
RadioLigand Therapy with [177Lu]Lu-PSMA-617 for Salivary Gland Cancers: Literature Review and First Compassionate Use in France
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Use of [177Lu]Lu-PSMA-617 in France
2.1. [177Lu]Lu-PSMA-617 Used in Castration-Resistant Prostate Cancer
2.2. [177Lu]Lu-PSMA-617 Therapy Used in Salivary Gland Cancer
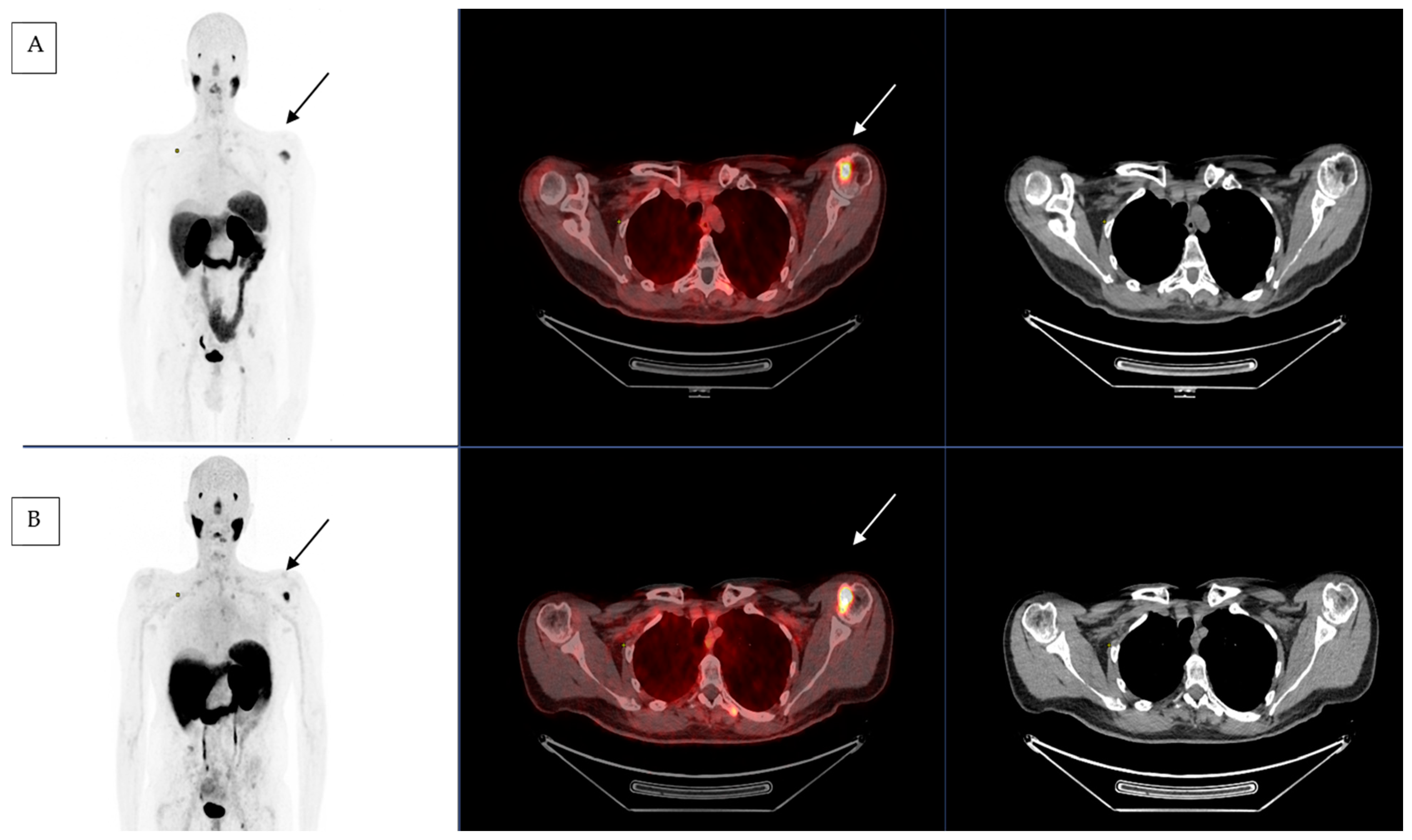
2.3. First Compassionate Use of [177Lu]Lu-PSMA-617 in Salivary Gland Cancer in France
3. Discussion
4. Conclusions
5. Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Skálová, A.; Hyrcza, M.D.; Leivo, I. Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Salivary Glands. Head Neck Pathol. 2022, 16, 40–53. [Google Scholar] [CrossRef]
- Nishida, H.; Kondo, Y.; Kusaba, T.; Kadowaki, H.; Daa, T. Immunohistochemical Reactivity of Prostate-Specific Membrane Antigen in Salivary Gland Tumors. Head Neck Pathol. 2022, 16, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Van Boxtel, W.; Uijen, M.J.M.; Verhaegh, G.W.; Willems, S.M.; Jonker, M.A.; PALGA Group; Schalken, J.A.; van Engen-van Grunsven, I.C.H.; van Herpen, C.M.L. Prognostic value of PSMA, c-MET and E-cadherin in salivary duct carcinoma. Oral Oncol. 2020, 110, 105018. [Google Scholar] [CrossRef] [PubMed]
- Aegerter, D.P.; Cosmidis, D.A. Participants Bureau REFCOR. Available online: http://refcor.org/files/116/recommandations/refcor_glandes_salivaires.pdf (accessed on 19 September 2022).
