
Dilemmas in the Choice of Adequate Therapeutic Treatment in Patients with Acute Pulmonary Embolism—From Modern Recommendations to Clinical Application

 , , , ,
, , , ,
Abstract
:1. From Diagnostic Doubts to the Correct Diagnosis of Pulmonary Embolism
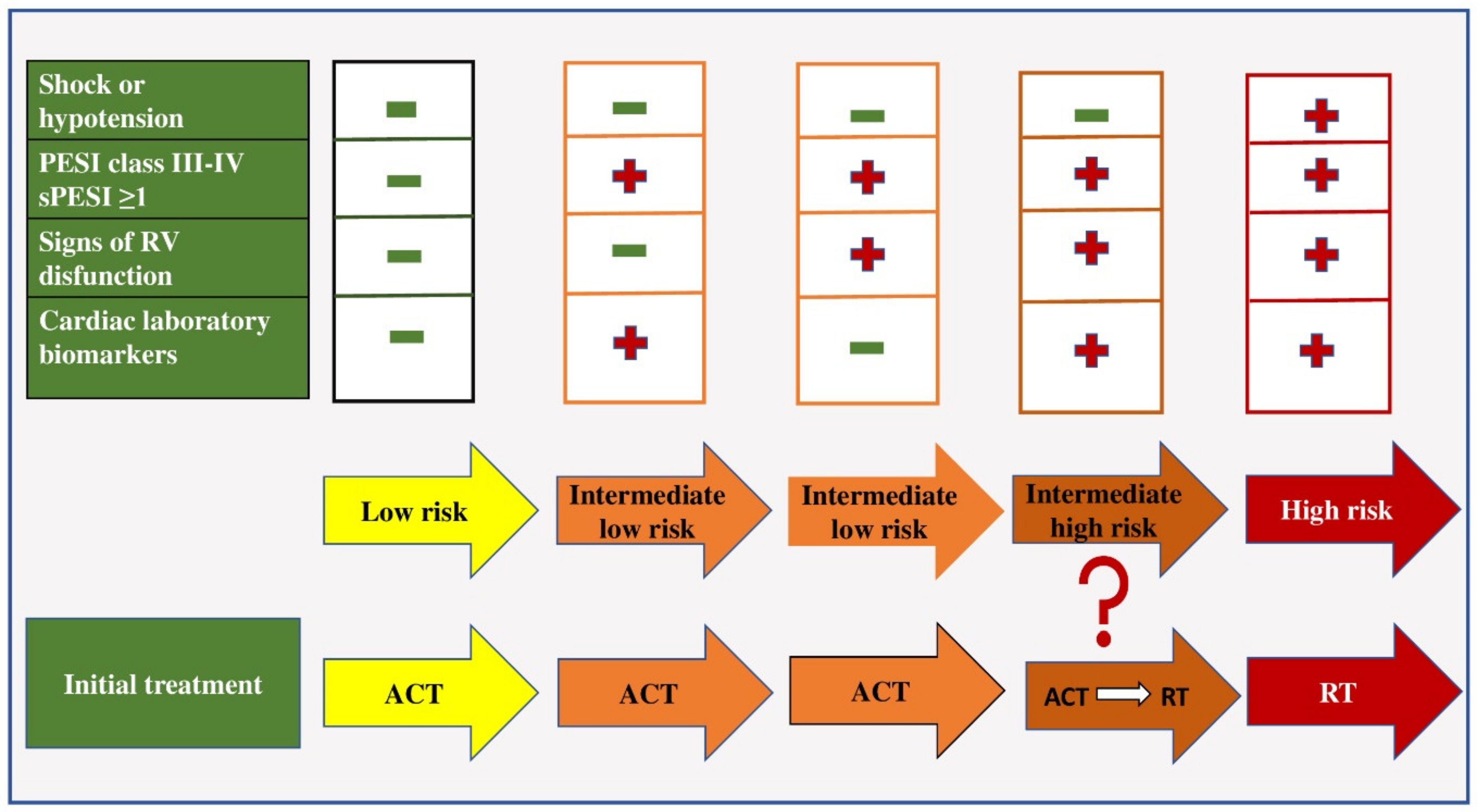
2. Risk Stratification in Patients with PE
3. Initial Therapeutic Regimen in the Acute Phase of PE
3.1. Anticoagulant Therapy
3.1.1. Unfractionated Heparin
3.1.2. Low-Molecular-Weight Heparin
3.1.3. Fondaparinux
3.1.4. Direct Thrombin Inhibitors
3.2. Thrombolytic Therapy
3.3. Embolectomy
3.3.1. Surgical Embolectomy
3.3.2. Percutaneous Catheter Embolectomy
3.4. Initial Therapeutic Regimen in Patients with Intermediate–High-Risk Pulmonary Embolism
4. Prolonged Treatment with Anticoagulant Therapy of Patients with PE
4.1. Vitamin K Antagonists
4.2. New Oral Anticoagulant Drugs
4.2.1. Apixaban
4.2.2. Rivaroxaban
4.2.3. Dabigatran
4.2.4. Edoxaban
4.2.5. Inhibitori Aktiviranog Faktora XIa
5. Treatment of PE in Specific Patient Populations
5.1. Treatment of PE in Pregnancy
5.2. Treatment of PE in Antiphospholipid Syndrome
5.3. Treatment of PE in Patients with Cancer
5.4. Treatment of PE in Elderly and Frail Patients
5.5. Treatment of PE in Patients with Renal Failure
5.6. Treatment of PE in Obese Patients
5.7. Treatment of PE in HIV Patients
5.8. Treatment of Patients with PE Who Have Epilepsy
5.9. Treatment of Chronic Thromboembolic Pulmonary Hypertension (CTEPH)
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heit, J.A.; Spencer, F.A.; White, R.H. The epidemiology of venous thromboembolism. J. Thromb. Thrombolysis 2016, 41, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Raskob, G.E.; Angchaisuksiri, P.; Blanco, A.N.; Buller, H.; Gallus, A.; Hunt, B.J.; Hylek, E.; Kakkar, A.; Konstantinides, S.V.; McCumber, M.; et al. ISTH Steering Committee for World Thrombosis Day. Thrombosis: A major contributor to global disease burden. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2363–2371. [Google Scholar] [CrossRef] [PubMed]
- Mazzolai, L.; Aboyans, V.; Ageno, W.; Agnelli, G.; Alatri, A.; Bauersachs, R.; Brekelmans, M.P.A.; Büller, H.R.; Elias, A.; Farge, D.; et al. Diagnosis and management of acute deep vein thrombosis: A joint consensus document from the European Society of Cardiology working groups of aorta and peripheral vascular diseases and pulmonary circulation and right ventricular function. Eur. Heart J. 2018, 39, 4208–4218. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed]
- Tsuyuki, H.; Yamamoto, N.; Unno, N.; Inuzuka, K.; Sano, M.; Katahashi, K.; Yata, T.; Kayama, T.; Yamanaka, Y.; Endo, Y.; et al. Characteristics and Prognostic Factors of Venous Thromboembolism in Cancer Patients. Ann. Vasc. Dis. 2022, 15, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Gussoni, G.; Frasson, S.; La Regina, M.; Di Micco, P.; Monreal, M. RIETE Investigators. Three-month mortality rate and clinical predictors in patients with venous thromboembolism and cancer. Findings from the RIETE registry. Thromb. Res. 2013, 131, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Gialeraki, A.; Valsami, S.; Pittaras, T.; Panayiotakopoulos, G.; Politou, M. Oral Contraceptives and HRT Risk of Thrombosis. Clin. Appl. Thromb. Hemost. 2018, 24, 217–225. [Google Scholar] [CrossRef]
- Kukla, P.; McIntyre, W.F.; Koracevic, G.; Kutlesic-Kurtovic, D.; Fijorek, K.; Atanaskovic, V.; Krupa, E.; Mirek-Bryniarska, E.; Jastrzębski, M.; Bryniarski, L.; et al. Relation of atrial fibrillation and right-sided cardiac thrombus to outcomes in patients with acute pulmonary embolism. Am. J. Cardiol. 2015, 115, 825–830. [Google Scholar] [CrossRef]
- Righini, M.; Robert-Ebadi, H.; Le Gal, G. Diagnosis of acute pulmonary embolism. J. Thromb. Haemost. 2017, 15, 1251–1261. [Google Scholar] [CrossRef]
- Morrone, D.; Morrone, V. Acute Pulmonary Embolism: Focus on the Clinical Picture. Korean Circ. J. 2018, 48, 365–381. [Google Scholar] [CrossRef] [Green Version]
- Nilsson, L.T.; Andersson, T.; Larsen, F.; Lang, I.M.; Liv, P.; Söderberg, S. Dyspnea after pulmonary embolism: A nation-wide population-based case-control study. Pulm. Circ. 2021, 11, 20458940211046831. [Google Scholar] [CrossRef]
- Pollack, C.V.; Schreiber, D.; Goldhaber, S.Z.; Slattery, D.; Fanikos, J.; O’Neil, B.J.; Thompson, J.R.; Hiestand, B.; Briese, B.A.; Pendleton, R.C.; et al. Clinical characteristics, management, and outcomes of patients diagnosed with acute pulmonary embolism in the emergency department: Initial report of EMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the Real World Registry). J. Am. Coll. Cardiol. 2011, 57, 700–706. [Google Scholar] [CrossRef]
- Stein, P.D.; Beemath, A.; Matta, F.; Weg, J.G.; Yusen, R.D.; Hales, C.A.; Hull, R.D.; Leeper, K.V.; Sostman, H.D., Jr.; Tapson, V.F.; et al. Clinical characteristics of patients with acute pulmonary embolism: Data from PIOPED II. Am. J. Med. 2007, 120, 871–879. [Google Scholar] [CrossRef]
