
Choroidal Morphology on Ultra-Widefield Indocyanine Green Angiography and Response to Aflibercept in Pachychoroid Neovasculopathy

Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Treatment and Assessment Schedule
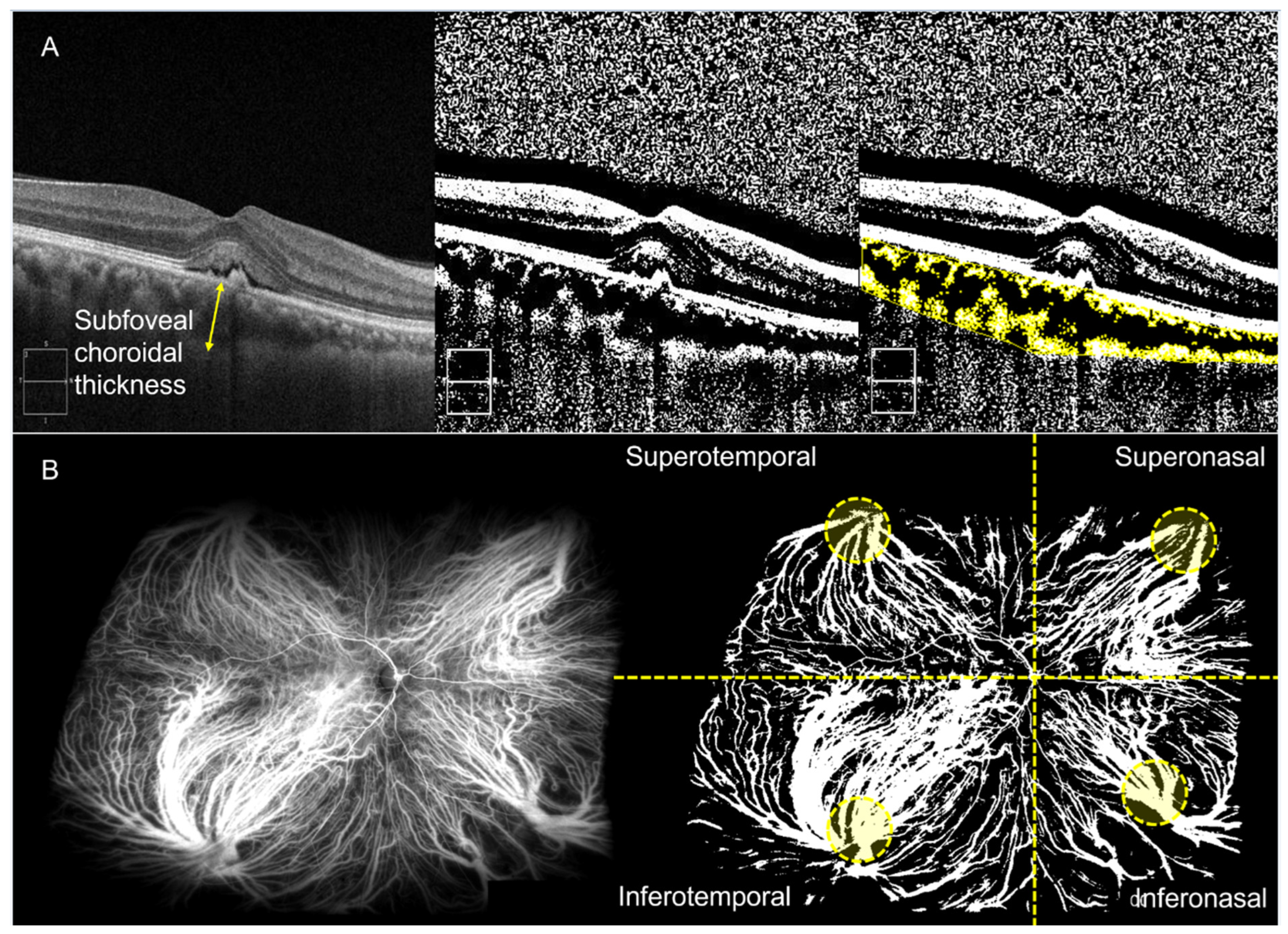
2.3. Imaging Analysis
2.4. Statistical Analysis
3. Results
3.1. Comparison of OCT Parameters between the Dry and Non-Dry Group
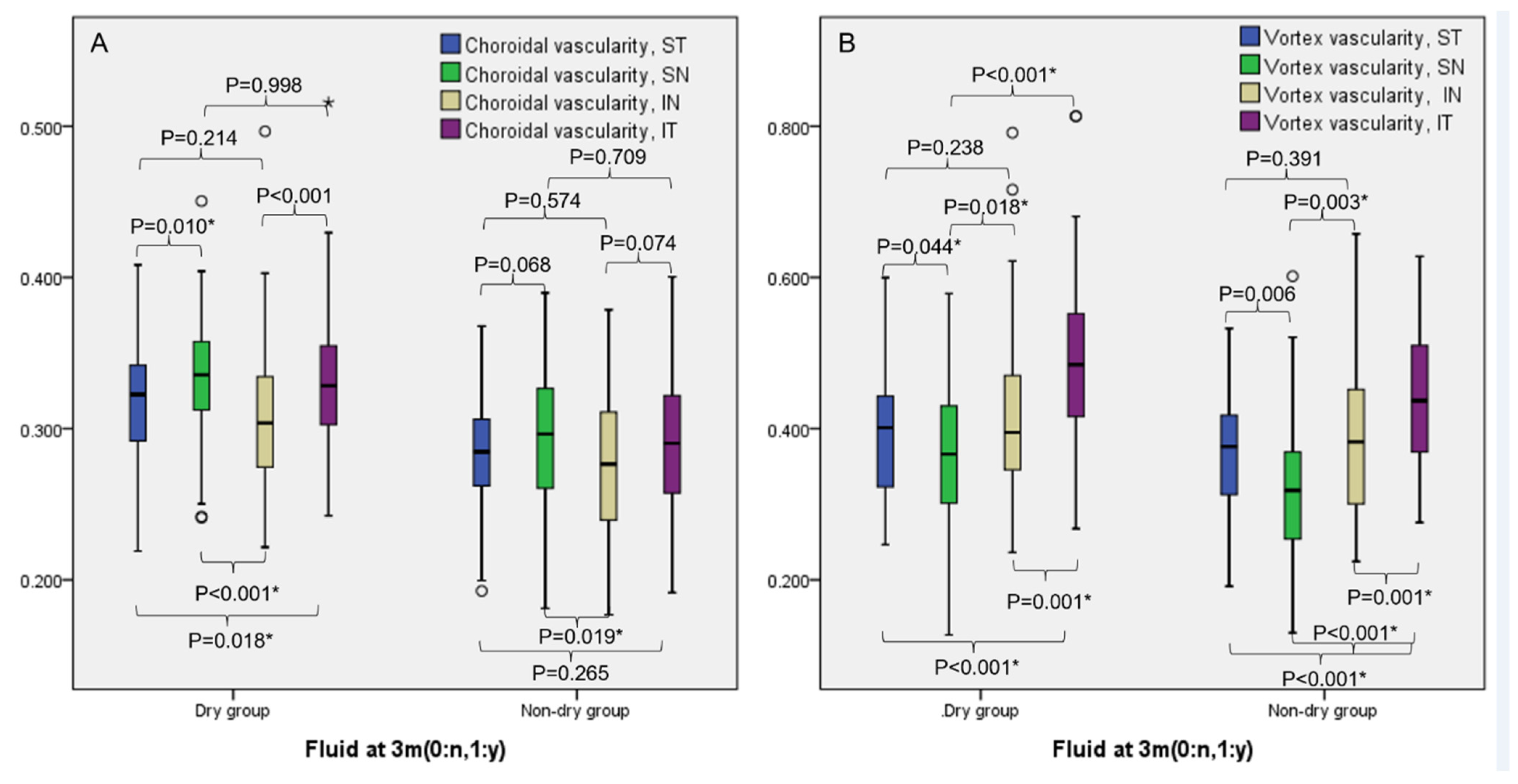
3.2. Comparison of UWICGA CVD between the Dry and Non-Dry Group
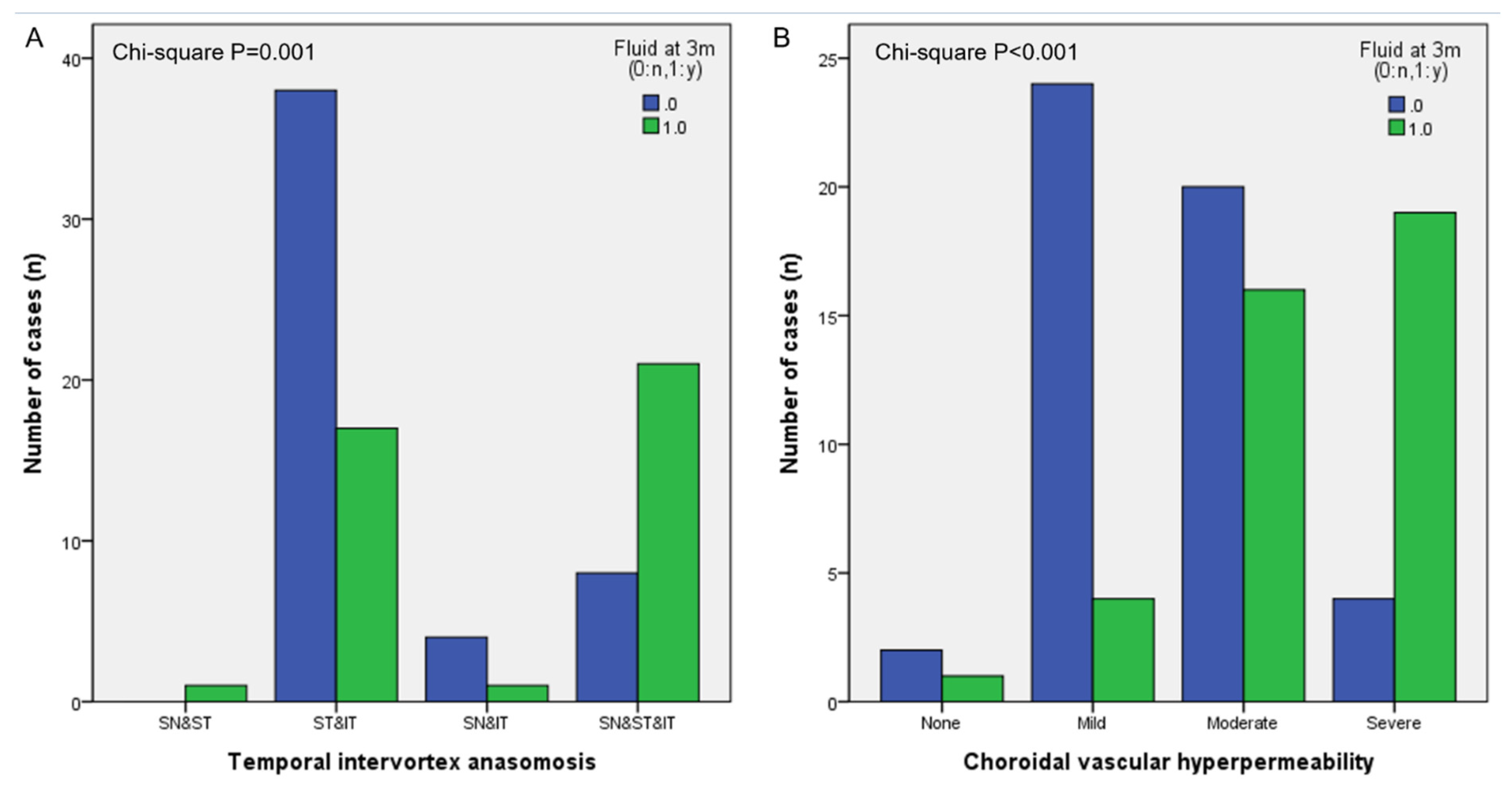
3.3. Analysis of Other Choroidal Vascular Features on UWICGA Images
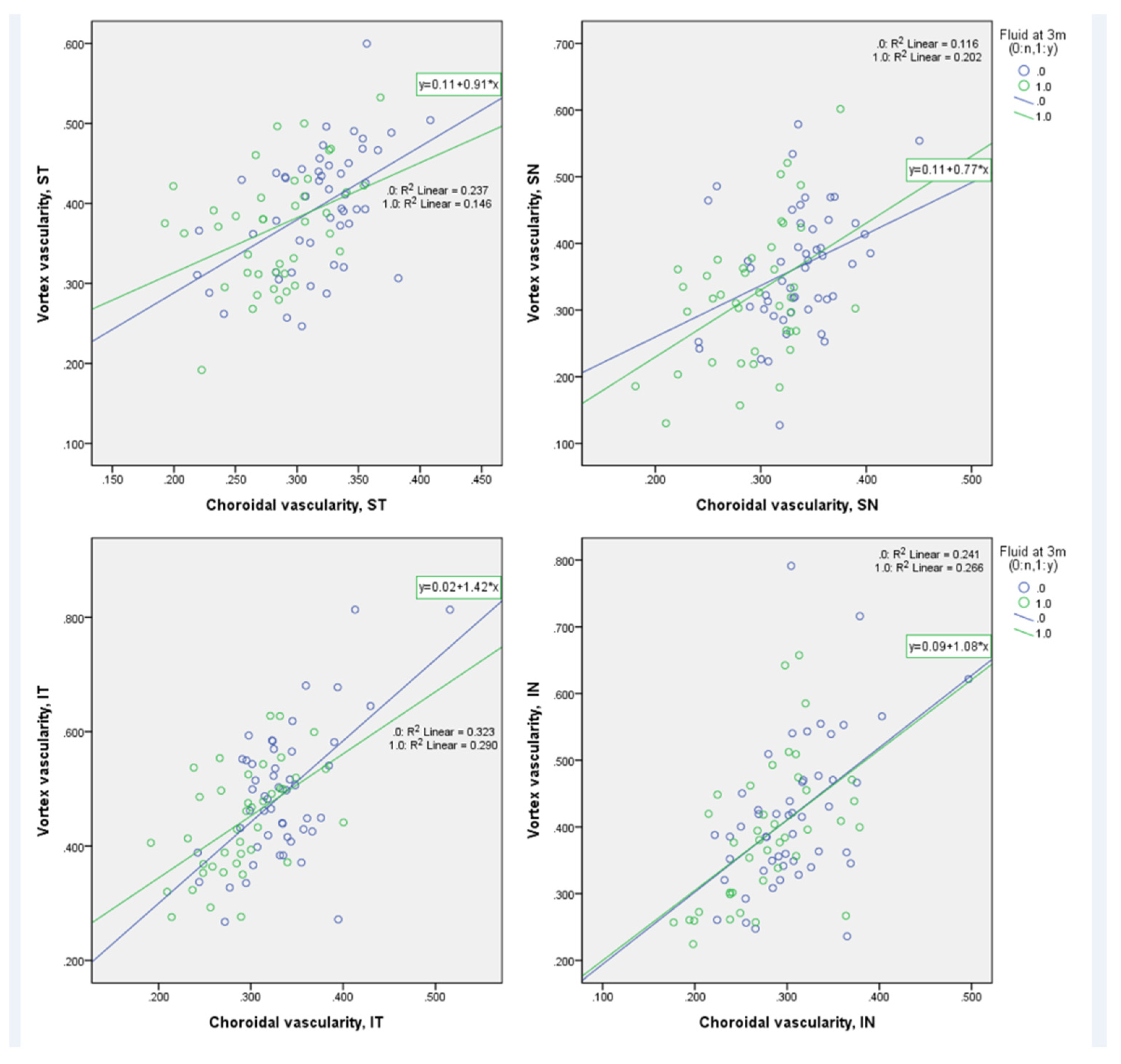
3.4. Correlation among Parameters
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pang, C.E.; Freund, K.B. Pachychoroid Neovasculopathy. Retina 2015, 35, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.M.G.; Lai, T.Y.Y.; Ruamviboonsuk, P.; Chen, S.J.; Chen, Y.; Freund, K.B.; Gomi, F.; Koh, A.H.; Lee, W.K.; Wong, T.Y. Polypoidal Choroidal Vasculopathy: Definition, Pathogenesis, Diagnosis, and Management. Ophthalmology 2018, 125, 708–724. [Google Scholar] [CrossRef] [Green Version]
- Warrow, D.J.; Hoang, Q.V.; Freund, K.B. Pachychoroid pigment epitheliopathy. Retina 2013, 33, 1659–1672. [Google Scholar] [CrossRef]
- Elfandi, S.; Ooto, S.; Miyata, M.; Ueda-Arakawa, N.; Subhi, Y.; Yamashiro, K.; Tamura, H.; Oishi, A.; Hata, M.; Yoshimura, N.; et al. Effects of Intravitreous Aflibercept Injection in Pachychoroid Neovasculopathy: Comparison with Typical Neovascular Age-Related Macular Degeneration. Clin. Ophthalmol. 2021, 15, 1539–1549. [Google Scholar] [CrossRef]