- Airoldi, M.; Pedani, F.; Succo, G.; Gabriele, A.M.; Ragona, R.; Marchionatti, S.; Bumma, C. Phase II randomized trial comparing vinorelbine versus vinorelbine plus cisplatin in patients with recurrent salivary gland malignancies. Cancer 2001, 91, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, M.J.; Johns, M.E.; Cantrell, R.W. Chemotherapy for salivary gland cancer. Otolaryngol. Head Neck Surg. 1986, 95, 165–170. [Google Scholar] [CrossRef]
- Tsukuda, M.; Kokatsu, T.; Ito, K.; Mochimatsu, I.; Kubota, A.; Sawaki, S. Chemotherapy for recurrent adeno- and adenoidcystic carcinomas in the head and neck. J. Cancer Res. Clin. Oncol. 1993, 119, 756–758. [Google Scholar] [CrossRef]
- Ruzich, J.C.; Ciesla, M.C.; Clark, J.I. Response to paclitaxel and carboplatin in metastatic salivary gland cancer: A case report. Head Neck 2002, 24, 406–410. [Google Scholar] [CrossRef]
- Javaheripour, A.; Saatloo, M.V.; Vahed, N.; Gavgani, L.F.; Kouhsoltani, M. Evaluation of HER2/neu expression in different types of salivary gland tumors: A systematic review and meta-analysis. J. Med. Life 2022, 15, 595–600. [Google Scholar] [CrossRef]
- Trigo, J.; García-Cosío, M.; García-Castaño, A.; Gomà, M.; Mesia-Nin, R.; Ruiz-Bravo, E.; Soria-Rivas, A.; Castillo, P.; Braña-García, I.; Alberola-Ferranti, M. Recommendations for the use of biomarkers for head and neck cancer, including salivary gland tumours: A consensus of the Spanish Society of Medical Oncology and the Spanish Society of Pathology. Clin. Transl. Oncol. 2022, 24, 1890–1902. [Google Scholar] [CrossRef]
- Qin, C.; Lu, Y.; Zhang, H.; Zhang, Z.; Xu, W.; Wen, S.; Gao, W.; Wu, Y. Biological roles and clinical significance of estrogen and androgen receptors in head and neck cancers. J. Cancer 2022, 13, 2189–2199. [Google Scholar] [CrossRef]
- Even, C.; Baste, N.; Classe, M. New approaches in salivary gland carcinoma. Curr. Opin. Oncol. 2019, 31, 169–174. [Google Scholar] [CrossRef]
- van Boxtel, W.; Lütje, S.; van Engen-van Grunsven, I.C.H.; Verhaegh, G.W.; Schalken, J.A.; Jonker, M.A.; Nagarajah, J.; Gotthardt, M.; van Herpen, C.M.L. 68Ga-PSMA-HBED-CC PET/CT imaging for adenoid cystic carcinoma and salivary duct carcinoma: A phase 2 imaging study. Theranostics 2020, 10, 2273–2283. [Google Scholar] [CrossRef] [PubMed]
- Uijen, M.J.M.; Derks, Y.H.W.; Merkx, R.I.J.; Schilham, M.G.M.; Roosen, J.; Privé, B.M.; van Lith, S.a.M.; van Herpen, C.M.L.; Gotthardt, M.; Heskamp, S.; et al. PSMA radioligand therapy for solid tumors other than prostate cancer: Background, opportunities, challenges, and first clinical reports. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4350–4368. [Google Scholar] [CrossRef]
- Lütje, S.; Sauerwein, W.; Lauenstein, T.; Bockisch, A.; Poeppel, T.D. In Vivo Visualization of Prostate-Specific Membrane Antigen in Adenoid Cystic Carcinoma of the Salivary Gland. Clin. Nucl. Med. 2016, 41, 476–477. [Google Scholar] [CrossRef] [PubMed]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, S.; Grewal, R.K.; Friedman, K.P.; Schöder, H.; Pandit-Taskar, N. Assessment of salivary gland function after 177Lu-PSMA radioligand therapy: Current concepts in imaging and management. Transl. Oncol. 2022, 21, 101445. [Google Scholar] [CrossRef] [PubMed]
- Langbein, T.; Kulkarni, H.R.; Schuchardt, C.; Mueller, D.; Volk, G.F.; Baum, R.P. Salivary Gland Toxicity of PSMA-Targeted Radioligand Therapy with 177Lu-PSMA and Combined 225Ac- and 177Lu-Labeled PSMA Ligands (TANDEM-PRLT) in Advanced Prostate Cancer: A Single-Center Systematic Investigation. Diagnostics 2022, 12, 1926. [Google Scholar] [CrossRef]