- Stein, P.D.; Hull, R.D.; Kayali, F.; Ghali, W.A.; Alshab, A.K.; Olson, R.E. Venous thromboembolism according to age: The impact of an aging population. Arch. Intern. Med. 2004, 164, 2260–2265. [Google Scholar] [CrossRef]
- Ji, Q.Y.; Wang, M.F.; Su, C.M.; Yang, Q.F.; Feng, L.F.; Zhao, L.Y.; Fang, S.Y.; Zhao, F.H.; Li, W.M. Clinical symptoms and related risk factors in pulmonary embolism patients and cluster analysis based on these symptoms. Sci. Rep. 2017, 7, 14887. [Google Scholar] [CrossRef]
- Kucher, N.; Rossi, E.; De Rosa, M.; Goldhaber, S.Z. Massive pulmonary embolism. Circulation 2006, 113, 577–582. [Google Scholar] [CrossRef]
- Khan, F.; Tritschler, T.; Kahn, S.R.; Rodger, M.A. Venous thromboembolism. Lancet. 2021, 398, 64–77. [Google Scholar] [CrossRef]
- Tarbox, A.K.; Swaroop, M. Pulmonary embolism. Int. J. Crit. Illn. Inj. Sci. 2013, 3, 69–72. [Google Scholar]
- Righini, M.; Robert-Ebadi, H. Diagnosis of acute Pulmonary Embolism. Hamostaseologie 2018, 38, 11–21. [Google Scholar] [CrossRef]
- Kearon, C.; de Wit, K.; Parpia, S.; Schulman, S.; Afilalo, M.; Hirsch, A.; Spencer, F.A.; Sharma, S.; D’Aragon, F.; Deshaies, J.F.; et al. PEGeD Study Investigators. Diagnosis of Pulmonary Embolism with d-Dimer Adjusted to Clinical Probability. N. Engl. J. Med. 2019, 381, 2125–2134. [Google Scholar] [CrossRef]
- Ziegler, T.; Murzik, M.; Schau, A.; Winkler, C.; Fünfstück, R. Interpretation erhöhter D-Dimerkonzentration [Interpretation of increased D-dimer values]. Hamostaseologie 2004, 24, 144–146. [Google Scholar]
- Shafiee, M.A.; Hosseini, S.F.; Mortazavi, M.; Emami, A.; Mojtahed Zadeh, M.; Moradi, S.; Shaker, P. Anticoagulation therapy in COVID-19 patients with chronic kidney disease. J. Res. Med. Sci. 2021, 26, 63. [Google Scholar] [CrossRef]
- Righini, M.; Goehring, C.; Bounameaux, H.; Perrier, A. Effects of age on the performance of common diagnostic tests for pulmonary embolism. Am. J. Med. 2000, 109, 357–361. [Google Scholar] [CrossRef]
- Righini, M.; Van Es, J.; Den Exter, P.L.; Roy, P.M.; Verschuren, F.; Ghuysen, A.; Rutschmann, O.T.; Sanchez, O.; Jaffrelot, M.; Trinh-Duc, A.; et al. Age-adjusted D-dimer cutoff levels to rule out pulmonary embolism: The ADJUST-PE study. JAMA 2014, 311, 1117–1124. [Google Scholar] [CrossRef]
- Van Es, N.; Kraaijpoel, N.; Klok, F.A.; Huisman, M.V.; Den Exter, P.L.; Mos, I.C.; Galipienzo, J.; Büller, H.R.; Bossuyt, P.M. The original and simplified Wells rules and age-adjusted D-dimer testing to rule out pulmonary embolism: An individual patient data meta-analysis. J. Thromb. Haemost. 2017, 15, 678–684. [Google Scholar] [CrossRef]
- Righini, M.; Robert-Ebadi, H.; Elias, A.; Sanchez, O.; Le Moigne, E.; Schmidt, J.; Le Gall, C.; Cornuz, J.; Aujesky, D.; Roy, P.M.; et al. CT-PE-Pregnancy Group. Diagnosis of Pulmonary Embolism During Pregnancy: A Multicenter Prospective Management Outcome Study. Ann. Intern. Med. 2018, 169, 766–773. [Google Scholar] [CrossRef]
- Tromeur, C.; van der Pol, L.M.; Le Roux, P.Y.; Ende-Verhaar, Y.; Salaun, P.Y.; Leroyer, C.; Couturaud, F.; Kroft, L.J.M.; Huisman, M.V.; Klok, F.A. Computed tomography pulmonary angiography versus ventilation-perfusion lung scanning for diagnosing pulmonary embolism during pregnancy: A systematic review and meta-analysis. Haematologica 2019, 104, 176–188. [Google Scholar] [CrossRef]
- Alonso-Martínez, J.L.; Sánchez, F.J.; Echezarreta, M.A. Delay and misdiagnosis in sub-massive and non-massive acute pulmonary embolism. Eur. J. Intern. Med. 2010, 21, 278–282. [Google Scholar] [CrossRef]
- Van der Hulle, T.; Cheung, W.Y.; Kooij, S.; Beenen, L.F.M.; van Bemmel, T.; van Es, J.; Faber, L.M.; Hazelaar, G.M.; Heringhaus, C.; Hofstee, H.; et al. YEARS study group. Simplified diagnostic management of suspected pulmonary embolism (the YEARS study): A prospective, multicentre, cohort study. Lancet 2017, 390, 289–297. [Google Scholar] [CrossRef]
- Kwok, C.S.; Wong, C.W.; Lovatt, S.; Myint, P.K.; Loke, Y.K. Misdiagnosis of pulmonary embolism and missed pulmonary embolism: A systematic review of the literature. Health Sci. Rev. 2022, 3, 100022. [Google Scholar] [CrossRef]
- Su, X.F.; Fan, N.; Yang, X.M.; Song, J.M.; Peng, Q.H.; Liu, X. A Novel Electrocardiography Model for the Diagnosis of Acute Pulmonary Embolism. Front. Cardiovasc. Med. 2022, 9, 825561. [Google Scholar] [CrossRef] [PubMed]
- Digby, G.C.; Kukla, P.; Zhan, Z.Q.; Pastore, C.A.; Piotrowicz, R.; Schapachnik, E.; Zareba, W.; Bayés de Luna, A.; Pruszczyk, P.; Baranchuk, A.M. The value of electrocardiographic abnormalities in the prognosis of pulmonary embolism: A consensus paper. Ann. Noninvasive Electrocardiol. 2015, 20, 207–223. [Google Scholar] [CrossRef] [PubMed]
- Vanni, S.; Polidori, G.; Vergara, R.; Pepe, G.; Nazerian, P.; Moroni, F.; Garbelli, E.; Daviddi, F.; Grifoni, S. Prognostic value of ECG among patients with acute pulmonary embolism and normal blood pressure. Am. J. Med. 2009, 122, 257–264. [Google Scholar] [CrossRef]
