
Quercetin as a Therapeutic Product: Evaluation of Its Pharmacological Action and Clinical Applications—A Review

 , ,
, ,
Abstract
:1. Introduction
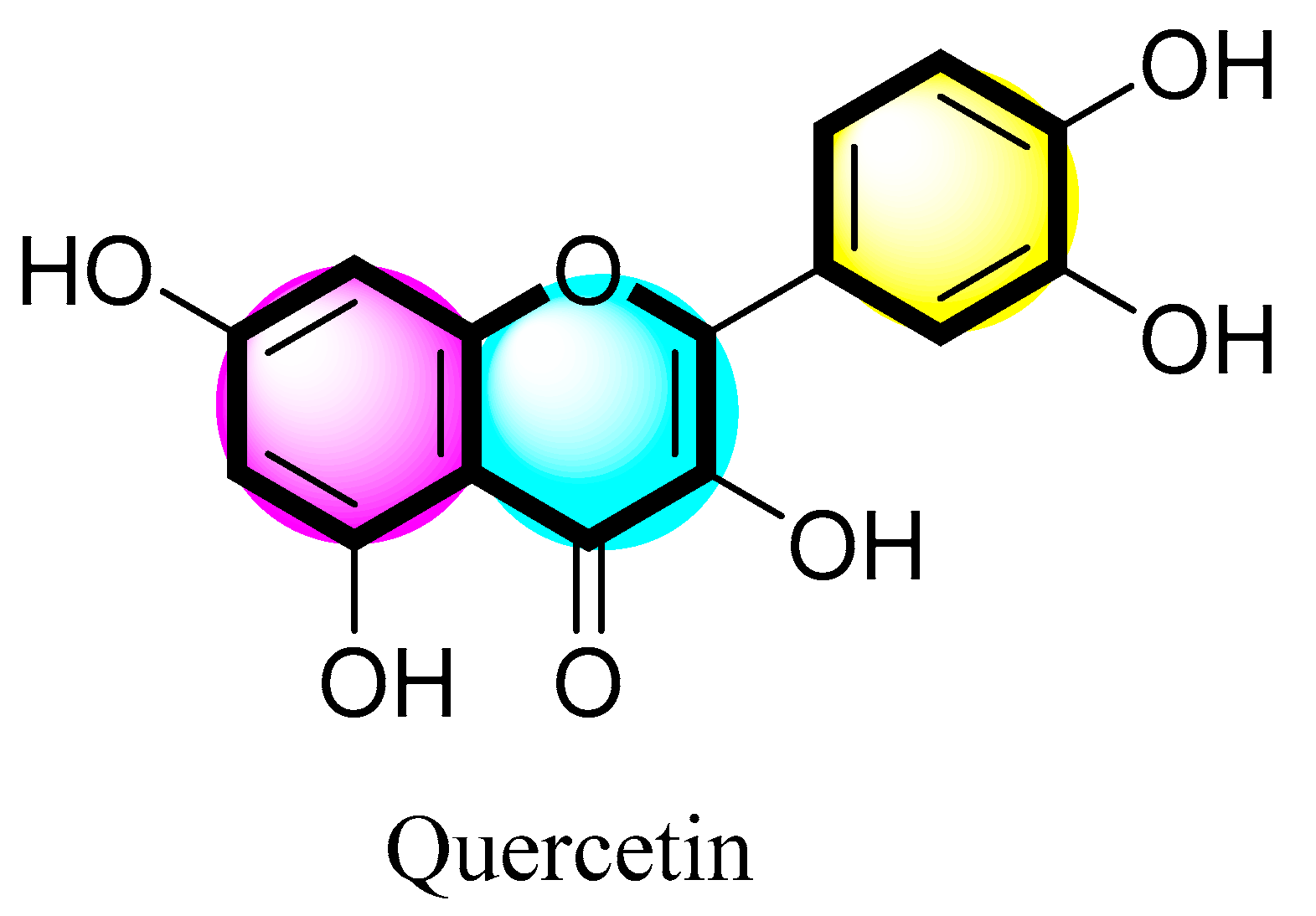
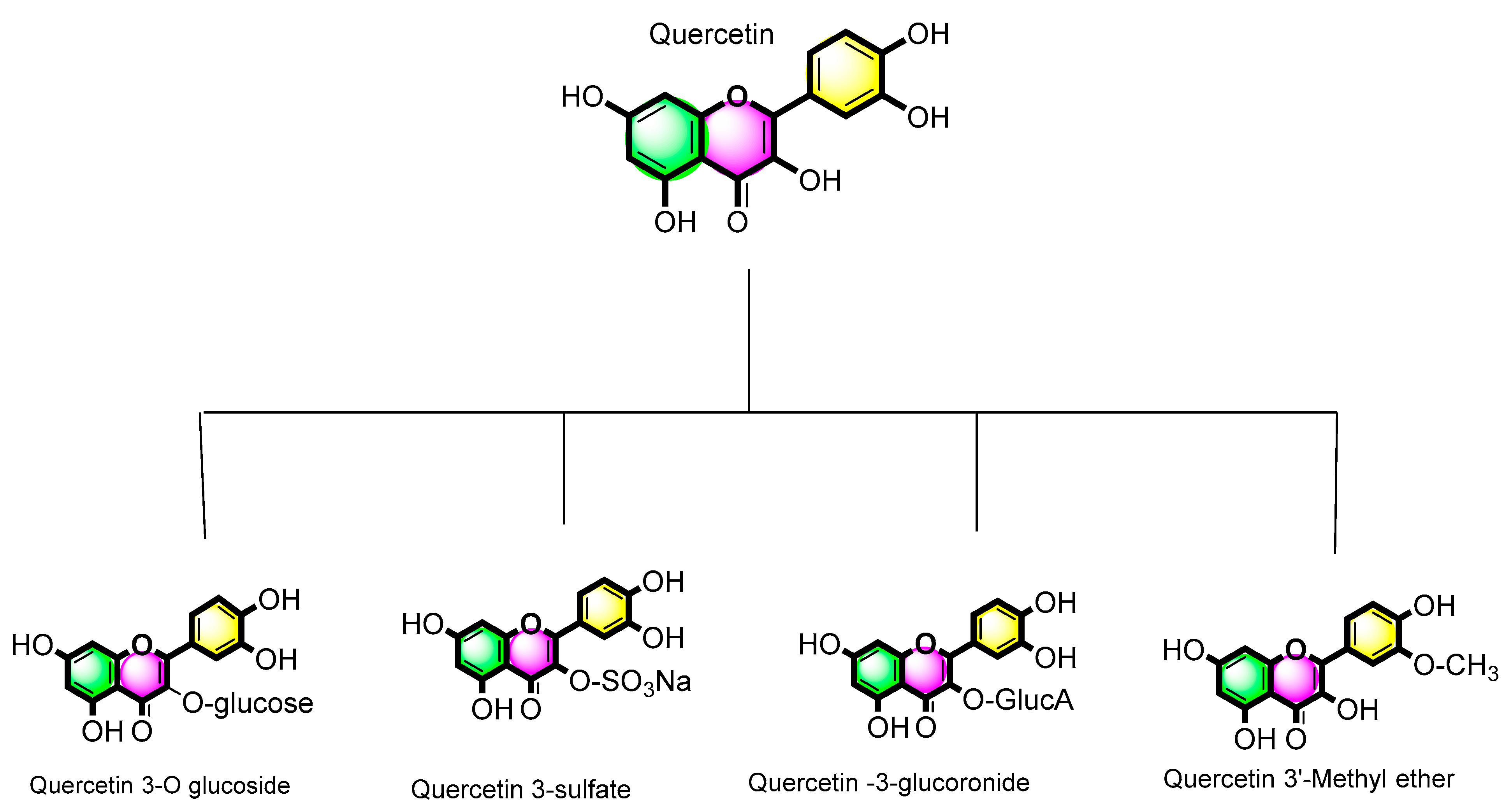
2. The Structure and Sources of Quercetin
Chemistry of Quercetin and Its Derivatives
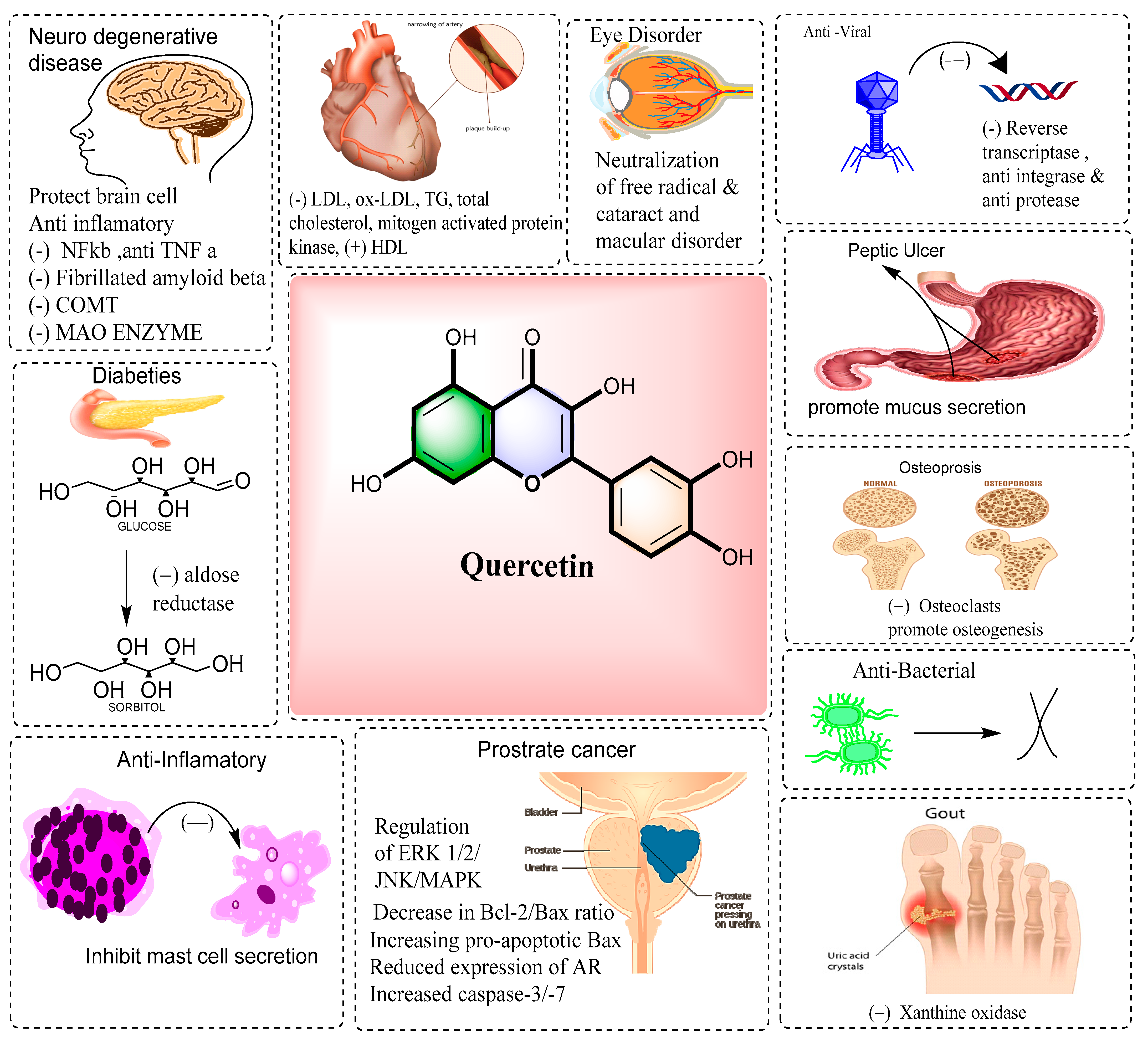
3. Pharmaceutical Applications and Activities of Quercetin
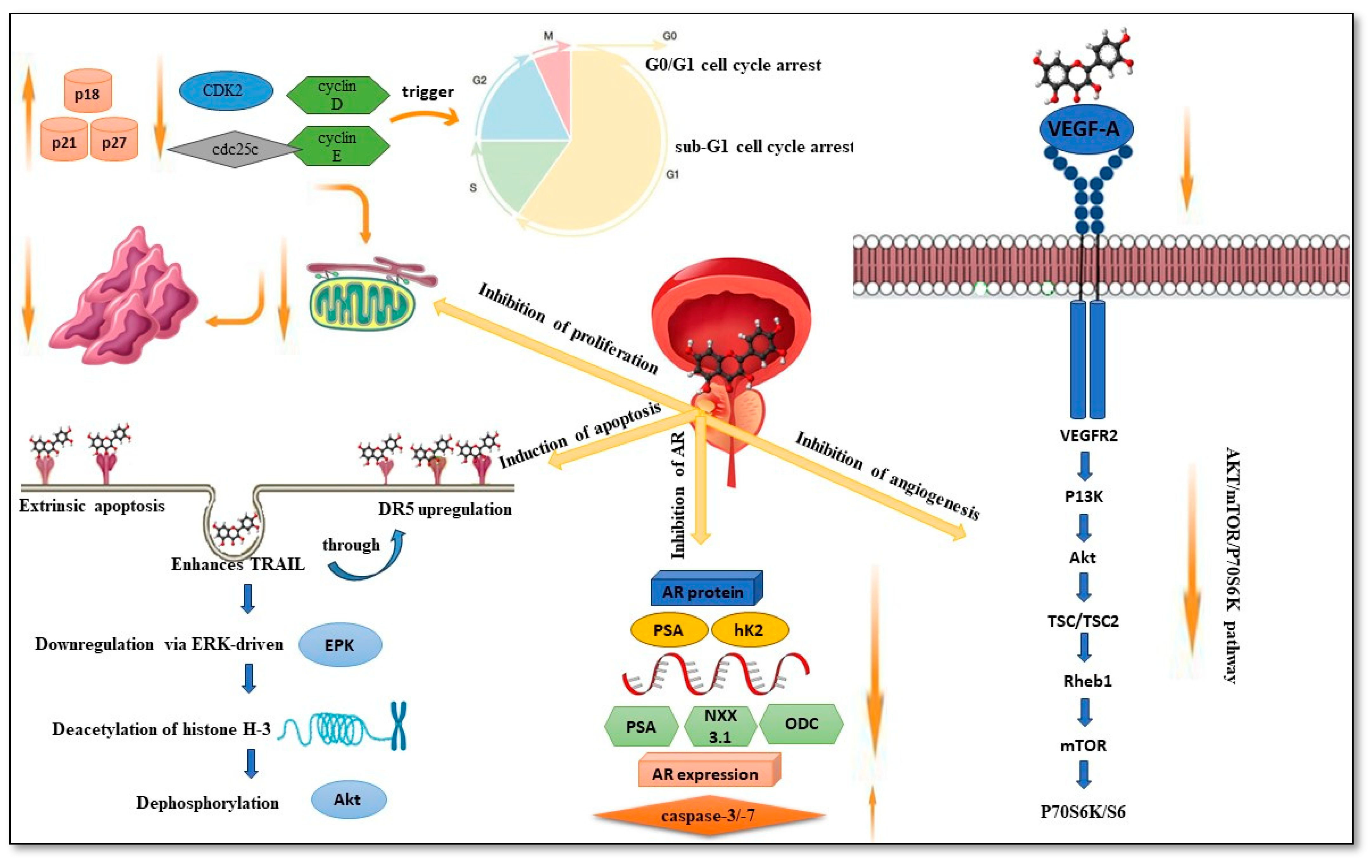
3.1. MOA of Quercetin in Prostate Cancer
3.1.1. Inhibition of Proliferation
3.1.2. Induction of Apoptosis
3.1.3. Inhibition of the Androgen Receptor (AR)
3.1.4. Inhibition of Angiogenesis
3.2. Patents Related to Therapeutic Uses of Quercetin

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. No. | Patent Publication Number | Title of the Patent | Activity and Application | Reference |
|---|---|---|---|---|
| 1. | US20040161247A1 | Therapeutic agent for osteoporosis comprising an active ingredient of quercetin derivatives | The present invention relates to a therapeutic agent for osteoporosis, which comprises an active ingredient of quercetin derivatives. | [60] |
| 2. | US8440704B2 | Quercetin-containing compositions | This invention relates to a composition containing quercetin, vitamin B3, and vitamin C. | [61] |
| 3. | JP3896577B2 | Quercetin glycoside composition and preparation method | Preparation of compounds containing saccharide radicals produced by the action of a beta-amylase, e.g., maltose. | [62] |
| 4. | AU2012340840B2 | Method for treating hepatitis C virus infection using quercetin-containing compositions | Heterocyclic compounds having nitrogen as a ring hetero atom, e.g., guanethidine. | [63] |
| 5. | WO2009045735A2 | Method for stabilizing quercetin | This invention relates to a method for stabilizing quercetin by placing it in a solution containing vitamin B3 and vitamin C and assessing the stability of the quercetin in the mixture. | [64] |
| 6. | CA2735826C | Reducing cholesterol levels with combined use of quercetin and statin | The use of a first composition containing quercetin, vitamin C, and vitamin B3, and a second composition containing a statin and a pharmaceutically acceptable carrier, for reducing the plasma cholesterol level in a subject is described. | [65] |
| 7. | CN103145669A | Process of clean production of quercetin | Process of clean production of quercetin. | [66] |
| 8. | US6562866B1 | Method for preventing or treating elevated blood lipid level-related diseases by administering rutin and quercetin | Method for treating or preventing an elevated blood lipid level-related disease in a mammal, which comprises administering thereto an effective amount of rutin, quercetin, or a mixture thereof. | [67] |
| 9. | US5445842A | Quercetin-containing coloring | A quercetin-containing colorant that has, as an effective component, a quercetin that is included by cyclodextrin. | [68] |
| 10. | CN101111244B | Composition for promoting production of hyaluronic acid containing kaempferol and quercetin | Disclosed is a composition for promoting the production of hyaluronic acid containing at least one of kaempferol and quercetin. | [69] |
| 11. | CN104817603A | Method for preparing quercetin-3-O-beta-D-glucuronide from lotus seedpod | The invention relates to a method for preparing quercetin-3-O-beta-D-glucuronide from lotus seedpod. | [70] |
| 12. | US7049301B2 | Quercetin derivatives and their medical usages | This invention relates to quercetin derivative, its preparation, and a pharmaceutical combination, as well as their medical uses for the prevention or treatment of diseases. | [71] |
| 13. | US9289444B2 | Composition for promoting hematogenesis containing quercetin 3-O-β-(2″-galloyl)-rhamnopyranoside as active ingredient | This invention relates to a composition for promoting hematopoiesis and for treating, preventing, or alleviating cytopenia or bone marrow failure comprising quercetin 3-O-β-(2″-galloyl)-rhamnopyranoside (QGR) as active ingredient. | [72] |
| 14. | CN101955514A | Method for synthesizing agarose gel hydrogen bond adsorbing chromatography medium by using quercetin as genin | The invention relates to a method for synthesizing a hydrogen bond adsorbing medium by taking agarose gel as a matrix and taking quercetin as genin. | [73] |
| 15. | TWI618573B | A quercetin-type surfactant, its preparation method and application. | The invention prepares a natural quercetin-type surfactant and uses the quercetin and the diol compound to synthesize a quercetin derivative under an acidic catalyst. | [74] |
| 16. | US20080031940A1 | Quercetin-containing composition, methods of making, and methods of using | The composition is a sustained release composition in tablet or capsule form suitable for oral administration to a human. Methods of making and using the composition are provided. | [75] |
| 17. | RU2745123C1 | Bioactive composition based on a cross-linked hyaluronic acid salt containing resveratrol and a method of its preparation a method for its preparation | Bioactive composition based on a cross-linked hyaluronic acid salt containing quercetin and a method for its preparation. | [76] |
| 18. | CN106822085B | Application of oncolytic adenovirus expressing TRAIL and quercetin in inhibition of liver cancer cell proliferation | Application of oncolytic adenovirus expressing TRAIL and quercetin in inhibition of liver cancer cell proliferation. | [77] |
3.3. Clinical Trials of the Therapeutic Effects of Quercetin
3.3.1. Cardiovascular Disease (CVD) Risk
3.3.2. Anti-Inflammatory
3.3.3. Pulmonary Diseases and COVID-19
3.3.4. Polycystic Ovary Syndrome (PCOS)
3.3.5. Diabetes Mellitus
3.3.6. Obesity
3.3.7. Antioxidant
3.3.8. Blood Pressure
3.3.9. Other Therapeutic Effects
| Therapeutic Effect | Design of the Study | Number of Subjects | Dosage of Quercetin | Duration | Results | Reference |
|---|---|---|---|---|---|---|
| Antioxidant | RCT | NA | 500 mg/day | 8 weeks | It significantly increased antioxidant capacity (TAC) and decreased TNF-α levels and it improved the insecurity dimension of quality of life. | [115] |
| Anti-inflammatory | RCT | 100 | 500 mg | 9 days | Quercetin supplementation may help limit the vigorous inflammatory response triggered by coronary artery bypass (CABG) and subsequent postoperative complications in patients suffering from an acute coronary syndrome. | [116] |
| A meta-analysis study of RCTs | NA | 500 mg/day | NA | It showed a significant effect on CRP. | [92] | |
| RCT | NA | >500 mg/day | 8 weeks | It reduced morning pain, after-activity pain, and early morning stiffness (EMS); hs-TNFa was significantly reduced while there were no significant differences in ESR, swollen (SSC), and tender joint counts (SJC). | [93] | |
| RCT | 42 | 500 mg/day | 12 weeks | It reduced iron, ferritin, transferrin saturation, and high sensitivity CRP while it increased transferrin, which makes it a potent agent in improving iron status in thalassemia. It was also found that quercetin had no significant effect on TNF-α and total iron binding capacity. | [91] | |
| Obesity | Meta-analysis study of RCTs | 525 subjects | NA | NA | No significant effect on body weight, body mass index, waist circumference, and waist-to-hip ratio, which confirms that there is no noticeable effect of quercetin on weight loss. | [108] |
