
Comprehensive Observational Study in a Large Cohort of Asthma Patients after Adding LAMA to ICS/LABA
 , , and
, , and
Abstract
:1. Introduction
2. Results
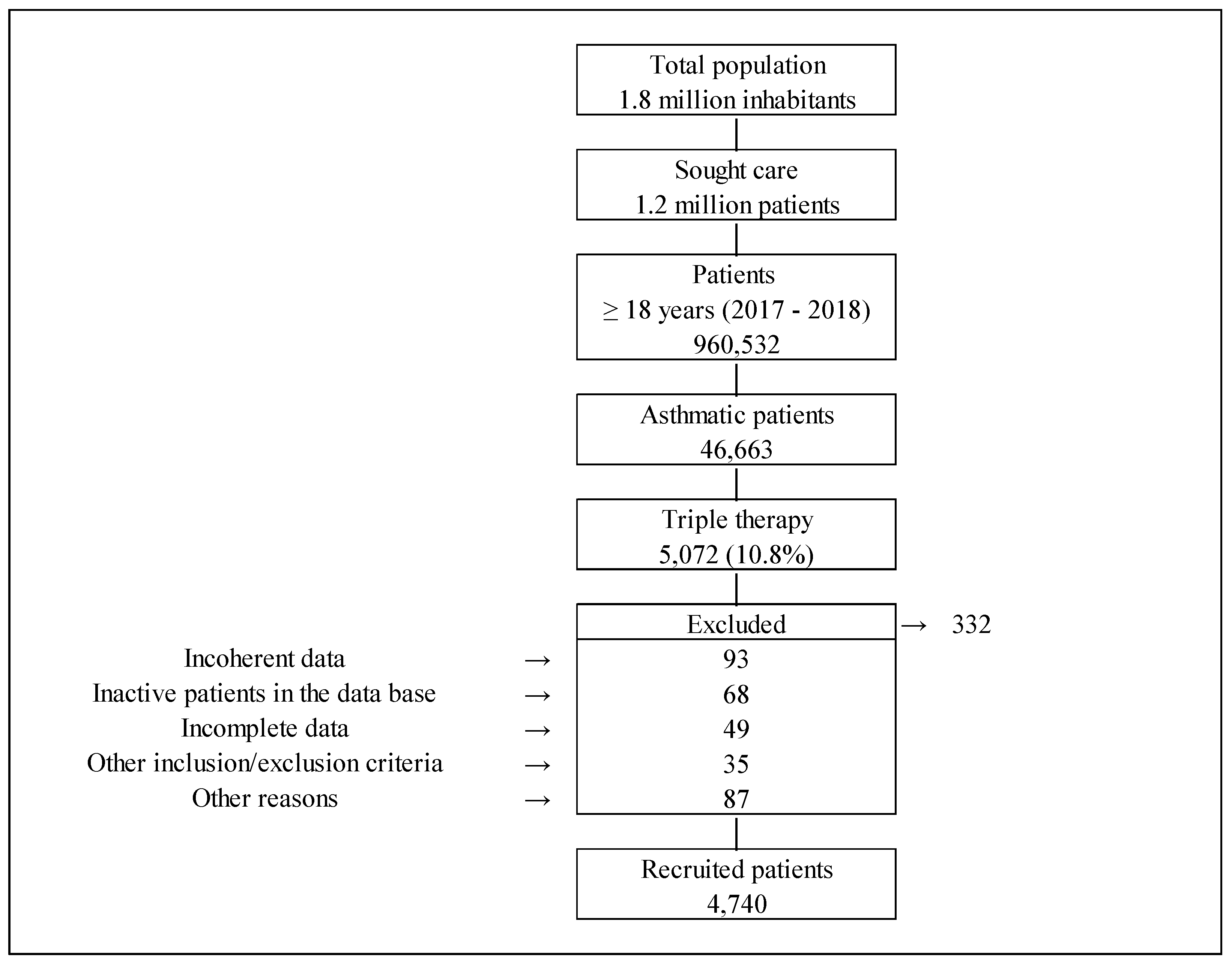
2.1. Study Population
2.2. Treatments
2.3. Clinical Outcomes and Deaths
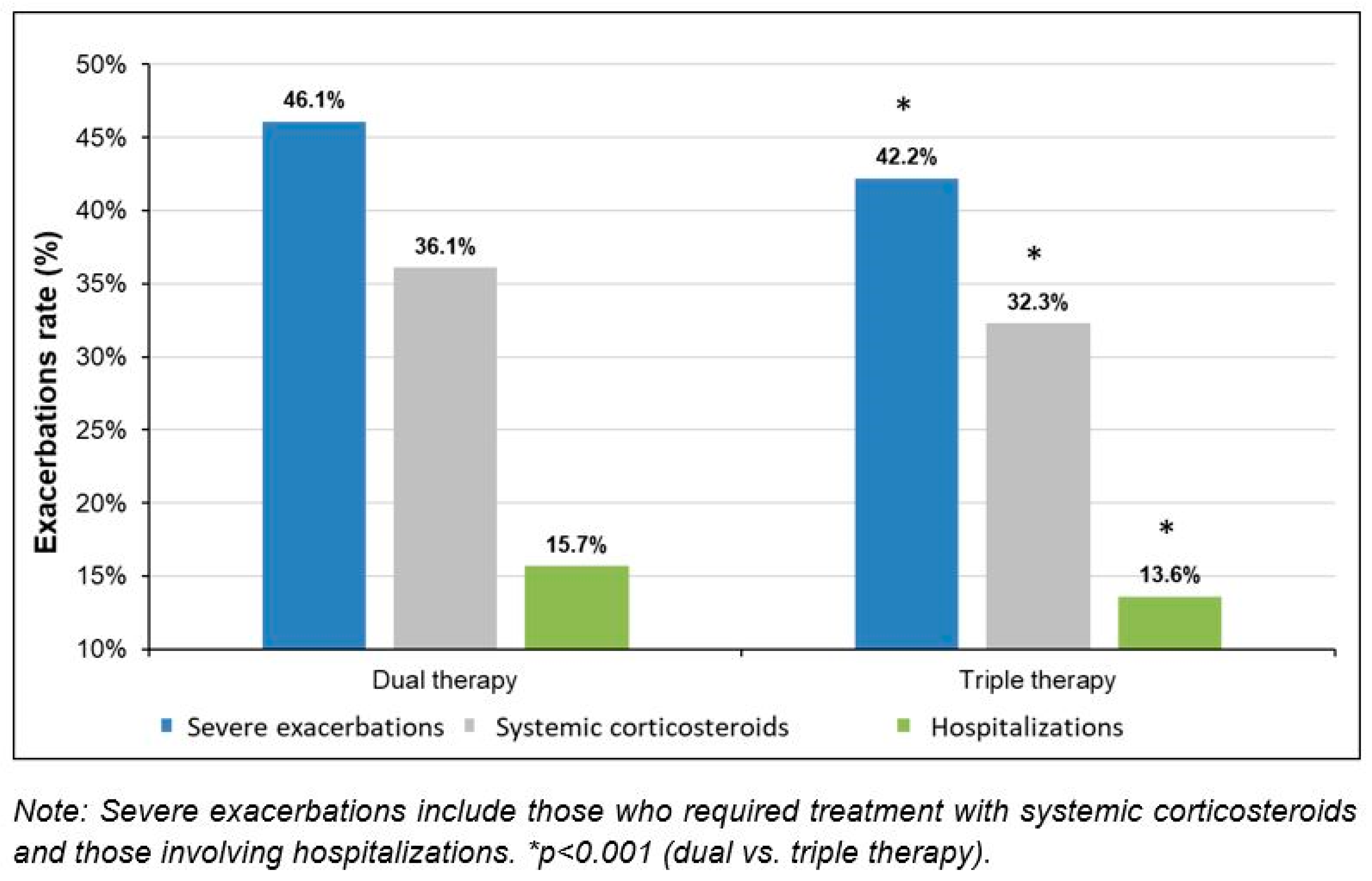
2.3.1. Severe Exacerbations and Deaths
2.3.2. Lung Function and Eosinophil Counts
2.4. Use of Healthcare Resources and Costs
3. Discussion
4. Materials and Methods
4.1. Study Population and Design
4.2. Demographic Variables, Comorbidities, and Treatments
4.3. Clinical Outcomes and Deaths
4.4. Resource Use and Costs
4.5. Statistical Analyses
4.6. Compliance with Ethics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Initiative for Asthma (GINA). Global Strategy for Asthma Management. 2020. Available online: https://ginasthma.org/wp-content/uploads/2020/04/GINA-2020-full-report_-final-_wms.pdf (accessed on 19 April 2023).
- Ntontsi, P.; Photiades, A.; Zervas, E.; Xanthou, G.; Samitas, K. Genetics and Epigenetics in Asthma. Int. J. Mol. Sci. 2021, 22, 2412. [Google Scholar] [CrossRef]