- Novicic, N.; Dzudovic, B.; Subotic, B.; Shalinger-Martinovic, S.; Obradovic, S. Electrocardiography changes and their significance during treatment of patients with intermediate-high and high-risk pulmonary embolism. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 271–278. [Google Scholar] [CrossRef]
- Ermıs, N.; Ermıs, H.; Sen, N.; Kepez, A.; Cuglan, B. QT dispersion in patients with pulmonary embolism. Wien. Klin. Wochenschr. 2010, 122, 691–697. [Google Scholar] [CrossRef]
- Ptaszynska-Kopczynska, K.; Kiluk, I.; Sobkowicz, B. Atrial Fibrillation in Patients with Acute Pulmonary Embolism: Clinical Significance and Impact on Prognosis. Biomed Res. Int. 2019, 2019, 7846291. [Google Scholar] [CrossRef]
- Kucher, N.; Walpoth, N.; Wustmann, K.; Noveanu, M.; Gertsch, M. QR in V1--an ECG sign associated with right ventricular strain and adverse clinical outcome in pulmonary embolism. Eur. Heart J. 2003, 24, 1113–1119. [Google Scholar] [CrossRef]
- Kurnicka, K.; Lichodziejewska, B.; Goliszek, S.; Dzikowska-Diduch, O.; Zdończyk, O.; Kozłowska, M.; Kostrubiec, M.; Ciurzyński, M.; Palczewski, P.; Grudzka, K.; et al. Echocardiographic Pattern of Acute Pulmonary Embolism: Analysis of 511 Consecutive Patients. J. Am. Soc. Echocardiogr. 2016, 29, 907–913. [Google Scholar] [CrossRef]
- McConnell, M.V.; Solomon, S.D.; Rayan, M.E.; Lee, R.T.; Come, P.C.; Goldhaber, S.Z.; Lee, R.T. Regional right ventricular dysfunction detected by echocardiography in acute pulmonary embolism. Am. J. Cardiol. 1996, 78, 469–473. [Google Scholar] [CrossRef]
- Casazza, F.; Bongarzoni, A.; Capozi, A.; Agostoni, O. Regional right ventricular dysfunction in acute pulmonary embolism and right ventricular infarction. Eur. J. Echocardiogr. 2005, 6, 11–14. [Google Scholar] [CrossRef]
- Shafiq, Q.; Assaly, R.; Kanjwal, Y. McConnell Sign in a Patient with Massive Acute Pulmonary Embolism. Case Rep. Cardiol. 2011, 2011, 201097. [Google Scholar] [CrossRef]
- Naeem, K. Floating thrombus in the right heart associated with pulmonary embolism: The role of echocardiography. Pak. J. Med. Sci. 2015, 31, 233–235. [Google Scholar] [CrossRef]
- Bĕlohlávek, J.; Dytrych, V.; Linhart, A. Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism. Exp. Clin. Cardiol. 2013, 18, 129–138. [Google Scholar]
- Elias, A.; Mallett, S.; Daoud-Elias, M.; Poggi, J.N.; Clarke, M. Prognostic models in acute pulmonary embolism: A systematic review and meta-analysis. BMJ 2016, 6, e010324. [Google Scholar] [CrossRef]
- Duffett, L.; Castellucci, L.A.; Forgie, M.A. Pulmonary embolism: Update on management and controversies. BMJ 2020, 370, m2177. [Google Scholar] [CrossRef]
- Mirambeaux, R.; León, F.; Bikdeli, B.; Morillo, R.; Barrios, D.; Mercedes, E.; Moores, L.; Tapson, V.; Yusen, R.D.; Jiménez, D. Intermediate-High Risk Pulmonary Embolism. TH Open 2019, 3, e356–e363. [Google Scholar] [CrossRef]
- Yamamoto, T. Management of patients with high-risk pulmonary embolism: A narrative review. J. Intensive Care. 2018, 6, 16. [Google Scholar] [CrossRef]
- Bledsoe, J.R.; Woller, S.C.; Stevens, S.M.; Aston, V.; Patten, R.; Allen, T.; Horne, B.D.; Dong, L.; Lloyd, J.; Snow, G.; et al. Management of Low-Risk Pulmonary Embolism Patients Without Hospitalization: The Low-Risk Pulmonary Embolism Prospective Management Study. Chest 2018, 154, 249–256. [Google Scholar] [CrossRef]
- Piazza, G. Advanced Management of Intermediate- and High-Risk Pulmonary Embolism: JACC Focus Seminar. J. Am. Coll. Cardiol. 2020, 76, 2117–2127. [Google Scholar] [CrossRef]
- Konstantinides, S.; Mavromanoli, A.; Hobohm, L. Diagnostik und Therapie der Lungenembolie [Diagnosis and treatment of pulmonary embolism]. Herz 2021, 46, 589–604. [Google Scholar] [CrossRef]
- Hirsh, J.; Anand, S.S.; Halperin, J.L.; Fuster, V. Mechanism of action and pharmacology of unfractionated heparin. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 1094–1096. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Lu, D.; Chen, Y.; Zhao, M.; Zuo, L. Unfractionated Heparin Promotes Osteoclast Formation in Vitro by Inhibiting Osteoprotegerin Activity. Int. J. Mol. Sci. 2016, 17, 613. [Google Scholar] [CrossRef] [PubMed]
- Capila, I.; Linhardt, R.J. Heparin-protein interactions. Angew. Chem. Int. Ed. Engl. 2002, 41, 391–412. [Google Scholar] [CrossRef]
- Chan, A.K.; Paredes, N.; Thong, B.; Chindemi, P.; Paes, B.; Berry, L.R.; Monagle, P. Binding of heparin to plasma proteins and endothelial surfaces is inhibited by covalent linkage to antithrombin. Thromb. Haemost. 2004, 91, 1009–1018. [Google Scholar]
- Lovecchio, F. Heparin-induced thrombocytopenia. Clin. Toxicol. 2014, 52, 579–583. [Google Scholar] [CrossRef]
- Patriarcheas, V.; Pikoulas, A.; Kostis, M.; Charpidou, A.; Dimakakos, E. Heparin-induced Thrombocytopenia: Pathophysiology, Diagnosis and Management. Cureus 2020, 12, e7385. [Google Scholar] [CrossRef]
- Warkentin, T.E.; Greinacher, A.; Koster, A.; Lincoff, A.M. Treatment and prevention of heparin-induced thrombocytopenia: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008, 133, 340S–380S. [Google Scholar] [CrossRef]
