
Peripheral Neuropathy in Systemic Autoimmune Rheumatic Diseases—Diagnosis and Treatment
Abstract
:1. Introduction
2. Methodology
3. Review
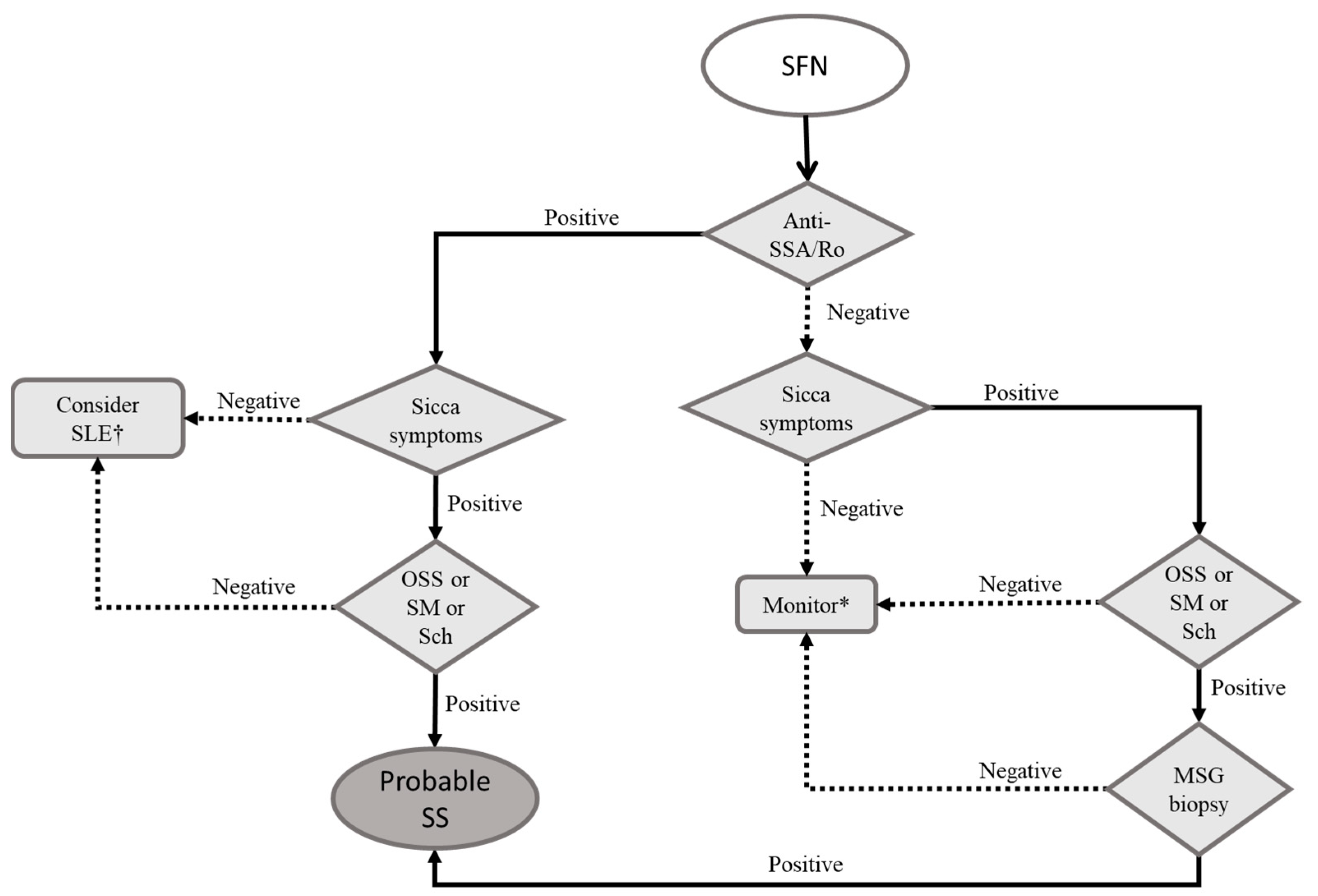
3.1. Small Fiber Neuropathy
3.2. Treatment of SFN
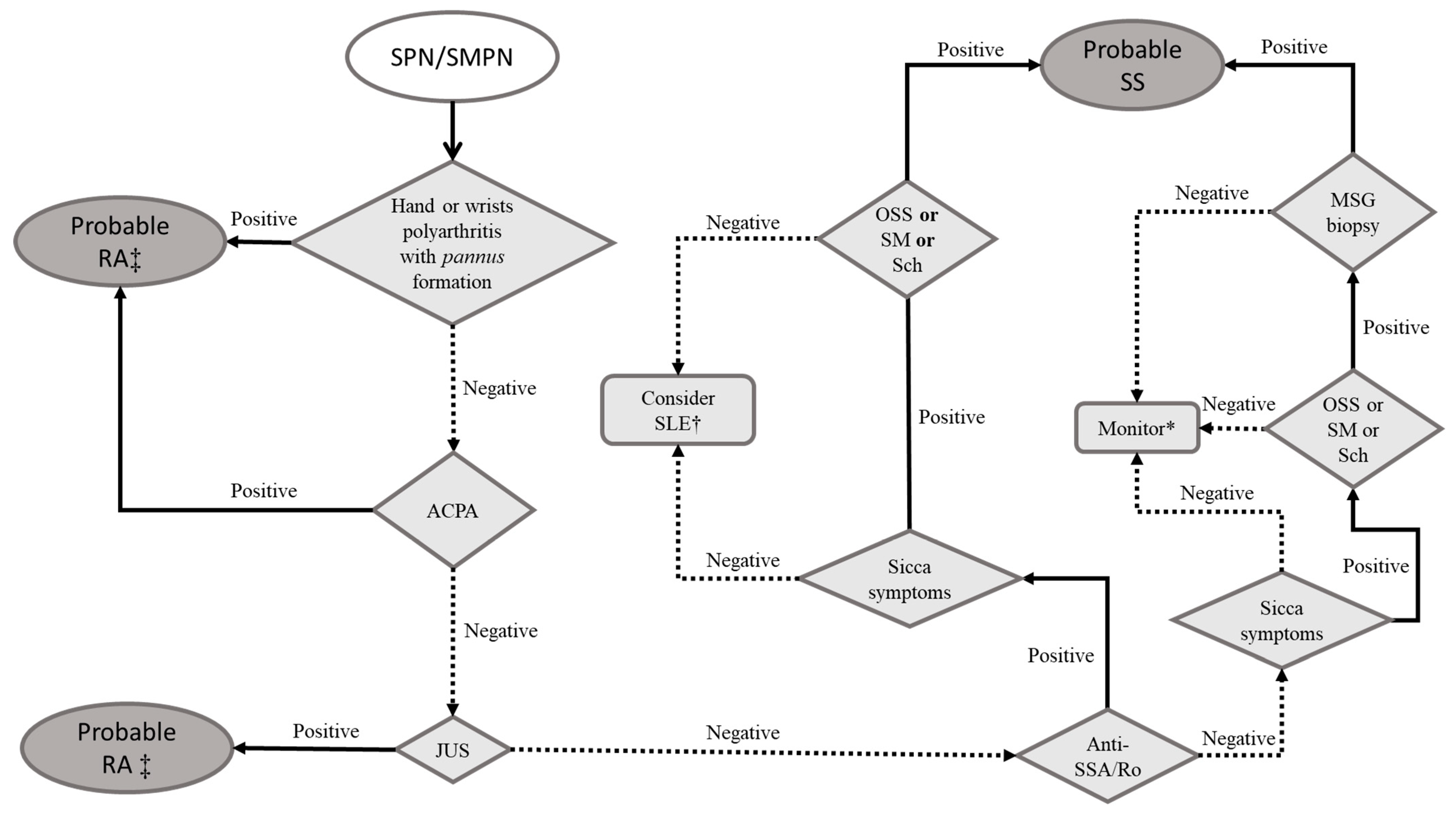
3.3. Axonal Sensory Polyneuropathy (SPN) and Sensorimotor Polyneuropathy (SMPN)
3.4. Treatment of SNP/SMNP
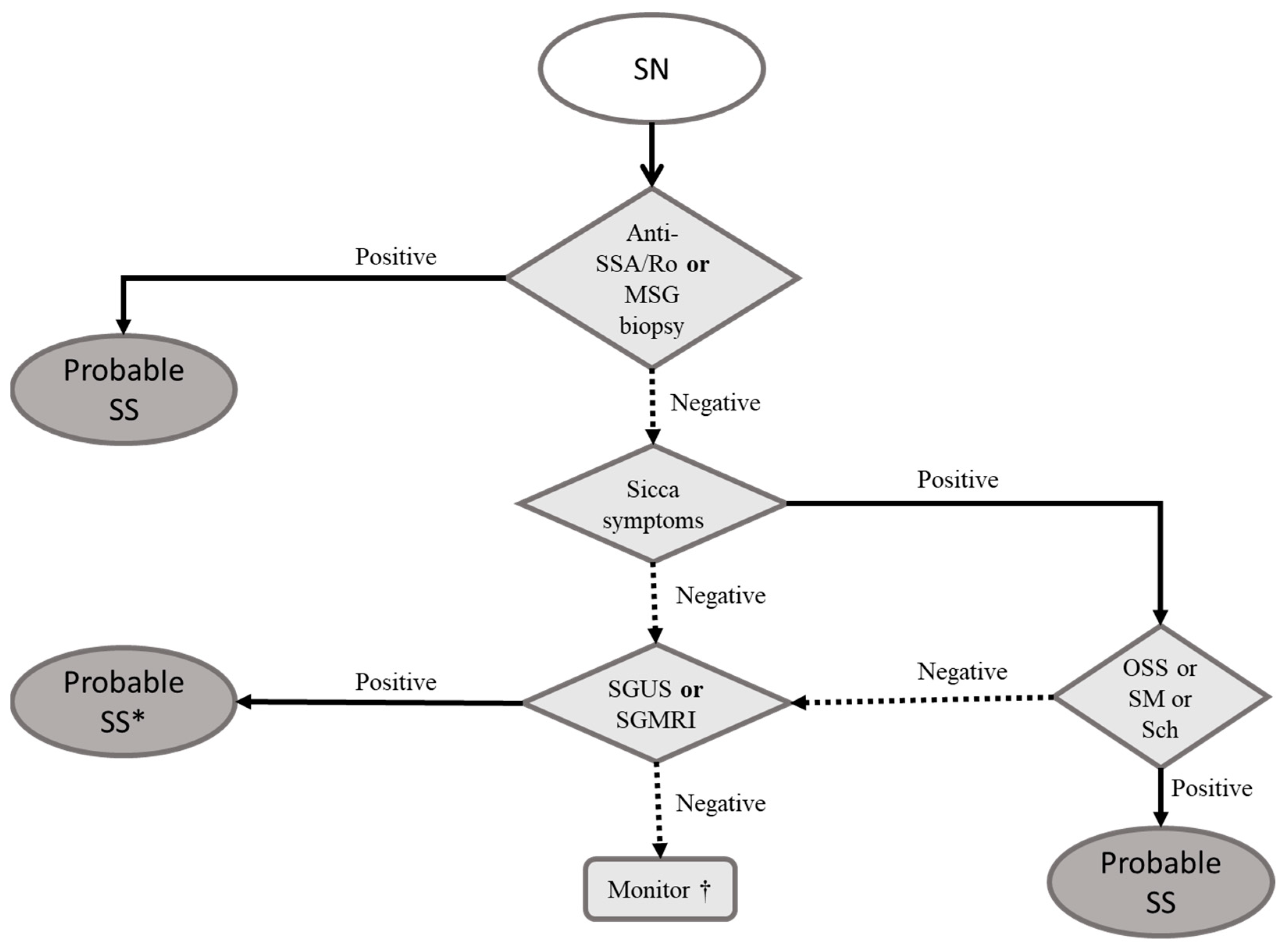
3.5. Sensory Neuronopathy
3.6. Treatment of Sensory Neuronopathy
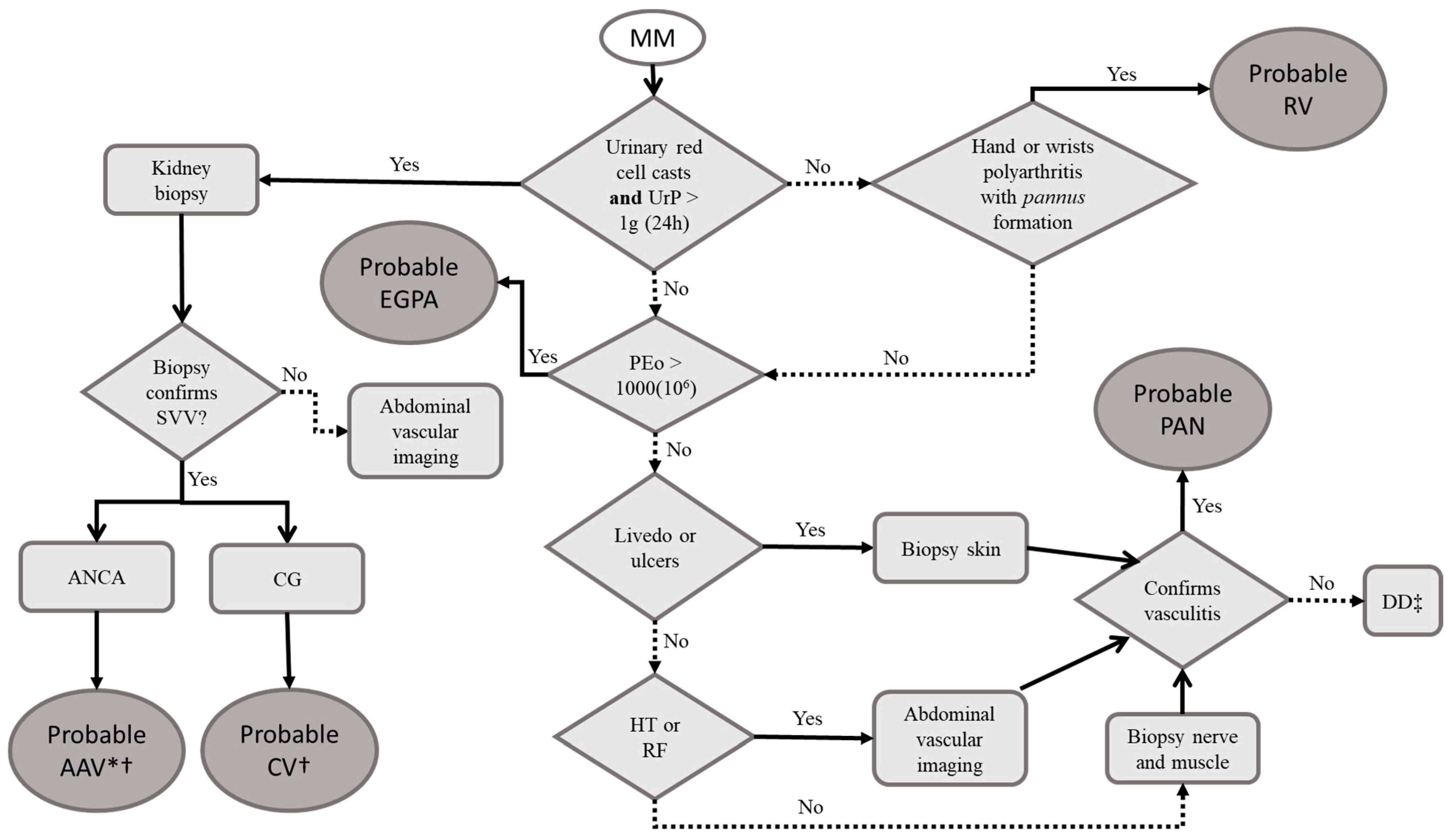
3.7. Multiple Mononeuritis (MM)
3.8. Treatment of MM
3.9. Isolated Mononeuropathies
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gwathmey, K.G.; Satkowiak, K. Peripheral nervous system manifestations of rheumatological diseases. J. Neurol. Sci. 2021, 424, 117421. [Google Scholar] [CrossRef] [PubMed]
- Margaretten, M. Neurologic manifestations of primary Sjögren syndrome. Rheum. Dis. Clin. N. Am. 2017, 43, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Florica, B.; Aghdassi, E.; Su, J.; Gladman, D.D.; Urowitz, M.B.; Fortin, P.R. Peripheral neuropathy in patients with systemic lupus erythematosus. Semin. Arthritis Rheum. 2011, 41, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Oomatia, A.; Fang, H.; Petri, M.; Birnbaum, J. Peripheral neuropathies in systemic lupus erythematosus: Clinical features, disease associations, and immunologic characteristics evaluated over a twenty-five-year study period. Arthritis Rheumatol. 2014, 66, 1000–1009. [Google Scholar] [CrossRef] [PubMed]
- Gwathmey, K.G.; Burns, T.M.; Collins, M.P.; Dyck, J.B. Vasculitic neuropathies. Lancet Neurol. 2014, 13, 67–82. [Google Scholar] [CrossRef]
- Ramos-Casals, M.; Brito-Zerón, P.; Bombardieri, S.; Bootsma, H.; De Vita, S.; Dörner, T.; Fisher, B.A.; Gottenberg, J.E.; Hernandez-Molina, G.; Kocher, A.; et al. EULAR recommendations for the management of Sjögren’s syndrome with topical and systemic therapies. Ann. Rheum. Dis. 2020, 79, 3–18. [Google Scholar] [CrossRef] [Green Version]
- Sène, D.; Jallouli, M.; Lefaucheur, J.P.; Saadoun, D.; Costedoat-Chalumeau, N.; Maisonobe, T.; Diemert, M.C.; Musset, L.; Haroche, J.; Piette, J.C.; et al. Peripheral neuropathies associated with primary Sjögren syndrome: Immunologic profiles of nonataxic sensory neuropathy and sensorimotor neuropathy. Medicine 2011, 90, 133–138. [Google Scholar] [CrossRef]