- Jung, B.J.; Kim, J.Y.; Lee, J.H.; Baek, J.; Lee, K.; Lee, W.K. Intravitreal aflibercept and ranibizumab for pachychoroid neovasculopathy. Sci. Rep. 2019, 9, 2055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsumoto, H.; Hiroe, T.; Morimoto, M.; Mimura, K.; Ito, A.; Akiyama, H. Efficacy of treat-and-extend regimen with aflibercept for pachychoroid neovasculopathy and Type 1 neovascular age-related macular degeneration. Jpn. J. Ophthalmol. 2018, 62, 144–150. [Google Scholar] [CrossRef]
- Baek, J.; Lee, J.H.; Jeon, S.; Lee, W.K. Choroidal morphology and short-term outcomes of combination photodynamic therapy in polypoidal choroidal vasculopathy. Eye 2019, 33, 419–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azuma, K.; Okubo, A.; Nomura, Y.; Zhou, H.; Terao, R.; Hashimoto, Y.; Asano, K.S.; Azuma, K.; Inoue, T.; Obata, R. Association between pachychoroid and long-term treatment outcomes of photodynamic therapy with intravitreal ranibizumab for polypoidal choroidal vasculopathy. Sci. Rep. 2020, 10, 8337. [Google Scholar] [CrossRef] [PubMed]
- Karasu, B.; Akbas, Y.B.; Kaskal, M.; Aykut, A.; Celebi, A.R.C. Long term results of three anti-vascular endothelial growth factor agents in pachychoroid neovasculopathy. Cutan. Ocul. Toxicol. 2022, 41, 145–154. [Google Scholar] [CrossRef]