- Arepally, G.M. Heparin-induced thrombocytopenia. Blood 2017, 129, 2864–2872. [Google Scholar] [CrossRef]
- Junqueira, D.R.; Perini, E.; Penholati, R.R.; Carvalho, M.G. Unfractionated heparin versus low molecular weight heparin for avoiding heparin-induced thrombocytopenia in postoperative patients. Cochrane Database Syst. Rev. 2012, 9, CD007557. [Google Scholar]
- Prandoni, P.; Siragusa, S.; Girolami, B.; Fabris, F. BELZONI Investigators Group. The incidence of heparin-induced thrombocytopenia in medical patients treated with low-molecular-weight heparin: A prospective cohort study. Blood 2005, 106, 3049–3054. [Google Scholar] [CrossRef]
- Leentjens, J.; Peters, M.; Esselink, A.C.; Smulders, Y.; Kramers, C. Initial anticoagulation in patients with pulmonary embolism: Thrombolysis, unfractionated heparin, LMWH, fondaparinux, or DOACs? Br. J. Clin. Pharmacol. 2017, 83, 2356–2366. [Google Scholar] [CrossRef]
- Costantino, G.; Ceriani, E.; Rusconi, A.M.; Podda, G.M.; Montano, N.; Duca, P.; Cattaneo, M.; Casazza, G. Bleeding risk during treatment of acute thrombotic events with subcutaneous LMWH compared to intravenous unfractionated heparin; a systematic review. PLoS ONE 2012, 7, e44553. [Google Scholar] [CrossRef]
- Van Rein, N.; Biedermann, J.S.; van der Meer, F.J.M.; Cannegieter, S.C.; Wiersma, N.; Vermaas, H.W.; Reitsma, P.H.; Kruip, M.J.H.A.; Lijfering, W.M. Major bleeding risks of different low-molecular-weight heparin agents: A cohort study in 12,934 patients treated for acute venous thrombosis. J. Thromb. Haemost. 2017, 15, 1386–1391. [Google Scholar] [CrossRef]
- Glauser, B.F.; Santos, G.R.C.; Silva, J.D.; Tovar, A.M.F.; Pereira, M.S.; Vilanova, E.; Mourão, P.A.S. Chemical and pharmacological aspects of neutralization of heparins from different animal sources by protamine. J. Thromb. Haemost. 2018, 16, 1789–1799. [Google Scholar] [CrossRef]
- Schroeder, M.; Hogwood, J.; Gray, E.; Mulloy, B.; Hackett, A.M.; Johansen, K.B. Protamine neutralisation of low molecular weight heparins and their oligosaccharide components. Anal. Bioanal. Chem. 2011, 399, 763–771. [Google Scholar] [CrossRef]
- Hogwood, J.; Mulloy, B.; Gray, E. Precipitation and Neutralization of Heparin from Different Sources by Protamine Sulfate. Pharmaceuticals 2017, 10, 59. [Google Scholar] [CrossRef]
- Saheb Sharif-Askari, F.; Syed Sulaiman, S.A.; Saheb Sharif-Askari, N. Anticoagulation Therapy in Patients with Chronic Kidney Disease. Adv. Exp. Med. Biol. 2017, 906, 101–114. [Google Scholar]
- Warkentin, T.E. Fondaparinux: Does it cause HIT? Can it treat HIT? Expert Rev. Hematol. 2010, 3, 567–581. [Google Scholar] [CrossRef]
- Linkins, L.A.; Hu, G.; Warkentin, T.E. Systematic review of fondaparinux for heparin-induced thrombocytopenia: When there are no randomized controlled trials. Res. Pract. Thromb. Haemost. 2018, 2, 678–683. [Google Scholar] [CrossRef]
- Cumbo-Nacheli, G.; Samavati, L.; Guzman, J.A. Bioavailability of fondaparinux to critically ill patients. J. Crit Care 2011, 26, 342–346. [Google Scholar] [CrossRef]
- Bijsterveld, N.R.; Moons, A.H.; Boekholdt, S.M.; van Aken, B.E.; Fennema, H.; Peters, R.J.; Meijers, J.C.; Büller, H.R.; Levi, M. Ability of recombinant factor VIIa to reverse the anticoagulant effect of the pentasaccharide fondaparinux in healthy volunteers. Circulation 2002, 106, 2550–2554. [Google Scholar] [CrossRef]
- Greinacher, A.; Völpel, H.; Janssens, U.; Hach-Wunderle, V.; Kemkes-Matthes, B.; Eichler, P.; Mueller-Velten, H.G.; for the HIT Investigators Group. Recombinant hirudin (lepirudin) provides safe and effective anticoagulation in patients with heparin-induced thrombocytopenia: A prospective study. Circulation 1999, 99, 73–80. [Google Scholar] [CrossRef]
- Greinacher, A.; Janssens, U.; Berg, G.; Böck, M.; Kwasny, H.; Kemkes-Matthes, B.; Eichler, P.; Völpel, H.; Pötzsch, B.; Luz, M.; et al. Lepirudin (recombinant hirudin) for parenteral anticoagulation in patients with heparin-induced thrombocytopenia. Circulation 1999, 100, 587–593. [Google Scholar] [CrossRef]
- Lubenow, N.; Eichler, P.; Lietz, T.; Greinacher, A.; Hit Investigators Group. Lepirudin in patients with heparin-induced thrombocytopenia—Results of the third prospective study (HAT-3) and a combined analysis of HAT-1, HAT-2, and HAT-3. J. Thromb. Haemost. 2005, 3, 2428–2436. [Google Scholar] [CrossRef]
- Dager, W.E.; White, R.H. Use of lepirudin in patients with heparin-induced thrombocytopenia and renal failure requiring hemodialysis. Ann. Pharmacother. 2001, 35, 885–890. [Google Scholar] [CrossRef]
- Bambrah, R.K.; Pham, D.C.; Rana, F. Argatroban in heparin-induced thrombocytopenia: Rationale for use and place in therapy. Ther. Adv. Chronic Dis. 2013, 4, 302–304. [Google Scholar] [CrossRef]
- Duewell, B.E.; Briski, M.J.; Feih, J.T.; Rinka, J.R.G.; Tawil, J.N. Argatroban Versus Bivalirudin in the Treatment of Suspected or Confirmed Heparin-Induced Thrombocytopenia. J. Pharm. Pract. 2021, 34, 529–534. [Google Scholar] [CrossRef]