- Mori, K.; Iijima, M.; Koike, H.; Hattori, N.; Tanaka, F.; Watanabe, H.; Katsuno, M.; Fujita, A.; Aiba, I.; Ogata, A.; et al. The wide spectrum of clinical manifestations in Sjögren’s syndrome-associated neuropathy. Brain 2005, 128 Pt 11, 2518–2534. [Google Scholar] [CrossRef] [Green Version]
- Hoeijmakers, J.G.; Faber, C.G.; Lauria, G.; Merkies, I.S.; Waxman, S.G. Small-fibre neuropathies—Advances in diagnosis, pathophysiology and management. Nat. Rev. Neurol. 2012, 8, 369–379. [Google Scholar] [CrossRef]
- Themistocleous, A.; Ramirez, J.D.; Serra, J.; Bennett, D.L.H. The clinical approach to small fibre neuropathy and painful channelopathy. Pract. Neurol. 2014, 14, 368–379. [Google Scholar] [CrossRef] [Green Version]
- Oaklander, A.L.; Nolano, M. Scientific Advances in and Clinical Approaches to Small-Fiber Polyneuropathy: A Review. JAMA Neurol. 2019, 76, 1240–1251. [Google Scholar] [CrossRef]
- Uceyler, N.; Kafke, W.; Riediger, N.; He, L.; Necula, G.; Toyka, K.V.; Sommer, C. Elevated proinflammatory cytokine expression in affected skin in small fiber neuropathy. Neurology 2010, 74, 1806–1813. [Google Scholar] [CrossRef]
- Birnbaum, J.; Lalji, A.; Saed, A.; Baer, A.N. Biopsy-proven small-fiber neuropathy in primary Sjögren’s syndrome: Neuropathic pain characteristics, autoantibody findings, and histopathologic features. Arthritis Care Res. 2019, 71, 936–948. [Google Scholar] [CrossRef]
- Gorson, K.C.; Herrmann, D.N.; Thiagarajan, R.; Brannagan, T.H.; Chin, R.L.; Kinsella, L.J.; Ropper, A.H. Non-length dependent small fibre neuropathy/ganglionopathy. J. Neurol. Neurosurg. Psychiatry 2008, 79, 163–169. [Google Scholar] [CrossRef]
- Siao, P.; Cros, D.P. Quantitative sensory testing. Phys. Med. Rehabil. Clin. N. Am. 2003, 14, 261–286. [Google Scholar] [CrossRef]
- Devigili, G.; Tugnoli, V.; Penza, P.; Camozzi, F.; Lombardi, R.; Melli, G.; Broglio, L.; Granieri, E.; Lauria, G. The diagnostic criteria for small fibre neuropathy: From symptoms to neuropathology. Brain 2008, 131, 1912–1925. [Google Scholar] [CrossRef] [Green Version]
- Lauria, G.; Hsieh, S.T.; Johansson, O.; Kennedy, W.R.; Leger, J.M.; Mellgren, S.I.; Nolano, M.; Merkies, I.S.; Polydefkis, M.; Smith, A.G.; et al. European Federation of Neurological Societies/Peripheral Nerve Society Guideline on the use of skin biopsy in the diagnosis of small fiber neuropathy. Report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society. Eur. J. Neurol. 2010, 17, 903–912. [Google Scholar]
- Katsarava, Z.; Ayzenberg, I.; Sack, F.; Limmroth, V.; Diener, H.C.; Kaube, H. A novel method of eliciting pain-related potentials by transcutaneous electrical stimulation. Headache 2006, 46, 1511–1517. [Google Scholar] [CrossRef]
