
Evaluation of Safety, Tolerability and Pharmacokinetic Characteristics of SA001 and Its Active Metabolite Rebamipide after Single and Multiple Oral Administration

Abstract
:1. Introduction
2. Results
2.1. Study Population
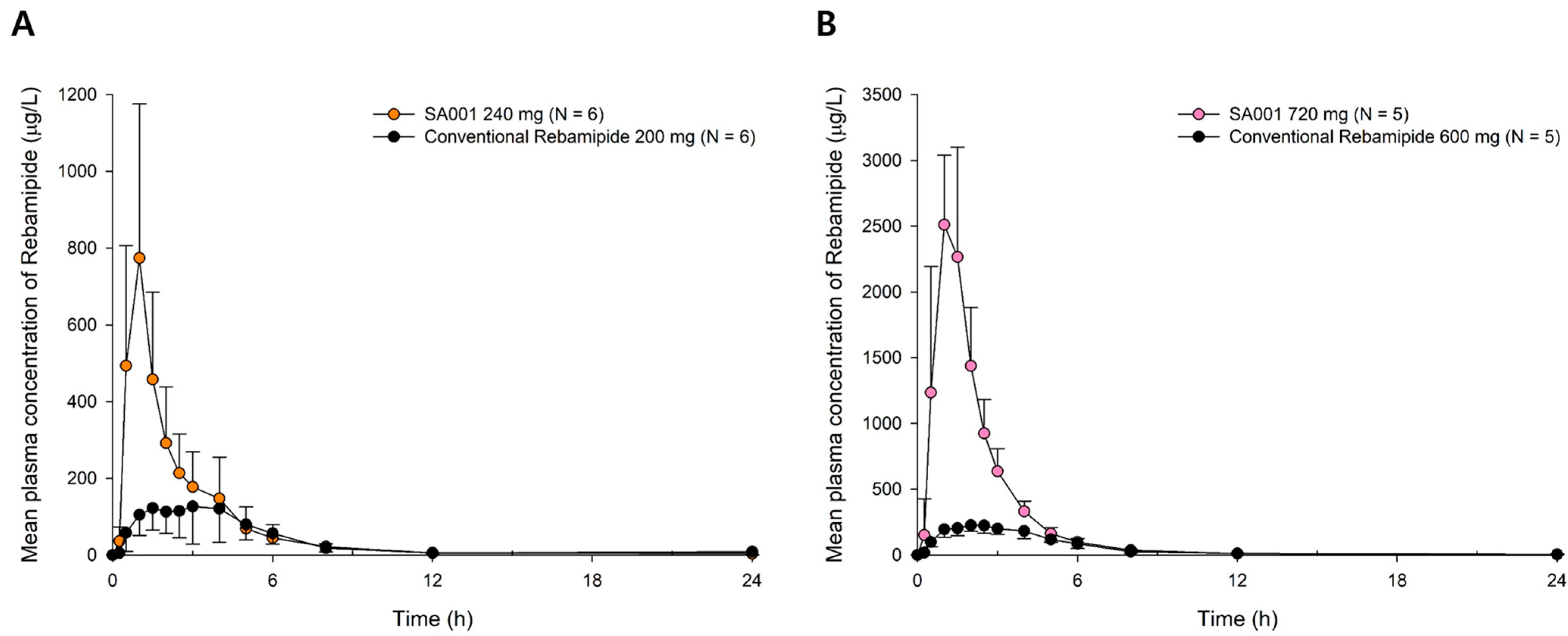
2.2. Pharmacokinetics
2.3. Safety and Tolerability
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Study Design
4.3. Pharmacokinetic Evaluation
4.4. Safety and Tolerability Evaluation
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barabino, S.; Labetoulle, M.; Rolando, M.; Messmer, E.M. Understanding Symptoms and Quality of Life in Patients with Dry Eye Syndrome. Ocul. Surf. 2016, 14, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Stapleton, F.; Alves, M.; Bunya, V.Y.; Jalbert, I.; Lekhanont, K.; Malet, F.; Na, K.S.; Schaumberg, D.; Uchino, M.; Vehof, J.; et al. Tfos Dews Ii epidemiology report. Ocul. Surf. 2017, 15, 334–365. [Google Scholar] [CrossRef] [PubMed]
- Tsubota, K.; Pflugfelder, S.C.; Liu, Z.; Baudouin, C.; Kim, H.M.; Messmer, E.M.; Kruse, F.; Liang, L.; Carreno-Galeano, J.T.; Rolando, M.; et al. Defining Dry Eye from a Clinical Perspective. Int. J. Mol. Sci. 2020, 21, 9271. [Google Scholar] [CrossRef] [PubMed]
- Messmer, E.M. The Pathophysiology, Diagnosis, and Treatment of Dry Eye Disease. Dtsch. Arztebl. Int. 2015, 112, 71–81. [Google Scholar] [CrossRef] [Green Version]
- Gupta, P.K.; Asbell, P.; Sheppard, J. Current and Future Pharmacological Therapies for the Management of Dry Eye. Eye Contact Lens 2020, 46 (Suppl. S2), S64–S69. [Google Scholar] [CrossRef]
- Jones, L.; Downie, L.E.; Korb, D.; Benitez-Del-Castillo, J.M.; Dana, R.; Deng, S.X.; Dong, P.N.; Geerling, G.; Hida, R.Y.; Liu, Y.; et al. Tfos Dews Ii Management and Therapy Report. Ocul. Surf. 2017, 15, 575–628. [Google Scholar] [CrossRef]
- Arakawa, T.; Higuchi, K.; Fujiwara, Y.; Watanabe, T.; Tominaga, K.; Sasaki, E.; Oshitani, N.; Yoshikawa, T.; Tarnawski, A.S. 15th Anniversary of Rebamipide: Looking Ahead to the New Mechanisms and New Applications. Dig. Dis. Sci. 2005, 50 (Suppl. S1), S3–S11. [Google Scholar] [CrossRef]
- Ríos, J.D.; Shatos, M.; Urashima, H.; Tran, H.; Dartt, D.A. Opc-12759 Increases Proliferation of Cultured Rat Conjunctival Goblet Cells. Cornea 2006, 25, 573–581. [Google Scholar] [CrossRef]
- Ríos, J.D.; Shatos, M.A.; Urashima, H.; Dartt, D.A. Effect of Opc-12759 on Egf Receptor Activation, P44/P42 Mapk Activity, and Secretion in Conjunctival Goblet Cells. Exp. Eye Res. 2008, 86, 629–636. [Google Scholar] [CrossRef]