| Randomized, double-blind, placebo-controlled study | 37 female | 100 mg capsule | 12 weeks | Quercetin-rich onion peel extract (OPE) supplementation significantly decreased the percent of body fat mass (PBFM) and induced plasma adiponectin levels compared with baseline values in addition also reduces the percentage of, BMI, and waist circumference, which corresponds to the results of this study. | [117] | |
| Double-blind cross-over study | 49 healthy candidates | 150 mg/day | 8 weeks, intermitted by washout phase for 3 weeks. | It reduced postprandial triacylglycerol, postprandial SBP, and waist circumference while increasing HDL and TNFα. | [92] | |
| Pulmonary diseases and COVID-19 | RCT | Chronic obstructive pulmonary disease patients | 500, 1000, or 2000 mg/day | 1 week | It showed that quercetin administration was safe up to 2000 mg/day as evaluated by blood profile and lung function questionnaire. | [94] |
| Open-label, randomized controlled clinical trial | 25 patients in early to mild stage of COVID-19 | 168 mg and 260 mg | NA | It exhibited a speed resolve in the treated patients. | [96] | |
| RCT | 60 severe cases hospitalized COVID-19 | 1000 mg/d | 1 week | It showed the effectiveness of quercetin in reducing LDH, q-CRP, and ALP levels, in addition to an increase in the respiratory rate and hemoglobin level. | [97] | |
| Open-label randomized controlled clinical trial | 50 outpatients with early to moderate stage of COVID-19 | 500 mg/d | 2 weeks | It showed a speedy recovery from COVID-19 as 34 patients tested negative in the treated group while 12 patients tested negative in the control group; the patients who received quercetin showed a significant reduction in lactate dehydrogenase (LDH) level. | [98] | |
| Randomized, open-label, and controlled clinical trial | 21 outpatients of COVID-19 | NA | 2 weeks | The add-on treatment with quercetin, decreased D-dimer, LDH, CRP, and ferritin levels. It can be concluded that add-on quercetin supplantation can reduce the severity and speed the recovery in COVID-19 patients. | [99] | |
| Randomized, double-blinded, placebo-controlled trial | 1002 patients with upper respiratory tract infection URTI | 500 and 1000 mg/day | 12 weeks | It was shown that there is no significant effect of quercetin on URTI rates as compared to placebo. | [95] | |
| Polycystic Ovary Syndrome (PCOS) | RCT | 84 women with PCOS | 1 g of quercetin daily for | 12 weeks | It was shown that quercetin supplements increased the expression of ADIPOR1 and ADIPOR2 transcript, and it also improved AMPK level by 12.3% when compared to the control group. | [100] |
| RCT | 84 women with PCOS | 1 g | 12 weeks | It slightly elevated adiponectin level by 5.56% as compared to placebo, and it also increased HMW adiponectin by 3.9% when compared to the placebo, while it reduced the level of LH and testosterone. It was also recorded that quercetin significantly lowered HOMA-IR levels by 1.84 compared to 2.21 in the placebo group. | [101] | |
| A systematic review of 3 RCTs | NA | NA | NA | It reported that quercetin was able to reduce LH, testosterone, and insulin resistance. Despite the fact that quercetin enhanced dyslipidemia, there was no significant difference in weight loss, suggesting that quercetin has anti-inflammatory and antioxidant features rather than weight-reducing effects. | [102] | |
| Diabetes Mellitus | Randomized blinded cross-over study | NA | 400 mg | NA | It was revealed that 400 mg of quercetin was able to reduce postprandial hyperglycemia in T2DM patients effectively. | [118] |
| RCT | 47 patients with T2DM | 250 mg/day | 8 weeks | It enhanced TAC significantly compared to cellulose placebo group, and it also showed a notable reduction in ox-LDL. | [105] | |
| A meta-analysis and systematic review of 9 RCTs | NA | ≥500 mg/day | ≥8 weeks | it was found that quercetin reduced FPG with ≥8 weeks of the treatment with a dosage of ≥500 mg/day, besides a significant reduction in insulin concentrations in a dosage of ≥500 mg/day. | [106] | |
| Cardiovascular risk | Double-blind randomized clinical trial | 72 women | 500 mg of quercetin daily | 10 weeks | It significantly decreased TNF-α, IL-6, HDL, and systolic blood pressure while LDL, total cholesterol, and TG were not significantly reduced. | [79] |
| RCT | 24 subjects | 100 mL of quercetin-rich onion juice daily | 8 weeks | It was proved that onion juice effectively reduced LDL-c and total cholesterol and increased TAC and also increased the lagtime of LDL oxidation. Suggesting that quercetin-rich onion juice might provide a markable effect on cardiovascular diseases. | [119] | |
| A meta-analysis and systemic review of 16 RCTs | NA | NA | NA | The pooled results found that quercetin supplements significantly decreased total cholesterol, LDL, and CRP. While there is no significant difference found in TG, HDL, IL-6, and TNF-α levels. | [82] | |
| RCT | Healthy candidates with 4.0–7.2 mmol/L cholesterol level | 1 g | 28 days | There was no alteration in the cardiovascular risk factors including HDL, LDL, and triglyceride levels. Also, no modification was noticed in the thrombogenic risk parameters including blood pressure and platelet thromboxane B2 production. | [81] | |
| Double-blind, randomized study was | Healthy persons with dyslipidemia | NA | 2 months | It decreased in TG, cholesterol (from 6.21 mmol/L to 5.09 mmol/L), and LDL (from 3.98 mmol/L to 2.91 mmol/L) and increased in HDL (from 0.89 mmol/L to 1.29 mmol/L). These findings agree that quercetin is a promising candidate for lowering blood lipids. | [85] | |
| Double-blinded, placebo-controlled cross-over trial | 33 overweight subjects with metabolic syndrome | 150 mg/day | 6 weeks | It was found that quercetin reduced SBP by 2.6 mmHg. It also reduced atherogenic oxidized LDL. | [82] | |
| Randomized, double-blinded, placebo-controlled study | 49 subjects | 100 mg/day | 10 weeks | It revealed that quercetin decreased total cholesterol, LDL, systolic, diastolic blood pressure, and Glucose concentrations significantly. Furthermore, it increased HDL. | [83] | |
| RCT | 530 healthy individuals | 16–1200 mg | 2–12 weeks | It showed a notable decrease in TC, LDL, and TG; additionally, a significant elevation was observed in HDL. | [87] | |
| Randomized double-blind placebo-controlled parallel-group | 70 healthy subjects | 3.12–3000 mg | 12 weeks | A reduction in LDL levels in the candidates whose LDL was higher than normal was observed. | [88] | |
| Double-blind cross-over | 49 healthy males | 150 mg | 8 weeks | The study revealed an increase in HDL, postprandial triacylglycerol, and TNFα levels. | [89] | |
| Blood pressure | Double-blind, placebo-controlled, cross-over study | 19 subjects with prehypertension, and 22 subjects with hypertension | 730 mg/d | 4 weeks | It was shown that blood pressure did not change in prehypertensive subjects. On the other hand, there was a notable reduction in the systolic and diastolic blood pressure in the hypertension subjects after quercetin supplantation, although no effect was detected in oxidative stress. | [110] |
| RCT | 896 subjects | 30–1000 mg | 2–12 weeks | SBP and DBP were significantly reduced. Another change was observed in HDL and TG in which candidates were given quercetin for 8 weeks or more. | [111] | |
