
Insulin-like Growth Factor-1 (IGF-1) Related Drugs in Pain Management
{kind=link}
Abstract
:1. Introduction
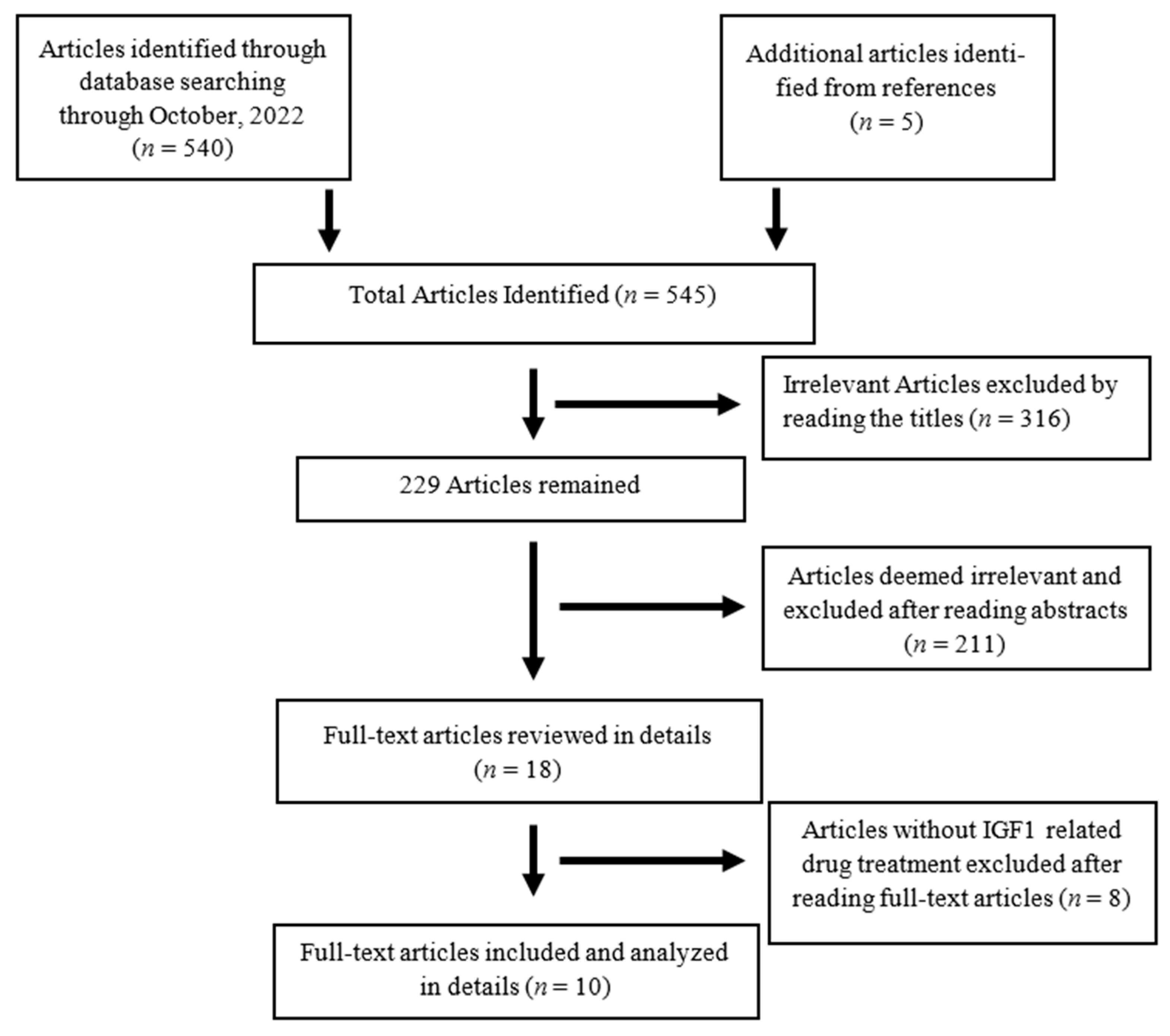
2. Methods
3. Results
3.1. IGF-1 on Neuropathic Pain
3.2. IGF-1 in Other Pain Conditions
3.3. IGF-1 on Pain in Humans
4. Discussion
Research Gaps and Prospects
5. Concluding Remarks
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Institute of Medicine. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research; The National Academies Press: Washington, DC, USA, 2011; pp. 1–364. [Google Scholar] [CrossRef]
- Denko, C.W.; Malemud, C.J. Role of the growth hormone/insulin-like growth factor-1 paracrine axis in rheumatic diseases. Semin Arthritis Rheum. 2005, 35, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Leal-Cerro, A.; Povedano, J.; Astorga, R.; Gonzalez, M.; Silva, H.; García-Pesquera, F.; Casanueva, F.F.; Diéguez, C. The growth hormone (GH)-releasing hormone-GH-insulin-like growth factor-1 axis in patients with fibromyalgia syndrome. J. Clin. Endocrinol. Metab. 1999, 84, 3378–3381. [Google Scholar] [CrossRef] [PubMed]
- Dubick, M.N.; Ravin, T.H.; Michel, Y.; Morrisette, D.C. Use of localized human growth hormone and testosterone injections in addition to manual therapy and exercise for lower back pain: A case series with 12-month follow-up. J. Pain Res. 2015, 8, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Bennett, R.M.; Clark, S.C.; Walczyk, J. A randomized, double-blind, placebo-controlled study of growth hormone in the treatment of fibromyalgia. Am. J. Med. 1998, 104, 227–231. [Google Scholar] [CrossRef]
- Cuatrecasas, G.; Alegre, C.; Fernandezsola, J.; Gonzalez, M.J.; Garciafructuoso, F.J.; Pocadias, V.; Nadal, A.; Cuatrecasas, G.; Navarro, F.J.; Mera, A.C.; et al. Growth hormone treatment for sustained pain reduction and improvement in quality of life in severe fibromyalgia. Pain 2012, 153, 1382–1389. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Casserly, E.; Yin, Y.; Cheng, J. A Systematic Review of Growth Hormone in Pain Medicine: From Rodents to Humans. Pain Med. 2020, 21, 21–31. [Google Scholar] [CrossRef]
- Cheng, J. Growth hormone treatment for sustained pain reduction and improvement in quality of life in severe fibromyalgia-too important to be tarnished by inconsistencies. Pain 2013, 154, 620. [Google Scholar] [CrossRef]
- Hepler, J.E.; Lund, P.K. Molecular biology of the insulin-like growth factors. Relevance to nervous system function. Mol. Neurobiol. 1990, 4, 93–127. [Google Scholar] [CrossRef]
- Hefti, F.; Hartikka, J.; Knusel, B. Function of neurotrophic factors in the adult and aging brain and their possible use in the treatment of neurodegenerative diseases. Neurobiol. Aging. 1989, 10, 515–533. [Google Scholar] [CrossRef]