- Azuma, K.; Tan, X.; Asano, S.; Shimizu, K.; Ogawa, A.; Inoue, T.; Murata, H.; Asaoka, R.; Obata, R. The association of choroidal structure and its response to anti-VEGF treatment with the short-time outcome in pachychoroid neovasculopathy. PLoS ONE 2019, 14, e0212055. [Google Scholar] [CrossRef]
- Hara, C.; Wakabayashi, T.; Toyama, H.; Fukushima, Y.; Sayanagi, K.; Sato, S.; Sakaguchi, H.; Nishida, K. Characteristics of patients with neovascular age-related macular degeneration who are non-responders to intravitreal aflibercept. Br. J. Ophthalmol. 2018, 103, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F. Disease expression in nonexudative age-related macular degeneration varies with choroidal thickness. Retina 2018, 38, 708–716. [Google Scholar] [CrossRef]
- Spaide, R.F.; Koizumi, H.; Pozonni, M.C. Enhanced Depth Imaging Spectral-Domain Optical Coherence Tomography. Am. J. Ophthalmol. 2008, 146, 496–500. [Google Scholar] [CrossRef]
- Lee, A.; Ra, H.; Baek, J. Choroidal vascular densities of macular disease on ultra-widefield indocyanine green angiography. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 1921–1929. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Ledesma-Gil, G.; Gemmy Cheung, C.M. Intervortex venous anastomosis in pachychoroid-related disorders. Retina 2021, 41, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Jirarattanasopa, P.; Ooto, S.; Nakata, I.; Tsujikawa, A.; Yamashiro, K.; Oishi, A.; Yoshimura, N. Choroidal thickness, vascular hyperpermeability, and complement factor H in age-related macular degeneration and polypoidal choroidal vasculopathy. Investig. Ophthalmol. Vis. Sci. 2012, 53, 3663–3672. [Google Scholar] [CrossRef]