- Cuker, A.; Arepally, G.M.; Chong, B.H.; Cines, D.B.; Greinacher, A.; Gruel, Y.; Linkins, L.A.; Rodner, S.B.; Selleng, S. American Society of Hematology 2018 guidelines for management of venous thromboembolism: Heparin-induced thrombocytopenia. Blood Adv. 2018, 2, 3360–3392. [Google Scholar] [CrossRef]
- Farasatinasab, M.; Zarei, B.; Moghtadaei, M.; Nasiripour, S.; Ansarinejad, N.; Zarei, M. Rivaroxaban as an Alternative Agent for Heparin-Induced Thrombocytopenia. J. Clin. Pharmacol. 2020, 60, 1362–1366. [Google Scholar] [CrossRef]
- Leidi, A.; Bex, S.; Righini, M.; Berner, A.; Grosgurin, O.; Marti, C. Risk Stratification in Patients with Acute Pulmonary Embolism: Current Evidence and Perspectives. J. Clin. Med. 2022, 11, 2533. [Google Scholar] [CrossRef]
- Ucar, E.Y. Update on Thrombolytic Therapy in Acute Pulmonary Thromboembolism. Eurasian J. Med. 2019, 51, 186–190. [Google Scholar] [PubMed]
- Chatterjee, S.; Chakraborty, A.; Weinberg, I.; Kadakia, M.; Wilensky, R.L.; Sardar, P.; Kumbhani, D.J.; Mukherjee, D.; Jaff, M.R.; Giri, J. Thrombolysis for pulmonary embolism and risk of all-cause mortality, major bleeding, and intracranial hemorrhage: A meta-analysis. JAMA 2014, 311, 2414–2421. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.; Itagaki, S.; Chiang, Y.P.; Egorova, N.N.; Adams, D.H.; Chikwe, J. Survival and recurrence after acute pulmonary embolism treated with pulmonary embolectomy or thrombolysis in New York State, 1999 to 2013. J. Thorac. Cardiovasc. Surg. 2018, 155, 1084–1090.e12. [Google Scholar] [CrossRef] [PubMed]
- Stein, P.D.; Alnas, M.; Beemath, A.; Patel, N.R. Outcome of pulmonary embolectomy. Am. J. Cardiol. 2007, 99, 421–423. [Google Scholar] [CrossRef]
- QiMin, W.; LiangWan, C.; DaoZhong, C.; HanFan, Q.; ZhongYao, H.; XiaoFu, D.; XueShan, H.; Feng, L.; HuaBin, C. Clinical outcomes of acute pulmonary embolectomy as the first-line treatment for massive and submassive pulmonary embolism: A single-centre study in China. J. Cardiothorac. Surg. 2020, 15, 321. [Google Scholar] [CrossRef]
- Martinez Licha, C.R.; McCurdy, C.M.; Maldonado, S.M.; Lee, L.S. Current Management of Acute Pulmonary Embolism. Ann. Thorac. Cardiovasc. Surg. 2020, 26, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Cui, M.; Zhang, K.; Liang, K.; Liu, H.; Zhai, S. Treatment of acute pulmonary embolism using rheolytic thrombectomy. EuroIntervention 2021, 17, e158–e166. [Google Scholar] [CrossRef]
- Sharifi, M.; Bay, C.; Skrocki, L.; Rahimi, F.; Mehdipour, M. “MOPETT” Investigators. Moderate pulmonary embolism treated with thrombolysis (from the “MOPETT” Trial). Am. J. Cardiol. 2013, 111, 273–277. [Google Scholar] [CrossRef]
- Konstantinides, S.; Geibel, A.; Heusel, G.; Heinrich, F.; Kasper, W. Management Strategies and Prognosis of Pulmonary Embolism-3 Trial Investigators. Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. N. Engl. J. Med. 2002, 347, 1143–1150. [Google Scholar] [CrossRef]
- Meyer, G.; Vicaut, E.; Danays, T.; Agnelli, G.; Becattini, C.; Beyer-Westendorf, J.; Bluhmki, E.; Bouvaist, H.; Brenner, B.; Couturaud, F.; et al. PEITHO Investigators. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N. Engl. J. Med. 2014, 370, 1402–1411. [Google Scholar] [CrossRef]
- Nakamura, S.; Takano, H.; Kubota, Y.; Asai, K.; Shimizu, W. Impact of the efficacy of thrombolytic therapy on the mortality of patients with acute submassive pulmonary embolism: A meta-analysis. J. Thromb. Haemost. 2014, 12, 1086–1095. [Google Scholar] [CrossRef]
- Bova, C.; Sanchez, O.; Prandoni, P.; Lankeit, M.; Konstantinides, S.; Vanni, S.; Jiménez, D. Identification of intermediate-risk patients with acute symptomatic pulmonary embolism. Eur. Respir. J. 2014, 44, 694–703. [Google Scholar] [CrossRef]
- Stevens, S.M.; Woller, S.C.; Kreuziger, L.B.; Bounameaux, H.; Doerschug, K.; Geersing, G.J.; Huisman, M.V.; Kearon, C.; King, C.S.; Knighton, A.J.; et al. Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report. Chest 2021, 160, e545–e608. [Google Scholar] [CrossRef]
- Wang, C.; Zhai, Z.; Yang, Y.; Wu, Q.; Cheng, Z.; Liang, L.; Dai, H.; Huang, K.; Lu, W.; Zhang, Z.; et al. China Venous Thromboembolism (VTE) Study Group. Efficacy and safety of low dose recombinant tissue-type plasminogen activator for the treatment of acute pulmonary thromboembolism: A randomized, multicenter, controlled trial. Chest 2010, 137, 254–262. [Google Scholar] [CrossRef]
- Alexander, P.; Visagan, S.; Issa, R.; Gorantla, V.R. Thomas SE. Current Trends in the Duration of Anticoagulant Therapy for Venous Thromboembolism: A Systematic Review. Cureus 2021, 13, e18992. [Google Scholar]
- Chopard, R.; Albertsen, I.E.; Ecarnot, F.; Guth, S.; Besutti, M.; Falvo, N.; Piazza, G.; Meneveau, N. Extended Anticoagulation After Pulmonary Embolism: A Multicenter Observational Cohort Analysis. J. Am. Heart Assoc. 2022, 11, e024425. [Google Scholar] [CrossRef]
