beaumont, G.; Blanco, F.J.; Gómez, R.B.; Burlato, M.C.; González, C.G.; Vázquez, J.L.G.; et al. Combined Treatment with Chondroitin Sulfate and Glucosamine Sulfate Shows No Superiority over Placebo for Reduction of Joint Pain and Functional Impairment in Patients with Knee Osteoarthritis: A Six-Month Multicenter, Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Arthritis Rheumatol. 2017, 69, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Bruns, C.; Labisch, S.; Dirks, J.H. 3D escape: An alternative paradigm for spatial orientation studies in insects. J. Comp. Physiol. A Neuroethol. Sens. Neural Behav. Physiol. 2022, 209, 285–297. [Google Scholar] [CrossRef] [PubMed]
- Meng, Z.; Liu, J.; Zhou, N. Efficacy and safety of the combination of glucosamine and chondroitin for knee osteoarthritis: A systematic review and meta-analysis. Arch. Orthop. Trauma Surg. 2023, 143, 409–421. [Google Scholar] [CrossRef]
- da Costa, B.R.; Pereira, T.V.; Saadat, P.; Rudnicki, M.; Iskander, S.M.; Bodmer, N.S.; Bobos, P.; Gao, L.; Kiyomoto, H.D.; Montezuma, T.; et al. Effectiveness and safety of non-steroidal anti-inflammatory drugs and opioid treatment for knee and hip osteoarthritis: Network meta-analysis. BMJ (Clin. Res. Ed.) 2021, 375, n2321. [Google Scholar] [CrossRef]
- Maheu, E.; Bannuru, R.R.; Herrero-Beaumont, G.; Allali, F.; Bard, H.; Migliore, A. Why we should definitely include intra-articular hyaluronic acid as a therapeutic option in the management of knee osteoarthritis: Results of an extensive critical literature review. Semin. Arthritis Rheum. 2019, 48, 563–572. [Google Scholar] [CrossRef]
- Ghosh, P.; Guidolin, D. Potential mechanism of action of intra-articular hyaluronan therapy in osteoarthritis: Are the effects molecular weight dependent? Semin. Arthritis Rheum. 2002, 32, 10–37. [Google Scholar] [CrossRef]
- Lin, W.; Liu, Z.; Kampf, N.; Klein, J. The Role of Hyaluronic Acid in Cartilage Boundary Lubrication. Cells 2020, 9, 1606. [Google Scholar] [CrossRef]
- Iannitti, T.; Lodi, D.; Palmieri, B. Intra-articular injections for the treatment of osteoarthritis: Focus on the clinical use of hyaluronic acid. Drugs RD 2011, 11, 13–27. [Google Scholar] [CrossRef]
- Gotoh, S.; Onaya, J.; Abe, M.; Miyazaki, K.; Hamai, A.; Horie, K.; Tokuyasu, K. Effects of the molecular weight of hyaluronic acid and its action mechanisms on experimental joint pain in rats. Ann. Rheum. Dis. 1993, 52, 817–822. [Google Scholar] [CrossRef]
- Wang, C.C.; Lee, S.H.; Lin, H.Y.; Liu, F.W.; Chiou, H.J.; Chan, R.C.; Chou, C.L. Short-term effect of ultrasound-guided low-molecular-weight hyaluronic acid injection on clinical outcomes and imaging changes in patients with rheumatoid arthritis of the ankle and foot joints. A randomized controlled pilot trial. Mod. Rheumatol. 2017, 27, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.; Wang, C.T.; Chou, W.C.; Kao, C.L.; Tsai, K.L. Hyaluronic acid injection reduces inflammatory and apoptotic markers through modulation of AKT by repressing the oxidative status of neutrophils from osteoarthritic synovial fluid. Int. J. Biol. Macromol. 2020, 165, 2765–2772. [Google Scholar] [CrossRef] [PubMed]