- Kim, H.; Lee, S.C.; Kwon, K.Y.; Lee, J.H.; Koh, H.J.; Byeon, S.H.; Kim, S.S.; Kim, M.; Lee, C.S. Subfoveal choroidal thickness as a predictor of treatment response to anti-vascular endothelial growth factor therapy for polypoidal choroidal vasculopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2016, 254, 1497–1503. [Google Scholar] [CrossRef] [PubMed]
- Kong, M.; Kim, S.M.; Ham, D.I. Comparison of clinical features and 3-month treatment response among three different choroidal thickness groups in polypoidal choroidal vasculopathy. PLoS ONE 2017, 12, e0184058. [Google Scholar] [CrossRef] [PubMed]
- Sakurada, Y.; Sugiyama, A.; Tanabe, N.; Kikushima, W.; Kume, A.; Iijima, H. Choroidal thickness as a prognostic factor of photodynamic therapy with aflibercept or ranibizumab for polypoidal choroidal vasculopathy. Retina 2017, 37, 1866–1872. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.C.; Cheng, C.K. Difference between Pachychoroid and Nonpachychoroid Polypoidal Choroidal Vasculopathy and Their Response to Anti-Vascular Endothelial Growth Factor Therapy. Retina 2019, 40, 1403–1411. [Google Scholar] [CrossRef]