| Randomized, double-blind, placebo-controlled cross-over trial | 37 nonsmoking healthy adults with SBP between 125 and 160 mm Hg | 160 mg/day | 4 weeks | Quercetin might play a key role in the treatment of diseases in which Methylglyoxal (MGO) plays a pivotal role. | [120] | |
| Other therapeutic effects | Randomized, double-blind, placebo-controlled trial | NA | NA | 2 weeks | It was revealed that ALT, AST, and GGT were decreased by 50.4%, 37.2%, and 89.9%, respectively. The levels of TG, TC, and TNF-α reduced by 33.3%, 16.7%, and 39.8%, respectively, suggesting the potential value of quercetin in treating Non-alcoholic fatty liver disease (NAFLD). | [112] |
| RCT | 480 participants | NA | NA | BYLY has 132 active components, and quercetin might be the key effective component that could decrease the rate of early abortion. It is believed that a possible mechanism is the protective effect of quercetin on trophoblasts by decreasing Drp1 expression through regulating miR-34a-5p. | [111] | |
| Double-blind, placebo-controlled randomized trial | 20 adult patients who received high-dose chemotherapy for the treatment of blood malignancies | 250 mg capsules twice daily | 4 weeks | It was concluded that the incidence of oral mucositis was lower in the quercetin group (3 patients in the intervention group and 6 patients in the control group), but the severity of oral mucositis was higher in the treated group compared to the control group (2.6 vs. 2. respectively), which might be due to lower oral health care in the intervention group. | [113] |
3.4. Marketed Products
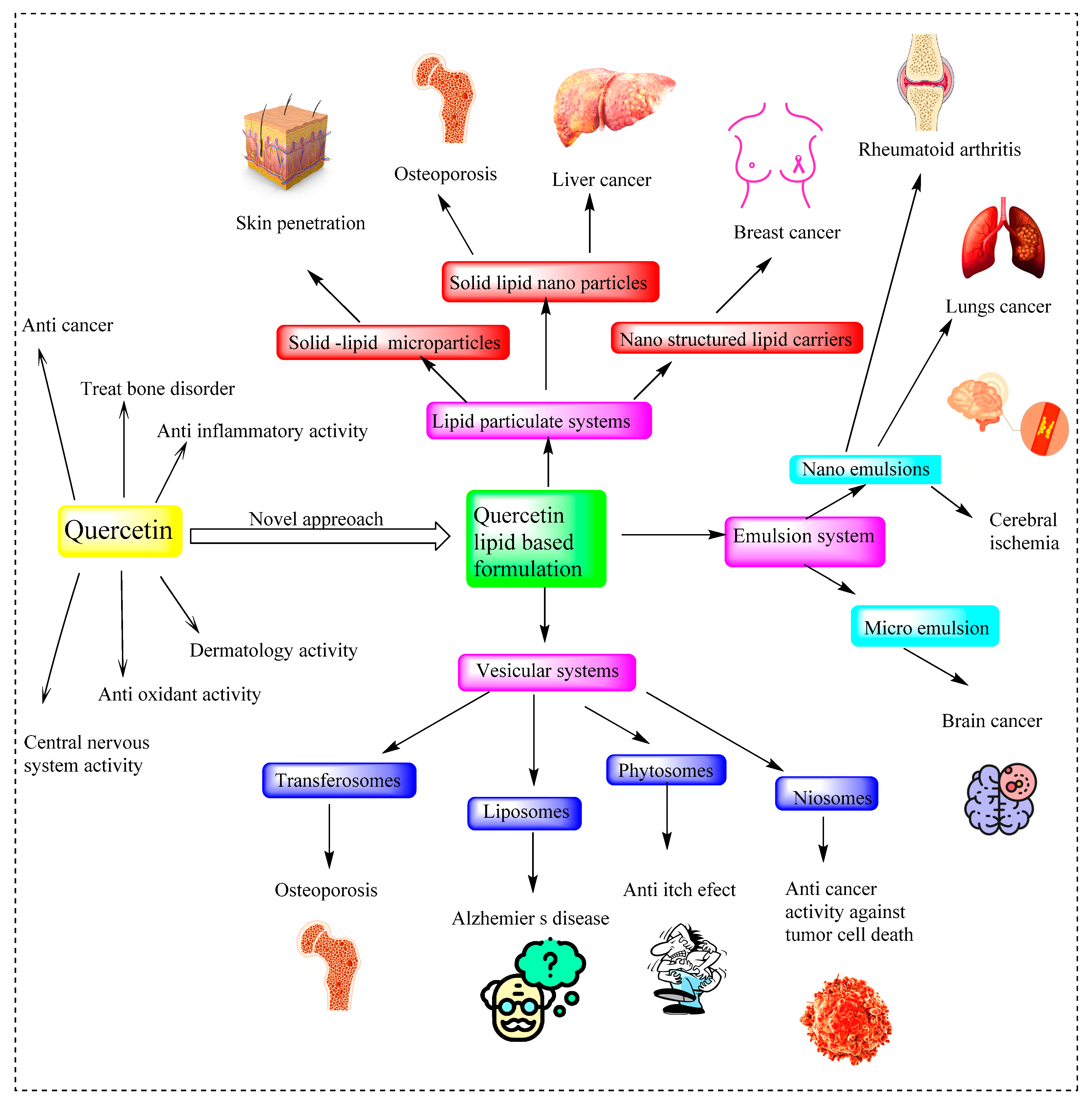
4. Approaches for Improving Quercetin Pharmacokinetics Quercetin-Based Nanoformulation
4.1. Solid Lipid Nanoparticles
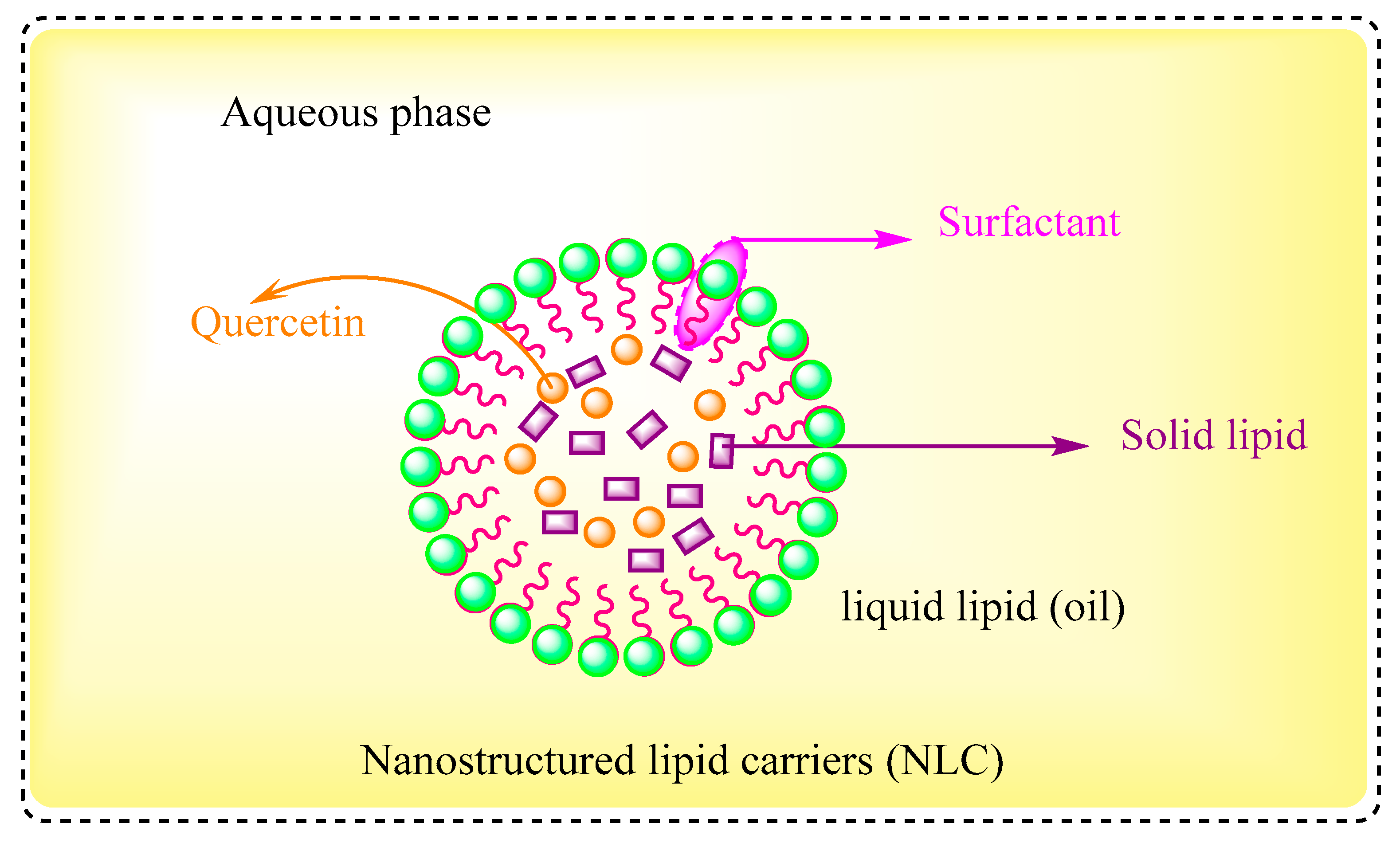
4.2. Nanostructured Lipid Carriers
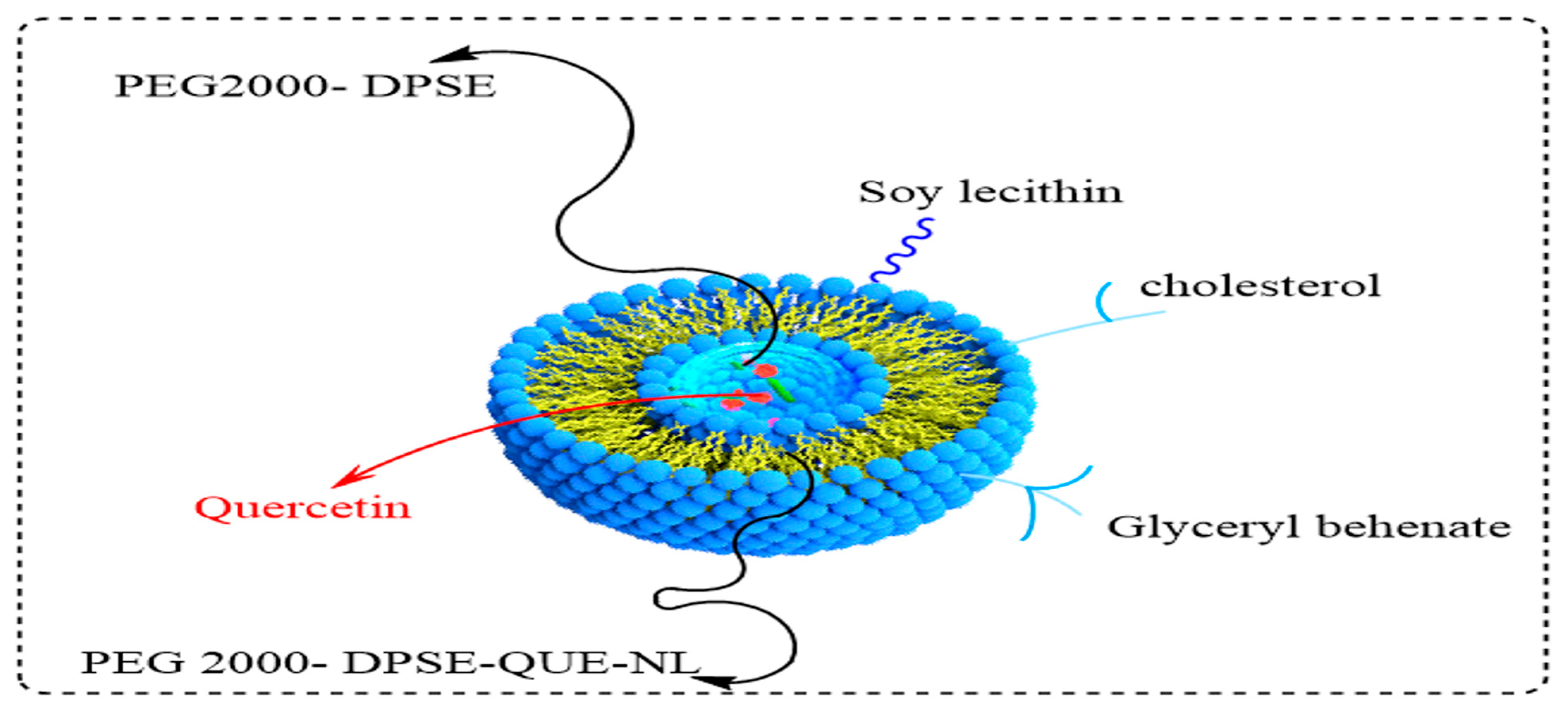
4.3. Liposomes
4.4. Niosomes
4.5. Transferosomes
4.6. Nanoemulsions
4.7. Microemulsion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Massi, A.; Bortolini, O.; Ragno, D.; Bernardi, T.; Sacchetti, G.; Tacchini, M.; De Risi, C. Research progress in the modification of quercetin leading to anticancer agents. Molecules 2017, 22, 1270. [Google Scholar] [CrossRef]
- Aucoin, M.; Cooley, K.; Saunders, P.R.; Cardozo, V.; Remy, D.; Cramer, H.; Abad, C.N.; Hannan, N. The effect of quercetin on the prevention or treatment of COVID-19 and other respiratory tract infections in humans: A rapid review. Adv. Integr. Med. 2020, 7, 247–251. [Google Scholar] [CrossRef]
- David, A.V.A.; Arulmoli, R.; Parasuraman, S. Overviews of biological importance of quercetin: A bioactive flavonoid. Pharmacogn. Rev. 2016, 10, 84–89. [Google Scholar]
- Kwak, J.H.; Seo, J.M.; Kim, N.H.; Arasu, M.V.; Kim, S.; Yoon, M.K.; Kim, S.J. Variation of quercetin glycoside derivatives in three onion (Allium cepa L.) varieties. Saudi J. Biol. Sci. 2017, 24, 1387–1391. [Google Scholar] [CrossRef]
- Aghababaei, F.; Hadidi, M. Recent advances in potential health benefits of quercetin. Pharmaceuticals 2023, 16, 1020. [Google Scholar] [CrossRef] [PubMed]
- Gallelli, G.; Cione, E.; Serra, R.; Leo, A.; Citraro, R.; Matricardi, P.; Di Meo, C.; Bisceglia, F.; Caroleo, M.C.; Basile, S.; et al. Nano-hydrogel embedded with quercetin and oleic acid as a new formulation in the treatment of diabetic foot ulcer: A pilot study. Int. Wound J. 2020, 17, 485–490. [Google Scholar] [CrossRef]
- Tran, T.H.; Guo, Y.; Song, D.; Bruno, R.S.; Lu, X. Quercetin-containing self-nanoemulsifying drug delivery system for improving oral bioavailability. J. Pharm. Sci. 2014, 103, 840–852. [Google Scholar] [CrossRef] [PubMed]
- Shabir, I.; Pandey, V.K.; Dar, A.H.; Pandiselvam, R.; Manzoor, S.; Mir, S.A.; Shams, R.; Dash, K.K.; Fayaz, U.; Khan, S.A.; et al. Nutritional profile, phytochemical compounds, biological activities, and utilisation of onion peel for food applications: A review. Sustainability 2022, 14, 11958. [Google Scholar] [CrossRef]
- Li, Y.; Yao, J.; Han, C.; Yang, J.; Chaudhry, M.T.; Wang, S.; Liu, H.; Yin, Y. Quercetin, inflammation and immunity. Nutrients 2016, 8, 167. [Google Scholar] [CrossRef]
- Zaplatic, E.; Bule, M.; Shah, S.Z.A.; Uddin, M.S.; Niaz, K. Molecular mechanisms underlying protective role of quercetin in attenuating Alzheimer’s disease. Life Sci. 2019, 224, 109–119. [Google Scholar] [CrossRef]
- Khajuria, R.; Singh, S.; Bahl, A. General introduction and sources of flavonoids. In Current Aspects of Flavonoids: Their Role in Cancer Treatment; Springer: Singapore, 2019; pp. 1–7. [Google Scholar]
- Yi, H.; Peng, H.; Wu, X.; Xu, X.; Kuang, T.; Zhang, J.; Du, L.; Fan, G. The therapeutic effects and mechanisms of quercetin on metabolic diseases: Pharmacological data and clinical evidence. Oxidative Med. Cell. Longev. 2021, 2021, 6678662. [Google Scholar] [CrossRef] [PubMed]
- Ren, F.; Perussello, C.A.; Zhang, Z.; Gaffney, M.T.; Kerry, J.P.; Tiwari, B.K. Effect of agronomic practices and drying techniques on nutritional and quality parameters of onions (Allium cepa L.). Dry. Technol. 2018, 36, 435–447. [Google Scholar] [CrossRef]
- Wang, J.; Yin, L.; Hobbi, P.; Okoro, O.V.; Hajiabbas, M.; Hamidi, M. Chemical Composition, Antioxidant Activity and Cytocompatibility of Polyphenolic Compounds Extracted from Food Industry Apple Waste: Potential in Biomedical. Molecules 2023, 28, 675. [Google Scholar] [CrossRef]
- Savic, I.M.; Nikolic, V.D.; Savic, I.M.; Nikolic, L.B.; Stankovic, M.Z. Development and validation of a new RP-HPLC method for determination of quercetin in green tea. J. Anal. Chem. 2023, 68, 906–911. [Google Scholar] [CrossRef]
- Natividade, M.M.P.; Corrêa, L.C.; de Souza, S.V.C.; Pereira, G.E.; de Oliveira Lima, L.C. Simultaneous analysis of 25 phenolic compounds in grape juice for HPLC: Method validation and characterization of São Francisco Valley samples. Microchem. J. 2013, 110, 665–674. [Google Scholar] [CrossRef]
- Nandasiri, H.M.A.R. Antioxidant, Antihypertensive and Lipid Lowering Properties of Fruit Vinegar Beverages. Master Thesis, Dalhousie University, Halifax, NS, Canada, 2012. [Google Scholar]
- White, B.L.; Howard, L.R.; Prior, R.L. Proximate and polyphenolic characterization of cranberry pomace. J. Agric. Food Chem. 2010, 58, 4030–4036. [Google Scholar] [CrossRef] [PubMed]
- Nagraj, G.S.; Chouksey, A.; Jaiswal, S.; Jaiswal, A.K. Broccoli. In Nutritional Composition and Antioxidant Properties of Fruits and Vegetables. Academic Press: Cambridge, MA, USA, 2020; pp. 5–17. [Google Scholar]
- Abraão, A.S.; Fernandes, N.; Silva, A.M.; Domínguez-Perles, R.; Barros, A. Prunus lusitanica L. fruits as a novel source of bioactive compounds with antioxidant potential: Exploring the unknown. Antioxidants 2022, 11, 1738. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.B.; Walsh, K.B.; Naiker, M.; Ameer, K. The use of infrared spectroscopy for the quantification of bioactive compounds in food: A review. Molecules 2023, 28, 3215. [Google Scholar] [CrossRef]
- Suntornsuk, L.; Kasemsook, S.; Wongyai, S. Quantitative analysis of aglycone quercetin in mulberry leaves (Morus alba L.) by capillary zone electrophoresis. Electrophoresis 2003, 24, 1236–1241. [Google Scholar] [CrossRef] [PubMed]
