
P2Y12 Inhibitor Monotherapy versus Conventional Dual Antiplatelet Therapy in Patients with Acute Coronary Syndrome after Percutaneous Coronary Intervention: A Meta-Analysis
 , , and
, , and
Abstract
:1. Introduction
2. Results
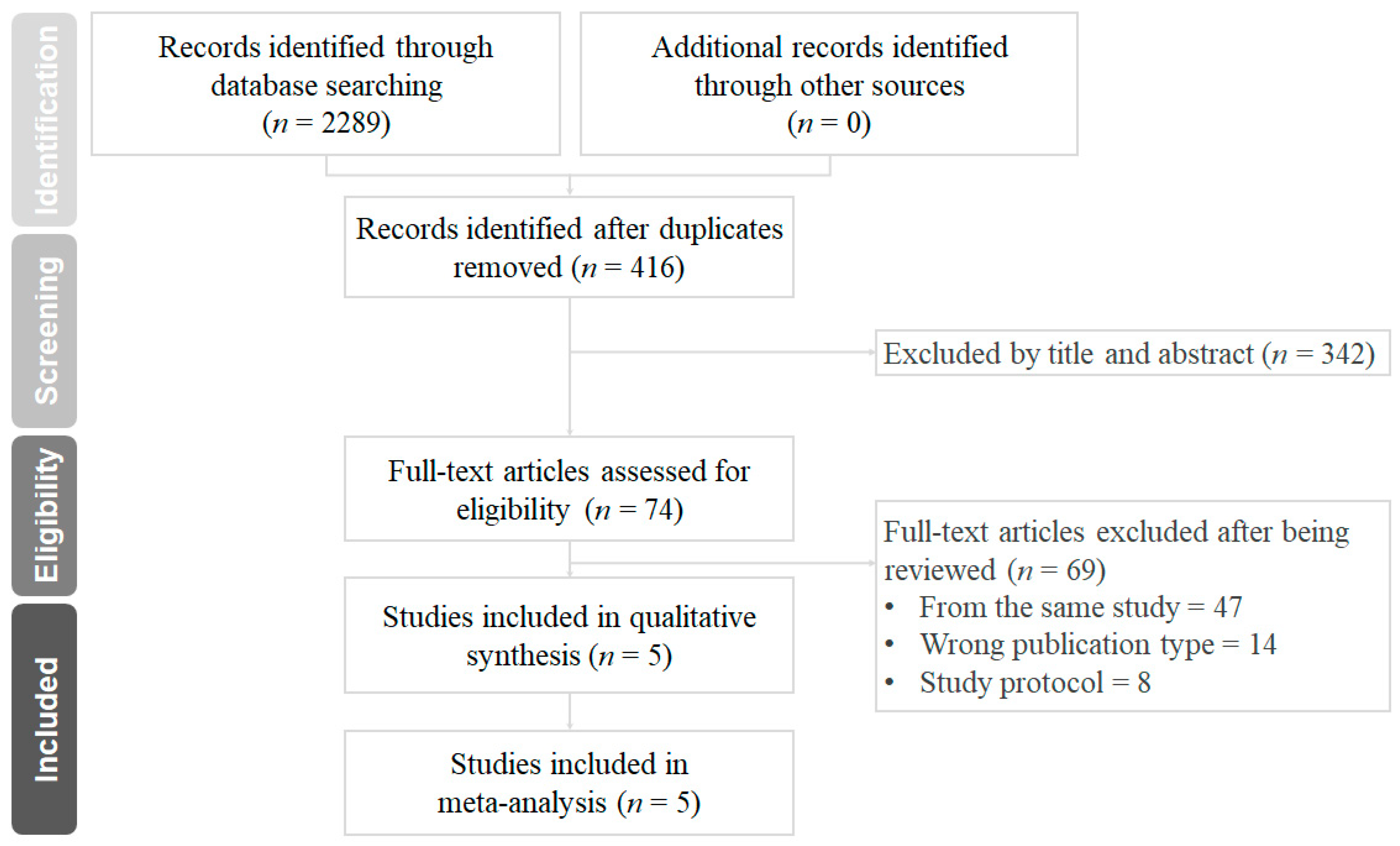
2.1. Search Results and Characteristics of Included Trials
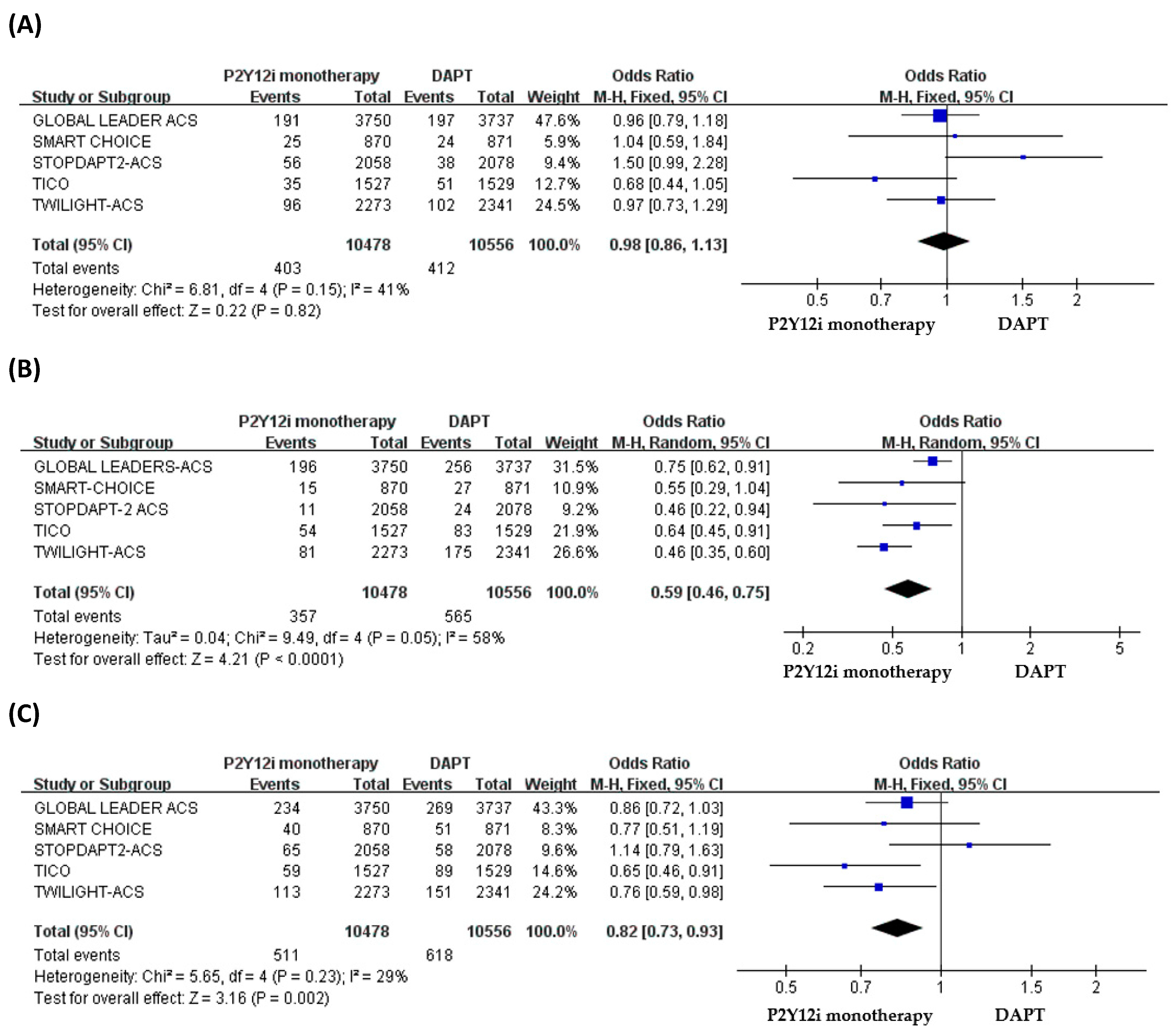
2.2. The Primary and Secondary Outcomes
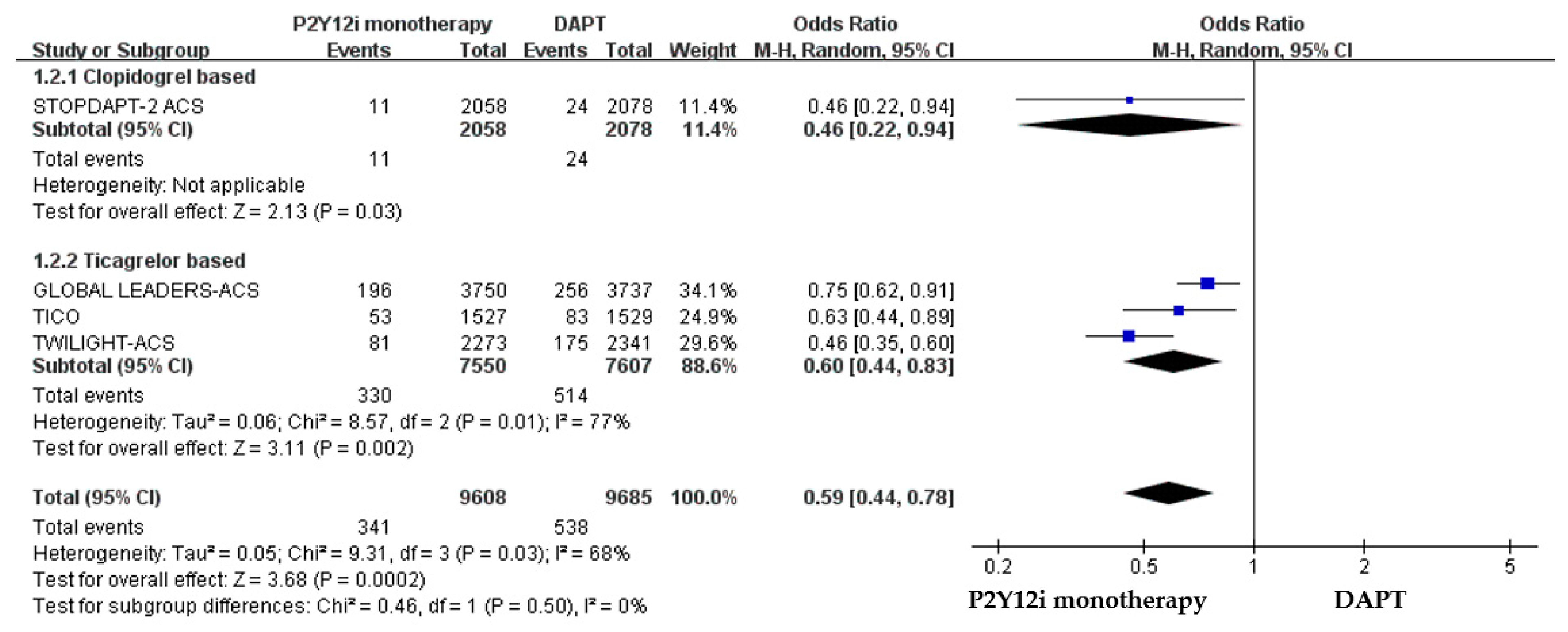
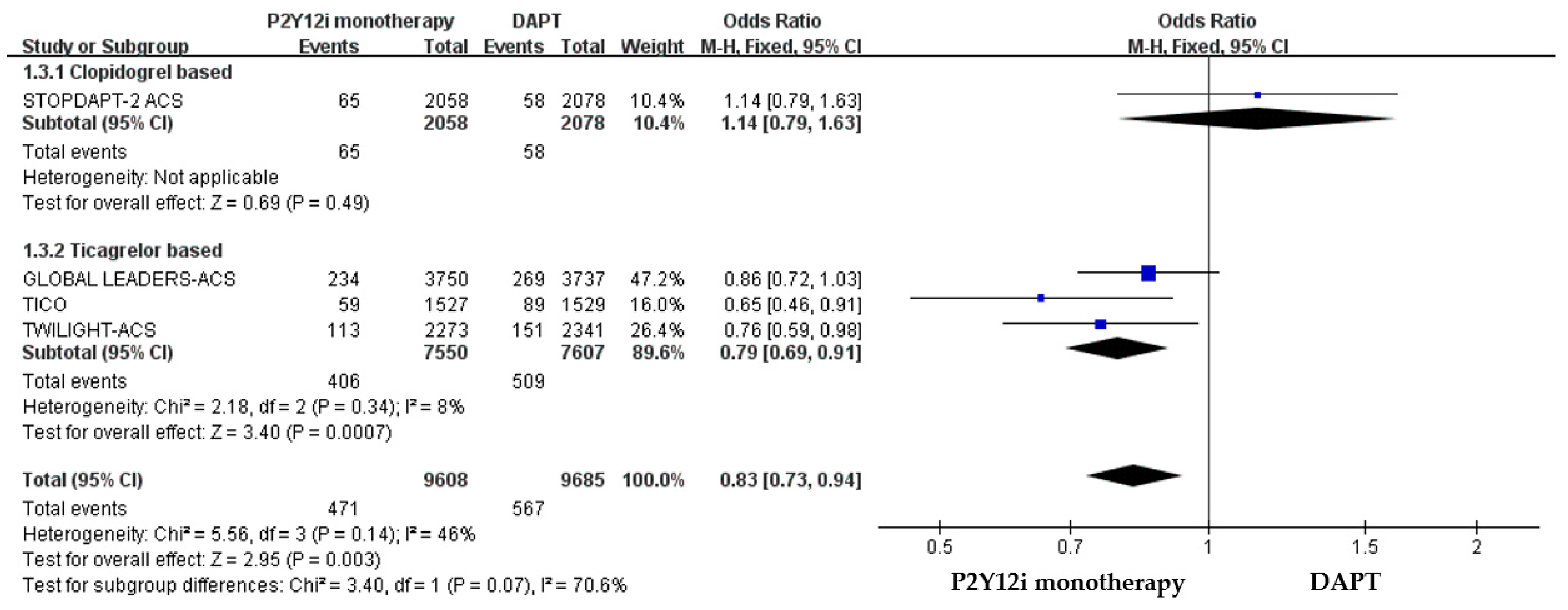
2.3. Subgroup Analysis of Different P2Y12 Inhibitors
2.4. Extrapolatory Analysis of P2Y12 Inhibitor Monotherapy in Non-ACS Patients as Compared with ACS Patients
2.5. Extraploartory Analysis of P2Y12 Inhibitor Monotherapy in STE-ACS Patients as Compared with NSTE-ACS Patients
2.6. Quality Assessment and Publication Bias
3. Materials and Methods
3.1. Data Sources and Searching
3.2. Study Selection
3.3. Data Extraction and Clinical Outcomes
3.4. Assessment of Risk of Bias
3.5. Data Synthesis and Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yusuf, S.; Zhao, F.; Mehta, S.R.; Chrolavicius, S.; Tognoni, G.; Fox, K.K. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N. Engl. J. Med. 2001, 345, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Camenzind, E.; Steg, P.G.; Wijns, W. Stent thrombosis late after implantation of first-generation drug-eluting stents: A cause for concern. Circulation 2007, 115, 1440–1455. [Google Scholar] [CrossRef]
- Généreux, P.; Giustino, G.; Witzenbichler, B.; Weisz, G.; Stuckey, T.D.; Rinaldi, M.J.; Neumann, F.J.; Metzger, D.C.; Henry, T.D.; Cox, D.A.; et al. Incidence, Predictors, and Impact of Post-Discharge Bleeding After Percutaneous Coronary Intervention. J. Am. Coll. Cardiol. 2015, 66, 1036–1045. [Google Scholar] [CrossRef] [PubMed]
- Palmerini, T.; Bacchi Reggiani, L.; Della Riva, D.; Romanello, M.; Feres, F.; Abizaid, A.; Gilard, M.; Morice, M.C.; Valgimigli, M.; Hong, M.K.; et al. Bleeding-Related Deaths in Relation to the Duration of Dual-Antiplatelet Therapy After Coronary Stenting. J. Am. Coll. Cardiol. 2017, 69, 2011–2022. [Google Scholar] [CrossRef] [PubMed]
- Gawaz, M.; Neumann, F.J.; Ott, I.; Schiessler, A.; Schömig, A. Platelet function in acute myocardial infarction treated with direct angioplasty. Circulation 1996, 93, 229–237. [Google Scholar] [CrossRef]
- Giustino, G.; Mehran, R.; Dangas, G.D.; Kirtane, A.J.; Redfors, B.; Généreux, P.; Brener, S.J.; Prats, J.; Pocock, S.J.; Deliargyris, E.N.; et al. Characterization of the Average Daily Ischemic and Bleeding Risk After Primary PCI for STEMI. J. Am. Coll. Cardiol. 2017, 70, 1846–1857. [Google Scholar] [CrossRef]