- Mueller, D.; Obermann, M.; Koeppen, S.; Kavuk, I.; Yoon, M.S.; Sack, F.; Diener, H.C.; Kaube, H.; Katsarava, Z. Electrically evoked nociceptive potentials for early detection of diabetic small-fiber neuropathy. Eur. J. Neurol. 2010, 17, 834–841. [Google Scholar] [CrossRef]
- Agostino, R.; Cruccu, G.; Romaniello, A.; Innocenti, P.; Inghilleri, M.; Manfredi, M. Dysfunction of small myelinated afferents in diabetic polyneuropathy, as assessed by laser evoked potentials. Clin. Neurophysiol. 2000, 111, 270–276. [Google Scholar] [CrossRef]
- Atherton, D.D.; Facer, P.; Roberts, K.M.; Misra, V.P.; Chizh, B.A.; Bountra, C.; Anand, P. Use of the novel Contact Heat Evoked Potential Stimulator (CHEPS) for the assessment of small fibre neuropathy: Correlations with skin flare responses and intra-epidermal nerve fibre counts. BMC Neurol. 2007, 7, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagerburg, V.; Bakkers, M.; Bouwhuis, A.; Hoeijmakers, J.G.; Smit, A.M.; Van Den Berg, S.J.; Hordijk-De Boer, I.; Brouwer-Van Der Lee, M.D.; Kranendonk, D.; Reulen, J.P.; et al. Contact heat evoked potentials: Normal values and use in small-fiber neuropathy. Muscle Nerve 2015, 51, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Gorson, K.C.; Ropper, A.H. Positive salivary gland biopsy, Sjögren syndrome, and neuropathy: Clinical implications. Muscle Nerve 2003, 28, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Biswas, M.; Chatterjee, A.; Ghosh, S.K.; Dasgupta, S.; Ghosh, K.; Ganguly, P.K. Prevalence, types, clinical associations, and determinants of peripheral neuropathy in rheumatoid patients. Ann. Indian Acad. Neurol. 2011, 14, 194–197. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, V.; Singh, R.; Wiclaf Chauhan, S.; Tahlan, A.; Ahuja, C.K.; Goel, D.; Pal, L. A clinical, electrophysiological, and pathological study of neuropathy in rheumatoid arthritis. Clin. Rheumatol. 2008, 27, 841–844. [Google Scholar] [CrossRef]
- Khan, S.; Zhou, L. Characterization of non-length-dependent small-fiber sensory neuropathy. Muscle Nerve 2012, 45, 86–91. [Google Scholar] [CrossRef]
- Mekinian, A.; Ravaud, P.; Hatron, P.Y.; Larroche, C.; Leone, J.; Gombert, B.; Hamidou, M.; Cantagrel, A.; Marcelli, C.; Rist, S.; et al. Efficacy of rituximab in primary Sjögren’s syndrome with peripheral nervous system involvement: Results from the AIR registry. Ann. Rheum. Dis. 2012, 71, 84–87. [Google Scholar] [CrossRef]
