

Effect of Ketamine on Sleep in Treatment-Resistant Depression: A Systematic Review

Abstract
:1. Introduction
2. Results
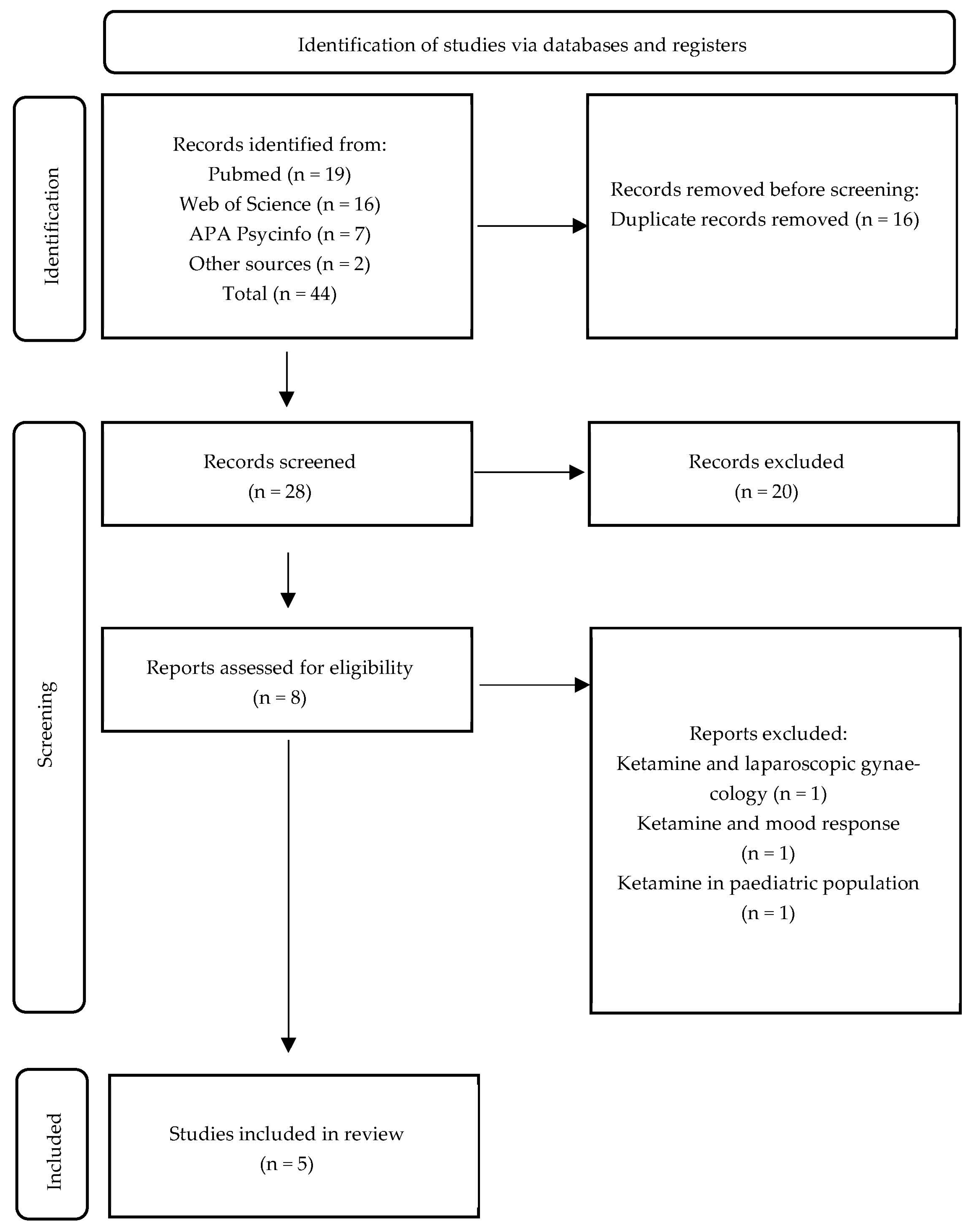
2.1. Study Selection
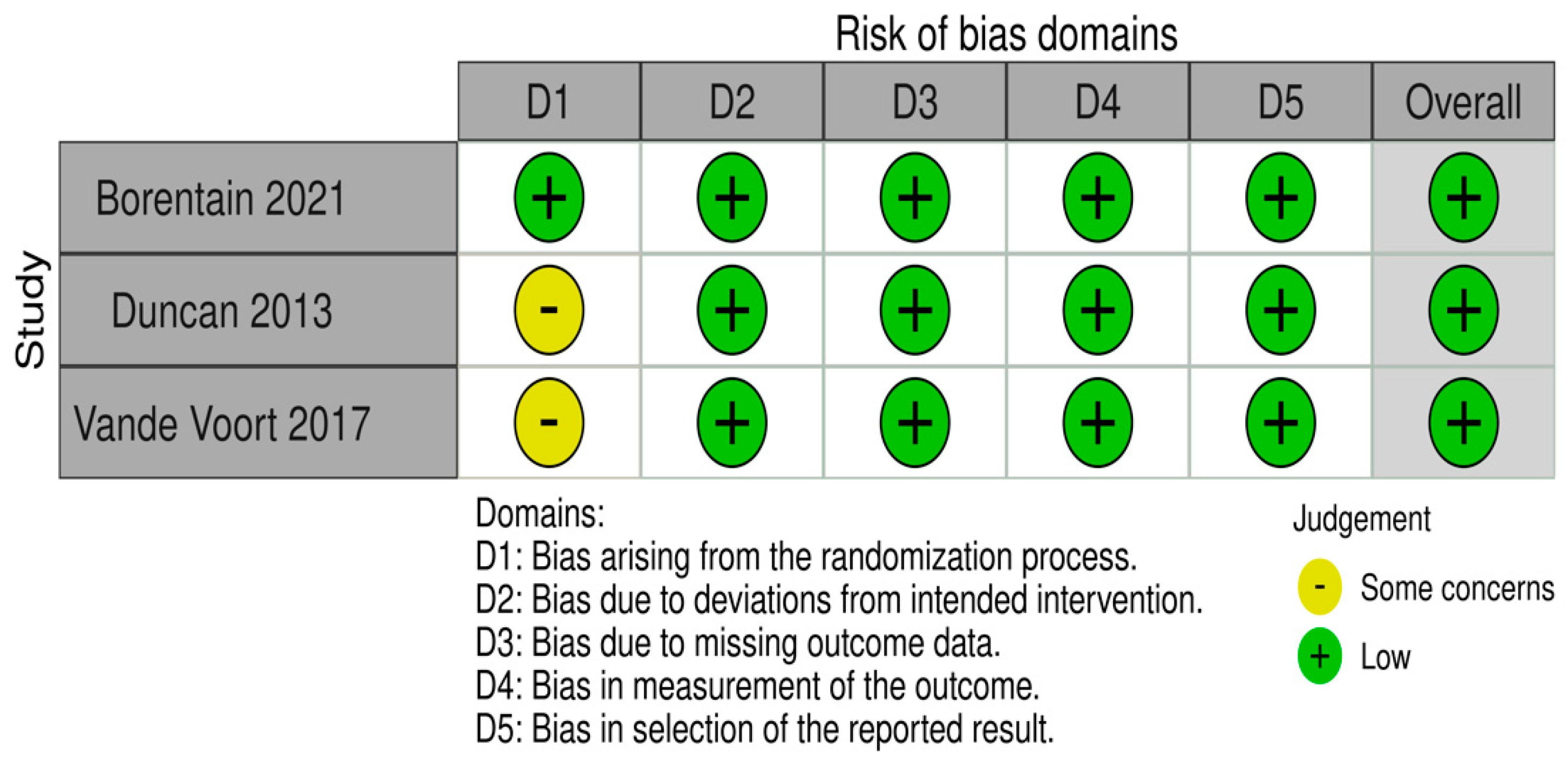
2.2. Risk of Bias in the Studies
2.3. Study Characteristics
2.3.1. Self-Reported and Clinician-Rated Sleep Patterns
2.3.2. Electroencephalographic Sleep Patterns
3. Discussion
4. Materials and Methods
4.1. Information Sources, Search Strategy and Selection Process
- Primary research articles;
- Patients had either major depressive disorder or bipolar depression according to DSM or ICD criteria (without restrictions on editions);
- Participants were exposed to ketamine or its enantiomers;
- Pre- and posttreatment sleep outcome was available;
- Patients were over 18 years of age.
