
Umbilical Cord Mesenchymal Stromal Cells for Steroid-Refractory Acute Graft-versus-Host Disease
 , , , , , , add
Show full author list
, , , , , , add
Show full author list
Abstract
:1. Introduction
2. Results
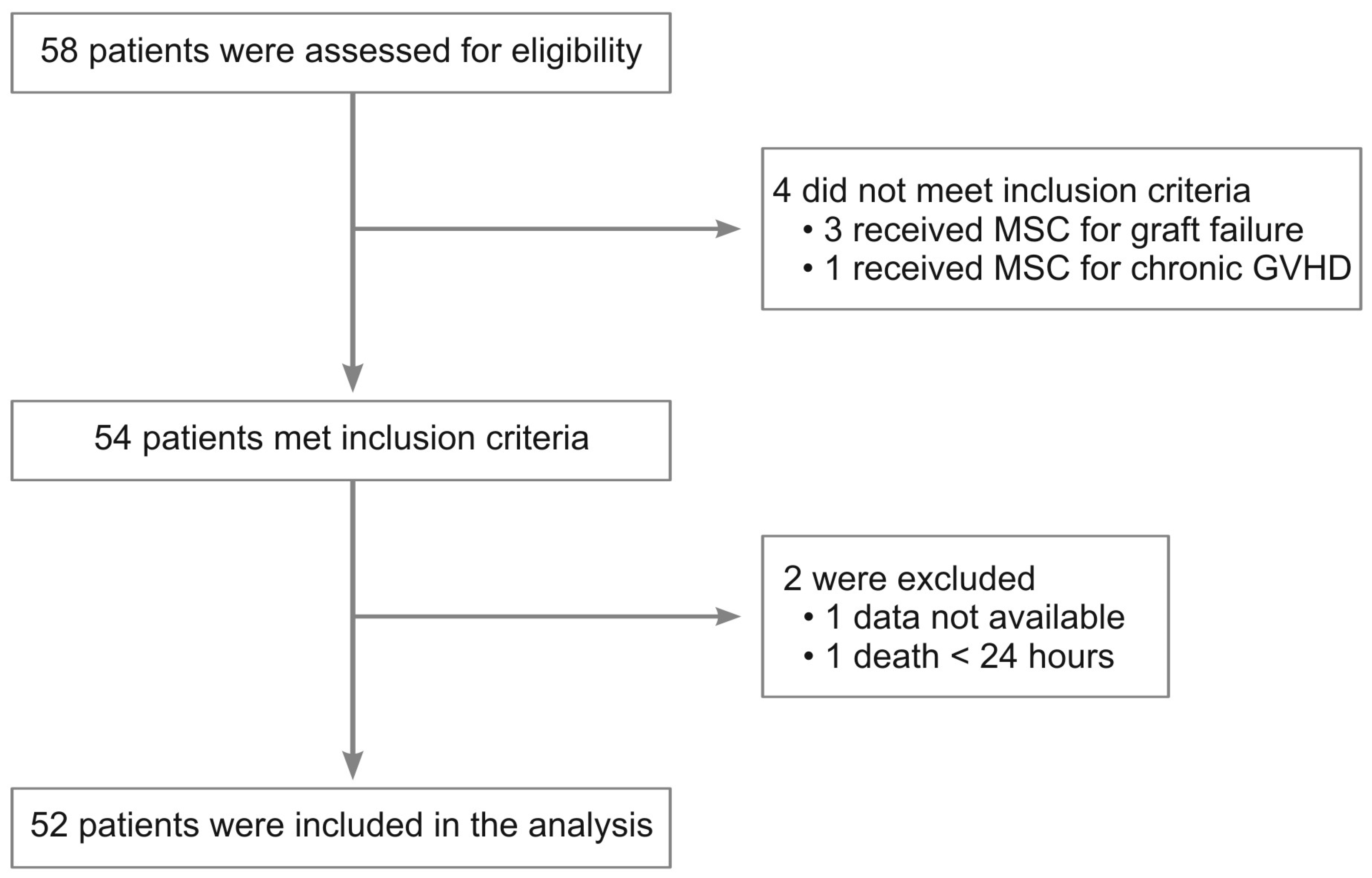
2.1. Patients’ Characteristics, Infused Cell Dose, and Schedule
2.2. Efficacy
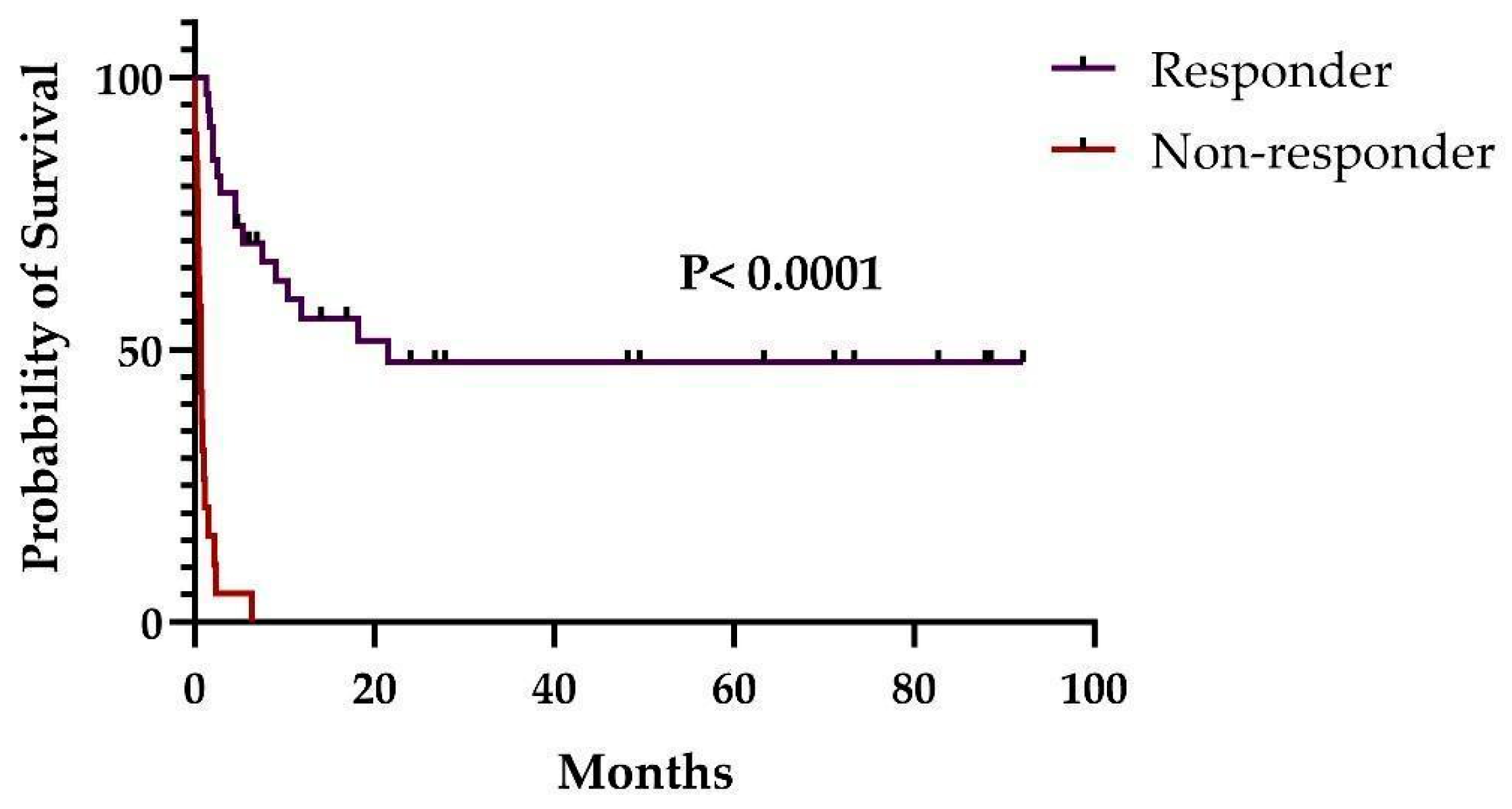
2.2.1. Overall Response (OR)
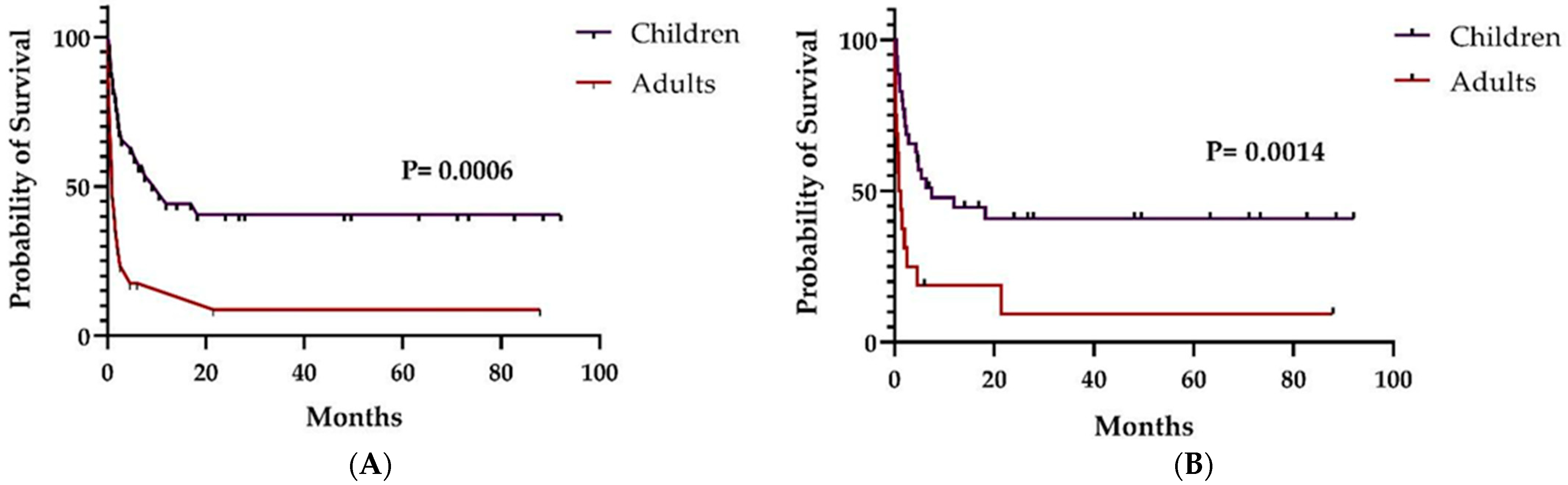
2.2.2. Overall (OS) and Relapse-Free Survival (RFS)
2.2.3. Chronic GVHD
2.3. Safety
3. Materials and Methods
3.1. Study Design
3.2. Patients
3.3. Mesenchymal Stromal Cells
3.4. Variables of Interest
3.5. Endpoints
3.6. Statistical Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zaia, J.; Baden, L.; Boeckh, M.J.; Chakrabarti, S.; Einsele, H.; Ljungman, P.; McDonald, G.B.; Hirsch, H. Viral Disease Prevention after Hematopoietic Cell Transplantation. Bone Marrow Transplant. 2009, 44, 471–482. [Google Scholar] [CrossRef]
- Girmenia, C.; Raiola, A.M.; Piciocchi, A.; Algarotti, A.; Stanzani, M.; Cudillo, L.; Pecoraro, C.; Guidi, S.; Iori, A.P.; Montante, B.; et al. Incidence and Outcome of Invasive Fungal Diseases after Allogeneic Stem Cell Transplantation: A Prospective Study of the Gruppo Italiano Trapianto Midollo Osseo (GITMO). Biol. Blood Marrow Transplant. 2014, 20, 872–880. [Google Scholar] [CrossRef]
- Girmenia, C.; Bertaina, A.; Piciocchi, A.; Perruccio, K.; Algarotti, A.; Busca, A.; Cattaneo, C.; Raiola, A.M.; Guidi, S.; Iori, A.P.; et al. Incidence, Risk Factors and Outcome of Pre-Engraftment Gram-Negative Bacteremia after Allogeneic and Autologous Hematopoietic Stem Cell Transplantation: An Italian Prospective Multicenter Survey. Clin. Infect. Dis. 2017, 65, 1884–1896. [Google Scholar] [CrossRef]
- Anasetti, C.; Beatty, P.G.; Storb, R.; Martin, P.J.; Mori, M.; Sanders, J.E.; Donnall Thomas, E.; Hansen, J.A. Effect of HLA Incompatibility on Graft-versus-Host Disease, Relapse, and Survival after Marrow Transplantation for Patients with Leukemia or Lymphoma. Hum. Immunol. 1990, 29, 79–91. [Google Scholar] [CrossRef]
- Lee, S.J.; Klein, J.; Haagenson, M.; Baxter-Lowe, L.A.; Confer, D.L.; Eapen, M.; Fernandez-Vina, M.; Flomenberg, N.; Horowitz, M.; Hurley, C.K.; et al. High-Resolution Donor-Recipient HLA Matching Contributes to the Success of Unrelated Donor Marrow Transplantation. Blood 2007, 110, 4576–4583. [Google Scholar] [CrossRef]