- Sadek, K.M.; Abouzed, T.K.; Abouelkhair, R.; Nasr, S. The chemo-prophylactic efficacy of an ethanol Moringa oleifera leaf extract against hepatocellular carcinoma in rats. Pharm. Biol. 2017, 55, 1458–1466. [Google Scholar] [CrossRef]
- Devaraj, V.C.; Krishna, B.G.; Viswanatha, G.L. Simultaneous determination of quercetin, rutin and kaempferol in the leaf extracts of Moringa oleifera Lam.; Raphinus sativus Linn. by liquid chromatography-tandem mass spectrometry. J. Chin. Integr. Med. 2011, 9, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- Bhandare, S.B.; Laddha, K.S. Simultaneous quantification of kaempferol and quercetin in medicinal plants using HPTLC. Int. J. Pharm. Sci. Res. 2016, 7, 2379. [Google Scholar]
- Zhang, H.; Birch, J.; Pei, J.; Mohamed Ahmed, I.A.; Yang, H.; Dias, G. Identification of Six Phytochemical Compounds from Asparagus officinalis L. Root Cultivars from New Zealand and China Using UAE-SPE-UPLC-MS/MS: Effects of Extracts on H2O2-Induced Oxidative Stress. Nutrients 2019, 11, 107. [Google Scholar] [CrossRef]
- Saygi, K.O. Quantification of Phenolics from Coriandrum sativum vulgare and Coriandrum sativum microcarpum by HPLC–DAD. Iran. J. Sci. Technol. Trans. A Sci. 2021, 45, 1319–1326. [Google Scholar] [CrossRef]
- Assefa, A.D.; Choi, S.; Lee, J.E.; Sung, J.S.; Hur, O.S.; Ro, N.Y.; Lee, H.S.; Jang, S.W.; Rhee, J.H. Identification and quantification of selected metabolites in differently pigmented leaves of lettuce (Lactuca sativa L.) cultivars harvested at mature and bolting stages. BMC Chem. 2019, 13, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Spagnuolo, C.; Moccia, S.; Russo, G.L. Anti-inflammatory effects of flavonoids in neurodegenerative disorders. Eur. J. Med. Chem. 2018, 153, 105–115. [Google Scholar] [CrossRef]
- Materska, M. Quercetin and its derivatives: Chemical structure and bioactivity—A review. Pol. J. Food Nutr. Sci. 2008, 58, 407–413. [Google Scholar]
- Nam, J.S.; Sharma, A.R.; Nguyen, L.T.; Chakraborty, C.; Sharma, G.; Lee, S.S. Application of bioactive quercetin in oncotherapy: From nutrition to nanomedicine. Molecules 2016, 21, 108. [Google Scholar] [CrossRef] [PubMed]
- Panthi, V.K.; Kaushal, S.; Adhikari, B.; Basnet, N.; Chaudhary, D.; Pajaruli, R.R.; Pokhrel, P. A Review of Quercetin: Anti-Cancer Activity. Int. J. Innov. Res. Rev. 2020, 4, 1–7. [Google Scholar]
- Ozgen, S.; Kilinc, O.K.; Selamoğlu, Z. Antioxidant activity of quercetin: A mechanistic review. Turk. J. Agric.-Food Sci. Technol. 2016, 4, 1134–1138. [Google Scholar] [CrossRef]
- Rauf, A.; Imran, M.; Khan, I.A.; ur-Rehman, M.; Gilani, S.A.; Mehmood, Z.; Mubarak, M.S. Anticancer potential of quercetin: A comprehensive review. Phytother. Res. 2018, 32, 2109–2130. [Google Scholar] [CrossRef]
- Liu, K.C.; Yen, C.Y.; Wu, R.S.C.; Yang, J.S.; Lu, H.F.; Lu, K.W. The roles of endoplasmic reticulum stress and mitochondrial apoptotic signaling pathway in quercetin-mediated cell death of human prostate cancer PC-3 cells. Environ. Toxicol. 2014, 29, 428–439. [Google Scholar] [CrossRef]
- Kumar, R.; Verma, V.; Jain, A.; Jain, R.K.; Maikhuri, J.P.; Gupta, G. Synergistic chemoprotective mechanisms of dietary phytoestrogens in a select combination against prostate cancer. J. Nutr. Biochem. 2011, 22, 723–731. [Google Scholar] [CrossRef] [PubMed]
- Mulholland, P.J.; Ferry, D.R.; Anderson, D.; Hussain, S.A.; Young, A.M.; Cook, J.E.; Hodgkin, E.; Seymour, L.W.; Kerr, D.J. Pre-clinical and clinical study of QC12, a water-soluble, pro-drug of quercetin. Ann. Oncol. 2001, 12, 245–248. [Google Scholar] [CrossRef]
- Wang, G.; Song, L.; Wang, H.; Xing, N. Quercetin synergizes with 2-methoxyestradiol inhibiting cell growth and inducing apoptosis in human prostate cancer cells. Oncol. Rep. 2013, 30, 357–363. [Google Scholar] [CrossRef]
- Yang, F.; Song, L.; Wang, H.; Wang, J.; Xu, Z.; Xing, N. Quercetin in prostate cancer: Chemotherapeutic and chemopreventive effects, mechanisms and clinical application potential. Oncol. Rep. 2015, 33, 2659–2668. [Google Scholar] [CrossRef] [PubMed]
- Xing, N.; Chen, Y.; Mitchell, S.H.; Young, C.Y. Quercetin inhibits the expression and function of the androgen receptor in LNCaP prostate cancer cells. Carcinogenesis 2001, 22, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Ferruelo, A.; Romero, I.; Cabrera, P.M.; Arance, I.; Andrés, G.; Angulo, J.C. Effects of resveratrol and other wine polyphenols on the proliferation, apoptosis and androgen receptor expression in LNCaP cells. Actas Urol. Esp. 2014, 38, 397–404. [Google Scholar] [CrossRef]
- Britton, R.G.; Horner-Glister, E.; Pomenya, O.A.; Smith, E.E.; Denton, R.; Jenkins, P.R.; Steward, W.P.; Brown, K.; Gescher, A.; Sale, S. Synthesis and biological evaluation of novel flavonols as potential anti-prostate cancer agents. Eur. J. Med. Chem. 2012, 54, 952–958. [Google Scholar] [CrossRef]
- Pratheeshkumar, P.; Budhraja, A.; Son, Y.O.; Wang, X.; Zhang, Z.; Ding, S. Quercetin Inhibits Angiogenesis Mediated Human Prostate Tumor Growth by Targeting VEGFR- 2 Regulated AKT/mTOR/P70S6K Signaling Pathways. PLoS ONE 2012, 7, e47516. [Google Scholar] [CrossRef]
- Sharma, S.; Sahni, J.K.; Ali, J.; Baboota, S. Patent perspective for potential antioxidant compounds-rutin and quercetin. Recent Pat. Nanomed. 2013, 3, 62–68. [Google Scholar] [CrossRef]
- Mokhtar, M.; Youcefi, F.; Keddari, S.; Saimi, Y.; Elhao, S.O.; Cacciola, F. Phenolic content and in vitro antioxidant and anti-inflammatory evaluation of Algerian Ruta graveolens L. Chem. Biodivers. 2022, 19, e202200545. [Google Scholar] [CrossRef]
- Joshi, N.S.; Aggarwal, P.; Hirpara, V.K.; Jaggi, M.; Singh, A.; Awasthi, A.; Verma, R. Novel Quercetin Derivatives as Anti-Cancer Agents. U.S. Patent Application No. 12/676,709, 10 February 2011. [Google Scholar]
- Shinke, Y.; Kuzumi, A.; Haneza, Y.; Matsukawa, T.; Matsui, T.; Yamada, Y.; Yamada, I. Novel Quercetin Derivative. Japan Patent Application No. JP2012099008A, 28 September 2016. [Google Scholar]
- Yoshimi, H.A.Z.A.; Kuzumi, A.; Matsukawa, T.; Matsui, T.; Yamada, Y.; Yamada, I. Reaction Product of Quercetin and P-Coumaric Acid. Japan Patent Application No. JP2015086186A, 24 May 2017. [Google Scholar]
- Uha Mikakuto Co. Ltd. New Quercetin Derivative. Japan Patent Application No. JP5888120B2, 16 March 2016. [Google Scholar]
- CETAR BIO-TECH Inc. Quercetin Hydrocarbylation Derivative and Preparation Method Thereof and Application. China Patent Application No. CN106674180A, 31 May 2019. [Google Scholar]
- Dalian Medical University. Quercetin Hydrocarbylation Derivative and Preparation Method Thereof and Application. China Patent Application No. CN103467426B, 18 November 2015. [Google Scholar]
- Uha Mikakuto Co. Ltd. New Quercetin Derivative. Japan Patent Application No. JP5888121B2, 16 March 2016. [Google Scholar]
- Uha Mikakuto Co. Ltd. New Quercetin Derivative. Japan Patent Application No. JP5891970B2, 23 March 2016. [Google Scholar]
- Gonos, E.; Chondrogianni, N.; Chinou, I. Anti-Aging Properties of Quercetin, 18alpha-Glycyrrhetinic Acid and Hederagenin and Their Derivatives. U.S. Patent Application No. US20110034427A1, 10 February 2011. [Google Scholar]
- Talbott, S.M. A Guide to Understanding Dietary Supplements, 1st ed.; Haworth Press: Philadelphia, PA, USA, 2003. [Google Scholar]