- Scalone, G.; Coviello, I.; Barone, L.; Battipaglia, I.; Aurigemma, C.; Careri, G.; Pinnacchio, G.; Tarzia, P.; Lanza, G.A.; Crea, F. Evidence of increased platelet reactivity in the first six months after acute ST segment elevation myocardial infarction. Thromb. Res. 2011, 128, 174–178. [Google Scholar] [CrossRef]
- Hahn, J.Y.; Song, Y.B.; Oh, J.H.; Cho, D.K.; Lee, J.B.; Doh, J.H.; Kim, S.H.; Jeong, J.O.; Bae, J.H.; Kim, B.O.; et al. 6-month versus 12-month or longer dual antiplatelet therapy after percutaneous coronary intervention in patients with acute coronary syndrome (SMART-DATE): A randomised, open-label, non-inferiority trial. Lancet 2018, 391, 1274–1284. [Google Scholar] [CrossRef]
- Palmerini, T.; Della Riva, D.; Benedetto, U.; Bacchi Reggiani, L.; Feres, F.; Abizaid, A.; Gilard, M.; Morice, M.C.; Valgimigli, M.; Hong, M.K.; et al. Three, six, or twelve months of dual antiplatelet therapy after DES implantation in patients with or without acute coronary syndromes: An individual patient data pairwise and network meta-analysis of six randomized trials and 11 473 patients. Eur. Heart J. 2017, 38, 1034–1043. [Google Scholar] [CrossRef]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2018, 39, 213–260. [Google Scholar] [CrossRef]
- Bittl, J.A.; Baber, U.; Bradley, S.M.; Wijeysundera, D.N. Duration of Dual Antiplatelet Therapy: A Systematic Review for the 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2016, 134, e156–e178. [Google Scholar] [CrossRef]
- Gimbel, M.E.; Ten Berg, J.M. Safety considerations with the use of platelet inhibitors for elderly patients with non-ST-elevation acute coronary syndrome. Expert Opin. Drug Saf. 2021, 20, 1545–1552. [Google Scholar] [CrossRef]
- von Kügelgen, I. Structure, Pharmacology and Roles in Physiology of the P2Y(12) Receptor. Adv. Exp. Med. Biol. 2017, 1051, 123–138. [Google Scholar] [CrossRef]
- Watanabe, H.; Domei, T.; Morimoto, T.; Natsuaki, M.; Shiomi, H.; Toyota, T.; Ohya, M.; Suwa, S.; Takagi, K.; Nanasato, M.; et al. Effect of 1-Month Dual Antiplatelet Therapy Followed by Clopidogrel vs 12-Month Dual Antiplatelet Therapy on Cardiovascular and Bleeding Events in Patients Receiving PCI: The STOPDAPT-2 Randomized Clinical Trial. JAMA 2019, 321, 2414–2427. [Google Scholar] [CrossRef]
- Hahn, J.Y.; Song, Y.B.; Oh, J.H.; Chun, W.J.; Park, Y.H.; Jang, W.J.; Im, E.S.; Jeong, J.O.; Cho, B.R.; Oh, S.K.; et al. Effect of P2Y12 Inhibitor Monotherapy vs Dual Antiplatelet Therapy on Cardiovascular Events in Patients Undergoing Percutaneous Coronary Intervention: The SMART-CHOICE Randomized Clinical Trial. JAMA 2019, 321, 2428–2437. [Google Scholar] [CrossRef]