- Becker, K.; Stegenga, S.; Conway, S. Role of insulin-like growth factor I in regulating growth hormone release and feedback in the male rat. Neuroendocrinology 1995, 61, 573–583. [Google Scholar] [CrossRef] [PubMed]
- Zackenfels, K.; Rohrer, H. IGF-I stimulates chick sympathetic neuron proliferation in vitro and in vivo. Ann. N. Y. Acad. Sci. 1993, 692, 302–303. [Google Scholar] [CrossRef] [PubMed]
- Hansson, H.-A.; Nilsson, A.; Isgaard, J.; Billig, H.; Isaksson, O.; Skottner, A.; Andersson, I.K.; Rozell, B. Immunohistochemical localization of insulin-like growth factor I in the adult rat. Histochemistry 1988, 89, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Sjöberg, J.; Kanje, M. Insulin-like growth factor (IGF-1) as a stimulator of regeneration in the freeze-injured rat sciatic nerve. Brain Res. 1989, 485, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Kanje, M.; Skottner, A.; Sjöberg, J.; Lundborg, G. Insulin-like growth factor I (IGF-I) stimulates regeneration of the rat sciatic nerve. Brain Res. 1989, 486, 396–398. [Google Scholar] [CrossRef]
- Ishii, D.N.; Glazner, G.W.; Pu, S.F. Role of insulin-like growth factors in peripheral nerve regeneration. Pharmacol Ther. 1994, 62, 125–144. [Google Scholar] [CrossRef]
- Glazner, G.W.; Lupien, S.; Miller, J.A.; Ishii, D.N. Insulin-like growth factor II increases the rate of sciatic nerve regeneration in rats. Neuroscience 1993, 54, 791–797. [Google Scholar] [CrossRef]
- Ishii, D.N.; Lupien, S.B. Insulin-like growth factors protect against diabetic neuropathy: Effects on sensory nerve regeneration in rats. J. Neurosci. Res. 1995, 40, 138–144. [Google Scholar] [CrossRef]
- Apfel, S.C.; Arezzo, J.C.; Lewis, M.E.; Kessler, J.A. The use of insulin-like growth factor I in the prevention of vincristine neuropathy in mice. Ann. N. Y. Acad. Sci. 1993, 692, 243–245. [Google Scholar] [CrossRef]
- Pluijms, W.; Huygen, F.; Cheng, J.; Mekhail, N.; Van Kleef, M.; Van Zundert, J.; Van Dongen, R. Evidence-based interventional pain medicine according to clinical diagnoses. 18. Painful diabetic polyneuropathy. Pain Pract. 2011, 11, 191–198. [Google Scholar] [CrossRef]
- Xu, L.; Sun, Z.; Casserly, E.; Nasr, C.; Cheng, J.; Xu, J. Advances in Interventional Therapies for Painful Diabetic Neuropathy: A Systematic Review. Anesth. Analg. 2022, 134, 1215–1228. [Google Scholar] [CrossRef]