- Urashima, H.; Takeji, Y.; Okamoto, T.; Fujisawa, S.; Shinohara, H. Rebamipide Increases Mucin-Like Substance Contents and Periodic Acid Schiff Reagent-Positive Cells Density in Normal Rabbits. J. Ocul. Pharmacol. Ther. 2012, 28, 264–270. [Google Scholar] [CrossRef]
- Ohguchi, T.; Kojima, T.; Ibrahim, O.M.; Nagata, T.; Shimizu, T.; Shirasawa, T.; Kawakita, T.; Satake, Y.; Tsubota, K.; Shimazaki, J.; et al. The Effects of 2% Rebamipide Ophthalmic Solution on the Tear Functions and Ocular Surface of the Superoxide Dismutase-1 (Sod1) Knockout Mice. Investig. Ophthalmol. Vis. Sci. 2013, 54, 7793–7802. [Google Scholar] [CrossRef] [Green Version]
- Jin-Sil, P.; Sun-Hee, H.; SeungCheon, Y.; JeongWon, C.; Kyung-Ah, J.; Mi-La, C.; Sung-Hwan, P. Immune Modulation by Rebamipide in a Mouse Model of Sjogren’s Syndrome Via T and B Cell Regulation. Immunol. Lett. 2019, 214, 1–7. [Google Scholar] [CrossRef]
- Min, H.K.; Kim, J.K.; Lee, S.Y.; Kim, E.K.; Lee, S.H.; Lee, J.; Kwok, S.K.; Cho, M.L.; Park, S.H. Rebamipide Prevents Peripheral Arthritis and Intestinal Inflammation by Reciprocally Regulating Th17/Treg Cell Imbalance in Mice with Curdlan-Induced Spondyloarthritis. J. Transl. Med. 2016, 14, 190. [Google Scholar] [CrossRef] [Green Version]
- Sugai, S.; Takahashi, H.; Ohta, S.; Nishinarita, M.; Takei, M.; Sawada, S.; Yamaji, K.; Oka, H.; Umehara, H.; Koni, I.; et al. Efficacy and Safety of Rebamipide for the Treatment of Dry Mouth Symptoms in Patients with Sjögren’s Syndrome: A Double-Blind Placebo-Controlled Multicenter Trial. Mod. Rheumatol. 2009, 19, 114–124. [Google Scholar] [CrossRef]
- Ogasawara, N.; Sasaki, M.; Hijikata, Y.; Masui, R.; Tanida, S.; Kanematsu, T.; Kamiya, T.; Kataoka, H.; Joh, T.; Kasugai, K. Successful Treatment for Pouchitis with Rebamipide Refractory to a Combination of Metronidazole (Mnz) and Ciprofloxacin (Cfx). Clin. J. Gastroenterol. 2009, 2, 404–407. [Google Scholar] [CrossRef]
- Kinoshita, S.; Awamura, S.; Oshiden, K.; Nakamichi, N.; Suzuki, H.; Yokoi, N. Rebamipide (Opc-12759) in the Treatment of Dry Eye: A Randomized, Double-Masked, Multicenter, Placebo-Controlled Phase Ii Study. Ophthalmology 2012, 119, 2471–2478. [Google Scholar] [CrossRef]