- Mehran, R.; Baber, U.; Sharma, S.K.; Cohen, D.J.; Angiolillo, D.J.; Briguori, C.; Cha, J.Y.; Collier, T.; Dangas, G.; Dudek, D.; et al. Ticagrelor with or without Aspirin in High-Risk Patients after PCI. N. Engl. J. Med. 2019, 381, 2032–2042. [Google Scholar] [CrossRef]
- Vranckx, P.; Valgimigli, M.; Jüni, P.; Hamm, C.; Steg, P.G.; Heg, D.; van Es, G.A.; McFadden, E.P.; Onuma, Y.; van Meijeren, C.; et al. Ticagrelor plus aspirin for 1 month, followed by ticagrelor monotherapy for 23 months vs aspirin plus clopidogrel or ticagrelor for 12 months, followed by aspirin monotherapy for 12 months after implantation of a drug-eluting stent: A multicentre, open-label, randomised superiority trial. Lancet 2018, 392, 940–949. [Google Scholar] [CrossRef]
- Feng, W.H.; Hsieh, I.C.; Li, Y.H. P2Y12 Inhibitor Monotherapy after Percutaneous Coronary Intervention: Is It Safe to Abandon Aspirin? Acta Cardiol. Sin. 2021, 37, 1–8. [Google Scholar] [CrossRef]
- Serebruany, V.L.; Steinhubl, S.R.; Berger, P.B.; Malinin, A.I.; Bhatt, D.L.; Topol, E.J. Variability in platelet responsiveness to clopidogrel among 544 individuals. J. Am. Coll. Cardiol. 2005, 45, 246–251. [Google Scholar] [CrossRef]
- Roden, D.M.; Shuldiner, A.R. Responding to the clopidogrel warning by the US food and drug administration: Real life is complicated. Circulation 2010, 122, 445–448. [Google Scholar] [CrossRef] [Green Version]
- Tomaniak, M.; Chichareon, P.; Onuma, Y.; Deliargyris, E.N.; Takahashi, K.; Kogame, N.; Modolo, R.; Chang, C.C.; Rademaker-Havinga, T.; Storey, R.F.; et al. Benefit and Risks of Aspirin in Addition to Ticagrelor in Acute Coronary Syndromes: A Post Hoc Analysis of the Randomized GLOBAL LEADERS Trial. JAMA Cardiol. 2019, 4, 1092–1101. [Google Scholar] [CrossRef] [PubMed]
- Baber, U.; Dangas, G.; Angiolillo, D.J.; Cohen, D.J.; Sharma, S.K.; Nicolas, J.; Briguori, C.; Cha, J.Y.; Collier, T.; Dudek, D.; et al. Ticagrelor alone vs. ticagrelor plus aspirin following percutaneous coronary intervention in patients with non-ST-segment elevation acute coronary syndromes: TWILIGHT-ACS. Eur. Heart J. 2020, 41, 3533–3545. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.K.; Hong, S.J.; Cho, Y.H.; Yun, K.H.; Kim, Y.H.; Suh, Y.; Cho, J.Y.; Her, A.Y.; Cho, S.; Jeon, D.W.; et al. Effect of Ticagrelor Monotherapy vs Ticagrelor With Aspirin on Major Bleeding and Cardiovascular Events in Patients With Acute Coronary Syndrome: The TICO Randomized Clinical Trial. JAMA 2020, 323, 2407–2416. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, H.; Morimoto, T.; Natsuaki, M.; Yamamoto, K.; Obayashi, Y.; Ogita, M.; Suwa, S.; Isawa, T.; Domei, T.; Yamaji, K.; et al. Comparison of Clopidogrel Monotherapy After 1 to 2 Months of Dual Antiplatelet Therapy With 12 Months of Dual Antiplatelet Therapy in Patients With Acute Coronary Syndrome: The STOPDAPT-2 ACS Randomized Clinical Trial. JAMA Cardiol. 