- Ghembaza, A.; Saadoun, D. Management of Antiphospholipid Syndrome. Biomedicines 2020, 8, 508. [Google Scholar] [CrossRef]
- Weitz, J.I.; Lensing, A.W.A.; Prins, M.H.; Bauersachs, R.; Beyer-Westendorf, J.; Bounameaux, H.; Brighton, T.A.; Cohen, A.T.; Davidson, B.L.; Decousus, H.; et al. EINSTEIN CHOICE Investigators. Rivaroxaban or Aspirin for Extended Treatment of Venous Thromboembolism. N. Engl. J. Med. 2017, 376, 1211–1222. [Google Scholar] [CrossRef]
- Tritschler, T.; Méan, M.; Limacher, A.; Rodondi, N.; Aujesky, D. Predicting recurrence after unprovoked venous thromboembolism: Prospective validation of the updated Vienna Prediction Model. Blood 2015, 126, 1949–1951. [Google Scholar] [CrossRef]
- Rodger, M.A.; Le Gal, G.; Langlois, N.J.; Gin, B.; Mallick, R.; Giulivi, A.; Freedman, M.; Kovacs, M.J.; REVERSE II investigators. “HERDOO2” clinical decision rule to guide duration of anticoagulation in women with unprovoked venous thromboembolism. Can I use any d-Dimer? Thromb. Res. 2018, 169, 82–86. [Google Scholar] [CrossRef]
- Wang, Y.; Bajorek, B. New oral anticoagulants in practice: Pharmacological and practical considerations. Am. J. Cardiovasc. Drugs 2014, 14, 175–189. [Google Scholar] [CrossRef] [PubMed]
- Di Minno, A.; Frigerio, B.; Spadarella, G.; Ravani, A.; Sansaro, D.; Amato, M.; Kitzmiller, J.P.; Pepi, M.; Tremoli, E.; Baldassarre, D. Old and new oral anticoagulants: Food, herbal medicines and drug interactions. Blood Rev. 2017, 31, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Chen, Y.; Zhu, H.; Huang, W.H.; Cai, X.H.; Li, D.; Lv, Y.J.; Si-Zhao; Zhou, H.H.; Luo, F.-Y.; et al. The Relationship Among Intestinal Bacteria, Vitamin K and Response of Vitamin K Antagonist: A Review of Evidence and Potential Mechanism. Front. Med. 2022, 9, 829304. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Chan, N.C. Bleeding in patients with atrial fibrillation treated with combined antiplatelet and anticoagulant therapy: Time to turn the corner. Ann. Transl. Med. 2019, 7, S198. [Google Scholar] [CrossRef]
- Schalekamp, T.; Klungel, O.H.; Souverein, P.C.; de Boer, A. Increased bleeding risk with concurrent use of selective serotonin reuptake inhibitors and coumarins. Arch. Intern. Med. 2008, 168, 180–185. [Google Scholar] [CrossRef]
- Sostres, C.; Gargallo, C.J.; Lanas, A. Nonsteroidal anti-inflammatory drugs and upper and lower gastrointestinal mucosal damage. Arthritis Res. Ther. 2013, 15, S3. [Google Scholar] [CrossRef]
- Wang, M.; Zeraatkar, D.; Obeda, M.; Lee, M.; Garcia, C.; Nguyen, L.; Agarwal, A.; Al-Shalabi, F.; Benipal, H.; Ahmad, A. Drug-drug interactions with warfarin: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 2021, 87, 4051–4100. [Google Scholar] [CrossRef]
- Westergren, T.; Johansson, P.; Molden, E. Probable warfarin-simvastatin interaction. Ann. Pharmacother. 2007, 41, 1292–1295. [Google Scholar] [CrossRef]
- Andrus, M.R. Oral anticoagulant drug interactions with statins: Case report of fluvastatin and review of the literature. Pharmacotherapy 2004, 24, 285–290. [Google Scholar] [CrossRef]
- Engell, A.E.; Svendsen, A.L.O.; Lind, B.S.; Andersen, C.L.; Andersen, J.S.; Willadsen, T.G.; Persson, F.; Pottegård, A. Drug-drug interaction between warfarin and statins: A Danish cohort study. Br. J. Clin. Pharmacol. 2021, 87, 694–699. [Google Scholar] [CrossRef]
- Fan, Y.; Adam, T.J.; McEwan, R.; Pakhomov, S.V.; Melton, G.B.; Zhang, R. Detecting Signals of Interactions Between Warfarin and Dietary Supplements in Electronic Health Records. Stud. Health Technol. Inform. 2017, 245, 370–374. [Google Scholar]
- Brandin, H.; Myrberg, O.; Rundlöf, T.; Arvidsson, A.K.; Brenning, G. Adverse effects by artificial grapefruit seed extract products in patients on warfarin therapy. Eur. J. Clin. Pharmacol. 2007, 63, 565–570. [Google Scholar] [CrossRef]
- Monterrey-Rodríguez, J. Interaction between warfarin and mango fruit. Ann. Pharmacother. 2002, 36, 940–941. [Google Scholar] [CrossRef]
- Ulbricht, C.; Chao, W.; Costa, D.; Rusie-Seamon, E.; Weissner, W.; Woods, J. Clinical evidence of herb-drug interactions: A systematic review by the natural standard research collaboration. Curr. Drug Metab. 2008, 9, 1063–1120. [Google Scholar] [CrossRef]
- Hamann, G.L.; Campbell, J.D.; George, C.M. Warfarin-cranberry juice interaction. Ann. Pharmacother. 2011, 45, e17. [Google Scholar] [CrossRef]
- Jiang, X.; Williams, K.M.; Liauw, W.S.; Ammit, A.J.; Roufogalis, B.D.; Duke, C.C.; Day, R.O.; McLachlan, A.J. Effect of St John’s wort and ginseng on the pharmacokinetics and pharmacodynamics of warfarin in healthy subjects. Br. J. Clin. Pharmacol. 2004, 57, 592–599. [Google Scholar] [CrossRef]
- Taylor, J.R.; Wilt, V.M. Probable antagonism of warfarin by green tea. Ann. Pharmacother. 1999, 33, 426–428. [Google Scholar] [CrossRef]
- Shikdar, S.; Vashisht, R.; Bhattacharya, P.T. International Normalized Ratio (INR) [Updated 8 May 2022]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK507707/ (accessed on 8 May 2022).