- Clausing, E.S.; Tomlinson, C.J.; Non, A.L. Epigenetics and Social Inequalities in Asthma and Allergy. J. Allergy Clin. Immunol. 2023, 151, 1468–1470. [Google Scholar] [CrossRef]
- Soriano, J.B.; Kendrick, P.J.; Paulson, K.R.; Gupta, V.; Abrams, E.M.; Adedoyin, R.A.; Adhikari, T.B.; Advani, S.M.; Agrawal, A.; Ahmadian, E.; et al. Prevalence and Attributable Health Burden of Chronic Respiratory Diseases, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef] [PubMed]
- Gibson, G.J.; Loddenkemper, R.; Sibille, Y.; Lundbäck, B.; Fletcher, M. Lung Health in Europe. Facts & Figures: A Better Understanding of Lung Disease and Respiratory Care in Europe; European Lung Foundation (ELF): Sheffield, UK, 2023; ISBN 978-1-84984-058-3. [Google Scholar]
- Khan, A.; Sternbach, N.; Kamat, S.; Annunziata, K.; Jaffe, D.; Gouia, I. Prevalence of Asthma in France, Germany, Italy, Spain and the United Kingdom, Based on the 2018 European National Health and Wellness Survey. Chest 2020, 158, A27. [Google Scholar] [CrossRef]
- GEMA 5.0. Guía Española Para El Manejo del Asma. 2020. ISBN 978-84-17372-97-2. Available online: https://www.semg.es/images/documentos/GEMA_5.0.pdf (accessed on 14 March 2022).