- Haneza, Y.; Kuzumi, A.; Matsukawa, T.; Yamada, Y.; Yamada, I. Novel Quercetin Derivative. Japan Patent Application No. JP2013227231A, 22 June 2016. [Google Scholar]
- Shandong University of Technology. Method for Preparing Quercetin Derivative Containing Benzylpiperazine and Gastric Mucosal Protection Effect of Quercetin Derivative. China Patent Application No. CN104274455A, 24 March 2018. [Google Scholar]
- Sharma, A.; Kashyap, D.; Sak, K.; Tuli, H.S.; Sharma, A.K. Therapeutic charm of quercetin and its derivatives: A review of research and patents. Pharm. Pat. Anal. 2018, 7, 15–32. [Google Scholar] [CrossRef]
- Lines, T.C. Method for Treating Thrombotic Disorders Using Quercetin-Containing Compositions. U.S. Patent Application No. US10391096B2, 27 August 2019. [Google Scholar]
- Kim, C.S.; Ha, H.K.; Song, K.Y. Therapeutic Agent or Osteoporosis Comprising an Active Ingredient of Quercetin Derivatives. U.S. Patent Application No. US20040162247A1, 27 August 2019. [Google Scholar]
- Lines, T.C. Quercetin-Containing Compositions. U.S Patent Application No US8440704B2, 14 May 2013. [Google Scholar]
- Ono, Y.; Tomimori, N.; Tateishi, N.; Moriwaki, M.; Emura, K.; Okuyama, S. Quercetin Glycoside Composition and Preparation Method. Japan Patent Application No. WO2006070883A1, 6 July 2006. [Google Scholar]
- Lines, T.C. Method for Treating Hepatitis C Virus Infection Using Quercetin-Containing Compositions. Australia Patent Application No. AU2012340840A1, 30 June 2016. [Google Scholar]
- Lines, T.C. Method for Stabilizing Quercetin. U.S Patent Application No US8202900B2, 11 June 2012. [Google Scholar]
- Lines, T.C. Reducing Cholesterol Levels with Combined Use of Quercetin and Statin. US Patent Application No. CA2735826C, 11 July 2017. [Google Scholar]
- Lee, Y. Process of Clean Production of Quercetin. China Patent Application No. CN103145669A, 12 June 2013. [Google Scholar]
- Lutum, E.; Semmler, K.; von Wolfersdorf, J. Method for Preventing or Treating Elevated Blood Lipid Level-Related Diseases by Administering Rutin and Quercetin. U.S. Patent Application No. US20010014669A1, 21 January 2003. [Google Scholar]
- Tanaka, T.; Okemoto, H.; Kuwahara, N. Quercetin-Containing Coloring. Canada Patent Application No. CA2112942A1, 26 August 1994. [Google Scholar]
- Kim, N.X. Promoting Production of Hyaluronic Acid Containing Kaempferol and Quercetin. China Patent Application No. CN101111244B, 27 April 2011. [Google Scholar]
- Yanbin, W.; Jinzhong, W.; Shuxia, Z.; Jianguo, W. Method for Preparing Quercetin-3-O-beta-D-glucuronide from Lotus Seedpot. China Patent Application No. CN104817603A, 27 July 2018. [Google Scholar]
- Zhao, Y.; Yang, M.; Li, Y.; Luan, X.; Luo, Z. Quercetin Derivatives and Their Medical Usages. China Patent Application No. WO2002076473A1, 26 September 2003. [Google Scholar]
- Ahn, B.W.; Kim, Y.S.; Jeong, H.S.; Shin, S.K.; Kim, T.W.; Youm, S.Y. Composition for Promoting Hematogenesis Containing Quercetin 3-O-β-(2″-galloyl)-Rhamnopyranoside as Active Ingredient. WIPO (PCT) Patent Application No. US9289444B2, 22 March 2016. [Google Scholar]
- Gu, M.; Gao, L. Method for Synthesizing Agarose Gel Hydrogen Bond Adsorbing Chromatography Medium by Using Quercetin as Genin. China Patent Application No. CN101955514A, 27 February 2013. [Google Scholar]
- Lin, L.; Cai, C.; Zhu, Y. A Quercetin Type Surfactant, Its Preparation Method and Application. China Patent Application No. CN101982168A, 23 May 2012. [Google Scholar]
- Lines, T.C. Quercetin-Containing Composition, Methods of Making, and Methods of Using. WIPO (PCT) Patent Application No. WO2008011363A2, 24 January 2008. [Google Scholar]
- Habarov, V.N.; Ivanov, P.L. Bioactive Composition Based on a Cross-Linked Hyaluronic Acid Salt Containing Resveratrol and a Method of Its Preparation a Method for Its Preparation. Russia Patent Application No. RU2745124C1, 22 March 2021. [Google Scholar]
- Huang, Z.H. Application of Oncolytic Adenovirus Expressing TRAIL and Quercetin in Inhibition of Liver Cancer Cell Proliferation. China Patent Application No. CN106822085A, 17 March 2020. [Google Scholar]
- Zahedi, M.; Ghiasvand, R.; Feizi, A.; Asgari, G.; Darvish, L. Does quercetin improve cardiovascular risk factors and inflammatory biomarkers in women with type 2 diabetes: A double-blind randomized controlled clinical trial. Int. J. Prev. Med. 2013, 4, 777. [Google Scholar]
- Papakyriakopoulou, P.; Velidakis, N.; Khattab, E.; Valsami, G.; Korakianitis, I.; Kadoglou, N.P. Potential pharmaceutical applications of quercetin in cardiovascular diseases. Pharmaceuticals 2022, 15, 1019. [Google Scholar] [CrossRef]
- Conquer, J.A.; Maiani, G.; Azzini, E.; Raguzzini, A.; Holub, B.J. Supplementation with quercetin markedly increases plasma quercetin concentration without effect on selected risk factors for heart disease in healthy subjects. J. Nutr. 1998, 128, 593–597. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, R.; Tamtaji, O.R.; Mirhosseini, N.; Lankarani, K.B.; Akbari, M.; Heydari, S.T.; Dadgostar, E.; Asemi, Z. The effects of quercetin supplementation on lipid profiles and inflammatory markers among patients with metabolic syndrome and related disorders: A systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2020, 60, 1855–1868. [Google Scholar] [CrossRef] [PubMed]
- Egert, S.; Bosy-Westphal, A.; Seiberl, J.; Kürbitz, C.; Settler, U.; Plachta-Danielzik, S. Quercetin reduces systolic blood pressure and plasma oxidised low-density lipoprotein concentrations in overweight subjects with a high-cardiovascular disease risk. Br. J. Nutr. 2009, 102, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Park, E.; Lee, H.J.; Kim, M.O.; Cha, Y.J.; Kim, J.M.; Lee, H.; Shin, M.J. Effects of daily quercetin-rich supplementation on cardiometabolic risks in male smokers. Nutr. Res. Pract. 2011, 5, 28–33. [Google Scholar] [CrossRef]
- Pfeuffer, M.; Auinger, A.; Bley, U.; Kraus-Stojanowic, I.; Laue, C.; Winkler, P.; Rüfer, C.E.; Frank, J.; Bösch-Saadatmandi, C.; Rimbach, G.; et al. Effect of quercetin on traits of the metabolic syndrome, endothelial function and inflammation in men with different APOE isoforms. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 403–409. [Google Scholar] [CrossRef]
- Talirevic, E.; Sehovic, J. Quercetin in the treatment of dyslipidemia. Med. Arch. 2012, 66, 87. [Google Scholar] [CrossRef] [PubMed]
- Mazza, A.; Nicoletti, M.; Lenti, S.; Torin, G.; Rigatelli, G.; Fratter, A.; Pellizzato, M. Effectiveness and safety of nutraceutical compounds added to ezetimibe treatment in hypertensive and hyper–cholesterolemic subjects with statin–intolerance. J. Hypertens. 2021, 39, e371. [Google Scholar] [CrossRef]
- Menezes, R.; Rodriguez-Mateos, A.; Kaltsatou, A.; González-Sarrías, A.; Greyling, A.; Giannaki, C.; Andres-Lacueva, C.; Milenkovic, D.; Gibney, E.R.; Dumont, J.; et al. Impact of flavonols on cardiometabolic biomarkers: A meta-analysis of randomized controlled human trials to explore the role of inter-individual variability. Nutrients 2017, 9, 117. [Google Scholar] [CrossRef]
- Nishimura, M.; Muro, T.; Kobori, M.; Nishihira, J. Effect of daily ingestion of quercetin-rich onion powder for 12 weeks on visceral fat: A randomised, double-blind, placebo-controlled, parallel-group study. Nutrients 2019, 12, 91. [Google Scholar] [CrossRef]