- Hovaguimian, A.; Gibbons, C.H. Diagnosis and treatment of pain in small-fiber neuropathy. Curr. Pain Headache Rep. 2011, 15, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Ho, T.W.; Backonja, M.; Ma, J.; Leibensperger, H.; Froman, S.; Polydefkis, M. Efficient assessment of neuropathic pain drugs in patients with small fiber sensory neuropathies. Pain 2009, 141, 19–24. [Google Scholar] [CrossRef]
- Morozumi, S.; Kawagashira, Y.; Iijima, M.; Koike, H.; Hattori, N.; Katsuno, M.; Tanaka, F.; Sobue, G. Intravenous immunoglobulin treatment for painful sensory neuropathy associated with Sjögren’s syndrome. J. Neurol. Sci. 2009, 279, 57–61. [Google Scholar] [CrossRef]
- Bril, V.; Katzberg, H.D. Acquired immune axonal neuropathies. Contin. Lifelong Learn. Neurol. 2014, 20, 1261–1273. [Google Scholar] [CrossRef]
- Delalande, S.; de Seze, J.; Fauchais, A.L.; Hachulla, E.; Stojkovic, T.; Ferriby, D.; Dubucquoi, S.; Pruvo, J.P.; Vermersch, P.; Hatron, P.Y. Neurologic manifestations in primary Sjögren syndrome: A study of 82 patients. Medicine 2004, 83, 280–291. [Google Scholar] [CrossRef]
- Jamilloux, Y.; Magy, L.; Hurtevent, J.F.; Gondran, G.; de Seze, J.; Launay, D.; Ly, K.H.; Lambert, M.; Hachulla, E.; Hatron, P.Y.; et al. Immunological profiles determine neurological involvement in Sjögren’s syndrome. Eur. J. Intern. Med. 2014, 25, 177–181. [Google Scholar] [CrossRef]
- Fargetti, S.; Ugolini-Lopes, M.R.; Pasoto, S.G.; Seguro, L.P.C.; Shinjo, S.K.; Bonfa, E.; Borba, E.F. Short- and Long-Term Outcome of Systemic Lupus Erythematosus Peripheral Neuropathy: Bimodal Pattern of Onset and Treatment Response. J. Clin. Rheumatol. 2021, 27, S212–S216. [Google Scholar] [CrossRef]
- Nishi, R.; Koike, H.; Ohyama, K.; Fukami, Y.; Ikeda, S.; Kawagashira, Y.; Iijima, M.; Katsuno, M.; Sobue, G. Differential clinicopathologic features of EGPA-associated neuropathy with and without ANCA. Neurology 2020, 94, e1726–e1737. [Google Scholar] [CrossRef]
- Imboden, J.B. Involvement of the Peripheral Nervous System in Polyarteritis Nodosa and Antineutrophil Cytoplasmic Antibodies-Associated Vasculitis. Rheum. Dis. Clin. N. Am. 2017, 43, 633–639. [Google Scholar] [CrossRef]
- de Boysson, H.; Guillevin, L. Polyarteritis Nodosa Neurologic Manifestations. Neurol. Clin. 2019, 37, 345–357. [Google Scholar] [CrossRef]
- Bortoluzzi, A.; Silvagni, E.; Furini, F.; Piga, M.; Govoni, M. Peripheral nervous system involvement in systemic lupus erythematosus: A review of the evidence. Clin. Exp. Rheumatol. 2019, 37, 146–155. [Google Scholar]