- Gómez Sáenz, J.T.; Gérez Callejas, M.J.; Hidalgo Requena, A.; Ginel Mendoza, L.; González Aguilera, J.; Quintano Jiménez, J.A. Mortalidad por asma en España, 1990–2015. Med. Fam. Semer. 2019, 45, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Metrics and Evaluation (IHME) GBD Comparison. Available online: http://vizhub.healthdata.org/gbd-compare (accessed on 21 July 2021).
- Global Burden Disease Causes of Death Collaborators. Global, Regional, and National Age-Sex-Specific Mortality for 282 Causes of Death in 195 Countries and Territories, 1980-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [PubMed]
- Global Burden Disease 2019 and Diseases Injuries Collaborators. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Sicras-Mainar, A.; Capel, M.; Navarro-Artieda, R.; Nuevo, J.; Orellana, M.; Resler, G. Real-Life Retrospective Observational Study to Determine the Prevalence and Economic Burden of Severe Asthma in Spain. J. Med. Econ. 2020, 23, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Melero Moreno, C.; Quirce, S.; Huerta, A.; Uría, E.; Cuesta, M. Economic Impact of Severe Asthma in Spain: Multicentre Observational Longitudinal Study. J. Asthma 2019, 56, 861–871. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Moragón, E.; Serra-Batllés, J.; De Diego, A.; Palop, M.; Casan, P.; Rubio-Terrés, C.; Pellicer, C. Economic Cost of Treating the Patient with Asthma in Spain: The AsmaCost Study. Arch. Bronconeumol. 2009, 45, 481–486. [Google Scholar] [CrossRef]
- Golam, S.M.; Janson, C.; Beasley, R.; FitzGerald, J.M.; Harrison, T.; Chipps, B.; Hughes, R.; Müllerová, H.; Olaguibel, J.M.; Rapsomaniki, E.; et al. The Burden of Mild Asthma: Clinical Burden and Healthcare Resource Utilisation in the NOVELTY Study. Respir. Med. 2022, 200, 106863. [Google Scholar] [CrossRef]
- Papi, A.; Brightling, C.; Pedersen, S.E.; Reddel, H.K. Asthma. Lancet 2018, 391, 783–800. [Google Scholar] [CrossRef]
- Côté, A.; Godbout, K.; Boulet, L.P. The Management of Severe Asthma in 2020. Biochem. Pharmacol. 2020, 179, 114112. [Google Scholar] [CrossRef]
- Cazzola, M.; Rogliani, P.; Ora, J.; Calzetta, L.; Matera, M.G. Asthma and Comorbidities: Recent Advances. Pol. Arch. Intern. Med. 2022, 132, 16250. [Google Scholar] [CrossRef] [PubMed]
- Bruurs, M.L.J.; van der Giessen, L.J.; Moed, H. The Effectiveness of Physiotherapy in Patients with Asthma: A Systematic Review of the Literature. Respir. Med. 2013, 107, 483–494. [Google Scholar] [CrossRef]
- Virchow, J.C.; Kuna, P.; Paggiaro, P.; Papi, A.; Singh, D.; Corre, S.; Zuccaro, F.; Vele, A.; Kots, M.; Georges, G.; et al. Single Inhaler Extrafine Triple Therapy in Uncontrolled Asthma (TRIMARAN and TRIGGER): Two Double-Blind, Parallel-Group, Randomised, Controlled Phase 3 Trials. Lancet 2019, 394, 1737–1749. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Virchow, J.C.; Canonica, G.W.; Vele, A.; Kots, M.; Georges, G.; Papi, A. Extrafine Triple Therapy in Patients with Asthma and Persistent Airflow Limitation. Eur. Respir. J. 2020, 56, 2000476. [Google Scholar] [CrossRef] [PubMed]
- Kotoulas, S.C.; Tsiouprou, I.; Domvri, K.; Ntontsi, P.; Pataka, A.; Porpodis, K. Open and Closed Triple Inhaler Therapy in Patients with Uncontrolled Asthma. Adv. Respir. Med. 2023, 91, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Moulton, B.C.; Fryer, A.D. Muscarinic Receptor Antagonists, from Folklore to Pharmacology; Finding Drugs That Actually Work in Asthma and COPD. Br. J. Pharmacol. 2011, 163, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.A.; Bailes, Z.; Barnes, N.; Boulet, L.-P.; Edwards, D.; Fowler, A.; Hanania, N.A.; Kerstjens, H.A.M.; Kerwin, E.; Nathan, R.; et al. Efficacy and Safety of Once-Daily Single-Inhaler Triple Therapy (FF/UMEC/VI) versus FF/VI in Patients with Inadequately Controlled Asthma (CAPTAIN): A Double-Blind, Randomised, Phase 3A Trial. Lancet Respir. Med. 2021, 9, 69–84. [Google Scholar] [CrossRef]