4.2. Data Collection Process
4.3. Study Risk of Bias Assessment
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferrari, A.J.; Charlson, F.J.; Norman, R.E.; Patten, S.B.; Freedman, G.; Murray, C.J.L.; Vos, T.; Whiteford, H.A. Burden of Depressive Disorders by Country, Sex, Age, and Year: Findings from the Global Burden of Disease Study 2010. PLoS Med. 2013, 10, e1001547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The Global Burden of Disease: 2004 Update; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Friedrich, M.J. Depression Is the Leading Cause of Disability Around the World. JAMA 2017, 317, 1517. [Google Scholar] [CrossRef] [PubMed]
- Herrman, H.; Kieling, C.; McGorry, P.; Horton, R.; Sargent, J.; Patel, V. Reducing the Global Burden of Depression: A Lancet-World Psychiatric Association Commission. Lancet 2019, 393, e42–e43. [Google Scholar] [CrossRef] [PubMed]
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.D.; et al. Acute and Longer-Term Outcomes in Depressed Outpatients Requiring One or Several Treatment Steps: A STAR*D Report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, M.H.; Rush, A.J.; Wisniewski, S.R.; Nierenberg, A.A.; Warden, D.; Ritz, L.; Norquist, G.; Howland, R.H.; Lebowitz, B.; McGrath, P.J.; et al. Evaluation of Outcomes with Citalopram for Depression Using Measurement-Based Care in STAR*D: Implications for Clinical Practice. Am. J. Psychiatry 2006, 163, 28–40. [Google Scholar] [CrossRef]
- Papp, M.; Cubała, W.J.; Swiecicki, L.; Newman-Tancredi, A.; Willner, P. Perspectives for Therapy of Treatment-resistant Depression. Br. J. Pharmacol. 2022, 179, 4181–4200. [Google Scholar] [CrossRef]
- Caraci, F.; Calabrese, F.; Molteni, R.; Bartova, L.; Dold, M.; Leggio, G.M.; Fabbri, C.; Mendlewicz, J.; Racagni, G.; Kasper, S.; et al. International Union of Basic and Clinical Pharmacology CIV: The Neurobiology of Treatment-Resistant Depression: From Antidepressant Classifications to Novel Pharmacological Targets. Pharmacol. Rev. 2018, 70, 475–504. [Google Scholar] [CrossRef] [Green Version]
- Halaris, A.; Sohl, E.; Whitham, E.A. Treatment-Resistant Depression Revisited: A Glimmer of Hope. J. Pers. Med. 2021, 11, 155. [Google Scholar] [CrossRef]
- FDA. FDA Guidance Document: Major Depressive Disorder: Developing Drugs for Treatment; FDA: Silver Spring, MD, USA, 2018. [Google Scholar]
- EMA. EMA Personalized Medicine Council Conclusions (2015/C 421/03); EMA: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Ng, C.H.; Kato, T.; Han, C.; Wang, G.; Trivedi, M.; Ramesh, V.; Shao, D.; Gala, S.; Narayanan, S.; Tan, W.; et al. Definition of Treatment-Resistant Depression—Asia Pacific Perspectives. J. Affect Disord. 2019, 245, 626–636. [Google Scholar] [CrossRef]
- Gaynes, B.N.; Lux, L.; Gartlehner, G.; Asher, G.; Forman-Hoffman, V.; Green, J.; Boland, E.; Weber, R.P.; Randolph, C.; Bann, C.; et al. Defining Treatment-resistant Depression. Depress. Anxiety 2020, 37, 134–145. [Google Scholar] [CrossRef]