- Imam, M.H.; Koriem, H.K.; Hassan, M.M.; El-Hadidi, A.S.; Ibrahim, N.A. Pattern of peripheral neuropathy in systemic lupus erythematosus: Clinical, electrophysiological, and laboratory properties and their association with disease activity. Egypt. Rheumatol. Rehabil. 2019, 46, 285–298. [Google Scholar] [CrossRef]
- Tulbă, D.; Popescu, B.O.; Manole, E.; Băicuș, C. Immune Axonal Neuropathies Associated with Systemic Autoimmune Rheumatic Diseases. Front. Pharmacol. 2021, 12, 610585. [Google Scholar] [CrossRef]
- Martinez, A.R.; Faber, I.; Nucci, A.; Appenzeller, S.; França, M.C., Jr. Autoimmune neuropathies associated to rheumatic diseases. Autoimmun. Rev. 2017, 16, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Julio, P.R.; Cortês, M.M.M.; Costallat, L.T.L.; Gaino, J.Z.; França, M.C., Jr.; Appenzeller, S. Chronic inflammatory demyelinating polyradiculoneuropathy associated with systemic lupus erythematosus. Semin. Arthritis Rheum. 2021, 51, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Constantin, A.; Năstase, D.; Tulbă, D.; Bălănescu, P.; Băicuș, C. Immunosuppressive therapy of systemic lupus erythematosus associated peripheral neuropathy: A systematic review. Lupus 2020, 29, 1509–1519. [Google Scholar] [CrossRef] [PubMed]
- DeQuattro, K.; Imboden, J.B. Neurologic Manifestations of Rheumatoid Arthritis. Rheum. Dis. Clin. N. Am. 2017, 43, 561–571. [Google Scholar] [CrossRef]
- Yates, M.; Watts, R.A.; Bajema, I.M.; Cid, M.C.; Crestani, B.; Hauser, T.; Hellmich, B.; Holle, J.U.; Laudien, M.; Little, M.A.; et al. EULAR/ERA-EDTA recommendations for the management of ANCA-associated vasculitis. Ann. Rheum. Dis. 2016, 75, 1583–1594. [Google Scholar] [CrossRef] [Green Version]
- Lauria, G.; Pareyson, D.; Grisoli, M.; Sghirlanzoni, A. Clinical and magnetic resonance imaging findings in chronic sensory ganglionopathies. Ann. Neurol. 2000, 47, 104–109. [Google Scholar] [CrossRef]
- Amato, A.A.; Ropper, A.H. Sensory Ganglionopathy. N. Engl. J. Med. 2020, 383, 1657–1662. [Google Scholar] [CrossRef]
- Martinez, A.R.; Nunes, M.B.; Nucci, A.; França, M.C., Jr. Sensory neuronopathy and autoimmune diseases. Autoimmune Dis. 2012, 2012, 873587. [Google Scholar] [CrossRef]
- Gøransson, L.G.; Herigstad, A.; Tjensvoll, A.B.; Harboe, E.; Mellgren, S.I.; Omdal, R. Peripheral neuropathy in primary Sjögren syndrome: A population-based study. Arch. Neurol. 2006, 63, 1612–1615. [Google Scholar] [CrossRef] [Green Version]