2022, 7, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Vranckx, P.; Valgimigli, M.; Odutayo, A.; Serruys, P.W.; Hamm, C.; Steg, P.G.; Heg, D.; Mc Fadden, E.P.; Onuma, Y.; Benit, E.; et al. Efficacy and Safety of Ticagrelor Monotherapy by Clinical Presentation: Pre-Specified Analysis of the GLOBAL LEADERS Trial. J. Am. Heart Assoc. 2021, 10, e015560. [Google Scholar] [CrossRef]
- Obayashi, Y.; Watanabe, H.; Morimoto, T.; Yamamoto, K.; Natsuaki, M.; Domei, T.; Yamaji, K.; Suwa, S.; Isawa, T.; Watanabe, H.; et al. Clopidogrel Monotherapy After 1-Month Dual Antiplatelet Therapy in Percutaneous Coronary Intervention: From the STOPDAPT-2 Total Cohort. Circ. Cardiovasc. Interv. 2022, 15, e012004. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger, C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2016, 68, 1082–1115. [Google Scholar] [CrossRef]
- Capodanno, D.; Mehran, R.; Valgimigli, M.; Baber, U.; Windecker, S.; Vranckx, P.; Dangas, G.; Rollini, F.; Kimura, T.; Collet, J.P.; et al. Aspirin-free strategies in cardiovascular disease and cardioembolic stroke prevention. Nat. Rev. Cardiol. 2018, 15, 480–496. [Google Scholar] [CrossRef]
- Cadroy, Y.; Bossavy, J.P.; Thalamas, C.; Sagnard, L.; Sakariassen, K.; Boneu, B. Early potent antithrombotic effect with combined aspirin and a loading dose of clopidogrel on experimental arterial thrombogenesis in humans. Circulation 2000, 101, 2823–2828. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, P.C.; Leadbeater, P.D.; Chan, M.V.; Kirkby, N.S.; Jakubowski, J.A.; Mitchell, J.A.; Warner, T.D. In the presence of strong P2Y12 receptor blockade, aspirin provides little additional inhibition of platelet aggregation. J. Thromb. Haemost. 2011, 9, 552–561. [Google Scholar] [CrossRef]
- Baos, S.; Underwood, W.; Culliford, L.; Reeves, B.C.; Rogers, C.A.; Bowles, R.; Johnson, T.; Baumbach, A.; Mumford, A. Platelet inhibition during ticagrelor monotherapy versus ticagrelor plus aspirin in patients with coronary artery disease (TEMPLATE study): Study protocol for a randomised controlled trial. Trials 2017, 18, 529. [Google Scholar] [CrossRef]
- Bhavaraju, K.; Georgakis, A.; Jin, J.; Gartner, T.K.; Tomiyama, Y.; Nurden, A.; Nurden, P.; Kunapuli, S.P. Antagonism of P2Y12 reduces physiological thromboxane levels. Platelets 2010, 21, 604–609. [Google Scholar] [CrossRef]
- Armstrong, P.C.; Dhanji, A.R.; Tucker, A.T.; Mitchell, J.A.; Warner, T.D. Reduction of platelet thromboxane A2 production ex vivo and in vivo by clopidogrel therapy. J. Thromb. Haemost. 2010, 8, 613–615. [Google Scholar] [CrossRef]