- Bauer, K.A. Pros and cons of new oral anticoagulants. Hematol. Am. Soc. Hematol. Educ. Program 2013, 2013, 464–470. [Google Scholar] [CrossRef] [Green Version]
- Cohen, A.T.; Sah, J.; Dhamane, A.D.; Lee, T.; Rosenblatt, L.; Hlavacek, P.; Emir, B.; Keshishian, A.; Yuce, H.; Luo, X. Effectiveness and Safety of Apixaban Versus Warfarin Among Older Patients with Venous Thromboembolism with Different Demographics and Socioeconomic Status. Adv. Ther. 2021, 38, 5519–5533. [Google Scholar] [CrossRef]
- Coleman, C.I.; Bunz, T.J.; Turpie, A.G.G. Effectiveness and safety of rivaroxaban versus warfarin for treatment and prevention of recurrence of venous thromboembolism. Thromb. Haemost. 2017, 117, 1841–1847. [Google Scholar]
- Alhousani, M.; Malik, S.U.; Abu-Hashyeh, A.; Poznanski, N.J.; Al-Hasan, S.; Roth, D.F.; Alsharedi, M.; Mustafa, B. Using oral anticoagulants among chronic kidney disease patients to prevent recurrent venous thromboembolism: A systematic review and meta-analysis. Thromb. Res. 2021, 198, 103–114. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, D.; Raghavan, N.; Yao, M.; Ma, L.; Frost, C.E.; Maxwell, B.D.; Chen, S.Y.; He, K.; Goosen, T.C.; et al. In vitro assessment of metabolic drug-drug interaction potential of apixaban through cytochrome P450 phenotyping, inhibition, and induction studies. Drug Metab. Dispos. 2010, 38, 448–458. [Google Scholar] [CrossRef]
- Panahi, L.; Udeani, G.; Horseman, M.; Weston, J.; Samuel, N.; Joseph, M.; Mora, A.; Bazan, D. Review of Medical Therapies for the Management of Pulmonary Embolism. Medicina 2021, 57, 110. [Google Scholar] [CrossRef]
- Mueck, W.; Stampfuss, J.; Kubitza, D.; Becka, M. Clinical pharmacokinetic and pharmacodynamic profile of rivaroxaban. Clin. Pharmacokinet. 2014, 53, 1–16. [Google Scholar] [CrossRef]
- Mueck, W.; Kubitza, D.; Becka, M. Co-administration of rivaroxaban with drugs that share its elimination pathways: Pharmacokinetic effects in healthy subjects. Br. J. Clin. Pharmacol. 2013, 76, 455–466. [Google Scholar]
- Reilly, P.A.; Lehr, T.; Haertter, S.; Connolly, S.J.; Yusuf, S.; Eikelboom, J.W.; Ezekowitz, M.D.; Nehmiz, G.; Wang, S.; Wallentin, L. RE-LY Investigators. The effect of dabigatran plasma concentrations and patient characteristics on the frequency of ischemic stroke and major bleeding in atrial fibrillation patients: The RE-LY Trial (Randomized Evaluation of Long-Term Anticoagulation Therapy). J. Am. Coll. Cardiol. 2014, 63, 321–328. [Google Scholar]
- Eikelboom, J.W.; Connolly, S.J.; Brueckmann, M.; Granger, C.B.; Kappetein, A.P.; Mack, M.J.; Blatchford, J.; Devenny, K.; Friedman, J.; Guiver, K.; et al. RE-ALIGN Investigators. Dabigatran versus warfarin in patients with mechanical heart valves. N. Engl. J. Med. 2013, 369, 1206–1214. [Google Scholar] [CrossRef]
- Eriksson, B.I.; Quinlan, D.J.; Weitz, J.I. Comparative pharmacodynamics and pharmacokinetics of oral direct thrombin and factor xa inhibitors in development. Clin. Pharmacokinetic. 2009, 48, 1. [Google Scholar] [CrossRef]
- Walenga, J.M.; Adiguzel, C. Drug and dietary interactions of the new and emerging oral anticoagulants. Int. J. Clin. Pract. 2010, 64, 956–967. [Google Scholar] [CrossRef]
- Grześk, G.; Rogowicz, D.; Wołowiec, Ł.; Ratajczak, A.; Gilewski, W.; Chudzińska, M.; Sinkiewicz, A.; Banach, J. The Clinical Significance of Drug–Food Interactions of Direct Oral Anticoagulants. Int. J. Mol. Sci. 2021, 22, 8531. [Google Scholar] [CrossRef]
- Chang, D.N.; Dager, W.E.; Chin, A.I. Removal of dabigatran by hemodialysis. Am. J. Kidney Dis. 2013, 61, 487–489. [Google Scholar] [CrossRef] [PubMed]
- Hokusai-VTE Investigators. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N. Engl. J. Med. 2013, 369, 1406–1415. [Google Scholar] [PubMed]
- Stangier, J.; Rathgen, K.; Stähle, H.; Gansser, D.; Roth, W. The pharmacokinetics, pharmacodynamics and tolerability of dabigatran etexilate, a new oral direct thrombin inhibitor, in healthy male subjects. Br. J. Clin. Pharmacol. 2007, 64, 292–303. [Google Scholar] [CrossRef] [PubMed]
- Bounameaux, H.; Camm, A.J. Edoxaban: An Update on the New Oral Direct Factor Xa Inhibitor. Drugs 2014, 74, 1209–1231. [Google Scholar] [CrossRef]
- Mendell, J.; Zahir, H.; Matsushima, N.; Noveck, R.; Lee, F.; Chen, S.; Zhang, G.; Shi, M. Drug-drug interaction studies of cardiovascular drugs involving P-glycoprotein, an efflux transporter, on the pharmacokinetics of edoxaban, an oral factor Xa inhibitor. Am. J. Cardiovasc. Drugs 2013, 13, 331–342. [Google Scholar] [CrossRef]
- Mainbourg, S.; Cucherat, M.; Provencher, S.; Bertoletti, L.; Nony, P.; Gueyffier, F.; Mismetti, P.; Grange, C.; Durieu, I.; Kilo, R.; et al. META-EMBOL group. Twice- or Once-Daily Dosing of Direct Oral Anticoagulants, a systematic review and meta-analysis. Thromb. Res. 2021, 197, 24–32. [Google Scholar]
- Puy, C.; Rigg, R.A.; McCarty, O.J. The hemostatic role of factor XI. Thromb. Res. 2016, 141, S8–S11. [Google Scholar] [CrossRef]