- Kawagashira, Y.; Koike, H.; Fujioka, Y.; Hashimoto, R.; Tomita, M.; Morozumi, S.; Iijima, M.; Katsuno, M.; Tanaka, F.; Sobue, G. Differential, size-dependent sensory neuron involvement in the painful and ataxic forms of primary Sjögren’s syndrome-associated neuropathy. J. Neurol. Sci. 2012, 319, 139–146. [Google Scholar] [CrossRef]
- Tholance, Y.; Moritz, C.P.; Rosier, C.; Ferraud, K.; Lassablière, F.; Reynaud-Federspiel, E.; França, M.C., Jr.; Martinez, A.R.M.; Camdessanché, J.P.; Antoine, J.C. Clinical characterisation of sensory neuropathy with anti-FGFR3 autoantibodies. J. Neurol. Neurosurg. Psychiatry 2020, 91, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Kuntzer, T.; Antoine, J.C.; Steck, A.J. Clinical features and pathophysiological basis of sensory neuronopathies (ganglionopathies). Muscle Nerve 2004, 30, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Lauria, G.; Pareyson, D.; Sghirlanzoni, A. Neurophysiological diagnosis of acquired sensory ganglionopathies. Eur. Neurol. 2003, 50, 146–152. [Google Scholar] [CrossRef]
- Lefter, S.; Monaghan, B.; McNamara, B.; Regan, M.J. Acute severe sensory ganglionopathy in systemic lupus erythematous. Neuromuscul. Disord. 2020, 30, 701–706. [Google Scholar] [CrossRef]
- Zis, P.; Hadjivassiliou, M.; Sarrigiannis, P.G.; Barker, A.S.J.E.; Rao, D.G. Rapid neurophysiological screening for sensory ganglionopathy: A novel approach. Brain Behav. 2017, 7, e00880. [Google Scholar] [CrossRef] [Green Version]
- Birnbaum, J. Peripheral nervous system manifestations of Sjögren syndrome: Clinical patterns, diagnostic paradigms, etiopathogenesis, and therapeutic strategies. Neurologist 2010, 16, 287–297. [Google Scholar] [CrossRef]
- Antoine, J.-C.; Robert-Varvat, F.; Maisonobe, T.; Créange, A.; Franques, J.; Mathis, S.; Delmont, E.; Kuntzer, T.; Lefaucheur, J.-P.; Pouget, J.; et al. Identifying a therapeutic window in acute and subacute inflammatory sensory neuronopathies. J. Neurol. Sci. 2016, 361, 187–191. [Google Scholar] [CrossRef]
- McCoy, S.S.; Baer, A.N. Neurological Complications of Sjögren’s Syndrome: Diagnosis and Management. Curr. Treat. Options Rheumatol. 2017, 3, 275–288. [Google Scholar] [CrossRef]
- Pereira, P.R.; Viala, K.; Maisonobe, T.; Haroche, J.; Mathian, A.; Hié, M.; Amoura, Z.; Cohen Aubart, F. Sjögren Sensory Neuronopathy (Sjögren Ganglionopathy): Long-Term Outcome and Treatment Response in a Series of 13 Cases. Medicine 2016, 95, e3632. [Google Scholar] [CrossRef]