- Dyer, A.H.; Vahdatpour, C.; Sanfeliu, A.; Tropea, D. The role of Insulin-Like Growth Factor 1 (IGF-1) in brain development, maturation and neuroplasticity. Neuroscience 2016, 325, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Kappeler, L.; Filho, C.D.M.; Dupont, J.; Leneuve, P.; Cervera, P.; Périn, L.; Loudes, C.; Blaise, A.; Klein, R.; Epelbaum, J.; et al. Brain IGF-1 receptors control mammalian growth and lifespan through a neuroendocrine mechanism. PLoS Biol. 2008, 6, e254. [Google Scholar] [CrossRef]
- Bitar, M.S.; Al-Bustan, M.; Nehme, C.L.; Pilcher, C.W.T. Antinociceptive action of intrathecally administered IGF-I and the expression of its receptor in rat spinal cord. Brain Res. 1996, 737, 292–294. [Google Scholar] [CrossRef]
- Miura, M.; Sasaki, M.; Mizukoshi, K.; Shibasaki, M.; Izumi, Y.; Shimosato, G.; Amaya, F. Peripheral sensitization caused by insulin-like growth factor 1 contributes to pain hypersensitivity after tissue injury. Pain 2011, 152, 888–895. [Google Scholar] [CrossRef]
- Sugawara, S.; Shinoda, M.; Hayashi, Y.; Saito, H.; Asano, S.; Kubo, A.; Shibuta, I.; Furukawa, A.; Toyofuku, A.; Iwata, K. Increase in IGF-1 Expression in the Injured Infraorbital Nerve and Possible Implications for Orofacial Neuropathic Pain. Int. J. Mol. Sci. 2019, 20, 6360. [Google Scholar] [CrossRef]
- Guyatt, G.; Gutterman, D.; Baumann, M.H.; Addrizzo-Harris, D.; Hylek, E.M.; Phillips, B.; Raskob, G.; Lewis, S.Z.; Schünemann, H. Grading Strength of Recommendations and Quality of Evidence in Clinical Guidelines: Report from an American College of Chest Physicians Task Force. CHEST 2006, 129, 174–181. [Google Scholar] [CrossRef]
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.H.; Yarnitsky, D.; Freeman, R.; Truini, A.; Attal, N.; Finnerup, N.; et al. Neuropathic pain. Nat. Rev. Dis. Prim. 2017, 3, 17002. [Google Scholar] [CrossRef]
- Gilron, I.; Baron, R.; Jensen, T. Neuropathic pain: Principles of diagnosis and treatment. In Mayo Clinic Proceedings; Elsevier Ltd.: Amsterdam, The Netherlands, 2015; Volume 90, pp. 532–545. [Google Scholar] [CrossRef]
- Chen, X.; Le, Y.; He, W.-Y.; He, J.; Wang, Y.-H.; Zhang, L.; Xiong, Q.-M.; Zheng, X.-Q.; Liu, K.-X.; Wang, H.-B. Abnormal Insulin-like Growth Factor 1 Signaling Regulates Neuropathic Pain by Mediating the Mechanistic Target of Rapamycin-Related Autophagy and Neuroinflammation in Mice. ACS Chem. Neurosci. 2021, 12, 2917–2928. [Google Scholar] [CrossRef] [PubMed]
- Takemura, H.; Kushimoto, K.; Horii, Y.; Fujita, D.; Matsuda, M.; Sawa, T.; Amaya, F. IGF1-driven induction of GPCR kinase 2 in the primary afferent neuron promotes resolution of acute hyperalgesia. Brain Res. Bull. 2021, 177, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Contreras, P.C.; Vaught, J.L.; Gruner, J.A.; Brosnan, C.; Steffler, C.; Arezzo, J.C.; Lewis, M.E.; Kessler, J.A.; Apfel, S.C. Insulin-like growth factor-I prevents development of a vincristine neuropathy in mice. Brain Res. 1997, 774, 20–26. [Google Scholar] [CrossRef]