- Ebrahimi, P.; Farhadi, Z.; Behzadifar, M.; Shabaninejad, H.; Abolghasem Gorji, H.; Taheri Mirghaed, M.; Salemi, M.; Amin, K.; Mohammadibakhsh, R.; Bragazzi, N.L.; et al. Prevalence rate of laboratory defined aspirin resistance in cardiovascular disease patients: A systematic review and meta-analysis. Casp. J. Intern. Med. 2020, 11, 124–134. [Google Scholar] [CrossRef]
- Krasopoulos, G.; Brister, S.J.; Beattie, W.S.; Buchanan, M.R. Aspirin “resistance” and risk of cardiovascular morbidity: Systematic review and meta-analysis. BMJ 2008, 336, 195–198. [Google Scholar] [CrossRef]
- Ho, A.C.; Egolum, U.; Parker, S.; Dimmel, J.; Hawkins, A.; Ling, H. P2Y12 Inhibitor Monotherapy After a Short Dual Antiplatelet Therapy Versus Standard-Term Dual Antiplatelet Therapy in Patients Undergoing Percutaneous Coronary Intervention: A Contemporary Meta-Analysis. Clin. Drug Investig. 2020, 40, 799–808. [Google Scholar] [CrossRef]
- Valgimigli, M.; Gragnano, F.; Branca, M.; Franzone, A.; Baber, U.; Jang, Y.; Kimura, T.; Hahn, J.Y.; Zhao, Q.; Windecker, S.; et al. P2Y12 inhibitor monotherapy or dual antiplatelet therapy after coronary revascularisation: Individual patient level meta-analysis of randomised controlled trials. BMJ 2021, 373, n1332. [Google Scholar] [CrossRef]
- Giacoppo, D.; Matsuda, Y.; Fovino, L.N.; D’Amico, G.; Gargiulo, G.; Byrne, R.A.; Capodanno, D.; Valgimigli, M.; Mehran, R.; Tarantini, G. Short dual antiplatelet therapy followed by P2Y12 inhibitor monotherapy vs. prolonged dual antiplatelet therapy after percutaneous coronary intervention with second-generation drug-eluting stents: A systematic review and meta-analysis of randomized clinical trials. Eur. Heart J. 2021, 42, 308–319. [Google Scholar] [CrossRef]
- Nicolas, J.; Dangas, G.; Chiarito, M.; Pivato, C.A.; Spirit, A.; Cao, D.; Giustino, G.; Beerkens, F.; Camaj, A.; Vogel, B.; et al. Efficacy and Safety of P2Y12 Inhibitor Monotherapy After Complex PCI: A Collaborative Systematic Review and Meta-Analysis. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 1, pvac071. [Google Scholar] [CrossRef]
- Capodanno, D.; Angiolillo, D.J. Timing, Selection, Modulation, and Duration of P2Y12 Inhibitors for Patients With Acute Coronary Syndromes Undergoing PCI. JACC Cardiovasc. Interv. 2023, 16, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Wallentin, L.; Varenhorst, C.; James, S.; Erlinge, D.; Braun, O.O.; Jakubowski, J.A.; Sugidachi, A.; Winters, K.J.; Siegbahn, A. Prasugrel achieves greater and faster P2Y12receptor-mediated platelet inhibition than clopidogrel due to more efficient generation of its active metabolite in aspirin-treated patients with coronary artery disease. Eur. Heart J. 2008, 29, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [PubMed]