- Lee, W.K.; Baek, J.; Dansingani, K.K.; Lee, J.H.; Freund, K.B. Choroidal morphology in eyes with polypoidal choroidal vasculopathy and normal or subnormal subfoveal choroidal thickness. Retina 2016, 36 (Suppl. S1), S73–S82. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.Y.; Kwon, K.Y.; Byeon, S.H. Association between choroidal thickness and the response to intravitreal ranibizumab injection in age-related macular degeneration. Acta Ophthalmol. 2015, 93, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F. Age-related choroidal atrophy. Am. J. Ophthalmol. 2009, 147, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.; Tsujikawa, A.; Yamashiro, K.; Ooto, S.; Oishi, A.; Tamura, H.; Nakata, I.; Matsuda, F.; Yoshimura, N. Choroidal neovascularization in eyes with choroidal vascular hyperpermeability. Investig. Ophthalmol. Vis. Sci. 2014, 55, 3223–3230. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Dry Group (n = 50) | Non-Dry Group (n = 40) | p-Value |
|---|---|---|---|
| Age (mean ± SD, years) | 59.74 ± 13.55 | 63.63 ± 12.91 | 0.169 a |
| Sex (male, %) | 62 | 75 | 0.190 b |
| Laterality (left eye, %) | 50 | 48 | 0.816 b |
| Diabetes (n, (%)) | 18 | 15 | 0.706 b |
| Hypertension (n, (%)) | 44 | 48 | 0.744 b |
| BCVA, baseline (mean ± SD, logMAR) | 0.175 ± 0.399 | 0.334 ± 0.306 | 0.035 a,* |
| Parameters | Dry Group (n = 50) | Non-Dry Group (n = 40) | p-Value |
|---|---|---|---|
| CMT, baseline (μm) | 316.84 ± 118.22 | 367.03 ± 185.21 | 0.142 |
| CMT, 3 m (μm) | 239.68 ± 65.81 | 297.83 ± 111.44 | 0.005 * |
| SFCT, baseline (μm) | 399.1 ± 60 | 342.13 ± 38.91 | <0.001 * |
| SFCT, 3 m (μm) | 367.2 ± 67.35 | 321.53 ± 46.54 | <0.001 * |