- Kim, L.H.Y.; Saleh, C.; Whalen-Browne, A.; O’Byrne, P.M.; Chu, D.K. Triple vs Dual Inhaler Therapy and Asthma Outcomes in Moderate to Severe Asthma: A Systematic Review and Meta-Analysis. JAMA 2021, 325, 2466–2479. [Google Scholar] [CrossRef]
- Rogliani, P.; Ritondo, B.L.; Calzetta, L. Triple Therapy in Uncontrolled Asthma: A Network Meta-Analysis of Phase III Studies. Eur. Respir. J. 2021, 58, 2004233. [Google Scholar] [CrossRef]
- Suzuki, T.; Fairburn-Beech, J.; Sato, K.; Kaise, T. Clinical Characteristics, Treatment Patterns, Disease Burden, and Persistence/Adherence in Patients with Asthma Initiating Inhaled Triple Therapy: Real-World Evidence from Japan. Curr. Med. Res. Opin. 2020, 36, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- Chipps, B.; Mosnaim, G.; Mathur, S.K.; Shaikh, A.; Khoury, S.; Gopalan, G.; Palli, S.R.; Lamerato, L.; Casciano, J.; Dotiwala, Z.; et al. Add-on Tiotropium versus Step-up Inhaled Corticosteroid plus Long-Acting Beta-2-agonist in Real-World Patients with Asthma. Allergy Asthma Proc. 2020, 41, 248–255. [Google Scholar] [CrossRef]
- Muiser, S.; Gosens, R.; van den Berge, M.; Kerstjens, H.A.M. Understanding the Role of Long-Acting Muscarinic Antagonists in Asthma Treatment. Ann. Allergy Asthma Immunol. 2022, 128, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Price, D.; Kaplan, A.; Jones, R.; Freeman, D.; Burden, A.; Gould, S.; von Ziegenweidt, J.; Ali, M.; King, C.; Thomas, M. Long-Acting Muscarinic Antagonist Use in Adults with Asthma: Real-Life Prescribing and Outcomes of Add-on Therapy with Tiotropium Bromide. J. Asthma Allergy 2015, 8, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Cheng, W.-C.; Wu, B.-R.; Liao, W.-C.; Chen, C.-Y.; Chen, W.-C.; Hsia, T.-C.; Tu, C.-Y.; Chen, C.-H.; Hsu, W.-H. Clinical Predictors of the Effectiveness of Tiotropium in Adults with Symptomatic Asthma: A Real-Life Study. J. Thorac. Dis. 2018, 10, 3661–3669. [Google Scholar] [CrossRef]
- Van Dijk, B.C.P.; Svedsater, H.; Heddini, A.; Nelsen, L.; Balradj, J.S.; Alleman, C. Relationship between the Asthma Control Test (ACT) and Other Outcomes: A Targeted Literature Review. BMC Pulm. Med. 2020, 20, 79. [Google Scholar] [CrossRef] [PubMed]
- Domınguez-Ortega, J.; Mullol, J.; Alvarez Gutierrez, F.J.; Miguel-Blanco, C.; Castillo, J.A.; Olaguibel, J.M.; Blanco-Aparicio, M. The Effect of Biologics in Lung Function and Quality of Life of Patients with United Airways Disease: A Systematic Review. J. Allergy Clin. Immunol. Glob. 2023, 3, 100174. [Google Scholar] [CrossRef] [PubMed]
- La Mantia, I.; Ragusa, M.; Grigaliute, E.; Cocuzza, S.; Radulesco, T.; Calvo-Henriquez, C.; Saibene, A.M.; Riela, P.M.; Lechien, J.R.; Fakhry, N.; et al. Sensibility, Specificity, and Accuracy of the Sinonasal Outcome Test 8 (SNOT-8) in Patients with Chronic Rhinosinusitis (CRS): A Cross-Sectional Cohort Study. Eur. Arch. Otorhinolaryngol. 2023, 280, 3259–3264. [Google Scholar] [CrossRef]
- Antonino, M.; Nicolò, M.; Jerome Renee, L.; Federico, M.; Chiara, V.; Stefano, S.; Maria, S.; Salvatore, C.; Antonio, B.; Calvo-Henriquez, C.; et al. Single-Nucleotide Polymorphism in Chronic Rhinosinusitis: A Systematic Review. Clin. Otolaryngol. 2022, 47, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Gomez, J.L. Epigenetics in Asthma. Curr. Allergy Asthma Rep. 2019, 19, 56. [Google Scholar] [CrossRef] [PubMed]
- Stikker, B.S.; Hendriks, R.W.; Stadhouders, R. Decoding the Genetic and Epigenetic Basis of Asthma. Allergy 2023, 78, 940–956. [Google Scholar] [CrossRef] [PubMed]
- Rathod, A.; Rathod, R.; Zhang, H.; Rahimabad, P.K.; Karmaus, W.; Arshad, H. Association of Asthma and Rhinitis with Epigenetics of Coronavirus Related Genes. Epigenet. Insights 2021, 14, 25168657211039224. [Google Scholar] [CrossRef]
- European Network of Centres for Pharmacoepidemiology and Pharmacovigilance Big-Pac. Available online: http://www.encepp.eu/encepp/viewResource.htm?id=29236 (accessed on 13 April 2021).