- Burak, C.; Wolffram, S.; Zur, B.; Langguth, P.; Fimmers, R.; Alteheld, B.; Egert, S. Effect of alpha-linolenic acid in combination with the flavonol quercetin on markers of cardiovascular disease risk in healthy, non-obese adults: A randomized, double-blinded placebo-controlled crossover trial. Nutrition 2019, 58, 47–56. [Google Scholar] [CrossRef]
- Hickson, L.J.; Prata, L.G.L.; Bobart, S.A.; Evans, T.K.; Giorgadze, N.; Hashmi, S.K.; Herrmann, S.M.; Jensen, M.D.; Jia, Q.; Jordan, K.L.; et al. Senolytics decrease senescent cells in humans: Preliminary report from a clinical trial of Dasatinib plus Quercetin in individuals with diabetic kidney disease. EBioMedicine 2019, 47, 446–456. [Google Scholar] [CrossRef]
- Hezaveh, Z.S.; Azarkeivan, A.; Janani, L.; Hosseini, S.; Shidfar, F. The effect of quercetin on iron overload and inflammation in β-thalassemia major patients: A double-blind randomized clinical trial. Complement. Ther. Med. 2019, 46, 24–28. [Google Scholar] [CrossRef]
- Mohammadi-Sartang, M.; Mazloom, Z.; Sherafatmanesh, S.; Ghorbani, M.; Firoozi, D. Effects of supplementation with quercetin on plasma C-reactive protein concentrations: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Clin. Nutr. 2017, 71, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Javadi, F.; Ahmadzadeh, A.; Eghtesadi, S.; Aryaeian, N.; Zabihiyeganeh, M.; Rahimi Foroushani, A. The Effect of Quercetin on Inflammatory Factors and Clinical Symptoms in Women with Rheumatoid Arthritis: A Double-Blind, Randomized Controlled Trial. J. Am. Coll. Nutr. 2017, 36, 9–15. [Google Scholar] [CrossRef]
- Han, M.K.; Barreto, T.A.; Martinez, F.J.; Comstock, A.T.; Sajjan, U.S. Randomised clinical trial to determine the safety of quercetin supplementation in patients with chronic obstructive pulmonary disease. BMJ Open Respir. Res. 2020, 7, e000392. [Google Scholar] [CrossRef]
- Heinz, S.A.; Henson, D.A.; Austin, M.D.; Jin, F.; Nieman, D.C. Quercetin supplementation and upper respiratory tract infection: A randomized community clinical trial. Pharmacol. Res. 2010, 62, 237–242. [Google Scholar] [CrossRef]
- Ujjan, I.D.; Khan, S.; Nigar, R.; Ahmed, H.; Ahmad, S.; Khan, A. The possible therapeutic role of curcumin and quercetin in the early-stage of COVID-19—Results from a pragmatic randomized clinical trial. Front. Nutr. 2023, 9, 1023997. [Google Scholar] [CrossRef]
- Shohan, M.; Nashibi, R.; Mahmoudian-Sani, M.R.; Abolnezhadian, F.; Ghafourian, M.; Alavi, S.M.; Sharhani, A.; Khodadadi, A. The therapeutic efficacy of quercetin in combination with antiviral drugs in hospitalized COVID-19 patients: A randomized controlled trial. Eur. J. Pharmacol. 2022, 914, 174615. [Google Scholar] [CrossRef] [PubMed]
- Di Pierro, F.; Khan, A.; Iqtadar, S.; Mumtaz, S.U.; Chaudhry, M.N.A.; Bertuccioli, A.; Derosa, G.; Maffioli, P.; Togni, S.; Riva, A.; et al. Quercetin as a possible complementary agent for early-stage COVID-19: Concluding results of a randomized clinical trial. Front. Pharmacol. 2023, 13, 1096853. [Google Scholar] [CrossRef] [PubMed]
- Di Pierro, F.; Iqtadar, S.; Khan, A.; Ullah Mumtaz, S.; Masud Chaudhry, M.; Bertuccioli, A.; Derosa, G.; Maffioli, P.; Togni, S.; Riva, A.; et al. Potential clinical benefits of quercetin in the early stage of COVID-19: Results of a second, pilot, randomized, controlled and open-label clinical trial. Int. J. Gen. Med. 2021, 14, 2807–2816. [Google Scholar] [CrossRef]
- Rezvan, N.; Moini, A.; Gorgani-Firuzjaee, S.; Hosseinzadeh-Attar, M.J. Oral quercetin supplementation enhances adiponectin receptor transcript expression in polycystic ovary syndrome patients: A randomized placebo-controlled double-blind clinical trial. Cell J. 2018, 19, 627. [Google Scholar]
- Rezvan, N.; Moini, A.; Janani, L.; Mohammad, K.; Saedisomeolia, A.; Nourbakhsh, M. Effects of Quercetin on Adiponectin-Mediated Insulin Sensitivity in Polycystic Ovary Syndrome: A Randomized Placebo-Controlled Double-Blind Clinical Trial. Horm. Metab. Res. 2017, 49, 115–121. [Google Scholar] [CrossRef]
- Tabrizi, F.P.F.; Hajizadeh-Sharafabad, F.; Vaezi, M.; Jafari-Vayghan, H.; Alizadeh, M.; Maleki, V. Quercetin and polycystic ovary syndrome, current evidence and future directions: A systematic review. J. Ovarian Res. 2020, 13, 1–10. [Google Scholar] [CrossRef]
- Hussain, S.A.; Ahmed, Z.A.; Mahwi, T.O.; Aziz, T.A. Quercetin Dampens Postprandial Hyperglycemia in Type 2 Diabetic Patients Challenged with Carbohydrates Load. Int. J. Diabetes Res. 2012, 1, 32–35. [Google Scholar]
- Michala, A.S.; Pritsa, A. Quercetin: A molecule of great biochemical and clinical value and its beneficial effect on diabetes and cancer. Diseases 2022, 10, 37. [Google Scholar] [CrossRef]
- Mazloom, Z.; Abdollahzadeh, S.M.; Dabbaghmanesh, M.-H.; Rezaianzadeh, A. The effect of quercetin supplementation on oxidative stress, glycemic control, lipid profile and insulin resistance in type 2 diabetes: A randomized clinical trial. J. Health Sci. Surveill. Sys. 2014, 2, 8–14. [Google Scholar]
- Ostadmohammadi, V.; Milajerdi, A.; Ayati, E.; Kolahdooz, F. Effects of quercetin supplementation on glycemic control among patients with metabolic syndrome and related disorders: A systematic review and meta-analysis of randomized controlled trials. Phytother. Res. 2019, 33, 1330–1340. [Google Scholar] [CrossRef]
- Lee, J.S.; Cha, Y.J.; Lee, K.H.; Yim, J.E. Onion peel extract reduces the percentage of body fat in overweight and obese subjects: A 12-week, randomized, double-blind, placebo-controlled study. Nutr. Res. Pract. 2016, 10, 175–181. [Google Scholar] [CrossRef]
- Huang, H.; Liao, D.; Dong, Y.; Pu, R. Clinical effectiveness of quercetin supplementation in the management of weight loss: A pooled analysis of randomized controlled trials. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 553–563. [Google Scholar] [CrossRef]
- Dehghani, F.; Sezavar Seyedi Jandaghi, S.H.; Janani, L.; Sarebanhassanabadi, M.; Emamat, H.; Vafa, M. Effects of quercetin supplementation on inflammatory factors and quality of life in post-myocardial infarction patients: A double blind, placebo-controlled, randomized clinical trial. Phytother. Res. 2021, 35, 2085–2098. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.L.; Lyon, T.; Litwin, S.E.; Rabovsky, A.; Symons, J.D.; Jalili, T. Quercetin reduces blood pressure in hypertensive subjects. J. Nutr. 2007, 137, 2405–2411. [Google Scholar] [CrossRef]
- Huang, H.; Liao, D.; Dong, Y.; Pu, R. Effect of quercetin supplementation on plasma lipid profiles, blood pressure, and glucose levels: A systematic review and meta-analysis. Nutr. Rev. 2020, 78, 615–626. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Li, L.; Pan, X.; Wang, J.; Qi, Q.; Sun, H. The effect of a traditional Chinese quadri-combination therapy and its component quercetin on recurrent spontaneous abortion: A clinical trial, network pharmacology and experiments-based study. Front. Pharmacol. 2022, 13, 965694. [Google Scholar] [CrossRef] [PubMed]
- Pasdar, Y.; Oubari, F.; Zarif, M.N.; Abbasi, M.; Pourmahmoudi, A.; Hosseinikia, M. Effects of quercetin supplementation on hematological parameters in non-alcoholic fatty liver disease: A randomized, double-blind, placebo-controlled pilot study. Clin. Nutr. Res. 2020, 9, 11–19. [Google Scholar] [CrossRef]