- Leighton, R.; Akermark, C.; Therrien, R.; Richardson, J.B.; Andersson, M.; Todman, M.G.; Arden, N.K. NASHA hyaluronic acid vs. methylprednisolone for knee osteoarthritis: A prospective, multi-centre, randomized, non-inferiority trial. Osteoarthr. Cartil. 2014, 22, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.A.; Erickson, B.J.; Saltzman, B.M.; Mascarenhas, R.; Bach, B.R., Jr.; Cole, B.J.; Verma, N.N. Is Local Viscosupplementation Injection Clinically Superior to Other Therapies in the Treatment of Osteoarthritis of the Knee: A Systematic Review of Overlapping Meta-analyses. Arthroscopy 2015, 31, 2036–2045. [Google Scholar] [CrossRef]
- Pasquali Ronchetti, I.; Guerra, D.; Taparelli, F.; Boraldi, F.; Bergamini, G.; Mori, G.; Zizzi, F.; Frizziero, L. Morphological analysis of knee synovial membrane biopsies from a randomized controlled clinical study comparing the effects of sodium hyaluronate (Hyalgan) and methylprednisolone acetate (Depomedrol) in osteoarthritis. Rheumatology 2001, 40, 158–169. [Google Scholar] [CrossRef]
- Pereira, T.V.; Jüni, P.; Saadat, P.; Xing, D.; Yao, L.; Bobos, P.; Agarwal, A.; Hincapié, C.A.; da Costa, B.R. Viscosupplementation for knee osteoarthritis: Systematic review and meta-analysis. BMJ (Clin. Res. Ed.) 2022, 378, e069722. [Google Scholar] [CrossRef]
- Zhao, K.; Wen, Y.; Bunpetch, V.; Lin, J.; Hu, Y.; Zhang, X.; Xie, Y.; Zhang, S.; Hongwei, O. Hype or hope of hyaluronic acid for osteoarthritis: Integrated clinical evidence synthesis with multi-organ transcriptomics. J. Orthop. Transl. 2022, 32, 91–100. [Google Scholar] [CrossRef]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. 2020, 72, 220–233. [Google Scholar] [CrossRef]
- Jevsevar, D.S.; Brown, G.A.; Jones, D.L.; Matzkin, E.G.; Manner, P.A.; Mooar, P.; Schousboe, J.T.; Stovitz, S.; Sanders, J.O.; Bozic, K.J.; et al. The American Academy of Orthopaedic Surgeons evidence-based guideline on: Treatment of osteoarthritis of the knee, 2nd edition. J. Bone Jt. Surg. Am. 2013, 95, 1885–1886. [Google Scholar] [CrossRef]
- Johansen, M.; Bahrt, H.; Altman, R.D.; Bartels, E.M.; Juhl, C.B.; Bliddal, H.; Lund, H.; Christensen, R. Exploring reasons for the observed inconsistent trial reports on intra-articular injections with hyaluronic acid in the treatment of osteoarthritis: Meta-regression analyses of randomized trials. Semin. Arthritis Rheum. 2016, 46, 34–48. [Google Scholar] [CrossRef]
- Kohn, M.D.; Sassoon, A.A.; Fernando, N.D. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clin. Orthop. Relat. Res. 2016, 474, 1886–1893. [Google Scholar] [CrossRef]
- Kaeley, G.S.; Bakewell, C.; Deodhar, A. The importance of ultrasound in identifying and differentiating patients with early inflammatory arthritis: A narrative review. Arthritis Res. Ther. 2020, 22, 1. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S. Overview of musculoskeletal ultrasound for the clinical rheumatologist. Clin. Exp. Rheumatol. 2018, 36 (Suppl. S1), 3–9. [Google Scholar]
- Möller, I.; Janta, I.; Backhaus, M.; Ohrndorf, S.; Bong, D.A.; Martinoli, C.; Filippucci, E.; Sconfienza, L.M.; Terslev, L.; Damjanov, N.; et al. The 2017 EULAR standardised procedures for ultrasound imaging in rheumatology. Ann. Rheum. Dis. 2017, 76, 1974–1979. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.; Wang, C.T.; Tsai, K.L.; Chou, C.L.; Chao, J.K.; Huang, H.Y.; Kao, C.L. Effect of ultrasound-detected synovitis on therapeutic efficacy of hyaluronic acid injection for symptomatic knee osteoarthritis. Rheumatology 2021, 60, 4486–4494. [Google Scholar] [CrossRef] [PubMed]
