
Adjuvant Anti-PD-1 Immunotherapy versus Conventional Therapy for Stage III Melanoma: A Real-World Retrospective Cohort Study
 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Survival Data
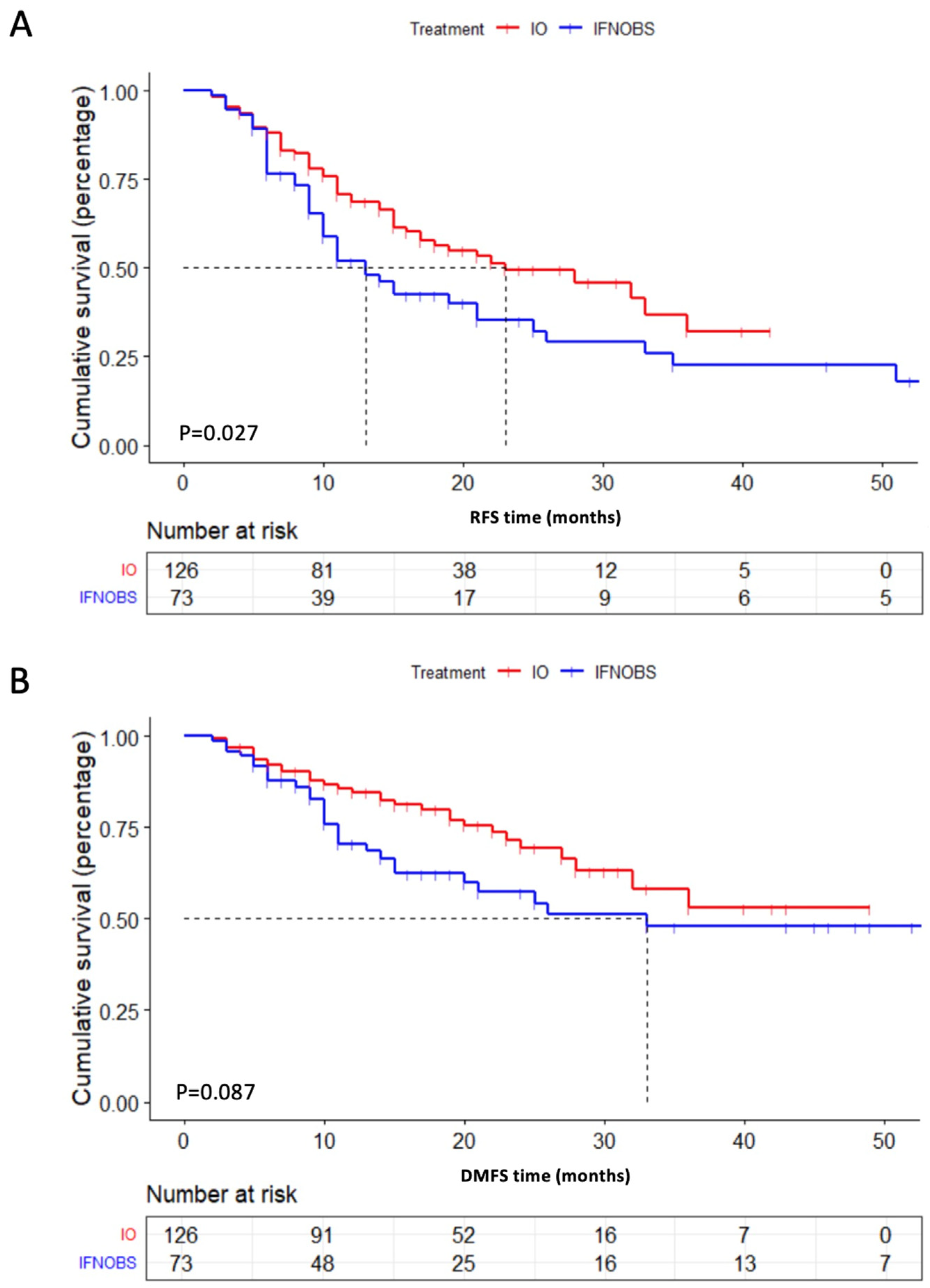
2.2.1. Relapse-Free Survival
2.2.2. Distant Metastasis-Free Survival
2.2.3. OS
2.3. Subgroup Analysis
3. Materials and Methods
3.1. Patients
3.2. Study Design
3.3. Data Retrieval and Follow-Up
3.4. Statistical Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Miller, A.J.; Mihm, M.C., Jr. Melanoma. N. Engl. J. Med. 2006, 355, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Gershenwald, J.E.; Scolyer, R.A. Melanoma Staging: American Joint Committee on Cancer (AJCC) 8th Edition and Beyond. Ann. Surg. Oncol. 2018, 25, 2105–2110. [Google Scholar] [CrossRef]
- Kirkwood, J.M.; Manola, J.; Ibrahim, J.; Sondak, V.; Ernstoff, M.S.; Rao, U. A pooled analysis of eastern cooperative oncology group and intergroup trials of adjuvant high-dose interferon for melanoma. Clin. Cancer Res. 2004, 10, 1670–1677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eggermont, A.M.; Suciu, S.; Testori, A.; Santinami, M.; Kruit, W.H.; Marsden, J.; Punt, C.J.; Salès, F.; Dummer, R.; Robert, C.; et al. Long-term results of the randomized phase III trial EORTC 18991 of adjuvant therapy with pegylated interferon alfa-2b versus observation in resected stage III melanoma. J. Clin. Oncol. 2012, 30, 3810–3818. [Google Scholar] [CrossRef] [PubMed]
- Pectasides, D.; Dafni, U.; Bafaloukos, D.; Skarlos, D.; Polyzos, A.; Tsoutsos, D.; Kalofonos, H.; Fountzilas, G.; Panagiotou, P.; Kokkalis, G.; et al. Randomized phase III study of 1 month versus 1 year of adjuvant high-dose interferon alfa-2b in patients with resected high-risk melanoma. J. Clin. Oncol. 2009, 27, 939–944. [Google Scholar] [CrossRef] [PubMed]
- Liguoro, D.; Fattore, L.; Mancini, R.; Ciliberto, G. Drug tolerance to target therapy in melanoma revealed at single cell level: What next? Biochim. Biophys. Acta Rev. Cancer. 2020, 1874, 188440. [Google Scholar] [CrossRef]
- Iwai, Y.; Ishida, M.; Tanaka, Y.; Okazaki, T.; Honjo, T.; Minato, N. Involvement of PD-L1 on tumor cells in the escape from host immune system and tumor immunotherapy by PD-L1 blockade. Proc. Natl. Acad. Sci. USA 2002, 99, 12293–12297. [Google Scholar] [CrossRef] [Green Version]
- Dong, H.; Strome, S.E.; Salomao, D.R.; Tamura, H.; Hirano, F.; Flies, D.B.; Roche, P.C.; Lu, J.; Zhu, G.; Tamada, K.; et al. Tumor-associated B7-H1 promotes T-cell apoptosis: A potential mechanism of immune evasion. Nat. Med. 2002, 8, 793–800. [Google Scholar] [CrossRef]
- Khoja, L.; Butler, M.O.; Kang, S.P.; Ebbinghaus, S.; Joshua, A.M. Pembrolizumab. J. Immunother. Cancer 2015, 3, 36. [Google Scholar] [CrossRef] [Green Version]