- Kooshyar, M.M.; Mozafari, P.M.; Amirchaghmaghi, M.; Pakfetrat, A.; Karoos, P.; Mohasel, M.R.; Orafai, H.; Azarian, A.A. A randomized placebo-controlled double blind clinical trial of quercetin in the prevention and treatment of chemotherapy-induced oral mucositis. J. Clin. Diagn. Res. JCDR 2017, 11, ZC46. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Ma, J.; Lei, P.; Yi, J.; Ma, Y.; Huang, Z.; Wang, T.; Ping, H.; Ruan, D.; Sun, D.; et al. Advances in Antioxidant Applications for Combating 131I Side Effects in Thyroid Cancer Treatment. Toxics 2023, 11, 529. [Google Scholar] [CrossRef]
- Dagher, O.; Mury, P.; Noly, P.E.; Fortier, A.; Lettre, G.; Thorin, E.; Carrier, M. Design of a randomized placebo-controlled trial to evaluate the anti-inflammatory and senolytic effects of quercetin in patients undergoing coronary artery bypass graft surgery. Front. Cardiovasc. Med. 2021, 8, 741542. [Google Scholar] [CrossRef]
- Kim, K.A.; Yim, J.E. The effect of onion peel extract on inflammatory mediators in Korean overweight and obese women. Clin. Nutr. Res. 2016, 5, 261–269. [Google Scholar] [CrossRef]
- Hussain, S.A.; Ahmed, Z.A.; Mahwi, T.O.; Aziz, T.A.; Hussain, S.A.; Ahmed, Z.A. Effect of quercetin on postprandial glucose excursion after mono-and disaccharides challenge in normal and diabetic rats. J. Diabetes Mellit. 2012, 2, 82–87. [Google Scholar] [CrossRef]
- Lu, T.M.; Chiu, H.F.; Shen, Y.C.; Chung, C.C.; Venkatakrishnan, K.; Wang, C.K. Hypocholesterolemic Efficacy of Quercetin Rich Onion Juice in Healthy Mild Hypercholesterolemic Adults: A Pilot Study. Plant Foods Hum. Nutr. 2015, 70, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Van Den Eynde, M.D.G.; Geleijnse, J.M.; Scheijen, J.L.J.M.; Hanssen, N.M.J.; Dower, J.I.; Afman, L.A. Quercetin, but Not Epicatechin, Decreases Plasma Concentrations of Methylglyoxal in Adults in a Randomized, Double-Blind, Placebo-Controlled, Crossover Trial with Pure Flavonoids. J. Nutr. 2018, 148, 1911–1916. [Google Scholar] [CrossRef] [PubMed]
- Dinç, E.; Üçer, A.; Ünal, N. Three-dimensional strategies in the quantitative resolution of kinetic UV absorbance measurements for monitoring the oxidation of quercetin by oxidant agents and analyzing dietary supplement product. J. Food Drug Anal. 2023, 31, 326. [Google Scholar] [CrossRef] [PubMed]
- Mehnert, W.; Mäder, K. Solid lipid nanoparticles: Production, characterization and applications. Adv. Drug Deliv. Rev. 2012, 64, 83–101. [Google Scholar] [CrossRef]
- Joye, I.J.; Davidov-Pardo, G.; McClements, D.J. Nanotechnology for increased micronutrient bioavailability. Trends Food Sci. Technol. 2014, 40, 168–182. [Google Scholar] [CrossRef]
- Li, H.; Zhao, X.; Ma, Y.; Zhai, G.; Li, L.; Lou, H. Enhancement of gastrointestinal absorption of quercetin by solid lipid nanoparticles. J. Control. Release 2009, 133, 238–244. [Google Scholar] [CrossRef]
- Bose, S.; Du, Y.; Takhistov, P.; Michniak-Kohn, B. Formulation optimization and topical delivery of quercetin from solid lipid based nanosystems. Int. J. Pharm. 2013, 441, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Varshosaz, J.; Jafarian, A.; Salehi, G.; Zolfaghari, B. Comparing different sterol containing solid lipid nanoparticles for targeted delivery of quercetin in hepatocellular carcinoma. J. Liposome Res. 2014, 24, 191–203. [Google Scholar] [CrossRef]
- Üner, M. Preparation, characterization and physico-chemical properties of solid lipid nanoparticles (SLN) and nanostructured lipid carriers (NLC): Their benefits as colloidal drug carrier systems. Die Pharm. Int. J. Pharm. Sci. 2006, 61, 375–386. [Google Scholar]
- Zhang, X.; Pan, W.; Gan, L.; Zhu, C.; Gan, Y.; Nie, S. Preparation of a dispersible PEGylate nanostructured lipid carriers (NLC) loaded with 10-hydroxycamptothecin by spray-drying. Chem. Pharm. Bull. 2008, 56, 1645–1650. [Google Scholar] [CrossRef] [PubMed]
- Khursheed, R.; Singh, S.K.; Wadhwa, S.; Gulati, M.; Awasthi, A. Enhancing the potential preclinical and clinical benefits of quercetin through novel drug delivery systems. Drug Discov. Today 2020, 25, 209–222. [Google Scholar] [CrossRef] [PubMed]
- Wanga, S.; Sua, R.; Niea, S.; Suna, M.; Zhanga, J.; Wub, D.; Moustaid-Moussaa, N. Application of nanotechnology in improving bioavailability and bioactivity of dietderived phytochemicals. J. Nutr. Biochem. 2014, 25, 363–376. [Google Scholar] [CrossRef] [PubMed]
- Du, M.; Ouyang, Y.; Meng, F.; Ma, Q.; Liu, H.; Zhuang, Y. Nanotargeted agents: An emerging therapeutic strategy for breast cancer. Nanomedicine 2019, 14, 1771–1786. [Google Scholar] [CrossRef]
- Mallya, R.; Patil, K. Recent Developments in Formulation Design of a Multifunctional Phytochemical Quercetin: A Review. Pharmacogn. Rev. 2021, 15, 32–46. [Google Scholar] [CrossRef]
- Mignet, N.; Seguin, J.; Romano, M.R.; Brullé, L.; Touil, Y.S.; Scherman, D.; Bessodes, M.; Chabot, G.G. Development of a liposomal formulation of the natural flavonoid fisetin. Int. J. Pharm. 2012, 423, 69–76. [Google Scholar] [CrossRef]
- Landi-Librandil, A.P.; Chrysostomol, T.N.; Caleiro Seixas Azzolini, A.E.; Marzocchi-Machado, C.M.; De Oliveira, C.A.; Lucisano-Valim, Y.M. Study of quercetin-loaded liposomes as potential drug carriers: In Vitro evaluation of human complement activation. J. Liposome Res. 2012, 22, 89–99. [Google Scholar] [CrossRef]
- Tefas, L.R.; Muntean, D.M.; Vlase, L.; Porfire, A.S.; Achim, M.; Tomuță, I. Quercetin-loaded liposomes: Formulation optimization through a D-optimal experimental design. Farmacia 2015, 63, 126–133. [Google Scholar]
- Siler-Marinkovic, S. Liposomes as drug delivery systems in dermal and transdermal drug delivery. In Percutaneous Penetration Enhancers Chemical Methods in Penetration Enhancement: Nanocarriers; Springer: Berlin/Heidelberg, Germany, 2016; pp. 15–38. [Google Scholar]
- Cai, X.; Fang, Z.; Dou, J.; Yu, A.; Zhai, G. Bioavailability of quercetin: Problems and promises. Curr. Med. Chem. 2013, 20, 2572–2582. [Google Scholar] [CrossRef] [PubMed]
- Saraswat, A.L.; Maher, T.J. Development and optimization of stealth liposomal system for enhanced in vitro cytotoxic effect of quercetin. J. Drug Deliv. Sci. Technol. 2020, 55, 101477. [Google Scholar] [CrossRef]
- Ahmed, H.M.; Nabavi, S.; Behzad, S. Herbal drugs and natural products in the light of nanotechnology and nanomedicine for developing drug formulations. Mini Rev. Med. Chem. 2021, 21, 302–313. [Google Scholar] [CrossRef]
- Javani, R.; Hashemi, F.S.; Ghanbarzadeh, B.; Hamishehkar, H. Quercetin-loaded niosomal nanoparticles prepared by the thin-layer hydration method: Formulation development, colloidal stability, and structural properties. LWT 2021, 141, 110865. [Google Scholar] [CrossRef]
- Muzzalupo, R.; Tavano, L. Niosomal drug delivery for transdermal targeting: Recent advances. Res. Rep. Transdermal Drug Deliv. 2015, 4, 23–33. [Google Scholar] [CrossRef]
- Tangri, P.; Khurana, S. Niosomes: Formulation and evaluation. Int. J. 2011, 2229, 7499. [Google Scholar]
- Kazi, K.M.; Mandal, A.S.; Biswas, N.; Guha, A.; Chatterjee, S.; Behera, M.; Kuotsu, K. Niosome: A future of targeted drug delivery systems. J. Adv. Pharm. Technol. Res. 2010, 1, 374. [Google Scholar]
- Lu, B.; Huang, Y.; Chen, Z.; Ye, J.; Xu, H.; Chen, W.; Long, X. Niosomal nanocarriers for enhanced skin delivery of quercetin with functions of anti-tyrosinase and antioxidant. Molecules 2019, 24, 2322. [Google Scholar] [CrossRef]