- Hamana, T.; Sawada, T.; Fujimoto, W.; Osue, T.; Tsukiyama, Y.; Uzu, K.; Takaya, T.; Yasaka, Y.; Kawai, H. Comparison of the 9-Month Intrastent Condition and 30-Month Clinical Outcomes After Resolute Zotarolimus-Eluting Stent Implantation Between Standard-Duration and 1-Month Dual Antiplatelet Therapy Followed by Prasugrel Monotherapy. Circ. Rep. 2020, 3, 55–65. [Google Scholar] [CrossRef]
- Nakamura, M.; Morino, Y.; Kakuta, T.; Hata, Y.; Takamisawa, I.; Tanabe, K.; Anzai, H.; Takahashi, A.; Kadota, K.; Suzuki, H.; et al. Monotherapy With Prasugrel After Dual-Antiplatelet Therapy for Japanese Percutaneous Coronary Intervention Patients With High Bleeding Risk—A Prospective Cohort Study (PENDULUM mono Study). Circ. J. Off. J. Jpn. Circ. Soc. 2020, 85, 27–36. [Google Scholar] [CrossRef]
- Nakamura, M.; Kadota, K.; Nakao, K.; Nakagawa, Y.; Shite, J.; Yokoi, H.; Kozuma, K.; Tanabe, K.; Akasaka, T.; Shinke, T.; et al. Single Antiplatelet Therapy With Prasugrel vs. Dual Antiplatelet Therapy in Japanese Percutaneous Coronary Intervention Patients With High Bleeding Risk. Circ. J. Off. J. Jpn. Circ. Soc. 2021, 85, 785–793. [Google Scholar] [CrossRef]
- Chen, P.W.; Feng, W.H.; Ho, M.Y.; Su, C.H.; Huang, S.W.; Cheng, C.W.; Yeh, H.I.; Chen, C.P.; Huang, W.C.; Fang, C.C.; et al. P2Y12 Inhibitor Monotherapy with Clopidogrel Versus Ticagrelor in Patients with Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention. J. Clin. Med. 2020, 9, 1657. [Google Scholar] [CrossRef]
- Tourdot, B.E.; Conaway, S.; Niisuke, K.; Edelstein, L.C.; Bray, P.F.; Holinstat, M. Mechanism of race-dependent platelet activation through the protease-activated receptor-4 and Gq signaling axis. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2644–2650. [Google Scholar] [CrossRef]
- Tamargo, J.; Kaski, J.C.; Kimura, T.; Barton, J.C.; Yamamoto, K.; Komiyama, M.; Drexel, H.; Lewis, B.S.; Agewall, S.; Hasegawa, K. Racial and ethnic differences in pharmacotherapy to prevent coronary artery disease and thrombotic events. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 738–751. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Trials | Global LEADERS ACS | Global LEADERS ACS | SMART- CHOICE | SMART- CHOICE | TWILIGHT ACS | TWILIGHT ACS | TICO | TICO | STOPDAPT-2 ACS | STOPDAPT-2 ACS |
|---|---|---|---|---|---|---|---|---|---|---|
| Year | 2018 | 2018 | 2019 | 2019 | 2019 | 2019 | 2020 | 2020 | 2022 | 2022 |
| Arm | Tica mono | DAPT | P2Y12i mono | DAPT | Tica mono | DAPT | Tica mono | DAPT | Clop mono | DAPT |
| DAPT months | 1 | 12 | 3 | 12 | 3 | 12 | 3 | 12 | 1 | 12 |