| CVD, Bscan, baseline | 0.768 ± 0.036 | 0.727 ± 0.039 | <0.001 * |
| CVD, Bscan, 3-months | 0.760 ± 0.042 | 0.731 ± 0.038 | 0.001 * |
| CVD, UWICGA, total | 0.323 ± 0.034 | 0.286 ± 0.038 | <0.001 * |
| CVD, UWICGA, ST | 0.317 ± 0.040 | 0.283 ± 0.04 | <0.001 * |
| CVD, UWICGA, SN | 0.334 ± 0.040 | 0.293 ± 0.045 | <0.001 * |
| CVD, UWICGA, IN | 0.306 ± 0.051 | 0.278 ± 0.052 | 0.010 * |
| CVD, UWICGA, IT | 0.334 ± 0.047 | 0.290 ± 0.046 | <0.001 * |
| CVD, vortex ampullae, total | 0.416 ± 0.053 | 0.381 ± 0.063 | 0.005 * |
| CVD, vortex ampullae, ST | 0.395 ± 0.075 | 0.370 ± 0.073 | 0.120 |
| CVD, vortex ampullae, SN | 0.363 ± 0.091 | 0.323 ± 0.102 | 0.056 |
| CVD, vortex ampullae, IN | 0.418 ± 0.113 | 0.387 ± 0.106 | 0.187 |
| CVD, vortex ampullae, IT | 0.490 ± 0.117 | 0.442 ± 0.094 | 0.034 * |
| Clinical Parameters | Choroidal Vessel Densities on UWICGA | |||||
|---|---|---|---|---|---|---|
| Total | ST | SN | IN | IT | ||
| Age | Coefficient | −0.174 | −0.184 | −0.226 * | −0.100 | −0.074 |
| p-value | 0.100 | 0.082 | 0.032 | 0.347 | 0.490 | |
| LogMAR BCVA, baseline | Coefficient | −0.291 ** | −0.385 ** | −0.245 * | −0.090 | −0.261 * |
| p-value | 0.005 | 0.000 | 0.020 | 0.400 | 0.013 | |
| LogMAR BCVA, 3 months | Coefficient | −0.351 ** | −0.468 ** | −0.265 * | −0.188 | −0.256 * |
| p-value | 0.001 | 0.000 | 0.012 | 0.076 | 0.015 | |
| CMT, baseline | Coefficient | −0.015 | −0.081 | −0.033 | 0.044 | 0.006 |
| p-value | 0.887 | 0.449 | 0.760 | 0.684 | 0.954 | |