- Kinoshita, S.; Oshiden, K.; Awamura, S.; Suzuki, H.; Nakamichi, N.; Yokoi, N. A Randomized, Multicenter Phase 3 Study Comparing 2% Rebamipide (Opc-12759) with 0.1% Sodium Hyaluronate in the Treatment of Dry Eye. Ophthalmology 2013, 120, 1158–1165. [Google Scholar] [CrossRef]
- United States District Court. Otsuka Pharmaceutical Co. V. Torrent Pharmaceuticals Ltd, 99 F. Supp. 3d 461; United States District Court: Camden, NJ, USA, 2015. [Google Scholar]
- Bertens, C.J.F.; Gijs, M.; van den Biggelaar, F.; Nuijts, R. Topical Drug Delivery Devices: A Review. Exp. Eye Res. 2018, 168, 149–160. [Google Scholar] [CrossRef]
- Narala, A.; Guda, S.; Veerabrahma, K. Lipid Nanoemulsions of Rebamipide: Formulation, Characterization, and in Vivo Evaluation of Pharmacokinetic and Pharmacodynamic Effects. AAPS PharmSciTech 2019, 20, 26. [Google Scholar] [CrossRef]
- Markovic, M.; Zur, M.; Dahan, A.; Cvijić, S. Biopharmaceutical Characterization of Rebamipide: The Role of Mucus Binding in Regional-Dependent Intestinal Permeability. Eur. J. Pharm. Sci. 2020, 152, 105440. [Google Scholar] [CrossRef]
- Shi, Y.; Zou, M.; An, Y.; Ji, Z.; Gao, P.; Cheng, G. A Potent Preparation Method Combining Neutralization with Microfluidization for Rebamipide Nanosuspensions and Its in Vivo Evaluation. Drug Dev. Ind. Pharm. 2013, 39, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.T.; Lee, J.Y.; Park, J.H.; Cho, H.J.; Yoon, I.S.; Kim, D.D. Capmul Mcm/Solutol Hs15-Based Microemulsion for Enhanced Oral Bioavailability of Rebamipide. J. Nanosci. Nanotechnol. 2017, 17, 2340–2344. [Google Scholar] [CrossRef] [PubMed]
- Okawa, S.; Sumimoto, Y.; Masuda, K.; Ogawara, K.I.; Maruyama, M.; Higaki, K. Improvement of Lipid Solubility and Oral Bioavailability of a Poorly Water- and Poorly Lipid-Soluble Drug, Rebamipide, by Utilizing Its Counter Ion and Snedds Preparation. Eur. J. Pharm. Sci. 2021, 159, 105721. [Google Scholar] [CrossRef] [PubMed]
- Dhaneshwar, S.S.; Sharma, M.; Patel, V.; Desai, U.; Bhojak, J. Prodrug Strategies for Antihypertensives. Curr. Top. Med. Chem. 2011, 11, 2299–2317. [Google Scholar] [CrossRef] [PubMed]
- Barot, M.; Bagui, M.; Gokulgandhi, M.R.; Mitra, A.K. Prodrug Strategies in Ocular Drug Delivery. Med. Chem. 2012, 8, 753–768. [Google Scholar] [CrossRef] [Green Version]
- Hurwitz, S.J.; Schinazi, R.F. Prodrug Strategies for Improved Efficacy of Nucleoside Antiviral Inhibitors. Curr. Opin. HIV AIDS 2013, 8, 556–564. [Google Scholar] [CrossRef]