- Gorson, K.C.; Natarajan, N.; Ropper, A.H.; Weinstein, R. Rituximab treatment in patients with IVIg-dependent immune polyneuropathy: A prospective pilot trial. Muscle Nerve 2007, 35, 66–69. [Google Scholar] [CrossRef]
- Zhang, Y.S.; Sun, A.P.; Chen, L.; Dong, R.F.; Zhong, Y.F.; Zhang, J. Nerve biopsy findings contribute to diagnosis of multiple mononeuropathy: 78% of findings support clinical diagnosis. Neural. Regen. Res. 2015, 10, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, R. Neuromuscular complications of connective tissue diseases. Muscle Nerve 2001, 24, 154–169. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.P.; Mendell, J.R.; Periquet, M.I.; Sahenk, Z.; Amato, A.A.; Gronseth, G.S.; Barohn, R.J.; Jackson, C.E.; Kissel, J.T. Superficial peroneal nerve/peroneus brevis muscle biopsy in vasculitic neuropathy. Neurology 2000, 55, 636–643. [Google Scholar] [CrossRef]
- Ross, M.A. Electrodiagnosis of peripheral neuropathy. Neurol. Clin. 2012, 30, 529–549. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.A.; Gorelik, M.; Langford, C.A.; Maz, M.; Abril, A.; Guyatt, G.; Archer, A.M.; Conn, D.L.; Full, K.A.; Grayson, P.C.; et al. 2021 American College of Rheumatology/Vasculitis Foundation Guideline for the Management of Polyarteritis Nodosa. Arthritis Rheumatol. 2021, 73, 1384–1393. [Google Scholar] [CrossRef]
- Jennette, J.C.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.C.; et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013, 65, 1–11. [Google Scholar] [CrossRef]
- Chung, S.A.; Langford, C.A.; Maz, M.; Abril, A.; Gorelik, M.; Guyatt, G.; Archer, A.M.; Conn, D.L.; Full, K.A.; Grayson, P.C.; et al. 2021 American College of Rheumatology/Vasculitis Foundation Guideline for the Management of Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. Arthritis Care Res. 2021, 73, 1088–1105. [Google Scholar] [CrossRef]
- Mukhtyar, C.; Guillevin, L.; Cid, M.C.; Dasgupta, B.; de Groot, K.; Gross, W.; Hauser, T.; Hellmich, B.; Jayne, D.; Kallenberg, C.G.; et al. EULAR recommendations for the management of primary small and medium vessel vasculitis. Ann. Rheum. Dis. 2009, 68, 310–317. [Google Scholar] [CrossRef] [Green Version]
- Genta, M.S.; Genta, R.M.; Gabay, C. Systemic rheumatoid vasculitis: A review. Semin. Arthritis Rheum. 2006, 36, 88–98. [Google Scholar] [CrossRef]
- Mitka, M. FDA: Increased HBV reactivation risk with ofatumumab or rituximab. JAMA 2013, 310, 1664. [Google Scholar] [CrossRef]
- Smith, J.H.; Cutrer, F.M. Numbness matters: A clinical review of trigeminal neuropathy. Cephalalgia 2011, 31, 1131–1144. [Google Scholar] [CrossRef]