| Patients number | 3750 | 3737 | 870 | 871 | 2273 | 2341 | 1527 | 1529 | 2078 | 2091 |
| Age (mean) | 64.5 | 64.6 | 64.4 | 64.4 | 64.2 | 64.2 | 61 | 61 | 67.0 | 66.6 |
| Male | 2880 (76.8) | 2883 (77.1) | 629 (72.3) | N/A | 1693 (74.5) | 1760 (75.2) | 1204 (78.8) | 1224 (80.0) | 1631 (79.3) | 1649 (79.4) |
| Prior MI | 685 (18.3) | 695 (18.6) | 34 (3.9) | N/A | 578 (25.4) | 589 (25.2) | 64 (4.2) | 49 (3.2) | 135 (6.6) | 109 (5.3) |
| DM | 809 (21.6) | 795 (21.3) | 318 (36.6) | N/A | 810 (35.6) | 804 (34.3) | 418 (27.4) | 417 (27.2) | 608 (29.5) | 621 (29.9) |
| STEMI | 1062 (28.3) | 1030 (27.6) | 164 (18.9) | 150 (17.2) | Excluded | Excluded | 546 (35.7) | 557 (36.4) | 1179 (74.7) | 1145 (72.8) |
| NSTEMI | 1684 (44.9) | 1689 (45.2) | 239 (27.4) | 230 (26.4) | 2273 (100) | 2341 (100) | 539 (35.3) | 488 (31.9) | 399 (25.3) | 427 (27.2) |
| Ischemic outcomes | ||||||||||
| MACCE | 191 (5.1) | 197 (5.3) | 25 (3.0) | 24 (2.9) | 96 (4.3) | 102 (4.4) | 35 (2.3) | 51 (3.4) | 56 (2.7) | 38 (1.9) |
| All-cause death | 59 (1.6) | 75 (2.0) | 12 (1.4) | N/A | 22 (1.0) | 34 (1.5) | 16 (1.1) | 23 (1.5) | 28 (1.4) | 19 (0.9) |
| MI | 96 (2.6) | 88 (2.4) | 8 (0.9) | N/A | 70 (3.1) | 72 (3.1) | 6 (0.4) | 11 (0.7) | 32 (1.6) | 17 (0.9) |
| Stroke | 28 (0.8) | 26 (0.7) | 6 (0.7) | N/A | 11 (0.5) | 6 (0.3) | 8 (0.5) | 11 (0.7) | 15 (0.7) | 11 (0.5) |
| Stent thrombosis | 25 (0.7) | 23 (0.6) | N/A | N/A | 8 (0.4) | 14 (0.6) | 6 (0.4) | 4 (0.3) | 10 (0.5) | 4 (0.2) |
| Bleeding outcomes | ||||||||||
| Major or minor bleeding | 196 (5.2) | 256 (6.9) | 15 (1.8) | 27 (3.2) | 81 (3.6) | 175 (7.6) | 53 (3.6) | 83 (5.5) | 11 (0.5) | 24 (1.2) |
| Major bleeding | 57 (1.5) | 88 (2.4) | N/A | N/A | 17 (0.8) | 49 (2.1) | 25 (1.7) | 45 (3.0) | 7 (0.3) | 13 (0.6) |
| NACE | 234 (6.2) | 269 (7.2) | 40 (4.6) | 51 (5.9) | 113 (5.0) | 151 (6.5) | 59 (3.9) | 89 (5.9) | 65 (3.2) | 58 (2.8) |
| P2Y12i Monotherapy | DAPT | OR (95% CI) | |
|---|---|---|---|
| GLOBAL LEADERS-ACS [21] (n = 7487) | |||
| MACCE | 191 (5.1) | 197 (5.3) | 0.96 (0.77–1.18) |
| Major or minor bleeding | 196 (5.2) | 256 (6.9) | 0.84 (0.71–1.00) |
| NACE | 234 (6.2) | 269 (7.2) | 0.87 (0.76–1.01) |
| SMART-CHOICE [15] (n = 1741) | |||
| MACCE | 25 (3.0) | 24 (2.9) | 1.06 (0.61–1.85) |
| Major or minor bleeding | 15 (1.8) | 27 (3.2) | 0.56 (0.30–1.05) |
| NACE | 40 (4.6) | 51 (5.9) | 0.77 (0.51–1.19) |
| TWILIGHT-ACS [22] (n = 4614) | |||
| MACCE | 96 (4.3) | 102 (4.4) | 0.97 (0.74–1.28) |
| Major or minor bleeding | 81 (3.6) | 175 (7.6) | 0.47 (0.36–0.61) |
| NACE | 113 (5.0) | 151 (6.5) | 0.76 (0.59–0.98) |
| TICO [23] (n = 3056) | |||
| MACCE | 35 (2.3) | 51 (3.4) | 0.69 (0.45–1.06) |