- Shi, Q.; Liu, L.; Chen, J.; Zhang, W.; Guo, W.; Wang, X.; Wang, H.; Guo, S.; Yue, Q.; Ma, J.; et al. Integrative Genomic Profiling Uncovers Therapeutic Targets of Acral Melanoma in Asian Populations. Clin. Cancer Res. 2022, 28, 2690–2703. [Google Scholar] [CrossRef]
- Cho, K.H.; Han, K.H.; Minn, K.W. Superficial spreading melanoma arising in a longstanding melanocytic nevus on the sole. J. Dermatol. 1998, 25, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Carrera, C.; Podlipnik, S. Does acral melanoma need a distinctive prognostic staging system? Br. J. Dermatol. 2022, 186, 923–924. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.E.; Won, C.H.; Chang, S.E.; Lee, M.W.; Lee, W.J. Clinical and Prognostic Influence of Tumor Diameter in Acral Lentiginous Melanoma. J. Am. Acad. Dermatol. 2022. [Google Scholar] [CrossRef]
- Ishida, Y.; Agata, Y.; Shibahara, K.; Honjo, T. Induced expression of PD-1, a novel member of the immunoglobulin gene superfamily, upon programmed cell death. EMBO J. 1992, 11, 3887–3895. [Google Scholar] [CrossRef]
- Weber, J.; Del Vecchio, M.; Mandala, M.; Gogas, H.; Fernandez, A.A.; Dalle, S.; Cowey, C.L.; Schenker, M.; Grob, J.J.; Sileni, V.C.; et al. 1076O Adjuvant nivolumab (NIVO) vs ipilimumab (IPI) in resected stage III/IV melanoma: 4-y recurrence-free and overall survival (OS) results from CheckMate 238. Ann. Oncol. 2020, 31, S731–S732. [Google Scholar] [CrossRef]
- Ascierto, P.A.; Del Vecchio, M.; Mandalá, M.; Gogas, H.; Arance, A.M.; Dalle, S.; Cowey, C.L.; Schenker, M.; Grob, J.J.; Chiarion-Sileni, V.; et al. Adjuvant nivolumab versus ipilimumab in resected stage IIIB-C and stage IV melanoma (CheckMate 238): 4-year results from a multicentre, double-blind, randomised, controlled, phase 3 trial. Lancet Oncol. 2020, 21, 1465–1477. [Google Scholar] [CrossRef]
- Eggermont, A.M.; Blank, C.U.; Mandala, M.; Long, G.V.; Atkinson, V.; Dalle, S.; Haydon, A.; Lichinitser, M.; Khattak, A.; Carlino, M.S.; et al. Adjuvant Pembrolizumab versus Placebo in Resected Stage III Melanoma. N. Engl. J. Med. 2018, 378, 1789–1801. [Google Scholar] [CrossRef]
- Eggermont, A.M.; Blank, C.U.; Mandalà, M.; Long, G.V.; Atkinson, V.G.; Dalle, S.; Haydon, A.M.; Meshcheryakov, A.; Khattak, A.; Carlino, M.S.; et al. Adjuvant pembrolizumab versus placebo in resected stage III melanoma (EORTC 1325-MG/KEYNOTE-054): Distant metastasis-free survival results from a double-blind, randomised, controlled, phase 3 trial. Lancet Oncol. 2021, 22, 643–654. [Google Scholar] [CrossRef]