- Kuo, P.H.; Benson, T.; Messmann, R.; Groaning, M. Why We Did What We Did: PSMA PET/CT Selection Criteria for the VISION Trial. J. Nucl. Med. 2022, 63, 816–818. [Google Scholar] [CrossRef] [PubMed]
- Isgoren, S.; Hekimsoy, T.; Koroglu, E.; Demir, H. PET/CT With 68Ga-PSMA and 18F-FDG in Metastatic Adenoid Cystic Carcinoma: Report of 2 Cases. Clin. Nucl. Med. 2022, 47, e423–e424. [Google Scholar] [CrossRef]
- Tan, B.F.; Tan, W.C.C.; Wang, F.Q.; Lechner, M.; Schartinger, V.H.; Tan, D.S.W.; Loke, K.S.H.; Nei, W.L. PSMA PET Imaging and Therapy in Adenoid Cystic Carcinoma and Other Salivary Gland Cancers: A Systematic Review. Cancers 2022, 14, 3585. [Google Scholar] [CrossRef]
- Has Simsek, D.; Kuyumcu, S.; Agaoglu, F.Y.; Unal, S.N. Radionuclide Therapy With 177Lu-PSMA in a Case of Metastatic Adenoid Cystic Carcinoma of the Parotid. Clin. Nucl. Med. 2019, 44, 764–766. [Google Scholar] [CrossRef] [PubMed]
- Klein Nulent, T.J.W.; van Es, R.J.J.; Willems, S.M.; Braat, A.J.A.T.; Devriese, L.A.; de Bree, R.; de Keizer, B. First experiences with 177Lu-PSMA-617 therapy for recurrent or metastatic salivary gland cancer. EJNMMI Res. 2021, 11, 126. [Google Scholar] [CrossRef] [PubMed]
- Civan, C.; Kasper, S.; Berliner, C.; Fragoso-Costa, P.; Grünwald, V.; Pogorzelski, M.; Schaarschmidt, B.M.; Lang, S.; Kersting, D.; Nader, M.; et al. PSMA-Directed Imaging and Therapy of Salivary Gland Tumors: A Single-Center Retrospective Study. J. Nucl. Med. 2023, 64, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Wahl, R.L.; Jacene, H.; Kasamon, Y.; Lodge, M.A. From RECIST to PERCIST: Evolving Considerations for PET Response Criteria in Solid Tumors. J. Nucl. Med. 2009, 50, 122S–150S. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Common Terminology Criteria for Adverse Events (CTCAE). Protocol Development. CTEP. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm (accessed on 19 September 2022).
- Eiber, M.; Herrmann, K.; Calais, J.; Hadaschik, B.; Giesel, F.L.; Hartenbach, M.; Hope, T.; Reiter, R.; Maurer, T.; Weber, W.A.; et al. Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE): Proposed miTNM Classification for the Interpretation of PSMA-Ligand PET/CT. J. Nucl. Med. 2018, 59, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Stabin, M.G.; Sparks, R.B.; Crowe, E. OLINDA/EXM: The second-generation personal computer software for internal dose assessment in nuclear medicine. J. Nucl. Med. 2005, 46, 1023–1027. [Google Scholar] [CrossRef] [PubMed]
- Poty, S.; Francesconi, L.C.; McDevitt, M.R.; Morris, M.J.; Lewis, J.S. α-Emitters for Radiotherapy: From Basic Radiochemistry to Clinical Studies-Part 1. J. Nucl. Med. 2018, 59, 878–884. [Google Scholar] [CrossRef]
- Stangl-Kremser, J.; Ricaurte-Fajardo, A.; Subramanian, K.; Osborne, J.R.; Sun, M.; Tagawa, S.; Bander, N.H. Response to RL-225Ac in prostate cancer: Effect of prior treatment with RL-177Lu: A systematic review of the literature. Prostate 2023, 83, 1–11. [Google Scholar] [CrossRef]
- Lunger, L.; Tauber, R.; Feuerecker, B.; Gschwend, J.E.; Eiber, M.; Heck, M.M. Narrative review: Prostate-specific membrane antigen-radioligand therapy in metastatic castration-resistant prostate cancer. Transl. Urol. 2021, 10, 3963–3971. [Google Scholar] [CrossRef]


{kind=link}
| Malignant Epithelial Tumors | Androgen Receptor Expression | HER 2 Expression (%) | PSMA Expression (%) |