- Bhardwaj, V.; Shukla, V.; Singh, A.; Malviya, R.; Sharma, P.K. Transfersomes ultra flexible vesicles for transdermal delivery. Int. J. Pharm. Sci. Res. 2010, 1, 12–20. [Google Scholar]
- Pandit, A.P.; Omase, S.B.; Mute, V.M. A chitosan film containing quercetin-loaded transfersomes for treatment of secondary osteoporosis. Drug Deliv. Transl. Res. 2020, 10, 1495–1506. [Google Scholar] [CrossRef] [PubMed]
- Opatha, S.A.T.; Titapiwatanakun, V.; Chutoprapat, R. Transfersomes: A promising nanoencapsulation technique for transdermal drug delivery. Pharmaceutics 2020, 12, 855. [Google Scholar] [CrossRef] [PubMed]
- Sapkota, R.; Dash, A.K. Liposomes and transferosomes: A breakthrough in topical and transdermal delivery. Ther. Deliv. 2021, 12, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S. Sarangdevot. K. Nanoemulsions for cosmetics. Int. J. Adv. Res. Biol. Sci. 2012, 2, 408–415. [Google Scholar]
- Craig, D.; Siddiqui, A.; Jain, P.; Santosh, A.T.; Asgar, A.M.; Hassan, N.; Hannef, J.; Naseef, P.P.; Kuruniyan, M.S.; Mirza, M.A.; et al. Investigation of a Minocycline-Loaded Nanoemulgel for the Treatment of Acne Rosacea. Pharmaceutics 2022, 14, 2322. [Google Scholar]
- Yukuyama, M.N.; Ghisleni, D.D.M.; Pinto, T.D.J.A.; Bou-Chacra, N.A. Nanoemulsion: Process selection and application in cosmetics–a review. Int. J. Cosmet. Sci. 2016, 38, 13–24. [Google Scholar] [CrossRef]
- Arbain, N.H.; Salim, N.; Masoumi, H.R.F.; Wong, T.W.; Basri, M.; Abdul Rahman, M.B. In vitro evaluation of the inhalable quercetin loaded nanoemulsion for pulmonary delivery. Drug Deliv. Transl. Res. 2019, 9, 497–507. [Google Scholar] [CrossRef]
- Zorzi, G.K.; Caregnato, F.; Moreira, J.C.F.; Teixeira, H.F.; Carvalho, E.L.S. Antioxidant Effect of Nanoemulsions Containing Extract of Achyrocline satureioides (Lam) D.C.—Asteraceae. AAPS PharmSciTech 2016, 17, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Akhtar, S.; Yadav, Y.; Atiya, A.; Alelwani, W.; Bannunah, A.M.; Mahmood, S. Lopinavir-Loaded Self-Nanoemulsifying Drug Delivery System for Enhanced Solubility: Development, Characterisation and Caco-2 Cell Uptake. Curr. Drug Deliv. 2023, 20, 1474–1486. [Google Scholar] [CrossRef] [PubMed]
- Alireza, S.; Mina, R.F. Solvent effect on the size of platinum nanoparticle synthesized in microemulsion systems. Russ. J. Phys. Chem. A 2012, 86, 981. [Google Scholar]
- Mandavi, N.; Ansari, N.; Bharti, R.; Kader, N.; Sahu, G.K.; Sharma, H. Microemulsion: A Potential Novel Drug Delivery System. Res. J. Pharm. Dos. Forms Technol. 2018, 10, 266–271. [Google Scholar] [CrossRef]
- Gao, Z.G. Thermal reversible microemulsion for oral delivery of poorly water-soluble drugs. In Microemulsions-An Introduction to Properties and Applications; IntechOpen: Rijeka, Croatia, 2012. [Google Scholar]
- Vicentini, F.T.; Fonseca, Y.M.; Pitol, D.L.; Iyomasa, M.M.; Bentley, M.V.L.; Fonseca, M.J. Evaluation of protective effect of a water-in-oil microemulsion incorporating quercetin against UVB-induced damage in hairless mice skin. J. Pharm. Pharm. Sci. 2010, 13, 274–285. [Google Scholar] [CrossRef] [PubMed]







| Biological Source | Genus | Species | Authorship | Specified Parts | Concentration | Reference |
|---|---|---|---|---|---|---|
| Onion (A. cepa L.) | Allium | A. cepa | Carl Linnaeus, 1753 | Bulb | 79–431 mg/kg of fresh weight | [13] |
| Apple (Malus Domestica S.) | Malus | M. domestica | 1300 BC | Pomace (peel, pulp, and seeds) | 1.61 g kg−1 DM | [14] |
| Green tea (Camellia Sinensis L.) | Camellia | C. sinensis | Shen Nong, 2700 BC | Leaf extract | 10–70 μg/mL | [15] |
| Grape (V. vinifera L.) | Vitis | V. vinifera | Caucasus region of Eurasia, 6000 BC | Peel extract | 0.45−57.6 μg/mL | [16] |
| Blueberry (Vaccinium corymbosum L.) | Vaccinium | V. corymbosum | Carl Linnaeus in 1753 | Fruit | 59.4% ± 8.7% w/w | [17] |
| Cranberry (Vaccinium Macrocarpon Aiton.) | Vaccinium | V. macrocarpon | James Gordon in 1760 | Pomace | 146.2 mg/100 g of dry weight | [18] |
| Broccoli (Brassica Oleracea L.) | Brassica | B. oleracea | 2000 BC | Whole vegetable | 0.03 to 10.85 mg/100 g of fresh weight | [19] |
| Chinese plum (Prunus salicina L.) | Prunus | P. salicina | China in 470 BC | Fruit | 32.7 mg/100 g of dry weight | [20] |
| Buckwheat (Fagopyrum esculentum Moench.) | Fagopyrum | F. esculentum | 2600 BC | Seed | 0.09–3 mg/g of fresh weight | [21] |
| Mulberry (Morus alba L.) | Morus | M. alba | 220 BC | Leaf | 0.452 g/100 g of dry weight. | [22] |
| Moringa oleifera L. | Moringa. | M. oleifera | Jean-Baptiste Lamarck in 1785 | Leaf extract | 5 to 2000 mg/mL | [23] |
| Rapinus sativus L. | Rapinus | R. sativus | Western Europe in 16th century | Leaf extract | 5 to 2000 mg/mL | [24] |
| Curcuma angustifolia Roxb. | Curcuma | C. angustifolia | China in 700 BC | Leaf | 4.5 µg/mg of fresh weight | [25] |
| Centella asiatica L. | Centella | C. asiatica | Southeast Asian countries | Leaf | Reported (not quantified) | [25] |
| Asparagus officinalis L. | Asparagus | A. officinalis | Root extract | 150 mg/mL | [26] | |
| Coriandrum sativum L. | Coriandrum | C. sativum | Carl Linnaeus in 1753 | Methanolic extract | 103.81 ± 4.76 mg kg−1 | [27] |
| Lactuca sativa L. | Lactuca | L. sativa | Carl Linnaeus in 1753 | Leaf | Reported (not quantified) | [28] |
| Mechanism of Action in Prostate Cancer | Reference |
|---|---|
| I. Inhibition of proliferation | [36] |
| Induction of G0/G1 (31.4–49.7%) and sub-G1 (19.77%) cell cycle arrest, which is caused by downregulation of cyclin D and E, CDK2, and cdc25c and upregulation of p21, p53, p18, and p27 in PC-3 and LNCaP cell lines. | |
| II. Induction of apoptosis | [38] |
| Increasing pro-apoptotic Bax and by decreasing anti-apoptotic Bcl-2 protein results in a significant decrease in the Bcl-2/Bax ratio. | |
| III. Inhibition of the androgen receptor (AR) | [41] |
| (i) Retardation of DNA synthesis and modulation of the AR signaling pathway. (ii) Reduced expression of AR and then increased caspase-3/-7 causing subsequent anti-proliferation and apoptosis in LNCaP cells. | |
| IV. Inhibition of angiogenesis | [43] |
| This was caused by a deleterious effect on the AKT/mTOR/P70S6K pathway. Quercetin decreases angiogenesis in LNCaP cells by lowering HIF-1α accumulation and VEGF release. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mirza, M.A.; Mahmood, S.; Hilles, A.R.; Ali, A.; Khan, M.Z.; Zaidi, S.A.A.; Iqbal, Z.; Ge, Y. Quercetin as a Therapeutic Product: Evaluation of Its Pharmacological Action and Clinical Applications—A Review. Pharmaceuticals 2023, 16, 1631. https://doi.org/10.3390/ph16111631
Mirza MA, Mahmood S, Hilles AR, Ali A, Khan MZ, Zaidi SAA, Iqbal Z, Ge Y. Quercetin as a Therapeutic Product: Evaluation of Its Pharmacological Action and Clinical Applications—A Review. Pharmaceuticals. 2023; 16(11):1631. https://doi.org/10.3390/ph16111631
Chicago/Turabian StyleMirza, Mohd Aamir, Syed Mahmood, Ayah Rebhi Hilles, Abuzer Ali, Mohammed Zaafar Khan, Syed Amir Azam Zaidi, Zeenat Iqbal, and Yi Ge. 2023. "Quercetin as a Therapeutic Product: Evaluation of Its Pharmacological Action and Clinical Applications—A Review" Pharmaceuticals 16, no. 11: 1631. https://doi.org/10.3390/ph16111631