- Larkin, J.; Weber, J.; Del Vecchio, M.; Gogas, H.; Arance, A.M.; Dalle, S.; Cowey, C.L.; Schenker, M.; Grob, J.J.; Chiarion-Sileni, V.; et al. Adjuvant nivolumab versus ipilimumab (CheckMate 238 trial): Reassessment of 4-year efficacy outcomes in patients with stage III melanoma per AJCC-8 staging criteria. Eur. J. Cancer 2022, 173, 285–296. [Google Scholar] [CrossRef]
- He, Z.; Xin, Z.; Yang, Q.; Wang, C.; Li, M.; Rao, W.; Du, Z.; Bai, J.; Guo, Z.; Ruan, X.; et al. Mapping the single-cell landscape of acral melanoma and analysis of the molecular regulatory network of the tumor microenvironments. Elife 2022, 11, e78616. [Google Scholar] [CrossRef]
- Si, L.; Zhang, X.; Shu, Y.; Pan, H.; Wu, D.; Liu, J.; Lou, F.; Mao, L.; Wang, X.; Wen, X.; et al. A Phase Ib Study of Pembrolizumab as Second-Line Therapy for Chinese Patients With Advanced or Metastatic Melanoma (KEYNOTE-151). Transl. Oncol. 2019, 12, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.; Chi, Z.; Chen, Y.; Liu, X.; Wu, D.; Chen, J.; Somg, X.; Wang, W.; Dong, L.; Song, H.; et al. Safety, Efficacy, and Biomarker Analysis of Toripalimab in Previously Treated Advanced Melanoma: Results of the POLARIS-01 Multicenter Phase II Trial. Clin. Cancer Res. 2020, 26, 4250–4259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, X.; Shoushtari, A.N.; Warner, A.B.; Si, L.; Tang, B.; Cui, C.; Yang, X.; Wei, X.; Quach, H.T.; Cann, C.G.; et al. Benefit and toxicity of programmed death-1 blockade vary by ethnicity in patients with advanced melanoma: An international multicentre observational study. Br. J. Dermatol. 2022, 187, 401–410. [Google Scholar] [CrossRef]
- Eggermont, A.M.; Blank, C.U.; Mandala, M.; Long, G.V.; Atkinson, V.G.; Dalle, S.; Haydon, A.M.; Meshcheryakov, A.; Khattak, A.; Carlino, M.S.; et al. Longer Follow-Up Confirms Recurrence-Free Survival Benefit of Adjuvant Pembrolizumab in High-Risk Stage III Melanoma: Updated Results From the EORTC 1325-MG/KEYNOTE-054 Trial. J. Clin. Oncol. 2020, 38, 3925–3936. [Google Scholar] [CrossRef] [PubMed]
- Yokota, K.; Uchi, H.; Uhara, H.; Yoshikawa, S.; Takenouchi, T.; Inozume, T.; Ozawa, K.; Ihn, H.; Fujisawa, Y.; Qureshi, A.; et al. Adjuvant therapy with nivolumab versus ipilimumab after complete resection of stage III/IV melanoma: Japanese subgroup analysis from the phase 3 CheckMate 238 study. J. Dermatol. 2019, 46, 1197–1201. [Google Scholar] [CrossRef]
- Grossmann, K.F.; Othus, M.; Tarhini, A.A.; Patel, S.P.; Moon, J.; Sondak, V.K.; Kirkwood, J.M.; Ribas, A. SWOG S1404: A phase III randomized trial comparing standard of care adjuvant therapy to pembrolizumab in patients with high risk resected melanoma. J. Clin. Oncol. 2016, 34 (Suppl. 15), e21032. [Google Scholar] [CrossRef]