- Morgado, C.; Silva, L.; Pereira-Terra, P.; Tavares, I. Changes in serotoninergic and noradrenergic descending pain pathways during painful diabetic neuropathy: The preventive action of IGF1. Neurobiol. Dis. 2011, 43, 275–284. [Google Scholar] [CrossRef]
- Bitar, M.S.; Pilcher, C.W.T. Attenuation of IGF-1 Antinociceptive Action and a Reduction in Spinal Cord Gene Expression of Its Receptor in Experimental Diabetes. Pain 1998, 75, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Cai, J.; Han, Y.; Xiao, X.; Meng, X.; Su, L.; Liu, F.; Xing, G.; Wan, Y. Enhanced function of TRPV1 via up-regulation by insulin-like growth factor-1 in a rat model of bone cancer pain. Eur. J. Pain 2014, 18, 774–784. [Google Scholar] [CrossRef]
- Forster, R.; Sarginson, A.; Velichkova, A.; Hogg, C.; Dorning, A.; Horne, A.W.; Saunders, P.T.K.; Greaves, E. Macrophage-derived insulin-like growth factor-1 is a key neurotrophic and nerve-sensitizing factor in pain associated with endometriosis. FASEB J. 2019, 33, 11210–11222. [Google Scholar] [CrossRef]
- Olesen, J.L.; Hansen, M.; Turtumoygard, I.F.; Hoffner, R.; Schjerling, P.; Christensen, J.; Mendias, C.L.; Magnusson, P.S.; Kjaer, M. No Treatment Benefits of Local Administration of Insulin-like Growth Factor-1 in Addition to Heavy Slow Resistance Training in Tendinopathic Human Patellar Tendons: A Randomized, Double-Blind, Placebo-Controlled Trial With 1-Year Follow-up. Am. J. Sport. Med. 2021, 49, 2361–2370. [Google Scholar] [CrossRef] [PubMed]
- Windebank, A.J.; Sorenson, E.J.; Civil, R.; O’Brien, P.C. Role of insulin-like growth factor-I in the treatment of painful small fiber predominant neuropathy. J. Peripher. Nerv. Syst. 2004, 9, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.J.; Kahaly, G.J.; Ezra, D.G.; Fleming, J.C.; Dailey, R.A.; Tang, R.A.; Harris, G.J.; Antonelli, A.; Salvi, M.; Goldberg, R.A.; et al. Teprotumumab for Thyroid-Associated Ophthalmopathy. N. Engl. J. Med. 2017, 376, 1748–1761. [Google Scholar] [CrossRef]
- Gao, W.Q.; Shinsky, N.; Ingle, G.; Beck, K.; Elias, K.A.; Powell-Braxton, L. IGF-I deficient mice show reduced peripheral nerve conduction velocities and decreased axonal diameters and respond to exogenous IGF-I treatment. J. Neurobiol. 1999, 39, 142–152. [Google Scholar] [CrossRef]
- Zochodne, D.W.; Cheng, C. Neurotrophins and other growth factors in the regenerative milieu of proximal nerve stump tips. J. Anat. 2000, 196 Pt 2, 279–283. [Google Scholar] [CrossRef]