- Akamatsu, T.; Nakamura, N.; Furuya, N.; Shimizu, T.; Gotou, A.; Kiyosawa, K.; Katsuyama, T.; Osumi, T.; Hirao, Y.; Miyamoto, G. Local Gastric and Serum Concentrations of Rebamipide Following Oral Ingestion in Healthy Volunteers. Dig. Dis. Sci. 2002, 47, 1399–1404. [Google Scholar] [CrossRef]
- Kim, J.H.; Park, S.H.; Cho, C.S.; Lee, S.T.; Yoo, W.H.; Kim, S.K.; Kang, Y.M.; Rew, J.S.; Park, Y.W.; Lee, S.K.; et al. Preventive Efficacy and Safety of Rebamipide in Nonsteroidal Anti-Inflammatory Drug-Induced Mucosal Toxicity. Gut Liver 2014, 8, 371–379. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.H.; Lee, H.L.; Joo, M.K.; Park, H.J.; Jung, S.W.; Lee, O.J.; Kim, H.; Chun, H.J.; Lee, S.T.; Kim, J.W.; et al. Efficacy and Safety of Rebamipide Versus Its New Formulation, Ad-203, in Patients with Erosive Gastritis: A Randomized, Double-Blind, Active Control, Noninferiority, Multicenter, Phase 3 Study. Gut Liver 2021, 15, 841–850. [Google Scholar] [CrossRef]
- FDA (Ed.) Guidance for Industry: Estimating the Maximum Safe Starting Dose in Adult Healthy Volunteer; FDA: Rockville, MD, USA, 2005. [Google Scholar]
- Nair, A.B.; Jacob, S. A Simple Practice Guide for Dose Conversion between Animals and Human. J. Basic Clin. Pharm. 2016, 7, 27–31. [Google Scholar] [CrossRef]
- Matsuda, T.; Ohno, S.; Hirohata, S.; Miyanaga, Y.; Ujihara, H.; Inaba, G.; Nakamura, S.; Tanaka, S.; Kogure, M.; Mizushima, Y. Efficacy of Rebamipide as Adjunctive Therapy in the Treatment of Recurrent Oral Aphthous Ulcers in Patients with Behçet’s Disease: A Randomised, Double-Blind, Placebo-Controlled Study. Drugs R D 2003, 4, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Fujimori, S.; Takahashi, Y.; Gudis, K.; Seo, T.; Ehara, A.; Kobayashi, T.; Mitsui, K.; Yonezawa, M.; Tanaka, S.; Tatsuguchi, A.; et al. Rebamipide Has the Potential to Reduce the Intensity of Nsaid-Induced Small Intestinal Injury: A Double-Blind, Randomized, Controlled Trial Evaluated by Capsule Endoscopy. J. Gastroenterol. 2011, 46, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Kamada, T.; Sato, M.; Tokutomi, T.; Watanabe, T.; Murao, T.; Matsumoto, H.; Manabe, N.; Ito, M.; Tanaka, S.; Inoue, K.; et al. Rebamipide Improves Chronic Inflammation in the Lesser Curvature of the Corpus after Helicobacter Pylori Eradication: A Multicenter Study. Biomed. Res. Int. 2015, 2015, 865146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ota, K.; Takeuchi, T.; Nouda, S.; Ozaki, H.; Kawaguchi, S.; Takahashi, Y.; Harada, S.; Edogawa, S.; Kojima, Y.; Kuramoto, T.; et al. Determination of the Adequate Dosage of Rebamipide, a Gastric Mucoprotective Drug, to Prevent Low-Dose Aspirin-Induced Gastrointestinal Mucosal Injury. J. Clin. Biochem. Nutr. 2016, 59, 231–237. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | SA001 60 mg (N = 6) | SA001 120 mg (N = 6) | SA001 180 mg (N = 6) | SA001 240 mg (N = 12) | SA001 300 mg (N = 6) | SA001 480 mg (N = 6) | SA001 720 mg (N = 5) | SA001 1080 mg (N = 6) | |
|---|---|---|---|---|---|---|---|---|---|
| SA001 | AUClast (μg ∗ h/L) | 5.76 ± 3.2 | 22.66 ± 11.69 | 59.12 ± 27.39 | 75.62 ± 39.13 | 98.81 ± 19.57 | 148.31 ± 42.56 | 348.64 ± 72.68 | 494.45 ± 128.20 |
| AUCinf (μg ∗ h/L) | 5.88 ± 3.21 | 22.91 ± 11.74 | 59.37 ± 27.35 | 75.97 ± 39.02 | 99.03 ± 19.71 | 148.80 ± 42.56 | 349.76 ± 72.80 | 495.44 ± 128.21 | |
| Cmax (μg/L) | 10.17 ± 6.7 | 47.56 ± 28.89 | 90.97 ± 61.92 | 100.71 ± 55.14 | 127.28 ± 21.03 | 192.52 ± 114.76 | 357.11 ± 149.04 | 495.27 ± 127.46 | |
| Tmax (h) | 0.4 (0.25, 1) | 0.5 (0.25, 1.5) | 0.5 (0.25, 1) | 0.5 (0.25, 1) | 0.5 (0.25, 1) | 0.5 (0.5, 1) | 1 (0.25, 1) | 0.75 (0.5, 2) | |
| Vz/F (L) | 11,222.46 ± 5808.18 | 8241 ± 7939.24 | 3826.44 ± 1925.96 | 4411.57 ± 2159.06 | 3681.79 ± 927.36 | 3931.61 ± 1094.99 | 2437.95 ± 628.76 | 2900.52 ± 572.15 | |
| CL/F (L/h) | 13,513.85 ± 7527.99 | 7430.12 ± 5249.91 | 3644.35 ± 1673.25 | 4032.10 ± 1969.11 | 3135.34 ± 645.44 | 3434.60 ± 901.37 | 2147.28 ± 542.00 | 2304.11 ± 584.09 | |
| t1/2 (h) | 0.59 ± 0.07 | 0.76 ± 0.25 | 0.72 ± 0.04 | 0.76 ± 0.89 | 0.84 ± 0.29 | 0.79 ± 0.08 | 0.80 ± 0.16 | 0.90 ± 0.22 | |
| MRTlast (h) ** | 0.84 ± 0.31 | 0.83 ± 0.28 | 0.90 ± 0.21 | 0.97 ± 0.20 | 1.03 ± 0.38 | 1.00 ± 0.23 | 1.23 ± 0.27 | 1.31 ± 0.40 | |
| Rebamipide | AUClast (μg ∗ h/L) | 378.39 ± 142.89 | 591.41 ± 265.58 | 1203.37 ± 404.34 | 1725.48 ± 745.67 | 2352.47 ± 700.48 | 2485.45 ± 358.24 | 5331.31 ± 1022.09 | 6705.68 ± 3193.37 |
| AUCinf (μg ∗ h/L) | 382.6 ± 142.39 | 599.48 ± 264.13 | 1227.52 ± 410.15 | 1743.88 ± 746.05 | 2436.55 ± 731.33 | 2498.92 ± 357.54 | 5399.58 ± 1078.78 | 6768.84 ± 3215.15 | |
| Cmax (μg/L) | 175.95 ± 50.12 | 344.94 ± 209.99 | 701.67 ± 184.94 | 958.11 ± 449.01 | 1148.74 ± 286.65 | 1415.42 ± 290.40 | 2772.00 ± 452.31 | 3458.74 ± 715.20 | |
| Tmax (h) | 0.75 (0.5, 1) | 0.5 (0.5, 1) | 1 (0.5, 1) | 1 (0.5, 1) | 1 (0.5, 1.5) | 0.5 (0.5, 1) | 1 (0.5, 1.5) | 1 (1, 2.5) | |