- Grossmann, K.F.; Othus, M.; Patel, S.P.; Tarhini, A.A.; Sondak, V.K.; Petrella, T.M.; Truong, T.G.; Khushalani, N.I.; Cohen, J.V.; Buchbinder, E.I.; et al. Final analysis of overall survival (OS) and relapse-free-survival (RFS) in the intergroup S1404 phase III randomized trial comparing either high-dose interferon (HDI) or ipilimumab to pembrolizumab in patients with high-risk resected melanoma. J. Clin. Oncol. 2021, 39, 9501. [Google Scholar] [CrossRef]
- Lian, B.; Si, L.; Chi, Z.H.; Sheng, X.N.; Kong, Y.; Wang, X.; Tian, H.; Li, K.; Mao, L.L.; Bai, X.; et al. Toripalimab (anti-PD-1) versus high-dose interferon-α2b as adjuvant therapy in resected mucosal melanoma: A phase II randomized trial. Ann. Oncol. 2022, 33, 1061–1070. [Google Scholar] [CrossRef]
- Hauschild, A.; Gogas, H.; Tarhini, A.; Middleton, M.R.; Testori, A.; Dréno, B.; Kirkwood, J.M. Practical guidelines for the management of interferon-alpha-2b side effects in patients receiving adjuvant treatment for melanoma: Expert opinion. Cancer 2008, 112, 982–994. [Google Scholar] [CrossRef]
- Trinh, V.A.; Zobniw, C.; Hwu, W.J. The efficacy and safety of adjuvant interferon-alfa therapy in the evolving treatment landscape for resected high-risk melanoma. Expert. Opin. Drug Saf. 2017, 16, 933–940. [Google Scholar] [CrossRef]
- Kilbridge, K.L.; Cole, B.F.; Kirkwood, J.M.; Haluska, F.G.; Atkins, M.A.; Ruckdeschel, J.C.; Sock, D.E.; Nease Jr, R.F.; Weeks, J.C. Quality-of-life-adjusted survival analysis of high-dose adjuvant interferon alpha-2b for high-risk melanoma patients using intergroup clinical trial data. J. Clin. Oncol. 2002, 20, 1311–1318. [Google Scholar] [CrossRef] [PubMed]
- Dixon, S.; Walters, S.J.; Turner, L.; Hancock, B.W. Quality of life and cost-effectiveness of interferon-alpha in malignant melanoma: Results from randomised trial. Br. J. Cancer 2006, 94, 492–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, L.; Si, L.; Chi, Z.; Cui, C.; Sheng, X.; Li, S.; Tang, B.; Guo, J. A randomised phase II trial of 1 month versus 1 year of adjuvant high-dose interferon α-2b in high-risk acral melanoma patients. Eur. J. Cancer 2011, 47, 1498–1503. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, J.; Li, D.; Wen, X.; Ding, Y.; Liu, X.; Jiang, H.; Huang, F.; Zhang, X. Adjuvant PD-1 inhibitor versus high-dose interferon α-2b for Chinese patients with cutaneous and acral melanoma: A retrospective cohort analysis. Dermatol. Ther. 2021, 34, e15067. [Google Scholar] [CrossRef]
- Li, T.; Jia, D.D.; Teng, L.S. Adjuvant pembrolizumab versus high-dose interferon α-2b for Chinese patients with resected stage III melanoma: A retrospective cohort study. Invest. New Drugs 2020, 38, 1334–1341. [Google Scholar] [CrossRef] [PubMed]