- Kahle, W.; Frotscher, M. Color Atlas and Textbook of Human Anatomy, 5th ed.; Thieme Flexibooks: Stuttgart, Germany; New York, NY, USA, 2002; p. v. <1,3>. [Google Scholar]
- Gomis, A.; Miralles, A.; Schmidt, R.F.; Belmonte, C. Intra-articular injections of hyaluronan solutions of different elastoviscosity reduce nociceptive nerve activity in a model of osteoarthritic knee joint of the guinea pig. Osteoarthr. Cartil. 2009, 17, 798–804. [Google Scholar] [CrossRef]
- Dray, A.; Read, S.J. Arthritis and pain. Future targets to control osteoarthritis pain. Arthritis Res. Ther. 2007, 9, 212. [Google Scholar] [CrossRef]
- Belluzzi, E.; Stocco, E.; Pozzuoli, A.; Granzotto, M.; Porzionato, A.; Vettor, R.; De Caro, R.; Ruggieri, P.; Ramonda, R.; Rossato, M.; et al. Contribution of Infrapatellar Fat Pad and Synovial Membrane to Knee Osteoarthritis Pain. BioMed Res. Int. 2019, 2019, 6390182. [Google Scholar] [CrossRef]
- Eitner, A.; Pester, J.; Nietzsche, S.; Hofmann, G.O.; Schaible, H.G. The innervation of synovium of human osteoarthritic joints in comparison with normal rat and sheep synovium. Osteoarthr. Cartil. 2013, 21, 1383–1391. [Google Scholar] [CrossRef]
- Gomis, A.; Miralles, A.; Schmidt, R.F.; Belmonte, C. Nociceptive nerve activity in an experimental model of knee joint osteoarthritis of the guinea pig: Effect of intra-articular hyaluronan application. Pain 2007, 130, 126–136. [Google Scholar] [CrossRef]
- Karatay, S.; Kiziltunc, A.; Yildirim, K.; Karanfil, R.C.; Senel, K. Effects of different hyaluronic acid products on synovial fluid levels of intercellular adhesion molecule-1 and vascular cell adhesion molecule-1 in knee osteoarthritis. Ann. Clin. Lab. Sci. 2004, 34, 330–335. [Google Scholar] [PubMed]
- Olivotto, E.; Trisolino, G.; Belluzzi, E.; Lazzaro, A.; Strazzari, A.; Pozzuoli, A.; Cigolotti, A.; Ruggieri, P.; Evangelista, A.; Ometto, F.; et al. Macroscopic Synovial Inflammation Correlates with Symptoms and Cartilage Lesions in Patients Undergoing Arthroscopic Partial Meniscectomy: A Clinical Study. J. Clin. Med. 2022, 11, 4330. [Google Scholar] [CrossRef] [PubMed]
- Fang, W.H.; Chen, X.T.; Vangsness, C.T., Jr. Ultrasound-Guided Knee Injections Are More Accurate Than Blind Injections: A Systematic Review of Randomized Controlled Trials. Arthrosc. Sports Med. Rehabil. 2021, 3, e1177–e1187. [Google Scholar] [CrossRef] [PubMed]
- Reichenbach, S.; Rutjes, A.W.; Nüesch, E.; Trelle, S.; Jüni, P. Joint lavage for osteoarthritis of the knee. Cochrane Database Syst. Rev. 2010, 12, Cd007320. [Google Scholar] [CrossRef] [PubMed]
- Paschos, N.K.; Giotis, D.; Abuhemoud, K.; Georgoulis, A.D. Effectiveness of aspiration in knee joint effusion management: A prospective randomized controlled study. Knee Surgery Sports Traumatol. Arthrosc. 2014, 22, 226–232. [Google Scholar] [CrossRef]
- Calvet, J.; Orellana, C.; Galisteo, C.; Garcia-Manrique, M.; Navarro, N.; Caixas, A.; Larrosa, M.; Gratacos, J. Clinical and ultrasonographic features associated to response to intraarticular corticosteroid injection. A one year follow up prospective cohort study in knee osteoarthritis patient with joint effusion. PLoS ONE 2018, 13, e0191342. [Google Scholar] [CrossRef]
- Beitinger, N.; Ehrenstein, B.; Schreiner, B.; Fleck, M.; Grifka, J.; Lüring, C.; Hartung, W. The value of colour Doppler sonography of the knee joint: A useful tool to discriminate inflammatory from non-inflammatory disease? Rheumatology 2013, 52, 1425–1428. [Google Scholar] [CrossRef]
- Parisi, S.; Ditto, M.C.; Priora, M.; Borrelli, R.; Laganà, A.; Peroni, C.L.; Fusaro, E. Ultrasound-guided intra-articular injection: Efficacy of hyaluronic acid compared to glucocorticoid in the treatment of knee osteoarthritis. Minerva Medica 2019, 110, 515–523. [Google Scholar] [CrossRef]
- Ingegnoli, F.; Soldi, A.; Meroni, P.L. Power Doppler sonography and clinical monitoring for hyaluronic Acid treatment of rhizarthrosis: A pilot study. J. Hand Microsurg. 2011, 3, 51–54. [Google Scholar] [CrossRef]
- Roemer, F.W.; Guermazi, A.; Felson, D.T.; Niu, J.; Nevitt, M.C.; Crema, M.D.; Lynch, J.A.; Lewis, C.E.; Torner, J.; Zhang, Y. Presence of MRI-detected joint effusion and synovitis increases the risk of cartilage loss in knees without osteoarthritis at 30-month follow-up: The MOST study. Ann. Rheum. Dis. 2011, 70, 1804–1809. [Google Scholar] [CrossRef]
- Crema, M.D.; Roemer, F.W.; Li, L.; Alexander, R.C.; Chessell, I.P.; Dudley, A.D.; Karlsten, R.; Rosen, L.B.; Guermazi, A. Comparison between semiquantitative and quantitative methods for the assessment of knee synovitis in osteoarthritis using non-enhanced and gadolinium-enhanced MRI. Osteoarthr. Cartil. 2017, 25, 267–271. [Google Scholar] [CrossRef]
- Liu, H.; Huang, C.; Chen, S.; Zheng, Q.; Ye, Y.; Ye, Z.; Lv, G. Value of contrast-enhanced ultrasound for detection of synovial vascularity in experimental rheumatoid arthritis: An exploratory study. J. Int. Med. Res. 2019, 47, 5740–5751. [Google Scholar] [CrossRef]
- Felson, D.T.; McAlindon, T.E.; Anderson, J.J.; Naimark, A.; Weissman, B.W.; Aliabadi, P.; Evans, S.; Levy, D.; LaValley, M.P. Defining radiographic osteoarthritis for the whole knee. Osteoarthr. Cartil. 1997, 5, 241–250. [Google Scholar] [CrossRef]
- Altman, R.; Asch, E.; Bloch, D.; Bole, G.; Borenstein, D.; Brandt, K.; Christy, W.; Cooke, T.D.; Greenwald, R.; Hochberg, M.; et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986, 29, 1039–1049. [Google Scholar] [CrossRef]
- Huang, T.L.; Chang, C.C.; Lee, C.H.; Chen, S.C.; Lai, C.H.; Tsai, C.L. Intra-articular injections of sodium hyaluronate (Hyalgan®) in osteoarthritis of the knee. a randomized, controlled, double-blind, multicenter trial in the Asian population. BMC Musculoskelet. Disord. 2011, 12, 221. [Google Scholar] [CrossRef] [PubMed]
- Torp-Pedersen, S.T.; Terslev, L. Settings and artefacts relevant in colour/power Doppler ultrasound in rheumatology. Ann. Rheum. Dis. 2008, 67, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Sarmanova, A.; Hall, M.; Fernandes, G.S.; Valdes, A.M.; Walsh, D.A.; Doherty, M.; Zhang, W. Thresholds of ultrasound synovial abnormalities for knee osteoarthritis—A cross sectional study in the general population. Osteoarthr. Cartil. 2019, 27, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Sarmanova, A.; Hall, M.; Fernandes, G.S.; Bhattacharya, A.; Valdes, A.M.; Walsh, D.A.; Doherty, M.; Zhang, W. Association between ultrasound-detected synovitis and knee pain: A population-based case-control study with both cross-sectional and follow-up data. Arthritis Res. Ther. 2017, 19, 281. [Google Scholar] [CrossRef] [PubMed]
- Torp-Pedersen, S.; Christensen, R.; Szkudlarek, M.; Ellegaard, K.; D′Agostino, M.A.; Iagnocco, A.; Naredo, E.; Balint, P.; Wakefield, R.J.; Torp-Pedersen, A.; et al. Power and color Doppler ultrasound settings for inflammatory flow: Impact on scoring of disease activity in patients with rheumatoid arthritis. Arthritis Rheumatol. 2015, 67, 386–395. [Google Scholar] [CrossRef]
- Szkudlarek, M.; Court-Payen, M.; Strandberg, C.; Klarlund, M.; Klausen, T.; Ostergaard, M. Power Doppler ultrasonography for assessment of synovitis in the metacarpophalangeal joints of patients with rheumatoid arthritis: A comparison with dynamic magnetic resonance imaging. Arthritis Rheum 2001, 44, 2018–2023. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| N | 103 |
| Age (years), mean (95% CI) | 70.09 (66.6–73.9) |
| M:F ratio, % | 42:61 |
| BMI (Kg/m2), mean (95% CI) | 25.1 (22.9–27.2) |
| OA stage, median (IQR) | 2 (1–4) |
| Disease duration (month), mean (95% CI) | 22.22 (11.12–33) |
| Characteristics | Baseline | 1-Month Evaluation | 6-Month Evaluation | p Value (1 Month to Baseline) | p Value (6 Months to Baseline) |
|---|---|---|---|---|---|
| Effusion | 0.49 (0.43–0.56) | 0.50 (0.43–0.57) | 0.48 (0.42–0.54) | 0.49 | 0.118 |
| Synovial hypertrophy | 0.34 (0.28–0.41) | 0.35 (0.28–0.41) | 0.38 (0.31–0.44) | 0.918 | 0.446 |
| Color flow Doppler | 0.64 (0.50–0.78) | 0.63 (0.49–0.77) | 0.58 (0.44–0.72) | 0.102 | 0.06 |
| Global pain (VAS) | 50.3 (40.3–55.3) | 37.3 (26.8–47.7) * | 36.0 (31.1–41.0) * | <0.001 | <0.001 |
| WOMAC | 46.7 (42.6–50.8) | 27.1 (22.9–31.1) * | 42 (37.8–49.3) | <0.001 | 0.25 |
| Color Doppler Grade | 0 | 1 | 2 |
|---|---|---|---|
| Baseline evaluation | n = 39 (37.9%) | n = 61 (59.2%) | 3 (2.9%) |
| 1-month evaluation | n = 42 (40.8%) | n = 58 (56.3%) | 3 (2.9%) |
| 6-month evaluation | n = 47 (45.6%) | n = 53 (51.5%) | 3 (2.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.-C.; Hu, T.-M.; Chen, C.-L.; Hong, C.-C.; Chang, Y.-H.; Kao, C.-L. Concurrent Imaging and Clinical Study of the Efficacy of Hyaluronic Acid Injection for Knee Osteoarthritis: A Synovial Membrane Investigation with Ultrasound Imaging. Pharmaceuticals 2023, 16, 1186. https://doi.org/10.3390/ph16081186
Wang C-C, Hu T-M, Chen C-L, Hong C-C, Chang Y-H, Kao C-L. Concurrent Imaging and Clinical Study of the Efficacy of Hyaluronic Acid Injection for Knee Osteoarthritis: A Synovial Membrane Investigation with Ultrasound Imaging. Pharmaceuticals. 2023; 16(8):1186. https://doi.org/10.3390/ph16081186
Chicago/Turabian StyleWang, Chien-Chih, Tsung-Ming Hu, Chien-Lung Chen, Chung-Chih Hong, Yu-Hui Chang, and Chung-Lan Kao. 2023. "Concurrent Imaging and Clinical Study of the Efficacy of Hyaluronic Acid Injection for Knee Osteoarthritis: A Synovial Membrane Investigation with Ultrasound Imaging" Pharmaceuticals 16, no. 8: 1186. https://doi.org/10.3390/ph16081186