- Jääskeläinen, S.K. The utility of clinical neurophysiological and quantitative sensory testing for trigeminal neuropathy. J. Orofac. Pain 2004, 18, 355–359. [Google Scholar]
- Wilder-Smith, E.P.; Seet, R.C.S.; Lim, E.C.H. Diagnosing carpal tunnel syndrome—Clinical criteria and ancillary tests. Nat. Clin. Pract. Neurol. 2006, 2, 366–374. [Google Scholar] [CrossRef]
- Bland, J.D. Carpal tunnel syndrome. Curr. Opin. Neurol. 2005, 18, 581–585. [Google Scholar] [CrossRef]
- Ahmad, M.; Tsang, K.; Mackenney, P.J.; Adedapo, A.O. Tarsal tunnel syndrome: A literature review. Foot Ankle Surg. 2012, 18, 149–152. [Google Scholar] [CrossRef]
- Fraenkel, L.; Bathon, J.M.; England, B.R.; St. Clair, E.W.; Arayssi, T.; Carandang, K.; Deane, K.D.; Genovese, M.; Huston, K.K.; Kerr, G.; et al. 2021 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Care Res. 2021, 73, 924–939. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | Induction | Maintenance |
|---|---|---|
| Small fiber neuropathy | Intravenous methylprednisolone pulse; intravenous immunoglobulin * | Evidence limited, consider gabapentin and/or tramadol for neuropathic pain |
| Axonal sensory neuropathy/sensorimotor polyneuropathy | Intravenous methylprednisolone pulse, intravenous cyclophosphamide pulses | Azathioprine, methotrexate, mycophenolate mofetil, rituximab |
| Sensory neuronopathy | Intravenous methylprednisolone pulse; intravenous immunoglobulin * | Mycophenolate mofetil |
| Multiple mononeuritis | Intravenous methylprednisolone pulse, intravenous cyclophosphamide pulses, rituximab | Azathioprine, methotrexate, mycophenolate mofetil, rituximab |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Souza, J.M.; Trevisan, T.J.; Sepresse, S.R.; Londe, A.C.; França Júnior, M.C.; Appenzeller, S. Peripheral Neuropathy in Systemic Autoimmune Rheumatic Diseases—Diagnosis and Treatment. Pharmaceuticals 2023, 16, 587. https://doi.org/10.3390/ph16040587
De Souza JM, Trevisan TJ, Sepresse SR, Londe AC, França Júnior MC, Appenzeller S. Peripheral Neuropathy in Systemic Autoimmune Rheumatic Diseases—Diagnosis and Treatment. Pharmaceuticals. 2023; 16(4):587. https://doi.org/10.3390/ph16040587
Chicago/Turabian StyleDe Souza, Jean Marcos, Thiago Junqueira Trevisan, Samara Rosa Sepresse, Ana Carolina Londe, Marcondes Cavalcante França Júnior, and Simone Appenzeller. 2023. "Peripheral Neuropathy in Systemic Autoimmune Rheumatic Diseases—Diagnosis and Treatment" Pharmaceuticals 16, no. 4: 587. https://doi.org/10.3390/ph16040587