- Flowers, M.E.D.; Pepe, M.S.; Longton, G.; Doney, K.C.; Monroe, D.; Witherspoon, R.P.; Sullivan, K.M.; Storb, R. Previous Donor Pregnancy as a Risk Factor for Acute Graft-versus-Host Disease in Patients with Aplastic Anaemia Treated by Allogeneic Marrow Transplantation. Br. J. Haematol. 1990, 74, 492–496. [Google Scholar] [CrossRef]
- Eisner, M.D.; August, C.S. Impact of Donor and Recipient Characteristics on the Development of Acute and Chronic Graft-versus-Host Disease Following Pediatric Bone Marrow Transplantation. Bone Marrow Transplant. 1995, 15, 663–668. [Google Scholar]
- Hahn, T.; McCarthy, P.L.; Zhang, M.-J.; Wang, D.; Arora, M.; Frangoul, H.; Gale, R.P.; Hale, G.A.; Horan, J.; Isola, L.; et al. Risk Factors for Acute Graft-Versus-Host Disease After Human Leukocyte Antigen–Identical Sibling Transplants for Adults With Leukemia. J. Clin. Oncol. 2008, 26, 5728–5734. [Google Scholar] [CrossRef]
- Holtick, U.; Albrecht, M.; Chemnitz, J.M.; Theurich, S.; Skoetz, N.; Scheid, C.; von Bergwelt-Baildon, M. Bone Marrow versus Peripheral Blood Allogeneic Haematopoietic Stem Cell Transplantation for Haematological Malignancies in Adults. Cochrane Database Syst. Rev. 2014, 4, 010189. [Google Scholar] [CrossRef]
- Zeiser, R.; Blazar, B.R. Acute Graft-versus-Host Disease Biology, Prevention and Therapy. N. Engl. J. Med. 2017, 377, 2167–2179. [Google Scholar] [CrossRef]
- Schoemans, H.M.; Lee, S.J.; Ferrara, J.L.; Wolff, D.; Levine, J.E.; Schultz, K.R.; Shaw, B.E.; Flowers, M.E.; Ruutu, T.; Greinix, H.; et al. EBMT—NIH—CIBMTR Task Force Position Statement on Standardized Terminology & Guidance for Graft-versus-Host Disease Assessment. Bone Marrow Transplant. 2018, 53, 1401–1415. [Google Scholar] [CrossRef]
- Ferrara, J.L.; Levine, J.E.; Reddy, P.; Holler, E. Graft-versus-Host Disease. Lancet 2009, 373, 1550–1561. [Google Scholar] [CrossRef]
- Harris, A.C.; Young, R.; Devine, S.; Hogan, W.J.; Ayuk, F.; Bunworasate, U.; Chanswangphuwana, C.; Efebera, Y.A.; Holler, E.; Litzow, M.; et al. International, Multicenter Standardization of Acute Graft-versus-Host Disease Clinical Data Collection: A Report from the Mount Sinai Acute GVHD International Consortium. Biol. Blood Marrow Transplant. 2016, 22, 4–10. [Google Scholar] [CrossRef]
- Martin, P.J.; Rizzo, J.D.; Wingard, J.R.; Ballen, K.; Curtin, P.T.; Cutler, C.; Litzow, M.R.; Nieto, Y.; Savani, B.N.; Schriber, J.R.; et al. First- and Second-Line Systemic Treatment of Acute Graft-versus-Host Disease: Recommendations of the American Society of Blood and Marrow Transplantation. Biol. Blood Marrow Transplant. 2012, 18, 1150–1163. [Google Scholar] [CrossRef]
- MacMillan, M.L.; Robin, M.; Harris, A.C.; DeFor, T.E.; Martin, P.J.; Alousi, A.; Ho, V.T.; Bolaños-Meade, J.; Ferrara, J.L.M.; Jones, R.; et al. A Refined Risk Score for Acute Graft-versus-Host Disease That Predicts Response to Initial Therapy, Survival, and Transplant-Related Mortality. Biol. Blood Marrow Transplant. 2015, 21, 761–767. [Google Scholar] [CrossRef]
- Westin, J.R.; Saliba, R.M.; De Lima, M.; Alousi, A.; Hosing, C.; Qazilbash, M.H.; Khouri, I.F.; Shpall, E.J.; Anderlini, P.; Rondon, G.; et al. Steroid-Refractory Acute GVHD: Predictors and Outcomes. Adv. Hematol. 2011, 2011, 601953. [Google Scholar] [CrossRef]
- Jagasia, M.; Perales, M.-A.; Schroeder, M.A.; Ali, H.; Shah, N.N.; Chen, Y.-B.; Fazal, S.; Dawkins, F.W.; Arbushites, M.C.; Tian, C.; et al. Ruxolitinib for the Treatment of Steroid-Refractory Acute GVHD (REACH1): A Multicenter, Open-Label Phase 2 Trial. Blood 2020, 135, 1739–1749. [Google Scholar] [CrossRef]
- Zeiser, R.; von Bubnoff, N.; Butler, J.; Mohty, M.; Niederwieser, D.; Or, R.; Szer, J.; Wagner, E.M.; Zuckerman, T.; Mahuzier, B.; et al. Ruxolitinib for Glucocorticoid-Refractory Acute Graft-versus-Host Disease. N. Engl. J. Med. 2020, 382, 1800–1810. [Google Scholar] [CrossRef]
- Abedin, S.; Hamadani, M. Experimental Pharmaceuticals for Steroid-Refractory Acute Graft-versus-Host Disease. J. Exp. Pharm. 2020, 12, 549–557. [Google Scholar] [CrossRef]
- Mizukami, A.; Swiech, K. Mesenchymal Stromal Cells: From Discovery to Manufacturing and Commercialization. Stem Cells Int. 2018, 2018, 4083921. [Google Scholar] [CrossRef]
- Mushahary, D.; Spittler, A.; Kasper, C.; Weber, V.; Charwat, V. Isolation, Cultivation, and Characterization of Human Mesenchymal Stem Cells. Cytom. A 2018, 93, 19–31. [Google Scholar] [CrossRef]
- De Santis, G.C.; de Macedo, L.D.; Orellana, M.D.; Innocentini, L.M.A.R.; Ferrari, T.C.; Ricz, H.M.A.; Caruso, S.R.; Fernandes, T.R.; Covas, D.T. Mesenchymal Stromal Cells Administration for Osteonecrosis of the Jaw Caused by Bisphosphonate: Report of Two Cases. Acta Oncol. 2020, 59, 789–792. [Google Scholar] [CrossRef]
- Farina Junior, J.A.; De Santis, G.C.; Orellana, M.D.; Silva-Pinto, A.C.; de Oliveira Guirro, E.C.; de Carvalho, C.S.; Zampar, A.G.; Coltro, P.S.; Tirapeli, L.F.; Covas, D.T. Autologous Adipose-Derived Stem Cell for Painful Leg Ulcers in Patients with Sickle Cell Disease. A Preliminary Study. Br. J. Haematol. 2019, 186, e47–e50. [Google Scholar] [CrossRef]
- Markov, A.; Thangavelu, L.; Aravindhan, S.; Zekiy, A.O.; Jarahian, M.; Chartrand, M.S.; Pathak, Y.; Marofi, F.; Shamlou, S.; Hassanzadeh, A. Mesenchymal Stem/Stromal Cells as a Valuable Source for the Treatment of Immune-Mediated Disorders. Stem Cell Res. Ther. 2021, 12, 192. [Google Scholar] [CrossRef]
- Burnham, A.J.; Daley-Bauer, L.P.; Horwitz, E.M. Mesenchymal Stromal Cells in Hematopoietic Cell Transplantation. Blood Adv. 2020, 4, 5877–5887. [Google Scholar] [CrossRef]
- Cheung, T.S.; Bertolino, G.M.; Giacomini, C.; Bornhäuser, M.; Dazzi, F.; Galleu, A. Mesenchymal Stromal Cells for Graft Versus Host Disease: Mechanism-Based Biomarkers. Front. Immunol. 2020, 11, 1338. [Google Scholar] [CrossRef]
- Le Blanc, K.; Rasmusson, I.; Sundberg, B.; Götherström, C.; Hassan, M.; Uzunel, M.; Ringdén, O. Treatment of Severe Acute Graft-versus-Host Disease with Third Party Haploidentical Mesenchymal Stem Cells. Lancet 2004, 363, 1439–1441. [Google Scholar] [CrossRef]
- Le Blanc, K.; Frassoni, F.; Ball, L.; Locatelli, F.; Roelofs, H.; Lewis, I.; Lanino, E.; Sundberg, B.; Bernardo, M.E.; Remberger, M.; et al. Mesenchymal Stem Cells for Treatment of Steroid-Resistant, Severe, Acute Graft-versus-Host Disease: A Phase II Study. Lancet 2008, 371, 1579–1586. [Google Scholar] [CrossRef]
- Kurtzberg, J.; Abdel-Azim, H.; Carpenter, P.; Chaudhury, S.; Horn, B.; Mahadeo, K.; Nemecek, E.; Neudorf, S.; Prasad, V.; Prockop, S.; et al. A Phase 3, Single-Arm, Prospective Study of Remestemcel-L, Ex Vivo Culture-Expanded Adult Human Mesenchymal Stromal Cells for the Treatment of Pediatric Patients Who Failed to Respond to Steroid Treatment for Acute Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2020, 26, 845–854. [Google Scholar] [CrossRef]
- Kurtzberg, J.; Prockop, S.; Chaudhury, S.; Horn, B.; Nemecek, E.; Prasad, V.; Satwani, P.; Teira, P.; Hayes, J.; Burke, E.; et al. Study 275: Updated Expanded Access Program for Remestemcel-L in Steroid-Refractory Acute Graft-versus-Host Disease in Children. Biol. Blood Marrow Transplant. 2020, 26, 855–864. [Google Scholar] [CrossRef]
- Kelly, K.; Rasko, J.E.J. Mesenchymal Stromal Cells for the Treatment of Graft Versus Host Disease. Front. Immunol. 2021, 26, 761616. [Google Scholar] [CrossRef] [PubMed]
- Penack, O.; Marchetti, M.; Ruutu, T.; Aljurf, M.; Bacigalupo, A.; Bonifazi, F.; Ciceri, F.; Cornelissen, J.; Malladi, R.; Duarte, R.F.; et al. Prophylaxis and Management of Graft versus Host Disease after Stem-Cell Transplantation for Haematological Malignancies: Updated Consensus Recommendations of the European Society for Blood and Marrow Transplantation. Lancet Haematol. 2020, 7, e157–e167. [Google Scholar] [CrossRef]
- Dotoli, G.M.; De Santis, G.C.; Orellana, M.D.; de Lima Prata, K.; Caruso, S.R.; Fernandes, T.R.; Rensi Colturato, V.A.; Kondo, A.T.; Hamerschlak, N.; Simões, B.P.; et al. Mesenchymal Stromal Cell Infusion to Treat Steroid-Refractory Acute GvHD III/IV after Hematopoietic Stem Cell Transplantation. Bone Marrow Transplant. 2017, 52, 859–862. [Google Scholar] [CrossRef]
- Ding, Y.; Liu, C.; Cai, Y.; Hou, C.; Chen, G.; Xu, Y.; Hu, S.; Wu, D. The Efficiency of Human Umbilical Cord Mesenchymal Stem Cells as a Salvage Treatment for Steroid-Refractory Acute Graft-versus-Host Disease. Clin. Exp. Med. 2023. [Google Scholar] [CrossRef]
- Mendoza, T.R.; Dueck, A.C.; Bennett, A.V.; Mitchell, S.A.; Reeve, B.B.; Atkinson, T.M.; Li, Y.; Castro, K.M.; Denicoff, A.; Rogak, L.J.; et al. Evaluation of Different Recall Periods for the US National Cancer Institute’s Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). Clin. Trials 2017, 14, 255–263. [Google Scholar] [CrossRef]
- Bacigalupo, A.; Ballen, K.; Rizzo, D.; Giralt, S.; Lazarus, H.; Ho, V.; Apperley, J.; Slavin, S.; Pasquini, M.; Sandmaier, B.M.; et al. Defining the Intensity of Conditioning Regimens: Working Definitions. Biol. Blood Marrow Transplant. 2009, 15, 1628–1633. [Google Scholar] [CrossRef]
- Kebriaei, P.; Hayes, J.; Daly, A.; Uberti, J.; Marks, D.I.; Soiffer, R.; Waller, E.K.; Burke, E.; Skerrett, D.; Shpall, E.; et al. A Phase 3 Randomized Study of Remestemcel-L versus Placebo Added to Second-Line Therapy in Patients with Steroid-Refractory Acute Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2020, 26, 835–844. [Google Scholar] [CrossRef]
- Murata, M.; Terakura, S.; Wake, A.; Miyao, K.; Ikegame, K.; Uchida, N.; Kataoka, K.; Miyamoto, T.; Onizuka, M.; Eto, T.; et al. Off-the-Shelf Bone Marrow-Derived Mesenchymal Stem Cell Treatment for Acute Graft-versus-Host Disease: Real-World Evidence. Bone Marrow Transplant. 2021, 56, 2355–2366. [Google Scholar] [CrossRef]
- Locatelli, F.; Kang, H.J.; Bruno, B.; Gandemer, V.; Rialland, F.; Faraci, M.; Takahashi, Y.; Koh, K.; Bittencourt, H.; Cleary, G.; et al. Ruxolitinib in Pediatric Patients with Treatment-Naïve or Steroid-Refractory Acute Graft-Versus-Host Disease: Primary Findings from the Phase I/II REACH4 Study. Blood 2022, 140, 1376–1378. [Google Scholar] [CrossRef]
- Arai, S.; Arora, M.; Wang, T.; Spellman, S.R.; He, W.; Couriel, D.R.; Urbano-Ispizua, A.; Cutler, C.S.; Bacigalupo, A.A.; Battiwalla, M.; et al. Increasing Incidence of Chronic Graft-versus-Host Disease in Allogeneic Transplantation—A Report from CIBMTR. Biol. Blood Marrow Transplant. 2015, 21, 266–274. [Google Scholar] [CrossRef]
- Fisher, S.A.; Cutler, A.; Doree, C.; Brunskill, S.J.; Stanworth, S.J.; Navarrete, C.; Girdlestone, J. Mesenchymal Stromal Cells as Treatment or Prophylaxis for Acute or Chronic Graft-versus-host Disease in Haematopoietic Stem Cell Transplant (HSCT) Recipients with a Haematological Condition. Cochrane Database Syst. Rev. 2019, 2019, CD009768. [Google Scholar] [CrossRef] [PubMed]
- Lalu, M.M.; McIntyre, L.; Pugliese, C.; Fergusson, D.; Winston, B.W.; Marshall, J.C.; Granton, J.; Stewart, D.J. Safety of Cell Therapy with Mesenchymal Stromal Cells (SafeCell): A Systematic Review and Meta-Analysis of Clinical Trials. PLoS ONE 2012, 7, e47559. [Google Scholar] [CrossRef]
- Thompson, M.; Mei, S.H.J.; Wolfe, D.; Champagne, J.; Fergusson, D.; Stewart, D.J.; Sullivan, K.J.; Doxtator, E.; Lalu, M.; English, S.W.; et al. Cell Therapy with Intravascular Administration of Mesenchymal Stromal Cells Continues to Appear Safe: An Updated Systematic Review and Meta-Analysis. EClinicalMedicine 2020, 19, 100249. [Google Scholar] [CrossRef] [PubMed]
- Ringdén, O.; Moll, G.; Gustafsson, B.; Sadeghi, B. Mesenchymal Stromal Cells for Enhancing Hematopoietic Engraftment and Treatment of Graft-Versus-Host Disease, Hemorrhages and Acute Respiratory Distress Syndrome. Front. Immunol. 2022, 13, 945. [Google Scholar] [CrossRef] [PubMed]
- Kuçi, Z.; Bönig, H.; Kreyenberg, H.; Bunos, M.; Jauch, A.; Janssen, J.W.G.; Škifić, M.; Michel, K.; Eising, B.; Lucchini, G.; et al. Mesenchymal Stromal Cells from Pooled Mononuclear Cells of Multiple Bone Marrow Donors as Rescue Therapy in Pediatric Severe Steroid-Refractory Graft-versus-Host Disease: A Multicenter Survey. Haematologica 2016, 101, 985–994. [Google Scholar] [CrossRef] [PubMed]
- Ringdén, O.; Gustafsson, B.; Sadeghi, B. Mesenchymal Stromal Cells in Pediatric Hematopoietic Cell Transplantation a Review and a Pilot Study in Children Treated with Decidua Stromal Cells for Acute Graft-versus-Host Disease. Front. Immunol. 2020, 11, 567210. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 52) | Children (n = 35) | Adults (n = 17) | p-Value | |
|---|---|---|---|---|
| Age (years), median (range) | 12.5 (0.3–65) | 8 (0.3–16) | 32 (20–65) | |
| Male (%) | 34 (65.4) | 23 (65.7) | 11 (64.7) | 1.0 |
| Diagnosis (%) | 0.02 | |||
| Acute leukemia/MDS | 39 (75.0) | 30 (85.7) | 9 (52.9) | |
| Lymphoma | 3 (5.8) | 0 | 3 (17.6) | |
| Aplastic anemia | 4 (7.7) | 2 (5.7) | 2 (11.8) | |
| Others | 7 (11.5) | 3 (8.6) | 3 (17.6) | |
| Conditioning regimen (%) | 0.002 | |||
| MAC | 41 (78.8) | 32 (91.4) | 9 (52.9) | |
| RIC | 11 (21.2) | 3 (8.6) | 8 (47.1) | |
| Graft source (%) | <0.0001 | |||
| BM | 30 (57.7) | 27 (77.1) | 3 (17.6) | |
| PBSC | 20 (38.5) | 6 (17.2) | 14 (82.4) | |
| UCB | 2 (3.8) | 2 (5.7) | 0 | |
| aGVHD severity (%) | 0.37 | |||
| II | 2 (3.8) | 2 (5.7) | 0 | |
| III | 13 (25.0) | 10 (28.6) | 3 (17.6) | |
| IV | 37 (71.2) | 23 (65.7) | 14 (82.4) | |
| Organs affected (%) | 0.79 | |||
| Skin | 39 (75.0) | 23 (65.7) | 16 (94.1) | |
| Gut | 50 (96.2) | 33 (94.3) | 17 (100) | |
| Liver | 21 (38.5) | 13 (37.1) | 8 (47.1) | |
| Days to MSCs infusion *, median (range) | 36.5 (4–294) | 39 (4–250) | 27 (12–294) | 0.6 |
| N° of MSCs infusions, median (range) | 4 (1–11) | 4 (1–11) | 3 (1–8) | 0.06 |
| MSCs Dose (×106/kg), mean ± SD | 4.73 ± 1.30 | 4.93 ± 1.4 | 4.31 ± 0.98 | 0.11 |
| Total (n = 52) | Children (n = 35) | Adults (n = 17) | p-Value | |
|---|---|---|---|---|
| OR day 28 (%) | 33 (63.5) | 25 (71.5) | 8 (47.1) | 0.12 |
| CR | 19 (36.6) | 17 (48.6) | 2 (11.8) | 0.03 |
| PR | 14 (26.9) | 8 (22.9) | 6 (35.3) | |
| OR day 100 (%) | 19 (36.6) | 16 (45.7) | 3 (17.7) | 0.06 |
| CR | 16 (30.8) | 15 (42.8) | 1 (5.9) | 0.008 |
| PR | 3 (5.8) | 1 (2.9) | 2 (11.8) | |
| OR day 180 (%) | 18 (34.6) | 16 (45.7) | 2 (11.8) | 0.02 |
| CR | 17 (32.7) | 15 (42.8) | 2 (11.8) | 0.05 |
| PR | 1 (1.9) | 1 (2.9) | 0 | |
| OR 1 year (%) | 15 (28.8) | 13 (37.2) | 2 (11.8) | 0.1 |
| CR | 14 (26.9) | 12 (34.3) | 2 (11.8) | 0.15 |
| PR | 1 (1.9) | 1 (2.9) | 0 | |
| OR 2 years (%) | 14 (26.9) | 12 (34.3) | 2 (11.8) | 0.1 |
| CR | 14 (26.9) | 12 (34.3) | 2 (11.8) | |
| PR | 0 | 0 | 0 |
| Total (n = 52) | Children (n = 35) | Adults (n = 17) | p-Value | |
|---|---|---|---|---|
| Adverse Events (%) | 17 (32.7) | 12 (34.3) | 5 (29.4) | 1.0 |
| Tachycardia/bradycardia | 6 (11.5) | 2 | 4 | |
| Hypertension/Hypotension | 4 (7.7) | 2 | 2 | |
| Dyspnea | 2 (3.8) | 1 | 1 | |
| Nausea/vomit/abdominal cramps | 7 (13.5) | 7 | 0 | |
| Headache/dizziness | 5 (9.6) | 4 | 1 | |
| Seizures | 1 (1.9) | 1 | 0 | |
| Fever/chills | 5 (9.6) | 4 | 1 | |
| Rash/pruritus | 2 (3.8) | 1 | 1 | |
| Angioedema | 1 (1.9) | 1 | 0 |
| Kebriaei (2020) [37] | Kurtzberg (2020) [29] | Kurtzberg (2020) [30] | Murata (2021) [38] | Ding (2023) [34] | Donadel c (2023) | |
|---|---|---|---|---|---|---|
| Type of study | phase 3 | phase 3 | expanded access | retrospective | retrospective | retrospective |
| Participants | 163 | 54 | 241 | 309 | 54 | 52 |
| Age a | 43.8 | 7.0 | 9.6 | 49 | 12.5 | 12.5 |
| Severe aGVHD b (%) | 77.3 | 88.8 | 80.1 | 80.5 | 88.8 | 96.2 |
| Source of MSC | BM | BM | BM | BM | UC | UC |
| Lines of therapy | ≥3 | 2 | ≥2 | ≥1 | ≥3 | ≥3 |
| No of infusions a | 8.8 | 9.9 | 11 | 8 | 2 | 4 |
| Dose per infusion (×106/kg) | 2 | 2 | 2 | 2 | 2.54 | 4.73 |
| Time to infusion (days) a | - | 12 | 23 | 29 | 19 | 36.5 |
| OR day 28 (%) | 58.3 | 70.4 | 65.1 | 56 | 59.3 | 63.5 (71.5) d |
| CR day 28 (%) | - | 29.6 | 14.1 | 24 | 44.4 | 36.6 (48.6) d |
| OS day 100 (%) | - | 74.1 | 66.9 | - | - | 51.9 (62.9) d |
| OS day 180 (%) | 34 | 68.5 | - | 40 | - | 38.5 (48.6) d |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donadel, C.D.; Pires, B.G.; André, N.C.; Costa, T.C.M.; Orellana, M.D.; Caruso, S.R.; Seber, A.; Ginani, V.C.; Gomes, A.A.; Novis, Y.; et al. Umbilical Cord Mesenchymal Stromal Cells for Steroid-Refractory Acute Graft-versus-Host Disease. Pharmaceuticals 2023, 16, 512. https://doi.org/10.3390/ph16040512
Donadel CD, Pires BG, André NC, Costa TCM, Orellana MD, Caruso SR, Seber A, Ginani VC, Gomes AA, Novis Y, et al. Umbilical Cord Mesenchymal Stromal Cells for Steroid-Refractory Acute Graft-versus-Host Disease. Pharmaceuticals. 2023; 16(4):512. https://doi.org/10.3390/ph16040512
Chicago/Turabian StyleDonadel, Camila Derminio, Bruno Garcia Pires, Nathália Cristine André, Thalita Cristina Mello Costa, Maristela Delgado Orellana, Sâmia Rigotto Caruso, Adriana Seber, Valéria Cortez Ginani, Alessandra Araújo Gomes, Yana Novis, and et al. 2023. "Umbilical Cord Mesenchymal Stromal Cells for Steroid-Refractory Acute Graft-versus-Host Disease" Pharmaceuticals 16, no. 4: 512. https://doi.org/10.3390/ph16040512