|---|---|---|---|
| Acinic cell carcinoma | 16.2 | 94 | |
| Mucoepidermoid carcinoma | 12.9 | ||
| Adenoid cystic carcinoma | 17.2 | ||
| Polymorphous low-grade adenocarcinoma | 4.0 | ||
| Epithelial–myoepithelial carcinoma | 5.2 | ||
| Clear cell carcinoma, not otherwise specified | |||
| Basal cell adenocarcinoma | 4.7 | ||
| Sebaceous carcinoma | |||
| Sebaceous lymphadenocarcinoma | |||
| Cystadenocarcinoma | 3.3 | ||
| Low-grade cribriform cystadenocarcinoma | |||
| Mucinous adenocarcinoma | |||
| Oncocytic carcinoma | 4.6 | ||
| Salivary duct carcinoma | Often | 44.9 | 62.5 |
| Adenocarcinoma, not otherwise specified | Often | 22.3 | |
| Myoepithelial carcinoma | 5.1 | ||
| Carcinoma ex pleomorphic adenoma | 33.7 | ||
| Carcinosarcoma | |||
| Metastasizing pleomorphic adenoma | |||
| Squamous cell carcinoma | 21.4 | ||
| Small cell carcinoma | |||
| Large cell carcinoma | |||
| Lymphoepithelial carcinoma | |||
| Sialoblastoma |
| Study Author (Year of Publication) | Type of Study | No. of Patients | Tumor Type | PSMA Expression (% by IHC) | [68Ga]Ga-PSMA-11 PET CT | SUV Max | [177Lu]Lu-PSMA-617 | No of Cycles | Response to Treatment | Toxicities | Dosimetry |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Has Simsek et al. 2019 [22] | Case report | 1 | ACC | No data | Yes (1) | No data | yes | 1 | Bone pain decrease | None | No data |
| Klein Nulent et al. 2021 [23] | Retrospective | 6 | ACC (4) Adenoma NOS (1) Acinic cell carcinoma (1) | 5 to 95 | Yes (6) | 3.5 to 10.2 | Yes | 1 to 4 | PR (1) SD (1) PD (3) NA (1) | Grade 1–2 | No data |
| Civan et al. 2023 [24] | Retrospective | 5 (from 28 for PET imaging) | ACC (4) Acinic cell carcinoma (1) | No data | Yes (28) | 10.7 (average) | Yes (5 from 28) | 1 to 6 | SD (2) PD (1) NA (2) | SD (2) PD (1) NA (2) None | Yes (olinda/MIRD) |
| Score | Reported PSMA Expression | Uptake |
|---|---|---|
| 0 | No | Below blood pool |
| 1 | Low | Equal to or above blood pool and lower than liver * |
| 2 | Intermediate | Equal to or above liver and lower than parotid gland |
| 3 | High | Equal to or above parotid gland |
| Alpha Particle Radiation | Beta Particle Radiation | |
|---|---|---|
| Energy | 5–9 meV | 50–2300 keV |
| Range | 40–100 um | 0.05–12 mm |
| Linear energy transfer | 80 keV/mm | 0.2 keV/mm |
| Mass | 4 amu | 1/2000 amu |
| Charge | 3.1 × 10−19 C | 1.6 × 10−19 C |
| Penetrate power | 101 mm Al, 3–8 cm air | 5 mm Al, 1 mm lead |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terroir, M.; Lamesa, C.; Krim, M.; Vija, L.; Texier, J.-S.; Cassou-Mounat, T.; Delord, J.-P.; Vallot, D.; Courbon, F. RadioLigand Therapy with [177Lu]Lu-PSMA-617 for Salivary Gland Cancers: Literature Review and First Compassionate Use in France. Pharmaceuticals 2023, 16, 754. https://doi.org/10.3390/ph16050754
Terroir M, Lamesa C, Krim M, Vija L, Texier J-S, Cassou-Mounat T, Delord J-P, Vallot D, Courbon F. RadioLigand Therapy with [177Lu]Lu-PSMA-617 for Salivary Gland Cancers: Literature Review and First Compassionate Use in France. Pharmaceuticals. 2023; 16(5):754. https://doi.org/10.3390/ph16050754
Chicago/Turabian StyleTerroir, Marie, Chloé Lamesa, Mehdi Krim, Lavinia Vija, Jean-Sébastien Texier, Thibaut Cassou-Mounat, Jean-Pierre Delord, Delphine Vallot, and Frédéric Courbon. 2023. "RadioLigand Therapy with [177Lu]Lu-PSMA-617 for Salivary Gland Cancers: Literature Review and First Compassionate Use in France" Pharmaceuticals 16, no. 5: 754. https://doi.org/10.3390/ph16050754