- Kautzky, A.; Dold, M.; Bartova, L.; Spies, M.; Kranz, G.S.; Souery, D.; Montgomery, S.; Mendlewicz, J.; Zohar, J.; Fabbri, C.; et al. Clinical Factors Predicting Treatment Resistant Depression: Affirmative Results from the European Multicenter Study. Acta Psychiatr. Scand. 2019, 139, 78–88. [Google Scholar] [CrossRef] [Green Version]
- Gałecki, P.; Samochowiec, J.; Mikułowska, M.; Szulc, A. Treatment-Resistant Depression in Poland-Epidemiology and Treatment. J. Clin. Med. 2022, 11, 480. [Google Scholar] [CrossRef]
- Zhang, K.; Yao, Y.; Hashimoto, K. Ketamine and Its Metabolites: Potential as Novel Treatments for Depression. Neuropharmacology 2023, 222, 109305. [Google Scholar] [CrossRef]
- Domino, E.F.; Warner, D.S. Taming the Ketamine Tiger. Anesthesiology 2010, 113, 678–684. [Google Scholar] [CrossRef] [Green Version]
- Hirota, K.; Lambert, D.G. Ketamine; History and Role in Anesthetic Pharmacology. Neuropharmacology 2022, 216, 109171. [Google Scholar] [CrossRef]
- Hashimoto, K. Rapid-acting Antidepressant Ketamine, Its Metabolites and Other Candidates: A Historical Overview and Future Perspective. Psychiatry Clin. Neurosci. 2019, 73, 613–627. [Google Scholar] [CrossRef]
- Pai, S.M.; Gries, J.-M. ACCP Public Policy Committee Off-Label Use of Ketamine: A Challenging Drug Treatment Delivery Model With an Inherently Unfavorable Risk-Benefit Profile. J. Clin. Pharmacol. 2022, 62, 10–13. [Google Scholar] [CrossRef]
- Berman, R.M.; Cappiello, A.; Anand, A.; Oren, D.A.; Heninger, G.R.; Charney, D.S.; Krystal, J.H. Antidepressant Effects of Ketamine in Depressed Patients. Biol. Psychiatry 2000, 47, 351–354. [Google Scholar] [CrossRef]
- Kim, J.; Farchione, T.; Potter, A.; Chen, Q.; Temple, R. Esketamine for Treatment-Resistant Depression—First FDA-Approved Antidepressant in a New Class. N. Engl. J. Med. 2019, 381, 1–4. [Google Scholar] [CrossRef]
- Zarate, C.A.; Singh, J.B.; Carlson, P.J.; Brutsche, N.E.; Ameli, R.; Luckenbaugh, D.A.; Charney, D.S.; Manji, H.K. A Randomized Trial of an N-Methyl-D-Aspartate Antagonist in Treatment-Resistant Major Depression. Arch. Gen. Psychiatry 2006, 63, 856–864. [Google Scholar] [CrossRef]
- Witt, K.; Potts, J.; Hubers, A.; Grunebaum, M.F.; Murrough, J.W.; Loo, C.; Cipriani, A.; Hawton, K. Ketamine for Suicidal Ideation in Adults with Psychiatric Disorders: A Systematic Review and Meta-Analysis of Treatment Trials. Aust. N. Z. J. Psychiatry 2020, 54, 29–45. [Google Scholar] [CrossRef]
- Wilkowska, A.; Wiglusz, M.S.; Gałuszko-Wegielnik, M.; Włodarczyk, A.; Cubała, W.J. Antianhedonic Effect of Repeated Ketamine Infusions in Patients With Treatment Resistant Depression. Front. Psychiatry 2021, 12, 704330. [Google Scholar] [CrossRef]
- Jawad, M.Y.; Di Vincenzo, J.D.; Badulescu, S.; Teopiz, K.M.; Tabassum, A.; Ceban, F.; Mckenzie, A.; Meshkat, S.; Rosenblat, J.D.; Ho, R.C.; et al. The Therapeutic Role of Ketamine and Esketamine in Treating Psychopathological Domains of Depression. Neuropharmacology 2023, 223, 109299. [Google Scholar] [CrossRef]
- Song, B.; Zhu, J.-C. Mechanisms of the Rapid Effects of Ketamine on Depression and Sleep Disturbances: A Narrative Review. Front. Pharmacol. 2021, 12, 782457. [Google Scholar] [CrossRef]
- Wang, C.S.; Kavalali, E.T.; Monteggia, L.M. BDNF Signaling in Context: From Synaptic Regulation to Psychiatric Disorders. Cell 2022, 185, 62–76. [Google Scholar] [CrossRef]
- Duncan, W.C.; Sarasso, S.; Ferrarelli, F.; Selter, J.; Riedner, B.A.; Hejazi, N.S.; Yuan, P.; Brutsche, N.; Manji, H.K.; Tononi, G.; et al. Concomitant BDNF and Sleep Slow Wave Changes Indicate Ketamine-Induced Plasticity in Major Depressive Disorder. Int. J. Neuropsychopharmacol. 2013, 16, 301–311. [Google Scholar] [CrossRef]
- Dunlap, J.C. Molecular Bases for Circadian Clocks. Cell 1999, 96, 271–290. [Google Scholar] [CrossRef] [Green Version]
- Bunney, B.G.; Li, J.Z.; Walsh, D.M.; Stein, R.; Vawter, M.P.; Cartagena, P.; Barchas, J.D.; Schatzberg, A.F.; Myers, R.M.; Watson, S.J.; et al. Circadian Dysregulation of Clock Genes: Clues to Rapid Treatments in Major Depressive Disorder. Mol. Psychiatry 2015, 20, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Serretti, A.; Benedetti, F.; Mandelli, L.; Lorenzi, C.; Pirovano, A.; Colombo, C.; Smeraldi, E. Genetic Dissection of Psychopathological Symptoms: Insomnia in Mood Disorders and CLOCK Gene Polymorphism. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2003, 121B, 35–38. [Google Scholar] [CrossRef]
- Katzenberg, D.; Young, T.; Finn, L.; Lin, L.; King, D.P.; Takahashi, J.S.; Mignot, E. A CLOCK Polymorphism Associated with Human Diurnal Preference. Sleep 1998, 21, 569–576. [Google Scholar] [CrossRef] [Green Version]
- Duncan, W.C.; Slonena, E.; Hejazi, N.S.; Brutsche, N.; Yu, K.C.; Park, L.; Ballard, E.D.; Zarate, C.A. Motor-Activity Markers of Circadian Timekeeping Are Related to Ketamine’s Rapid Antidepressant Properties. Biol. Psychiatry 2017, 82, 361–369. [Google Scholar] [CrossRef]
- Regier, D.A.; Kuhl, E.A.; Kupfer, D.J. The DSM-5: Classification and Criteria Changes. World Psychiatry 2013, 12, 92–98. [Google Scholar] [CrossRef] [Green Version]
- McClintock, S.M.; Husain, M.M.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Trivedi, M.H.; Cook, I.; Morris, D.; Warden, D.; Rush, A.J. Residual Symptoms in Depressed Outpatients Who Respond by 50% but Do Not Remit to Antidepressant Medication. J. Clin. Psychopharmacol. 2011, 31, 180–186. [Google Scholar] [CrossRef] [Green Version]
- Nierenberg, A.A.; Husain, M.M.; Trivedi, M.H.; Fava, M.; Warden, D.; Wisniewski, S.R.; Miyahara, S.; Rush, A.J. Residual Symptoms after Remission of Major Depressive Disorder with Citalopram and Risk of Relapse: A STAR*D Report. Psychol. Med. 2010, 40, 41–50. [Google Scholar] [CrossRef] [Green Version]
- Judd, L.L.; Akiskal, H.S.; Maser, J.D.; Zeller, P.J.; Endicott, J.; Coryell, W.; Paulus, M.P.; Kunovac, J.L.; Leon, A.C.; Mueller, T.I.; et al. Major Depressive Disorder: A Prospective Study of Residual Subthreshold Depressive Symptoms as Predictor of Rapid Relapse. J. Affect Disord. 1998, 50, 97–108. [Google Scholar] [CrossRef]
- Malhi, G.S.; Morris, G.; Bell, E.; Hamilton, A. A New Paradigm for Achieving a Rapid Antidepressant Response. Drugs 2020, 80, 755–764. [Google Scholar] [CrossRef]
- Rodrigues, N.B.; McIntyre, R.S.; Lipsitz, O.; Cha, D.S.; Cao, B.; Lee, Y.; Gill, H.; Lui, L.M.W.; Cubała, W.J.; Ho, R.; et al. Do Sleep Changes Mediate the Anti-depressive and Anti-suicidal Response of Intravenous Ketamine in Treatment-resistant Depression? J. Sleep Res. 2022, 31, 13400. [Google Scholar] [CrossRef]
- Borentain, S.; Williamson, D.; Turkoz, I.; Popova, V.; McCall, W.V.; Mathews, M.; Wiegand, F. Effect of Sleep Disturbance on Efficacy of Esketamine in Treatment-Resistant Depression: Findings from Randomized Controlled Trials. NDT Neuropsychiatr. Dis. Treat. 2021, 17, 3459–3470. [Google Scholar] [CrossRef]
- Vande Voort, J.L.; Ballard, E.D.; Luckenbaugh, D.A.; Bernert, R.A.; Richards, E.M.; Niciu, M.J.; Park, L.T.; Machado-Vieira, R.; Duncan, W.C.; Zarate, C.A. Antisuicidal Response Following Ketamine Infusion Is Associated With Decreased Nighttime Wakefulness in Major Depressive Disorder and Bipolar Disorder. J. Clin. Psychiatry 2017, 78, 1068–1074. [Google Scholar] [CrossRef] [Green Version]
- Stultz, D.J.; Stanley, N.; Gills, T.; Osburn, S.; Burns, T.; Moomaw, S.; Pawlowska-Wajswol, S.; Walton, R. Three Months of Treatment With Esketamine: Effects on Depression, Insomnia, and Weight. Prim. Care Companion CNS Disord. 2020, 22, 19l02555. [Google Scholar] [CrossRef]
- Duncan, W.C.; Ballard, E.D.; Zarate, C.A. Ketamine-Induced Glutamatergic Mechanisms of Sleep and Wakefulness: Insights for Developing Novel Treatments for Disturbed Sleep and Mood. Handb. Exp. Pharmacol. 2019, 253, 337–358. [Google Scholar] [CrossRef]
- Bernert, R.A.; Turvey, C.L.; Conwell, Y.; Joiner, T.E. Association of Poor Subjective Sleep Quality with Risk for Death by Suicide during a 10-Year Period: A Longitudinal, Population-Based Study of Late Life. JAMA Psychiatry 2014, 71, 1129–1137. [Google Scholar] [CrossRef]
- Ballard, E.D.; Vande Voort, J.L.; Bernert, R.A.; Luckenbaugh, D.A.; Richards, E.M.; Niciu, M.J.; Furey, M.L.; Duncan, W.C.; Zarate, C.A. Nocturnal Wakefulness Is Associated With Next-Day Suicidal Ideation in Major Depressive Disorder and Bipolar Disorder. J. Clin. Psychiatry 2016, 77, 825–831. [Google Scholar] [CrossRef]
- Hiltunen, L.; Suominen, K.; Lönnqvist, J.; Partonen, T. Relationship between Daylength and Suicide in Finland. J. Circadian Rhythm. 2011, 9, 10. [Google Scholar] [CrossRef] [Green Version]
- Ballard, E.D.; Ionescu, D.F.; Vande Voort, J.L.; Niciu, M.J.; Richards, E.M.; Luckenbaugh, D.A.; Brutsché, N.E.; Ameli, R.; Furey, M.L.; Zarate, C.A. Improvement in Suicidal Ideation after Ketamine Infusion: Relationship to Reductions in Depression and Anxiety. J. Psychiatr. Res. 2014, 58, 161–166. [Google Scholar] [CrossRef] [Green Version]
- Benedetti, F.; Riccaboni, R.; Locatelli, C.; Poletti, S.; Dallaspezia, S.; Colombo, C. Rapid Treatment Response of Suicidal Symptoms to Lithium, Sleep Deprivation, and Light Therapy (Chronotherapeutics) in Drug-Resistant Bipolar Depression. J. Clin. Psychiatry 2014, 75, 133–140. [Google Scholar] [CrossRef]
- Breitstein, J.; Penix, B.; Roth, B.J.; Baxter, T.; Mysliwiec, V. Intensive Sleep Deprivation and Cognitive Behavioral Therapy for Pharmacotherapy Refractory Insomnia in a Hospitalized Patient. J. Clin. Sleep Med. 2014, 10, 689–690. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Lin, D.; Wu, B.; Zhou, W. Ketamine abuse potential and use disorder. Brain Res Bull. 2016, 126, 68–73. [Google Scholar] [CrossRef] [Green Version]
- Wichniak, A.; Wierzbicka, A.; Walęcka, M.; Jernajczyk, W. Effects of Antidepressants on Sleep. Curr. Psychiatry Rep. 2017, 19, 63. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, N.; Foy, K. The Impact of Residual Symptoms on Outcome of Major Depression. Curr. Psychiatry Rep. 2005, 7, 441–446. [Google Scholar] [CrossRef]
- Maj, M.; Stein, D.J.; Parker, G.; Zimmerman, M.; Fava, G.A.; De Hert, M.; Demyttenaere, K.; McIntyre, R.S.; Widiger, T.; Wittchen, H. The Clinical Characterization of the Adult Patient with Depression Aimed at Personalization of Management. World Psychiatry 2020, 19, 269–293. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Stang, A. Critical Evaluation of the Newcastle-Ottawa Scale for the Assessment of the Quality of Nonrandomized Studies in Meta-Analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- McGuinness, L.A.; Higgins, J.P. Risk-of-Bias VISualization (Robvis): An R Package and Shiny Web App for Visualizing Risk-of-Bias Assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Study Design | Number of Subjects | Population | Intervention and Route | Sleep Outcome Measures | Outcome |
|---|---|---|---|---|---|---|
| Rodrigues et al. 2022 [40] | Post hoc analysis Mean | 323 (175 female) 275 MDD 48 BPD | Treatment-resistant depression as part of major depressive disorder or bipolar depression Treatment resistance defined as failure of two or more adequate trials of different antidepressant classes | Four infusions of intravenous (IV) ketamine dosed at 0.5 mg/kg delivered over 40–45 min; dose increased to 0.75 mg/kg if no clinical response observed | QIDS-SR16 | Significant main effect of infusion on improvement in: insomnia, p < 0.001, effect size not stated; night-time restlessness, p = 0.007, effect size not stated; early morning waking, p = 0.04, effect size not stated; Non-significant effect of infusion on hypersomnia, p = 0.10 effect size not stated |
| Borentain et al. 2021 [41] | Post hoc analysis Mean ± SD Odds Ratio (95% CI) | 565 (379 female) | Treatment-resistant depression as part of MDD Treatment resistance defined as non-response to an adequate (dose and duration) course of at least two oral antidepressants during the current depressive episode | ADT + esketamine nasal spray in fixed or flexible dose; ADT + placebo | MADRSitem no. 4 | Significant improvement per MADRS item 4 in sleep disturbances in ketamine + ADT group compared to ADT standalone at every timepoint: on day 8 (p = 0.001, effect size not stated) and at all subsequent evaluation timepoints through day 28 (p = 0.020, effect size not stated) |