- Sicras-Mainar, A.; Enriquez, J.L.; Hernández, I.; Sicras-Navarro, A.; Aymerich, T.; Leon, M. PMU146 Validation and Representativeness of the Spanish BIG-PAC Database: Integrated Computerized Medical Records for Research into Epidemiology, Medicines and Health Resource Use (Real World Evidence). Value Health 2019, 22, S734. [Google Scholar] [CrossRef]
- Sicras-Mainar, A.; Sicras Navarro, A.; Enríquez, J.L.; Hernández, I.; Aymerich, T.; León, M.; Roca, F.; Figueras, C. Validation and Representativeness of the Spanish BIG-PAC Database: Integrated Computerized Medical Records for Research into Epidemiology, Medicines and Health Resource Use (Real Word Evidence). In Proceedings of the ISPOR Europe, Copenhagen, Denmark, 2–6 November 2019. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). The Anatomical Therapeutic Chemical Classification System with Defined Daily Doses (ATC/DDD). Available online: https://www.who.int/standards/classifications/other-classifications/the-anatomical-therapeutic-chemical-classification-system-with-defined-daily-doses (accessed on 8 April 2021).
- Reddel, H.K.; Taylor, D.R.; Bateman, E.D.; Boulet, L.-P.; Boushey, H.A.; Busse, W.W.; Casale, T.B.; Chanez, P.; Enright, P.L.; Gibson, P.G.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Asthma Control and Exacerbations: Standardizing Endpoints for Clinical Asthma Trials and Clinical Practice. Am. J. Respir. Crit. Care Med. 2009, 180, 59–99. [Google Scholar] [CrossRef]
- Consejo General de Colegios Oficiales de Farmacéuticos BOT Plus 2. Base de Datos de Medicamentos. Available online: https://botplusweb.portalfarma.com/ (accessed on 13 April 2021).
- Instituto Nacional de Estadística. Ganancia Media Laboral Por Edad y Sexo. Available online: https://www.ine.es/dynt3/inebase/index.htm?padre=4563&capsel=4563 (accessed on 8 April 2021).
- Boletín Oficial del Estado. Ley Orgánica 15/1999, de 13 de Diciembre, de Protección de Datos de Carácter Personal. 1999, Volume 298, pp. 43088–43099. Available online: https://www.boe.es/buscar/doc.php?id=BOE-A-1999-23750 (accessed on 19 April 2023).
- Boletín Oficial del Estado. Ley Orgánica 3/2018, de 5 de Diciembre, de Protección de Datos Personales y Garantía de Los Derechos Digitales. 2018, Volume 294, pp. 119788–119857. Available online: https://www.boe.es/buscar/doc.php?id=BOE-A-2018-16673 (accessed on 19 April 2023).



{kind=link}
{kind=link}
| Study population | |
| Number of patients | 4740 |
| Demographic characteristics | |
| Mean (SD) age, years | 64.1 (16.3) |
| Ranges (n, %) | |
| 18–44 years | 681 (14.4%) |
| 45–64 years | 1584 (33.4%) |
| 65–69 years | 1090 (23.0%) |
| ≥75 years | 1385 (29.2%) |
| Gender (female) (n, %) | 3025 (63.8%) |
| Comorbidities (n, %) | |
| Arterial hypertension | 2480 (52.3%) |
| Dyslipidemia | 1985 (41.9%) |
| Obesity | 1136 (24.0%) |
| Diabetes | 923 (19.5%) |
| Renal failure | 549 (11.6%) |
| Depressive syndrome | 529 (11.2%) |
| Heart failure | 490 (10.3%) |
| Ischemic heart disease | 474 (10.0%) |
| COPD | 363 (7.7%) |
| Peripheral arterial disease | 316 (6.7%) |
| Stroke | 302 (6.4%) |
| Malignant neoplasms | 298 (6.3%) |
| Specific comorbidities (n, %) | |
| Allergic rhinitis | 1906 (40.2%) |
| Atopic dermatitis | 1338 (28.2%) |
| Chronic rhinosinusitis with nasal polyposis | 455 (9.6%) |
| AERD | 109 (2.3%) |
| Comorbidities (general) | |
| Chronic diseases | |
| Mean (SD) | 2.9 (2.0) |
| Median (P25–P75) | 3 (1–4) |
| Charlson index (mean, SD) | 0.8 (1.4) |
| 0 (n, %) | 2902 (61.2%) |
| 1 (n, %) | 826 (17.4%) |
| 2 (n, %) | 417 (8.8%) |
| 3+ (n, %) | 595 (13.0%) |
| Other variables | |
| Time from diagnosis, years | 32.4 (15.8) |
| Median (P25–P75) | 33 (20–45) |
| BMI, (Kg/m2) | 28.6 (4.4) |
| Median (P25–P75) | 28 (26–31) |
| Active smoking (n, %) | 530 (11.2%) |
| Study Population (N = 4740) | Dual Therapy (before LAMA Treatment) | Triple Therapy | Difference | 95% CI | p |
|---|---|---|---|---|---|
| Maintenance therapy † | |||||
| Beclomethasone/Formoterol | 1516 (32.0%) | 1646 (34.7%) | 2.7% | 1.2%–3.8% | 0.005 |
| Budesonide/Formoterol | 1147 (24.2%) | 1091 (23.0%) | −1.2% | −1.9%–(−1.0%) | <0.001 |
| Fluticasone/Formoterol | 151 (3.2%) | 185 (3.9%) | 0.7% | 0.2%–(0.9%) | <0.001 |
| Fluticasone/Vilanterol | 385 (8.1%) | 435 (9.2%) | 1.1% | 1.1%–(2.4%) | <0.001 |
| Fluticasone/Salmeterol | 1541 (32.5%) | 1383 (29.2%) | −3.3% | −5.7%–(−1.5%) | 0.005 |
| Tiotropium | --- | 3032 (64.0%) | --- | ||
| Aclidinium * | --- | 664 (14.0%) | --- | ||
| Glycopyrronium * | --- | 723 (15.3%) | --- | ||
| Umeclidinium * | --- | 321 (6.8%) | --- | ||
| Concomitant therapy | |||||
| Oral corticosteroids | 1537 (32.4%) | 1316 (27.8%) | −4.7% | −6.4%–(−2.9%) | <0.001 |
| Chronic use of oral corticosteroids (>6 months) | 413 (8.7%) | 340 (7.2%) | −1.5% | −1.9%–(−1.2%) | <0.001 |
| Systemic antibiotics | 1201 (25.3%) | 903 (19.1%) | −6.3% | −7.8%–(−4.8%) | <0.001 |
| SABA | 4385 (92.5%) | 3797 (80.1%) | −12.4% | −14.0%–(−10.2%) | <0.001 |
| SAMA | 533 (11.2%) | 388 (8.2%) | −3.1% | −5.5%–(−1.2%) | <0.001 |
| Xanthines | 184 (3.9%) | 184 (3.9%) | 0.0% | −0.7%–0.7% | 0.999 |
| LRA | 1314 (27.7%) | 1196 (25.2%) | −2.5% | −3.9%–(−1.0%) | 0.001 |
| Biologics | 109 (2.3%) | 86 (1.8%) | −0.5% | −0.8%–(−0.1%) | 0.005 |
| Study Population (N = 4740) | Dual Therapy (before LAMA Treatment) | Triple Therapy | Absolute Difference | 95% CI | Relative Difference | p |
|---|---|---|---|---|---|---|
| Severe exacerbations | ||||||
| N, % patients with severe exacerbations | 2184 (46.1%) | 2002 (42.2%) | −3.9% | −6.0–(−2.7%) | −8.5% | <0.001 |
| Severe exacerbations, mean (SD) | 0.6 (0.7) | 0.5 (0.7) | −0.1 (0.7) | −0.2–0.0 | −16.7% | 0.044 |
| 0 (n, %) | 2556 (53.9%) | 2738 (57.8%) | 3.9% | 2.7–6.0% | 7.2% | <0.001 |
| 1 (n, %) | 1711 (36.1%) | 1627 (34.3%) | −1.8% | −2.2–(−1.4%) | −5.0% | 0.025 |
| 2+ (n, %) | 473 (10.0%) | 375 (7.9%) | −2.1% | −2.5–(−1.7%) | −21.0% | 0.018 |
| N, % patients who required systemic corticosteroids due to severe exacerbations | 1711 (36.1%) | 1529 (32.3%) | −3.8% | −5.6–(−2.3%) | −10.5% | <0.001 |
| Severe exacerbations requiring systemic corticosteroids, mean (SD) | 0.4 (0.5) | 0.4 (0.5) | 0.1 (0.5) | −0.8–0.2 | 22.5% | <0.001 |
| 0 (n, %) | 3029 (63.9%) | 3211 (67.7%) | 3.8% | 2.3–(5.6%) | 5.9% | <0.001 |
| 1 (n, %) | 1687 (35.6%) | 1399 (29.5%) | −6.1% | −7.2–(−5.0%) | −17.1% | <0.001 |
| 2+ (n, %) | 24 (0.5%) | 130 (2.8%) | 2.1% | 1.4–2.8 | 4.2% | <0.001 |
| N, % patients admitted to the hospital due to severe exacerbations | 745 (15.7%) | 643 (13.6%) | −2.1% | −3.9–(−1.3%) | −13.4% | <0.001 |
| Severe exacerbations requiring hospitalizations, mean (SD) | 0.3 (0.6) | 0.2 (0.4) | −0.1 (1.0) | −0.2–0.0 | −29.5% | <0.001 |
| 0 (n, %) | 3995 (84.3%) | 4097 (86.4%) | 2.1% | 1.3–3.9% | 2.5% | 0.005 |
| 1 (n, %) | 480 (10.1%) | 544 (11.5%) | 1.4% | 0.7–2.1% | 13.8% | 0.014 |
| 2+ (n, %) | 265 (6.6%) | 99 (2.1%) | −4.5% | −5.7–(−3.3%) | −67.2% | <0.001 |
| Lung function | ||||||
| FEV1 (mean, SD) | 55.3 (6.6) | 57.6 (6.5) | 2.4% | 2.2–2.6 | 4.3% | <0.001 |
| Median (P25–P75) | 56 (51–61) | 58 (53–63) | ||||
| FVC (mean, SD) | 85.5 (11.2) | 86.3 (11.2) | 0.8% | 0.6–1.1 | 1.0% | <0.001 |
| Median (P25–P75) | 86 (78–93) | 86 (79–94) | ||||
| FEV1/FVC (mean, SD) | 64.9 (3.7) | 64.7 (3.7) | −0.2% | −0.4–(−0.1) | −0.3% | 0.004 |
| Median (P25–P75) | 65 (62–68) | 64 (61–68) | ||||
| Eosinophil counts | ||||||
| Eosinophiles in blood (cells/μL) | ||||||
| Mean (SD) | 449.9 (165.5) | 443.2 (164.4) | −6.7 (9.8) | −13.3–(−0.2) | −1.5% | 0.046 |
| Median (P25–P75) | 450 (313–589) | 443 (307–582) | ||||
| Eosinophiles in blood, ≥ 300 cells/μL n, % | 3681 (77.7%) | 3623 (76.4%) | −1.2% | −2.9–(−0.5) | −1.7% | 0.153 |
| Time to first severe exacerbation, days | ||||||
| Mean (SD) | 191.7 (99.1) | 183.5 (99.1) | −8.2 (36.6) | −14.1–(−1.8) | −4.3% | 0.025 |
| Median (P25–P75) | 191 (104–278) | 184 (97–269) |
| Study Population (N = 4740) | Dual Therapy (before LAMA Treatment) | Triple Therapy | Absolute Difference | 95% CI | Relative Difference | p |
|---|---|---|---|---|---|---|
| Diagnosis of COPD | ||||||
| FEV1 | ||||||
| Without COPD | 55.3 (6.6) | 57.7 (6.5) | 2.4 | 2.3–2.4 | 4.3% | 0.008 |
| With COPD | 53.5 (6.5) | 56.0 (6.4) | 2.5 | 2.3–2.7 | 4.7% | 0.003 |
| Severe exacerbations | ||||||
| Without COPD | 46.2% | 42.3% | −3.9% | −5.0–(−2.8%) | −8.5% | <0.001 |
| With COPD | 47.5% | 43.4% | −4.1% | −5.0–(−3.2%) | −8.6% | <0.001 |
| Costs | ||||||
| Without COPD | €4711 | €4145 | −€565 | −829 €–(−300 €) | −12.0% | <0.001 |
| With COPD | €4959 | €4356 | −€603 | −982 €–(−224 €) | −12.2% | <0.001 |
| Age | ||||||
| FEV1 (mean, SD) | ||||||
| 18–44 years | 57.4 (6.3) | 62.0 (6.6) | 4.6 | 4.2–5.0 | 8.0% | <0.001 |
| 45–64 years | 56.0 (6.1) | 59.9 (6.0) | 3.9 | 3.5–4.3 | 7.0% | <0.001 |
| 65–74 years | 55.6 (6.7) | 57.9 (6.4) | 2.3 | 1.2–2.4 | 4.1% | 0.009 |
| 75+ years | 53.8 (6.6) | 55.7 (6.4) | 1.9 | 0.8–3.0 | 3.5% | 0.028 |
| Severe exacerbations | ||||||
| 18–44 years | 41.6% | 33.7% | −7.9% | −10.1–(−5.7%) | −18.9% | <0.001 |
| 45–64 years | 43.6% | 35.9% | −7.7% | −9.9–(−5.5%) | −17.7% | <0.001 |
| 65–74 years | 46.8% | 42.7% | −4.1% | −5.4–(−2.8%) | −8.7% | <0.001 |
| 75+ years | 49.1% | 46.2% | −3.0% | −3.6–(−2.4%) | −6.0% | <0.001 |
| Costs (€) | ||||||
| 18–44 years | €4019 | €3303 | −€717 | −949 €–(−485 €) | −17.8% | <0.001 |
| 45–64 years | €4354 | €3686 | −€669 | −1102 €–(−235 €) | −15.4% | <0.001 |
| 65–74 years | €4891 | €4400 | −€491 | −768 €–(−214 €) | −10.0% | <0.001 |
| 75+ years | €5387 | €4990 | −€397 | −687 €–(−108 €) | −7.4% | <0.001 |
| Asthma severity | ||||||
| FEV1 | ||||||
| FEV1 ≥ 60% at index date | 62.1 (2.8) | 64.5 (3.1) | 2.4 | 1.2–3.6 | 3.9% | 0.022 |
| FEV1 < 60% at index date | 50.0 (5.3) | 57.2 (5.2) | 7.2 | 6.8–7.6 | 14.4% | <0.001 |
| Severe exacerbations | ||||||
| FEV1 ≥ 60% at index date | 44.0% | 40.1% | −3.9% | −4.9–(−2.9%) | −8.9% | <0.001 |
| FEV1 < 60% at index date | 48.2% | 42.1% | −6.1% | −7.5–(−4.7%) | −12.7% | <0.001 |
| Costs | ||||||
| FEV1 ≥ 60% at index date | €4585 | €4155 | −€430 | −625 €–(−234 €) | −9.4% | <0.001 |
| FEV1 < 60% at index date | €4966 | €4214 | −€751 | −1167 €–(−335 €) | −15.1% | <0.001 |
| Study Population (N = 4740) | Dual Therapy (before LAMA Treatment) | Triple Therapy | Difference | 95% CI | p |
|---|---|---|---|---|---|
| Use of healthcare and non-healthcare resources † | |||||
| Primary care medical visits (mean, SD) | 10.4 (9) | 9.9 (10.5) | −0.5 (9.1) | −0.8–(−0.3) | <0.001 |
| Specialized care medical visits (mean, SD) | 1.2 (3.5) | 1 (1.5) | −0.2 (3.4) | −0.3–(−0.2) | <0.001 |
| Emergency medical visits (mean, SD) | 0.7 (1.6) | 0.6 (0.9) | −0.1 (1.7) | −0.2–0.0 | 0.035 |
| Hospitalized patients (n, %) | 745 (15.7%) | 643 (13.6%) | −2.1% | −3.9–(−1.3%) | <0.001 |
| Hospitalization days (mean, SD) | 4.6 (12.8) | 3.6 (10.6) | −1.1 (15) | −1.5–(−0.7) | <0.001 |
| Laboratory tests (mean, SD) | 1.3 (1.7) | 1.5 (2.0) | 0.2 (2.0) | 0.1–0.3 | <0.001 |
| Conventional radiology (mean, SD) | 0.6 (0.8) | 0.3 (0.6) | −0.2 (1) | −0.3–(−0.2) | <0.001 |
| Computed tomography (mean, SD) | 0.4 (0.5) | 0.3 (0.8) | −0.1 (0.9) | −0.3–(−0.1) | <0.001 |
| Magnetic nuclear resonance (mean, SD) | 0.2 (0.4) | 0.1 (0.3) | −0.1 (0.5) | −0.3–(−0.1) | <0.001 |
| Other diagnostic/therapeutic tests (mean, SD) | 2.4 (0.5) | 2.4 (0.5) | 0 (0.4) | −0.1–0.0 | 0.006 |
| Patients on sick leave (n, %) | 612 (12.9%) | 602 (12.7%) | −0.2% | −1.5–(−0.9) | 0.728 |
| Sick leave days (mean, SD) | 3.1 (10.7) | 2.8 (10.8) | −0.3 (14.3) | −0.7–(−0.1) | 0.129 |
| Healthcare and non-healthcare costs (€) † | |||||
| Primary care medical visits (mean, SD) | 251 (219) | 239 (254) | −11.8 (220) | −18.1–(−5.5) | <0.001 |
| Specialized care medical visits (mean, SD) | 120 (336) | 99 (144) | −20.7 (330.8) | −30.1–(−11.3) | <0.001 |
| Emergency medical visit (mean, SD) | 82 (195) | 75 (107) | −6.3 (204.8) | −12.1–(−0.4) | 0.035 |
| Hospitalizations (mean, SD) | 2638 (7298) | 2018 (6042) | −620.2 (8533.2) | −863.2–(−377.3) | <0.001 |
| Laboratory tests (mean, SD) | 44 (58) | 50 (68) | 6.1 (67.9) | 4.1–8.0 | <0.001 |
| Conventional radiology (mean, SD) | 17 (24) | 10 (18) | −7.3 (28.8) | −8.1–(−6.5) | <0.001 |
| Computed tomography (mean, SD) | 39 (49) | 28 (76) | −11.5 (86.4) | −13.9–(−9.0) | <0.001 |
| Magnetic nuclear resonance (mean, SD) | 38 (75) | 22 (60) | −16.1 (90.3) | −18.7–(−13.5) | <0.001 |
| Other diagnostic/therapeutic tests (mean, SD) | 116 (25) | 116 (25) | 0.7 (17.9) | 0.2–1.2 | 0.006 |
| Drugs (mean, SD) | 984 (1787) | 1209 (1572) | 225.1 (1431.9) | 184.3–265.8 | <0.001 |
| Healthcare cost (mean, SD) | 4406 (7870) | 3867 (6602) | −538.8 (9002.4) | −795.1–(−282.4) | <0.001 |
| Non-healthcare cost (productivity loss) (mean, SD) | 313 (1087) | 281 (1094) | −32 (1451.5) | −73.4–(−9.3) | 0.129 |
| Total cost (mean, SD) | 4719 (8110) | 4148 (6711) | −570.8 (8995.9) | −827.0–(−314.7) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plaza, V.; Domínguez-Ortega, J.; González-Segura Alsina, D.; Lo Re, D.; Sicras-Mainar, A. Comprehensive Observational Study in a Large Cohort of Asthma Patients after Adding LAMA to ICS/LABA. Pharmaceuticals 2023, 16, 1609. https://doi.org/10.3390/ph16111609
Plaza V, Domínguez-Ortega J, González-Segura Alsina D, Lo Re D, Sicras-Mainar A. Comprehensive Observational Study in a Large Cohort of Asthma Patients after Adding LAMA to ICS/LABA. Pharmaceuticals. 2023; 16(11):1609. https://doi.org/10.3390/ph16111609
Chicago/Turabian StylePlaza, Vicente, Javier Domínguez-Ortega, Diego González-Segura Alsina, Daniele Lo Re, and Antoni Sicras-Mainar. 2023. "Comprehensive Observational Study in a Large Cohort of Asthma Patients after Adding LAMA to ICS/LABA" Pharmaceuticals 16, no. 11: 1609. https://doi.org/10.3390/ph16111609