| t1/2 (h) | 1.85 ± 0.25 | 3.68 ± 2.13 | 10.56 ± 11.63 | 6.79 ± 5.96 * | 21.72 ± 13.03 | 2.27 ± 0.60 | 11.94 ± 13.56 | 7.72 ± 5.30 | |
| MRTlast (h) | 2.68 ± 0.40 | 2.92 ± 0.95 | 2.74 ± 0.56 | 2.80 ± 0.68 | 3.77 ± 0.58 | 2.35 ± 0.33 | 2.49 ± 0.45 | 2.62 ± 0.51 | |
| Metabolic ratio *** | 80.15 ± 41.66 | 28.44 ± 6.73 | 21.51 ± 3.64 | 25.35 ± 11.28 | 23.72 ± 4.76 | 17.33 ± 2.63 | 15.63 ± 3.20 | 13.47 ± 3.79 | |
| Parameter | SA001 360 mg (N = 6) | SA001 720 mg (N = 5) | SA001 1080 mg (N = 6) | ||||
|---|---|---|---|---|---|---|---|
| 180 mg b.i.d. | 120 mg t.i.d. | 360 mg b.i.d. | 240 mg t.i.d. | 540 mg b.i.d. | 360 mg t.i.d. | ||
| SA001 | AUC24h after the first dose (μg ∗ h/L) * | 70.18 ± 43.12 | 300.06 ± 137.61 | 352.14 ± 177.65 | |||
| AUC24h at steady state (μg ∗ h/L) * | 83.92 ± 26.95 | 76.23 ± 27.91 | 294.14 ± 134.65 | 285.86 ± 75.46 | 393.09 ± 125.71 | 456.06 ± 155.06 | |
| Cmax,ss (μg/L) | 53.71 ± 33.34 | 25.63 ± 13.65 | 160.82 ± 70.45 | 106.61 ± 27.65 | 226.03 ± 133.92 | 155.69 ± 50.43 | |
| Tmax,ss (h) | 0.5 (0.5, 4) | 0.8 (0.3, 3.0) | 0.5 (0.5, 2.03) | 0.5 (0.5, 1.77) | 0.75 (0.5, 3.0) | 0.5 (0.5, 1.5) | |
| RAUC24h * | 1.40 ± 0.54 | 1.23 ± 0.44 | 1.03 ± 0.28 | 1.09 ± 0.51 | 1.21 ± 0.30 | 1.49 ± 0.73 | |
| Rebamipide | AUC24h after the first dose (μg ∗ h/L) * | 2136.39 ± 914.52 | 5235.66 ± 1682.13 | 6415.98 ± 1866.11 | |||
| AUC24h at steady state (μg ∗ h/L) * | 2344.83 ± 629.89 | 2590.34 ± 877.18 | 5905.92 ± 2007.78 | 5961.95 ± 1456.02 | 7616.60 ± 2222.60 | 7978.21 ± 2332.03 | |
| Cmax,ss (μg/L) | 626.63 ± 222.76 | 380.12 ± 117.92 | 1266.13 ± 454.17 | 891.05 ± 255.37 | 2001.88 ± 616.93 | 1375.22 ± 309.73 | |
| Tmax,ss (h) | 1.0 (0.5, 4.0) | 1.25 (1.0, 3.02) | 1.5 (1.0, 2.03) | 1.0 (1.0, 1.77) | 1.0 (0.5, 3.0) | 1.0 (0.5, 2.03) | |
| RAUC24h * | 1.18 ± 0.28 | 1.26 ± 0.19 | 1.14 ± 0.19 | 1.23 ± 0.52 | 1.21 ± 0.28 | 1.25 ± 0.18 | |
| Parameter | SA001 240 mg (N = 6) | Conventional Rebamipide 200 mg (N = 6) | GMR * (90% CI) | SA001 720 mg (N = 5) | Conventional Rebamipide 600 mg (N = 5) | GMR * (90% CI) |
|---|---|---|---|---|---|---|
| AUClast (μg ∗ h/L) | 1516.87 ± 697.51 | 733.85 ± 344.36 | 5331.31 ± 1022.09 | 1220.53 ± 212.86 | ||
| AUClast/D (μg ∗ h/L/mg) ** | 8.23 ± 3.79 | 3.67 ± 1.72 | 2.20 (1.73–2.80) | 9.64 ± 1.85 | 2.03 ± 0.35 | 4.73 (3.46–6.46) |
| Cmax (μg/L) | 785.68 ± 393.39 | 158.73 ± 87.37 | 2772.00 ± 452.31 | 252.82 ± 46.06 | ||