| CMT, 3 months | Coefficient | −0.080 | −0.043 | −0.092 | −0.048 | −0.078 |
| p-value | 0.455 | 0.689 | 0.390 | 0.657 | 0.466 | |
| SFCT, baseline | Coefficient | 0.353 ** | 0.374 ** | 0.400 ** | 0.140 | 0.268 * |
| p-value | 0.001 | 0.000 | 0.000 | 0.187 | 0.011 | |
| SFCT, 3 months | Coefficient | 0.247 * | 0.350 ** | 0.291** | 0.038 | 0.164 |
| p-value | 0.019 | 0.001 | 0.005 | 0.721 | 0.123 | |
| CVD, Bscan, baseline | Coefficient | 0.480 ** | 0.425 ** | 0.423 ** | 0.362 ** | 0.365 ** |
| p-value | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| CVD, Bscan, 3 months | Coefficient | 0.315 ** | 0.356 ** | 0.273 ** | 0.216 * | 0.199 |
| p-value | 0.003 | 0.001 | 0.009 | 0.040 | 0.060 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, S.Y.; Lee, S.H.; Lee, P.-k.; Ra, H.; Baek, J. Choroidal Morphology on Ultra-Widefield Indocyanine Green Angiography and Response to Aflibercept in Pachychoroid Neovasculopathy. Pharmaceuticals 2023, 16, 73. https://doi.org/10.3390/ph16010073
Han SY, Lee SH, Lee P-k, Ra H, Baek J. Choroidal Morphology on Ultra-Widefield Indocyanine Green Angiography and Response to Aflibercept in Pachychoroid Neovasculopathy. Pharmaceuticals. 2023; 16(1):73. https://doi.org/10.3390/ph16010073
Chicago/Turabian StyleHan, Su Yeon, Seung Hoon Lee, Phil-kyu Lee, Ho Ra, and Jiwon Baek. 2023. "Choroidal Morphology on Ultra-Widefield Indocyanine Green Angiography and Response to Aflibercept in Pachychoroid Neovasculopathy" Pharmaceuticals 16, no. 1: 73. https://doi.org/10.3390/ph16010073