| Major or minor Bleeding | 53 (3.6) | 83 (5.5) | 0.64 (0.45–0.90) |
| NACE | 59 (3.9) | 89 (5.9) | 0.66 (0.48–0.92) |
| STOPDAPT-2 ACS [24] (n = 4136) | |||
| MACCE | 56 (2.7) | 38 (1.9) | 1.50 (0.99–2.26) |
| Major or minor Bleeding | 11 (0.5) | 24 (1.2) | 0.46 (0.23–0.94) |
| NACE | 65 (3.2) | 58 (2.8) | 1.14 (0.80–1.62) |
| ACS | Non-ACS | |||||
|---|---|---|---|---|---|---|
| P2Y12i Monotherapy | DAPT | OR (95% CI) | P2Y12i Monotherapy | DAPT | OR (95% CI) | |
| GLOBAL LEADERS (n) | 3750 | 3737 | 4230 | 4251 | ||
| MACCE | 191 (5.1) | 197 (5.3) | 0.96 (0.77–1.18) | 148 (3.5) | 141 (3.3) | 1.06 (0.84–1.34) |
| Major bleeding | 57 (1.5) | 88 (2.3) | 0.64 (0.46–0.90) | 60 (1.4) | 48 (1.1) | 1.26 (0.86–1.85) |
| SMART-CHOICE (n) | 870 | 871 | 625 | 625 | ||
| MACCE | 25 (3.0) | 24 (2.9) | 1.06 (0.61–1.85) | 17 (2.8) | 12 (2.0) | 1.43 (0.68–3.00) |
| Major or minor bleeding | 15 (1.8) | 27 (3.2) | 0.56 (0.30–1.05) | 13 (2.2) | 22 (3.6) | 0.59 (0.30–1.18) |
| TWILIGHT (n) | 2273 | 2341 | 1281 | 1222 | ||
| MACCE | 96 (4.3) | 102 (4.4) | 0.97 (0.74–1.28) | 39 (3.1) | 39 (3.2) | 0.96 (0.61–1.49) |
| Major or minor bleeding | 81 (3.6) | 175 (7.6) | 0.47 (0.36–0.61) | 60 (4.8) | 75 (6.2) | 0.76 (0.54–1.06) |
| STOPDAPT-2 (n) | 2058 | 2078 | 935 | 926 | ||
| MACCE | 56 (2.7) | 38 (1.9) | 1.50 (0.99–2.26) | 15 (1.6) | 20 (2.2) | 0.74 (0.38–1.45) |
| Major or minor Bleeding | 11 (0.5) | 24 (1.2) | 0.46 (0.23–0.94) | 4 (0.4) | 15 (1.6) | 0.26 (0.09–0.79) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feng, W.-H.; Chang, Y.-C.; Lin, Y.-H.; Chen, H.-L.; Chen, C.-Y.; Lin, T.-H.; Lin, T.-C.; Chang, C.-T.; Kuo, H.-F.; Chang, H.-M.; et al. P2Y12 Inhibitor Monotherapy versus Conventional Dual Antiplatelet Therapy in Patients with Acute Coronary Syndrome after Percutaneous Coronary Intervention: A Meta-Analysis. Pharmaceuticals 2023, 16, 232. https://doi.org/10.3390/ph16020232
Feng W-H, Chang Y-C, Lin Y-H, Chen H-L, Chen C-Y, Lin T-H, Lin T-C, Chang C-T, Kuo H-F, Chang H-M, et al. P2Y12 Inhibitor Monotherapy versus Conventional Dual Antiplatelet Therapy in Patients with Acute Coronary Syndrome after Percutaneous Coronary Intervention: A Meta-Analysis. Pharmaceuticals. 2023; 16(2):232. https://doi.org/10.3390/ph16020232
Chicago/Turabian StyleFeng, Wen-Han, Yong-Chieh Chang, Yi-Hsiung Lin, Hsiao-Ling Chen, Chun-Yin Chen, Tsung-Han Lin, Tzu-Chieh Lin, Ching-Tang Chang, Hsuan-Fu Kuo, Hsiu-Mei Chang, and et al. 2023. "P2Y12 Inhibitor Monotherapy versus Conventional Dual Antiplatelet Therapy in Patients with Acute Coronary Syndrome after Percutaneous Coronary Intervention: A Meta-Analysis" Pharmaceuticals 16, no. 2: 232. https://doi.org/10.3390/ph16020232