| Cmax/D (μg/L/mg) ** | 4.26 ± 2.13 | 0.79 ± 0.44 | 5.45 (4.22–7.03) | 5.01 ± 0.82 | 0.42 ± 0.08 | 11.94 (8.73–16.32) |
| System Organ Class Preferred Term | Placebo (N = 6) | SA001 360 mg (N = 6) | SA001 720 mg (N = 6) | SA001 1080 mg (N = 6) | Total (N = 24) |
|---|---|---|---|---|---|
| Subjects with TEAEs | 0 | 1 (16.7) (2) | 6 (100.0) (9) | 1 (16.7) (3) | 8 (33.3) (14) |
| Gastrointestinal disorders | 0 | 1 (16.7) (2) | 0 | 0 | 1 (4.2) (2) |
| Nausea | 0 | 1 (16.7) (1) | 0 | 0 | 1 (4.2) (1) |
| Vomiting | 0 | 1 (16.7) (1) | 0 | 0 | 1 (4.2) (1) |
| General disorders and administration site conditions | 0 | 0 | 1 (16.7) (1) | 0 | 1 (4.2) (1) |
| Catheter site erythema | 0 | 0 | 1 (16.7) (1) | 0 | 1 (4.2) (1) |
| Infections and infestations | 0 | 0 | 1 (16.7) (1) | 0 | 1 (4.2) (1) |
| Oral pustule | 0 | 0 | 1 (16.7) (1) | 0 | 1 (4.2) (1) |
| Musculoskeletal and connective tissue disorders | 0 | 0 | 1 (16.7) (1) | 0 | 1 (4.2) (1) |
| Myalgia | 0 | 0 | 1 (16.7) (1] | 0 | 1 (4.2) (1) |
| Respiratory, thoracic and mediastinal disorders | 0 | 0 | 4 (66.7) (5) | 1 (16.7) (2) | 5 (20.8) (7) |
| Dyspnea | 0 | 0 | 1 (16.7) (1) | 0 | 1 (4.2) (1) |
| Epistaxis | 0 | 0 | 1 (16.7) (1) | 0 | 1 (4.2) (1) |
| Nasal congestion | 0 | 0 | 1 (16.7) (1) | 1 (16.7) (1) | 2 (8.3) (2) |
| Rhinorrhea | 0 | 0 | 2 (33.3) (2) | 1 (16.7) (1) | 3 (12.5) (3) |
| Skin and subcutaneous tissue disorders | 0 | 0 | 1 (16.7) (1) | 1 (16.7) (1) | 2 (8.3) (2) |
| Papule | 0 | 0 | 1 (16.7) (1) | 0 | 1 (4.2) (1) |
| Erythema | 0 | 0 | 0 | 1 (16.7) (1) | 1 (4.2) (1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, S.; Huh, K.Y.; Oh, J.; Yu, K.-S.; Kim, A. Evaluation of Safety, Tolerability and Pharmacokinetic Characteristics of SA001 and Its Active Metabolite Rebamipide after Single and Multiple Oral Administration. Pharmaceuticals 2023, 16, 132. https://doi.org/10.3390/ph16010132
Bae S, Huh KY, Oh J, Yu K-S, Kim A. Evaluation of Safety, Tolerability and Pharmacokinetic Characteristics of SA001 and Its Active Metabolite Rebamipide after Single and Multiple Oral Administration. Pharmaceuticals. 2023; 16(1):132. https://doi.org/10.3390/ph16010132
Chicago/Turabian StyleBae, Sungyeun, Ki Young Huh, Jaeseong Oh, Kyung-Sang Yu, and Anhye Kim. 2023. "Evaluation of Safety, Tolerability and Pharmacokinetic Characteristics of SA001 and Its Active Metabolite Rebamipide after Single and Multiple Oral Administration" Pharmaceuticals 16, no. 1: 132. https://doi.org/10.3390/ph16010132