- Piccini, J.P.; Caso, V.; Connolly, S.J.; Fox, K.A.A.; Oldgren, J.; Jones, W.S.; Gorog, D.A.; Durdil, V.; Viethen, T.; Neumann, C. PACIFIC-AF Investigators. Safety of the oral factor XIa inhibitor asundexian compared with apixaban in patients with atrial fibrillation (PACIFIC-AF): A multicentre, randomised, double-blind, double-dummy, dose-finding phase 2 study. Lancet 2022, 399, 1383–1390. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Douketis, J.D. How I treat anticoagulated patients undergoing an elective procedure or surgery. Blood 2012, 120, 2954–2962. [Google Scholar] [CrossRef]
- Steffel, J.; Collins, R.; Antz, M.; Cornu, P.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; Rowell, N.; et al. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Europace 2021, 23, 1612–1676. [Google Scholar] [CrossRef]
- Hornor, M.A.; Duane, T.M.; Ehlers, A.P.; Jensen, E.H.; Brown, P.S.; Pohl, D., Jr.; da Costa, P.M.; Ko, C.Y.; Laronga, C. American College of Surgeons’ Guidelines for the Perioperative Management of Antithrombotic Medication. J. Am. Coll. Surg. 2018, 227, 521–536.e1. [Google Scholar] [CrossRef]
- Doherty, J.U.; Gluckman, T.J.; Hucker, W.J.; Januzzi, J.L.; Ortel, T.L., Jr.; Saxonhouse, S.J.; Spinler, S.A. 2017 ACC Expert Consensus Decision Pathway for Periprocedural Management of Anticoagulation in Patients With Nonvalvular Atrial Fibrillation: A Report of the American College of Cardiology Clinical Expert Consensus Document Task Force. J. Am. Coll. Cardiol. 2017, 69, 871–898. [Google Scholar] [CrossRef]
- Rutz, T.; Eggel-Hort, B.; Alberio, L.; Bouchardy, J. Anticoagulation of women with congenital heart disease during pregnancy. Int. J. Cardiol. Congenit. Heart Dis. 2021, 5, 100210. [Google Scholar] [CrossRef]
- Lameijer, H.; Aalberts, J.J.J.; van Veldhuisen, D.J.; Meijer, K.; Pieper, P.G. Efficacy and safety of direct oral anticoagulants during pregnancy; a systematic literature review. Thromb. Res. 2018, 169, 123–127. [Google Scholar] [CrossRef]
- Pengo, V.; Denas, G.; Zoppellaro, G.; Jose, S.P.; Hoxha, A.; Ruffatti, A.; Andreoli, L.; Tincani, A.; Cenci, C.; Prisco, D.; et al. Rivaroxaban vs warfarin in high-risk patients with antiphospholipid syndrome. Blood 2018, 132, 1365–1371. [Google Scholar] [CrossRef]
- Pengo, V.; Hoxha, A.; Andreoli, L.; Tincani, A.; Silvestri, E.; Prisco, D.; Fierro, T.; Gresele, P.; Cafolla, A.; De Micheli, V.; et al. Trial of Rivaroxaban in AntiPhospholipid Syndrome (TRAPS): Two-year outcomes after the study closure. J. Thromb. Haemost. 2021, 19, 531–535. [Google Scholar] [CrossRef]
- Camilli, M.; Lombardi, M.; Vescovo, G.M.; Del Buono, M.G.; Galli, M.; Aspromonte, N.; Zoccai, G.B.; Niccoli, G.; Montone, R.A.; Crea, F.; et al. Efficacy and safety of novel oral anticoagulants versus low molecular weight heparin in cancer patients with venous thromboembolism: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2020, 154, 103074. [Google Scholar]
- Raskob, G.E.; van Es, N.; Verhamme, P.; Carrier, M.; Di Nisio, M.; Garcia, D.; Grosso, M.A.; Kakkar, A.K.; Kovacs, M.J.; Mercuri, M.F.; et al. Hokusai VTE Cancer Investigators. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism. N. Engl. J. Med. 2018, 378, 615–624. [Google Scholar] [CrossRef]
- Clemens, A.; Strack, A.; Noack, H.; Konstantinides, S.; Brueckmann, M.; Lip, G.Y. Anticoagulant-related gastrointestinal bleeding—could this facilitate early detection of benign or malignant gastrointestinal lesions? Ann. Med. 2014, 46, 672–678. [Google Scholar] [CrossRef]
- Tsoukalas, N.; Brito-Dellan, N.; Font, C.; Butler, T.; Rojas-Hernandez, C.M.; Butler, T.; Escalante, C.; MASCC Hemostasis Study Group. Complexity and clinical significance of drug-drug interactions (DDIs) in oncology: Challenging issues in the care of patients regarding cancer-associated thrombosis (CAT). Support. Care Cancer, 2022; ahead-of-print. [Google Scholar] [CrossRef]
- Wang, T.F.; Baumann Kreuziger, L.; Leader, A.; Spectre, G.; Lim, M.Y.; Gahagan, A.; Gangaraju, R.; Sanfilippo, K.M.; Mallick, R.; Zwicker, J.I. Characteristics and outcomes of patients on concurrent direct oral anticoagulants and targeted anticancer therapies-TacDOAC registry: Communication from the ISTH SSC Subcommittee on Hemostasis and Malignancy. J. Thromb. Haemost. 2021, 19, 2068–2081. [Google Scholar] [CrossRef]
- Ferri, N.; Colombo, E.; Tenconi, M.; Baldessin, L.; Corsini, A. Drug-Drug Interactions of Direct Oral Anticoagulants (DOACs): From Pharmacological to Clinical Practice. Pharmaceutics 2022, 14, 1120. [Google Scholar] [CrossRef]
- Young, A.M.; Marshall, A.; Thirlwall, J.; Chapman, O.; Lokare, A.; Hill, C.; Hale, D.; Dunn, J.A.; Lyman, G.H.; Hutchinson, C.; et al. Comparison of an Oral Factor Xa Inhibitor With Low Molecular Weight Heparin in Patients With Cancer With Venous Thromboembolism: Results of a Randomized Trial (SELECT-D). J. Clin. Oncol. 2018, 36, 2017–2023. [Google Scholar] [CrossRef]
- Mokadem, M.E.; Hassan, A.; Algaby, A.Z. Efficacy and safety of apixaban in patients with active malignancy and acute deep venous thrombosis. Vascular 2021, 29, 745–750. [Google Scholar] [CrossRef]
- McBane, R.D.; Wysokinski, W.E.; Le-Rademacher, J.G.; Zemla, T.; Ashrani, A.; Tafur, A.; Perepu, U.; Anderson, D.; Gundabolu, K.; Kuzma, C.; et al. Apixaban and dalteparin in active malignancy-associated venous thromboembolism: The ADAM VTE trial. J. Thromb. Haemost. 2020, 18, 411–421. [Google Scholar] [CrossRef]
- