
Effects of Simvastatin on Pharmacokinetics and Anticoagulant Effects of Dabigatran in Healthy Subjects
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Subjects
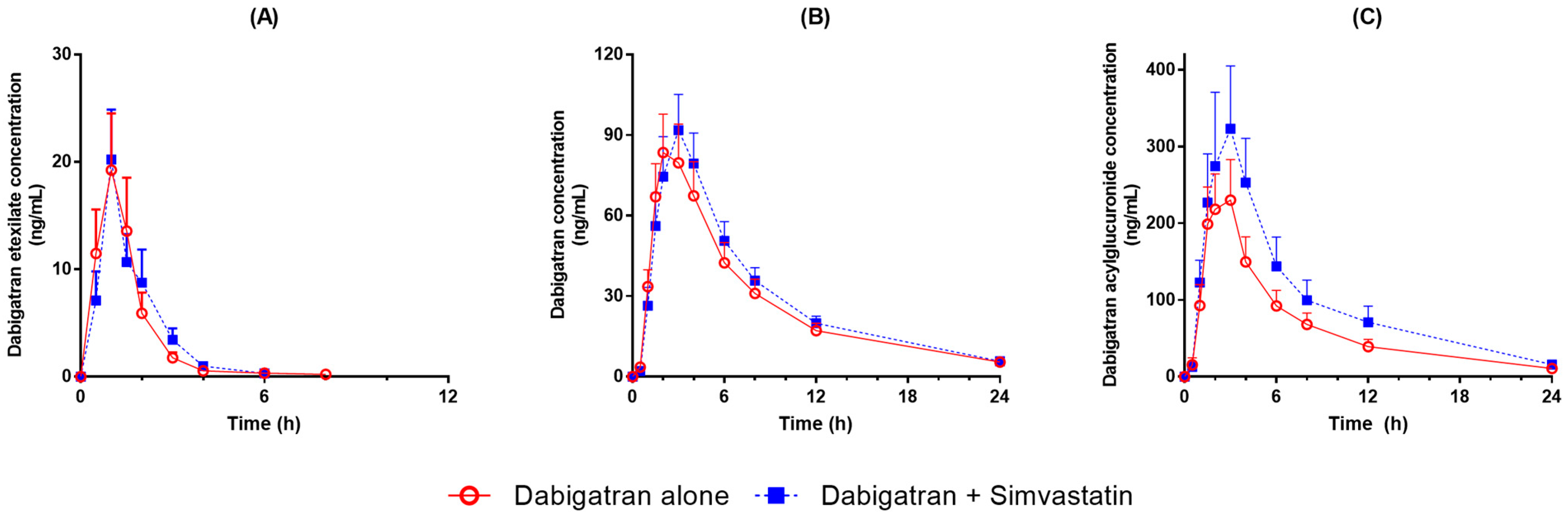
2.2. Effects of Simvastatin on Dabigatran Pharmacokinetics
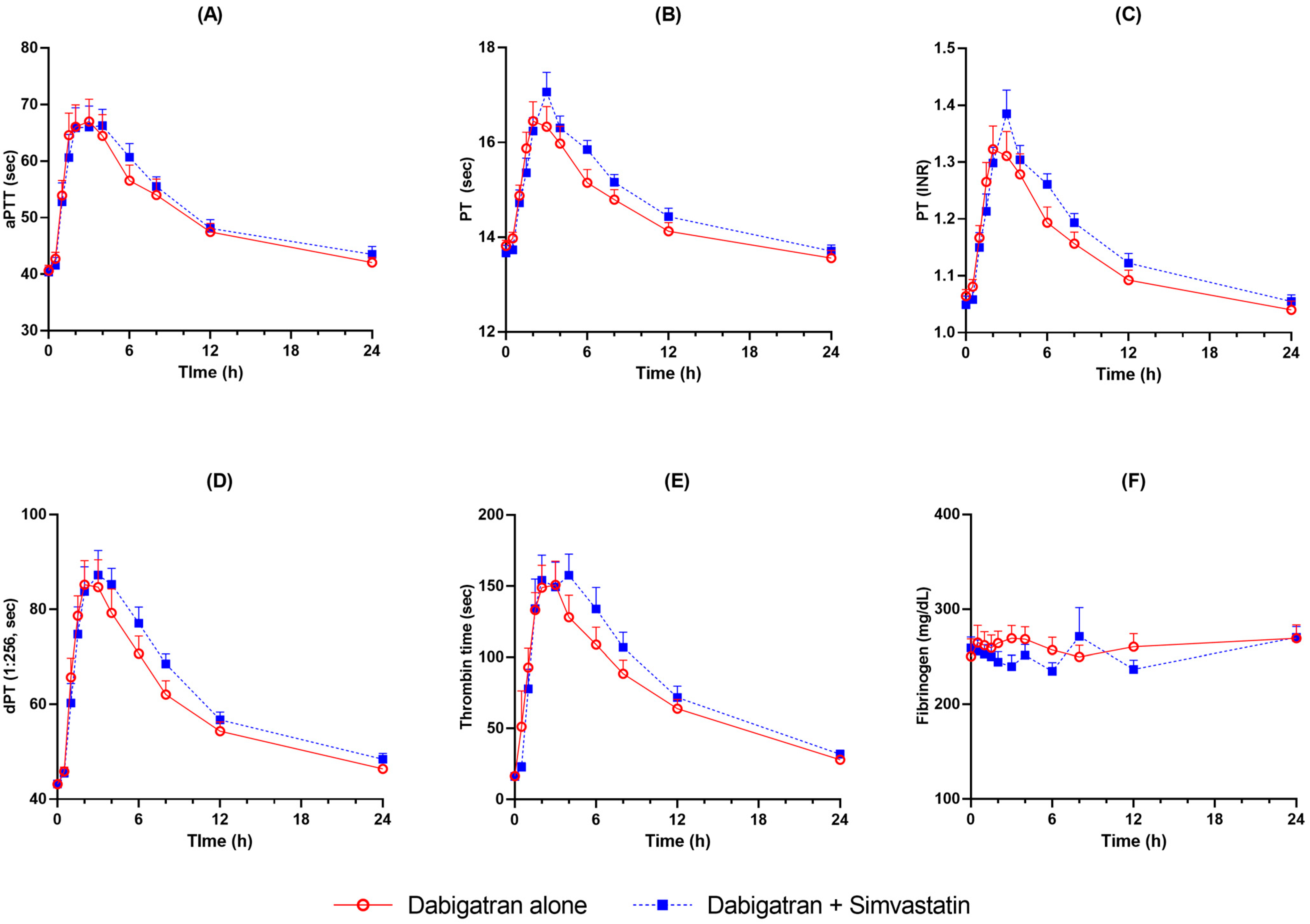
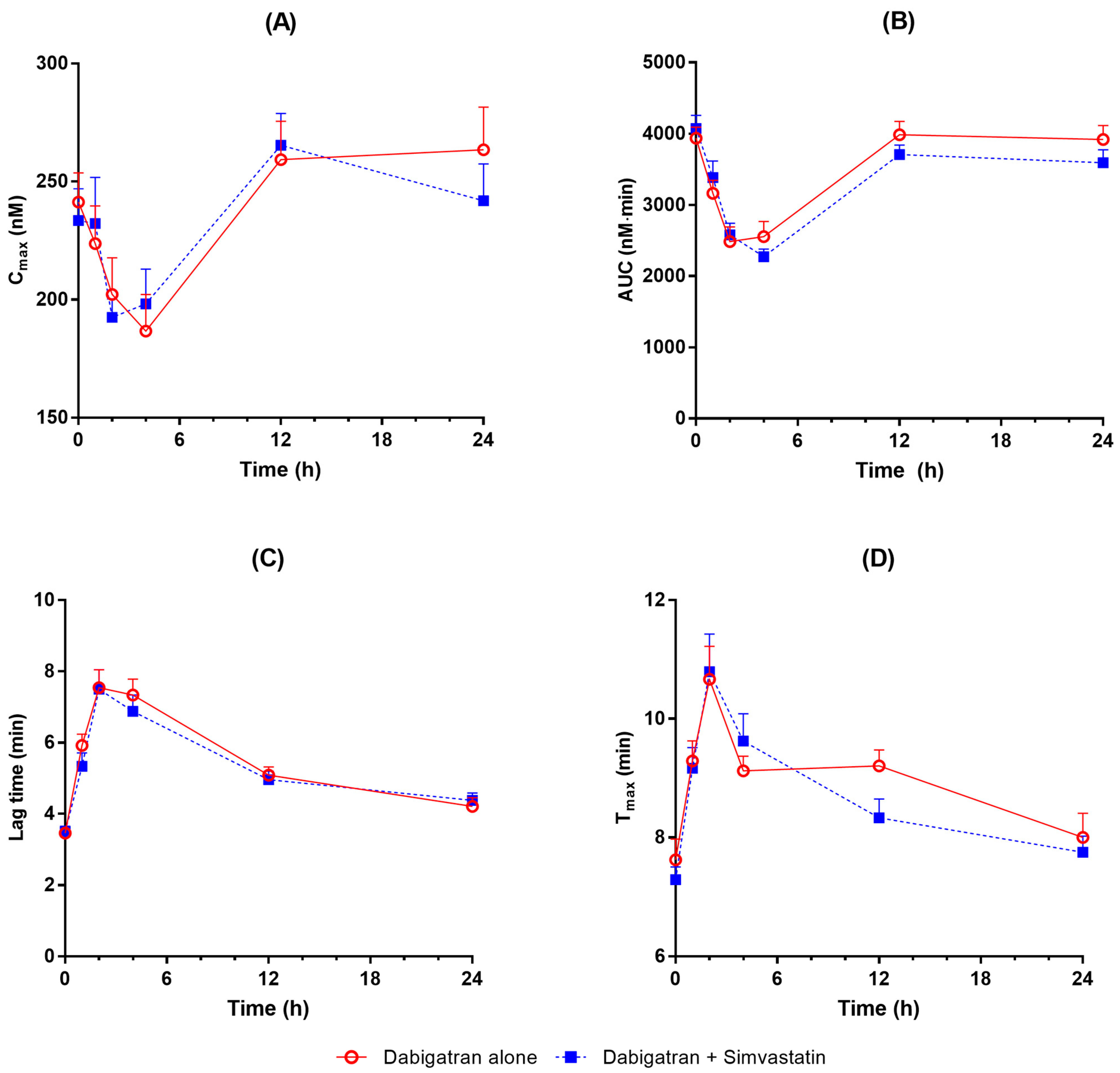
2.3. Effects of Simvastatin on Dabigatran Anticoagulant Effects
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Study Design
4.3. Determination of Dabigatran Etexilate, Dabigatran, and Dabigatran Acylglucuronide
4.4. Anticoagulant Assay
4.5. Pharmacokinetic and Pharmacodynamic Analyses
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wienen, W.; Stassen, J.M.; Priepke, H.; Ries, U.J.; Hauel, N. In-vitro profile and ex-vivo anticoagulant activity of the direct thrombin inhibitor dabigatran and its orally active prodrug, dabigatran etexilate. Thromb. Haemost. 2007, 98, 155–162. [Google Scholar]
- PRADAXA® Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/022512s041lbl.pdf (accessed on 13 September 2022).
- Stangier, J. Clinical pharmacokinetics and pharmacodynamics of the oral direct thrombin inhibitor dabigatran etexilate. Clin. Pharmacokinet. 2008, 47, 285–295. [Google Scholar] [CrossRef]
- Blech, S.; Ebner, T.; Ludwig-Schwellinger, E.; Stangier, J.; Roth, W. The metabolism and disposition of the oral direct thrombin inhibitor, dabigatran, in humans. Drug Metab. Dispos. Biol. Fate Chem. 2008, 36, 386–399. [Google Scholar] [CrossRef] [Green Version]
- Laizure, S.C.; Parker, R.B.; Herring, V.L.; Hu, Z.Y. Identification of carboxylesterase-dependent dabigatran etexilate hydrolysis. Drug Metab. Dispos. Biol. Fate Chem. 2014, 42, 201–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stangier, J.; Rathgen, K.; Stahle, H.; Gansser, D.; Roth, W. The pharmacokinetics, pharmacodynamics and tolerability of dabigatran etexilate, a new oral direct thrombin inhibitor, in healthy male subjects. Br. J. Clin. Pharmacol. 2007, 64, 292–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebner, T.; Wagner, K.; Wienen, W. Dabigatran acylglucuronide, the major human metabolite of dabigatran: In vitro formation, stability, and pharmacological activity. Drug Metab. Dispos. Biol. Fate Chem. 2010, 38, 1567–1575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baigent, C.; Keech, A.; Kearney, P.M.; Blackwell, L.; Buck, G.; Pollicino, C.; Kirby, A.; Sourjina, T.; Peto, R.; Collins, R.; et al. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005, 366, 1267–1278. [Google Scholar] [CrossRef]
- Steffel, J.; Collins, R.; Antz, M.; Cornu, P.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; Rowell, N.; et al. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Eur. Eur. Pacing Arrhythm. Card. Electrophysiol. J. Work. Groups Card. Pacing Arrhythm. Card. Cell. Electrophysiol. Eur. Soc. Cardiol. 2021, 23, 1612–1676. [Google Scholar] [CrossRef]
- Chang, S.H.; Chou, I.J.; Yeh, Y.H.; Chiou, M.J.; Wen, M.S.; Kuo, C.T.; See, L.C.; Kuo, C.F. Association Between Use of Non-Vitamin K Oral Anticoagulants With and Without Concurrent Medications and Risk of Major Bleeding in Nonvalvular Atrial Fibrillation. JAMA 2017, 318, 1250–1259. [Google Scholar] [CrossRef]
- Harskamp, R.E.; Himmelreich, J.C.L.; Wong, G.W.M.; Teichert, M. Prescription patterns of direct oral anticoagulants and concomitant use of interacting medications in the Netherlands. Neth. Heart J. Mon. J. Neth. Soc. Cardiol. Neth. Heart Found. 2021, 29, 451–459. [Google Scholar] [CrossRef]
- Douketis, J.D.; Melo, M.; Bell, C.M.; Mamdani, M.M. Does statin therapy decrease the risk for bleeding in patients who are receiving warfarin? Am. J. Med. 2007, 120, 369.e9–369.e14. [Google Scholar] [CrossRef]
- Schelleman, H.; Bilker, W.B.; Brensinger, C.M.; Wan, F.; Yang, Y.X.; Hennessy, S. Fibrate/Statin initiation in warfarin users and gastrointestinal bleeding risk. Am. J. Med. 2010, 123, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Antoniou, T.; Macdonald, E.M.; Yao, Z.; Hollands, S.; Gomes, T.; Tadrous, M.; Mamdani, M.M.; Juurlink, D.N.; Canadian Drug, S. Association between statin use and ischemic stroke or major hemorrhage in patients taking dabigatran for atrial fibrillation. CMAJ Can. Med. Assoc. J. = J. l’Association Med. Can. 2017, 189, E4–E10. [Google Scholar] [CrossRef] [Green Version]
- Ho, B.L.; Lin, Y.J.; Lin, S.F.; Chou, P.S.; Chen, C.F.; Lin, R.T.; Hu, H.H.; Chao, A.C. Statins and the risk of bleeding in patients taking dabigatran. Acta Neurol. Scand. 2019, 139, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Mauro, V.F. Clinical pharmacokinetics and practical applications of simvastatin. Clin. Pharmacokinet. 1993, 24, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Najib, N.M.; Idkaidek, N.; Adel, A.; Admour, I.; Astigarraga, R.E.; Nucci, G.D.; Alam, S.M.; Dham, R. Pharmacokinetics and bioequivalence evaluation of two simvastatin 40 mg tablets (Simvast and Zocor) in healthy human volunteers. Biopharm. Drug Dispos. 2003, 24, 183–189. [Google Scholar] [CrossRef]
- Schachter, M. Chemical, pharmacokinetic and pharmacodynamic properties of statins: An update. Fundam. Clin. Pharmacol. 2005, 19, 117–125. [Google Scholar] [CrossRef]
- Hartter, S.; Sennewald, R.; Nehmiz, G.; Reilly, P. Oral bioavailability of dabigatran etexilate (Pradaxa((R))) after co-medication with verapamil in healthy subjects. Br. J. Clin. Pharmacol. 2013, 75, 1053–1062. [Google Scholar] [CrossRef] [Green Version]
- Fukami, T.; Takahashi, S.; Nakagawa, N.; Maruichi, T.; Nakajima, M.; Yokoi, T. In vitro evaluation of inhibitory effects of antidiabetic and antihyperlipidemic drugs on human carboxylesterase activities. Drug Metab. Dispos. Biol. Fate Chem. 2010, 38, 2173–2178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Zhu, H.J.; Markowitz, J.S. Carboxylesterase 1-mediated drug-drug interactions between clopidogrel and simvastatin. Biol. Pharm. Bull. 2015, 38, 292–297. [Google Scholar] [CrossRef] [Green Version]
- Stangier, J.; Rathgen, K.; Stahle, H.; Reseski, K.; Kornicke, T.; Roth, W. Coadministration of dabigatran etexilate and atorvastatin: Assessment of potential impact on pharmacokinetics and pharmacodynamics. Am. J. Cardiovasc. Drugs Drugs Devices Other Interv. 2009, 9, 59–68. [Google Scholar] [CrossRef]
- Van Ryn, J.; Stangier, J.; Haertter, S.; Liesenfeld, K.H.; Wienen, W.; Feuring, M.; Clemens, A. Dabigatran etexilate--a novel, reversible, oral direct thrombin inhibitor: Interpretation of coagulation assays and reversal of anticoagulant activity. Thromb. Haemost. 2010, 103, 1116–1127. [Google Scholar] [CrossRef]
- Dager, W.E.; Gosselin, R.C.; Kitchen, S.; Dwyre, D. Dabigatran effects on the international normalized ratio, activated partial thromboplastin time, thrombin time, and fibrinogen: A multicenter, in vitro study. Ann. Pharmacother. 2012, 46, 1627–1636. [Google Scholar] [CrossRef]
- Undas, A.; Brummel-Ziedins, K.E.; Mann, K.G. Anticoagulant effects of statins and their clinical implications. Thromb. Haemost. 2014, 111, 392–400. [Google Scholar] [CrossRef]
- Bogman, K.; Peyer, A.K.; Torok, M.; Kusters, E.; Drewe, J. HMG-CoA reductase inhibitors and P-glycoprotein modulation. Br. J. Pharmacol. 2001, 132, 1183–1192. [Google Scholar] [CrossRef] [Green Version]
- Wang, E.; Casciano, C.N.; Clement, R.P.; Johnson, W.W. HMG-CoA reductase inhibitors (statins) characterized as direct inhibitors of P-glycoprotein. Pharm. Res. 2001, 18, 800–806. [Google Scholar] [CrossRef]
- Hochman, J.H.; Pudvah, N.; Qiu, J.; Yamazaki, M.; Tang, C.; Lin, J.H.; Prueksaritanont, T. Interactions of human P-glycoprotein with simvastatin, simvastatin acid, and atorvastatin. Pharm. Res. 2004, 21, 1686–1691. [Google Scholar] [CrossRef] [PubMed]
- Sakugawa, T.; Miura, M.; Hokama, N.; Suzuki, T.; Tateishi, T.; Uno, T. Enantioselective disposition of fexofenadine with the P-glycoprotein inhibitor verapamil. Br. J. Clin. Pharmacol. 2009, 67, 535–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prueksaritanont, T.; Subramanian, R.; Fang, X.; Ma, B.; Qiu, Y.; Lin, J.H.; Pearson, P.G.; Baillie, T.A. Glucuronidation of statins in animals and humans: A novel mechanism of statin lactonization. Drug Metab. Dispos. Biol. Fate Chem. 2002, 30, 505–512. [Google Scholar] [CrossRef] [Green Version]
- Iwuchukwu, O.F.; Feng, Q.; Wei, W.Q.; Jiang, L.; Jiang, M.; Xu, H.; Denny, J.C.; Wilke, R.A.; Krauss, R.M.; Roden, D.M.; et al. Genetic variation in the UGT1A locus is associated with simvastatin efficacy in a clinical practice setting. Pharmacogenomics 2014, 15, 1739–1747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stangier, J.; Stahle, H.; Rathgen, K.; Fuhr, R. Pharmacokinetics and pharmacodynamics of the direct oral thrombin inhibitor dabigatran in healthy elderly subjects. Clin. Pharmacokinet. 2008, 47, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Park, I.H.; Park, J.W.; Chung, H.; Kim, J.M.; Lee, S.; Kim, K.A.; Park, J.Y. Development and validation of LC-MS/MS method for simultaneous determination of dabigatran etexilate and its active metabolites in human plasma, and its application in a pharmacokinetic study. J. Pharm. Biomed. Anal. 2021, 203, 114220. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Noh, J.; Park, J.W.; Chung, H.; Kim, K.A.; Park, S.B.; Lee, J.S.; Park, J.Y. Dabigatran Acylglucuronide, the Major Metabolite of Dabigatran, Shows a Weaker Anticoagulant Effect than Dabigatran. Pharmaceutics 2022, 14, 257. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Dabigatran Alone | Dabigatran Co-Administered with Simvastatin | GMR (90% CI) | p-Value | |
|---|---|---|---|---|---|
| Dabigatran etexilate | AUCinf (h∙ng/mL) | 33.7 (26.0) | 36.4 (18.5) | 1.60 (0.89–2.88) | 0.3847 |
| AUClast (h∙ng/mL) | 26.1 (23.6) | 27.3 (16.4) | 1.47 (0.87–2.48) | 0.8242 | |
| CL/F (L/h) | 12,208.4 (16,447.7) | 5235.1 (2729.4) | - | ||
| Cmax (ng/mL) | 24.5 (19.2) | 25.1 (13.8) | 1.38 (0.81–2.35) | 0.9139 | |
| t1/2 (h) | 3.4 (5.8) | 6.4 (13.6) | - | ||
| MRT (h) | 1.9 (2.4) | 2.2 (1.8) | - | ||
| Tmax (h) | 1 (0.5–1.5) | 1 (0.5–2) | - | ||
| Dabigatran | AUCinf (h∙ng/mL) | 663.9 (377.5) | 740.2 (342.0) | 1.19 (0.71–2.00) | 0.6033 |
| AUClast (h∙ng/mL) | 617.1 (357.4) | 688.2 (318.9) | 1.21 (0.71–2.08) | 0.6079 | |
| CL/F (L/h) | 362.3 (331.8) | 275.8 (197.4) | - | ||
| Cmax (ng/mL) | 87.0 (51.4) | 98.6 (47.5) | 1.24 (0.72–2.12) | 0.5601 | |
| t1/2 (h) | 6.1 (0.9) | 6.2 (0.6) | - | ||
| MRT (h) | 7.1 (0.9) | 7.5 (0.7) | - | ||
| Tmax (h) | 2 (1–4) | 3 (1.5–4) | - | ||
| Dabigatran acylglucuronide | AUCinf (h∙ng/mL) | 1576.5 (1154.0) | 2376.8 (2096.8) | 1.56 (0.94–2.59) | 0.2903 |
| AUClast (h∙ng/mL) | 1480.1 (1090.5) | 2227.5 (1994.6) | 1.57 (0.93–2.66) | 0.3042 | |
| CL/F (L/h) | 176.8 (161.8) | 97.1 (56.1) | - | ||
| Cmax (ng/mL) | 266.8 (187.1) | 392.0 (290.2) | 1.63 (0.94–2.80) | 0.2885 | |
| t1/2 (h) | 6.4 (1.9) | 6.0 (1.8) | - | ||
| MRT (h) | 6.8 (0.9) | 7.1 (0.8) | - | ||
| Tmax (h) | 2 (1.5–4) | 2.5 (1–4) | - | ||
| AUClast ratio of dabigatran acylglucuronide to dabigatran | 3.03 (2.42) | 3.65 (2.54) | 1.30 (1.15–1.46) | 0.0025 | |
| Dabigatran Alone | Dabigatran with Simvastatin | p-Value | ||
|---|---|---|---|---|
| Thrombin Generation Assay | Cmax (nM) | 241.3 (43.0) | 233.6 (46.7) | 0.5629 |
| AUC (nM∙min) | 3937.1 (537.4) | 4073.1 (642.2) | 0.3383 | |
| lag time (min) | 3.5 (0.5) | 3.5 (0.5) | 0.3388 | |
| Tmax (min) | 7.6 (1.2) | 7.3 (0.8) | 0.2072 | |
| Coagulation Assay | aPTT (s) | 40.6 (3.3) | 40.4 (3.3) | 0.6502 |
| PT (s) | 13.8 (0.4) | 13.7 (0.6) | 0.2068 | |
| PT (INR) | 1.1 (0.0) | 1.0 (0.1) | 0.1718 | |
| dPT (s) | 43.2 (1.7) | 43.2 (1.8) | 0.9726 | |
| TT (s) | 16.5 (1.2) | 16.2 (0.9) | 0.4361 | |
| Fibrinogen (mg/dL) | 250.3 (63.9) | 259.3 (39.4) | 0.5432 |
| Parameter | Dabigatran Alone | Dabigatran with Simvastatin | p-Value | ||
|---|---|---|---|---|---|
| Thrombin Generation | Cmax | AUEC (nM∙h) | 5755.0 (1129.2) | 5734.0 (993.9) | 0.9369 |
| Rmax (nM) | 180.2 (48.8) | 177.8 (35.8) | 0.8684 | ||
| AUC | AUEC (nM∙min∙h) | 84,994.8 (14,977.1) | 79,286.4 (10,676.3) | 0.0746 | |
| Rmax (nM∙min) | 2423.6 (734.9) | 2231.7 (326.0) | 0.2944 | ||
| Lag time | AUEC (min∙h) | 131.7 (20.8) | 128.5 (20.1) | 0.6835 | |
| Rmax (min) | 7.8 (1.7) | 8.0 (1.5) | 0.7206 | ||
| Tmax | AUEC (min∙h) | 214.8 (21.9) | 207.0 (22.0) | 0.2667 | |
| Rmax (min) | 11.0 (1.6) | 11.3 (1.7) | 0.6767 | ||
| Coagulation assay | aPTT | AUEC (s∙h) | 1203.1 (153.1) | 1235.7 (131.7) | 0.4873 |
| Rmax (s) | 69.5 (13.8) | 71.7 (12.2) | 0.6408 | ||
| PT (sec) | AUEC (s∙h) | 344.9 (14.3) | 353.8 (12.3) | 0.0331 | |
| Rmax (s) | 16.6 (1.4) | 17.2 (1.4) | 0.3048 | ||
| PT (INR) | AUEC | 26.9 (1.4) | 27.7 (1.2) | 0.0474 | |
| Rmax | 1.3 (0.1) | 1.4 (0.1) | 0.3038 | ||
| dPT (1:256) | AUEC (s∙h) | 1404.8 (184.7) | 1482.9 (144.9) | 0.2977 | |
| Rmax (s) | 87.5 (19.2) | 92.5 (15.3) | 0.5068 | ||
| TT | AUEC (s∙h) | 1690.1 (535.9) | 1976.2 (643.8) | 0.3393 | |
| Rmax (s) | 169.2 (74.0) | 180.7 (50.4) | 0.6841 | ||
| Fibrinogen | AUEC (h∙mg/dL) | 6249.8 (1133.1) | 6040.9 (758.3) | 0.4101 | |
| Rmax (mg/dL) | 288.0 (55.9) | 309.3 (96.0) | 0.4907 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, H.; Kim, J.-M.; Park, J.-W.; Noh, J.; Kim, K.-A.; Park, J.-Y. Effects of Simvastatin on Pharmacokinetics and Anticoagulant Effects of Dabigatran in Healthy Subjects. Pharmaceuticals 2023, 16, 364. https://doi.org/10.3390/ph16030364
Chung H, Kim J-M, Park J-W, Noh J, Kim K-A, Park J-Y. Effects of Simvastatin on Pharmacokinetics and Anticoagulant Effects of Dabigatran in Healthy Subjects. Pharmaceuticals. 2023; 16(3):364. https://doi.org/10.3390/ph16030364
Chicago/Turabian StyleChung, Hyewon, Jong-Min Kim, Jin-Woo Park, Jihyeon Noh, Kyoung-Ah Kim, and Ji-Young Park. 2023. "Effects of Simvastatin on Pharmacokinetics and Anticoagulant Effects of Dabigatran in Healthy Subjects" Pharmaceuticals 16, no. 3: 364. https://doi.org/10.3390/ph16030364