- Russell, J.W.; Windebank, A.J.; Schenone, A.; Feldman, E.L. Insulin-like growth factor-I prevents apoptosis in neurons after nerve growth factor withdrawal. J. Neurobiol. 1998, 36, 455–467. [Google Scholar] [CrossRef]
- Lai, E.C.; Felice, K.J.; Festoff, B.W.; Gawel, M.J.; Gelinas, D.F.; Kratz, R.; Murphy, M.F.; Natter, H.M.; Norris, F.H.; Rudnicki, S.A.; et al. Effect of recombinant human insulin-like growth factor-I on progression of ALS. A placebo-controlled study. The North America ALS/IGF-I Study Group. Neurology 1997, 49, 1621–1630. [Google Scholar] [CrossRef] [PubMed]
- Borasio, G.D.; Robberecht, W.; Leigh, P.N.; Emile, J.; Guiloff, R.J.; Jerusalem, F.; Silani, V.; Vos, P.E.; Wokke, J.; Dobbins, T.; et al. A placebo-controlled trial of insulin-like growth factor-I in amyotrophic lateral sclerosis. European ALS/IGF-I Study Group. Neurology 1998, 51, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Pappo, A.S.; Patel, S.R.; Crowley, J.; Reinke, D.K.; Kuenkele, K.-P.; Chawla, S.P.; Toner, G.; Maki, R.G.; Meyers, P.; Chugh, R.; et al. R1507, a monoclonal antibody to the insulin-like growth factor 1 receptor, in patients with recurrent or refractory Ewing sarcoma family of tumors: Results of a phase II Sarcoma Alliance for Research through Collaboration study. J. Clin. Oncol. 2011, 29, 4541–4547. [Google Scholar] [CrossRef] [PubMed]
- Ramalingam, S.S.; Spigel, D.R.; Chen, D.; Steins, M.B.; Engelman, J.A.; Schneider, C.-P.; Novello, S.; Eberhardt, W.E.; Crino, L.; Habben, K.; et al. Randomized phase II study of erlotinib in combination with placebo or R1507, a monoclonal antibody to insulin-like growth factor-1 receptor, for advanced-stage non-small-cell lung cancer. J. Clin. Oncol. 2011, 29, 4574–4580. [Google Scholar] [CrossRef]
- Ma, H.; Zhang, T.; Shen, H.; Cao, H.; Du, J. The adverse events profile of anti-IGF-1R monoclonal antibodies in cancer therapy. Br. J. Clin. Pharmacol. 2014, 77, 917–928. [Google Scholar] [CrossRef]
- Werner, H.; Sarfstein, R.; Bruchim, I. Investigational IGF1R inhibitors in early stage clinical trials for cancer therapy. Expert Opin. Investig. Drugs 2019, 28, 1101–1112. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, S.; Cheng, J. Insulin-like Growth Factor-1 (IGF-1) Related Drugs in Pain Management. Pharmaceuticals 2023, 16, 760. https://doi.org/10.3390/ph16050760
Jin S, Cheng J. Insulin-like Growth Factor-1 (IGF-1) Related Drugs in Pain Management. Pharmaceuticals. 2023; 16(5):760. https://doi.org/10.3390/ph16050760
Chicago/Turabian StyleJin, Seokhyun, and Jianguo Cheng. 2023. "Insulin-like Growth Factor-1 (IGF-1) Related Drugs in Pain Management" Pharmaceuticals 16, no. 5: 760. https://doi.org/10.3390/ph16050760