- Menzies, A.M.; Long, G.V. Systemic treatment for BRAF-mutant melanoma: Where do we go next? Lancet Oncol. 2014, 15, e371–e381. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | PD-1 (%) n = 126 | IFN (%) n = 31 | OBS (%) n = 42 | p Value |
|---|---|---|---|---|
| Gender | 0.201 | |||
| Female | 63 (50.0%) | 11 (35.5%) | 16 (38.1%) | |
| Male | 63 (50.0%) | 20 (64.5%) | 26 (61.9%) | |
| Age | 0.148 | |||
| <60 yrs | 60 (47.6%) | 17 (54.8%) | 14 (33.3%) | |
| ≥60 yrs | 66 (52.4%) | 14 (45.2%) | 28 (66.7%) | |
| Subtype | 0.191 | |||
| Acral | 84 (66.7%) | 18 (58.1%) | 34 (81.0%) | |
| Cutaneous | 34 (27.0%) | 9 (29.0%) | 7 (16.7%) | |
| Unknown primary | 8 (6.3%) | 4 (12.9%) | 1 (2.4%) | |
| Gene Mutation | 0.060 | |||
| BRAF | 23 (18.3%) | 6 (19.4%) | 12 (28.6%) | |
| KIT | 10 (7.9%) | 1 (3.2%) | 4 (9.5%) | |
| NRAS | 24 (19.0%) | 2 (6.4%) | 8 (19.0%) | |
| Wildtype | 58 (46.0%) | 13 (41.9%) | 13 (31.0%) | |
| Untested | 11 (8.7%) | 9 (29.0%) | 5 (11.9%) | |
| T stage | 0.532 | |||
| T0 | 8 (6.3%) | 4 (12.9%) | 1 (2.4%) | |
| T1 | 5 (4.0%) | 3 (9.7%) | 1 (2.4%) | |
| T2 | 16 (12.7%) | 3 (9.7%) | 5 (11.9%) | |
| T3 | 36 (28.6%) | 10 (32.3%) | 15 (35.7%) | |
| T4 | 61 (48.4%) | 11 (35.5%) | 20 (47.6%) | |
| Ulceration | 0.573 | |||
| No | 40 (33.9%) | 7 (25.9%) | 11 (26.8%) | |
| Yes | 78 (66.1%) | 20 (74.1%) | 30 (73.2%) | |
| Nodal Involvement | 0.727 | |||
| Micrometastasis | 70 (55.6%) | 15 (48.4%) | 24 (57.1%) | |
| Macrometastasis | 56 (44.4%) | 16 (51.6%) | 18 (42.9%) | |
| N stage | 0.215 | |||
| N1 | 56 (44.4%) | 19 (61.3%) | 18 (42.9%) | |
| N2 | 39 (31.0%) | 9 (29.0%) | 17 (40.5%) | |
| N3 | 31 (24.6%) | 3 (9.7%) | 7 (16.7%) | |
| Stage III Subgroup | 0.217 | |||
| IIIA | 13 (10.3%) | 4 (12.9%) | 2 (4.8%) | |
| IIIB | 15 (11.9%) | 8 (25.8%) | 9 (21.4%) | |
| IIIC | 82 (65.1%) | 18 (58.1%) | 28 (66.7%) | |
| IIID | 16 (12.7%) | 1 (3.2%) | 3 (7.1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, T.; Xu, Y.; Sun, W.; Yan, W.; Wang, C.; Hu, T.; Zhang, X.; Luo, Z.; Liu, X.; Chen, Y. Adjuvant Anti-PD-1 Immunotherapy versus Conventional Therapy for Stage III Melanoma: A Real-World Retrospective Cohort Study. Pharmaceuticals 2023, 16, 41. https://doi.org/10.3390/ph16010041
Li T, Xu Y, Sun W, Yan W, Wang C, Hu T, Zhang X, Luo Z, Liu X, Chen Y. Adjuvant Anti-PD-1 Immunotherapy versus Conventional Therapy for Stage III Melanoma: A Real-World Retrospective Cohort Study. Pharmaceuticals. 2023; 16(1):41. https://doi.org/10.3390/ph16010041
Chicago/Turabian StyleLi, Tong, Yu Xu, Wei Sun, Wangjun Yan, Chunmeng Wang, Tu Hu, Xiaowei Zhang, Zhiguo Luo, Xin Liu, and Yong Chen. 2023. "Adjuvant Anti-PD-1 Immunotherapy versus Conventional Therapy for Stage III Melanoma: A Real-World Retrospective Cohort Study" Pharmaceuticals 16, no. 1: 41. https://doi.org/10.3390/ph16010041