| Vande Voort et al. 2017 [42] | Post hoc analysis Mean ± SEM | 34 (14 female) 23 MDD 11 BPD 22 healthy controls | Treatment-resistant depression in MDD or BPD Subjects must have failed to respond to an adequate dose and duration of at least one antidepressant (SSRI, bupropion, or venlafaxine) during a depressive episode | Intravenous ketamine hydrochloride (0.5 mg/kg over 40 min) At least two weeks without psychotropic therapy (5 weeks for fluoxetine) prior to ketamine administration. Patients with BPD were medicated with either lithium or valproate. A subset of eleven patients received a single dose of riluzole. Analyses were conducted for both riluzole + ketamine and ketamine only. Since differences were not significant, analyses were conducted for the entire sample. | Nighttime electroencephalography (EEG) the night before and the night after a single ketamine infusion | Significant reduction of nocturnal wakefulness in suicide responder group (p = 0.04, d = 0.96) A trend between suicide responders to healthy controls (p = 0.08; d = 0.56), suggesting potential difference in mean minutes awake by hour of night |
| Duncan et al. 2013 [29] | Randomised controlled trial Mean ± SEM | 30 (10 female) | Treatment-resistant MDD TRD defined as a current or history of non-response to two adequate antidepressant trials | Ketamine + riluzole 100 mg/d; Ketamine + placebo Single IV infusion of 0.5 mg/kg ketamine hydrochloride over the course of 40 min At least two weeks without psychotropic therapy (5 weeks for fluoxetine) prior to ketamine administration. Groups were subsequently merged for statistical analysis, since riluzole had no statistical significance when it came to sleep outcome. | Nighttime EEG the night before and two nights after the infusion | Increase in total sleep time, slow wave sleep, and REM sleep (p < 0.05) and slow wave activity (p < 0.01) the night after single ketamine infusion. Reduction in S1, S2, REM latency and waking time the day after infusion (p < 0.05) |
| Stultz et al. 2020 [43] | Case report | 1 | Treatment-resistant depression Unsatisfactory response, despite taking fluoxetine, duloxetine, escitalopram, and bupropion in the past | Esketamine nasal spray up to 84 mg | ISI PSQI | PSQI score decreased from 13 to 8; ISI score decreased from 11 to 7. |
| Study | Rodrigues 2022 [40] | |
|---|---|---|
| Selection | Representativeness of the exposed cohort | 1 |
| Selection of the non-exposed cohort | − | |
| Ascertainment of exposure | 1 | |
| Demonstration that outcome of interest was not present at start of study | 1 | |
| Comparability | Comparability of cohorts on the basis of the design or analysis controlled for confounders | 2 |
| Outcome | Assessment of outcome | − |
| Was follow-up long enough for outcomes to occur | 1 | |
| Adequacy of follow-up of cohorts | 1 | |
| Total | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwaśny, A.; Włodarczyk, A.; Ogonowski, D.; Cubała, W.J. Effect of Ketamine on Sleep in Treatment-Resistant Depression: A Systematic Review. Pharmaceuticals 2023, 16, 568. https://doi.org/10.3390/ph16040568
Kwaśny A, Włodarczyk A, Ogonowski D, Cubała WJ. Effect of Ketamine on Sleep in Treatment-Resistant Depression: A Systematic Review. Pharmaceuticals. 2023; 16(4):568. https://doi.org/10.3390/ph16040568
Chicago/Turabian StyleKwaśny, Aleksander, Adam Włodarczyk, Damian Ogonowski, and Wiesław Jerzy Cubała. 2023. "Effect of Ketamine on Sleep in Treatment-Resistant Depression: A Systematic Review" Pharmaceuticals 16, no. 4: 568. https://doi.org/10.3390/ph16040568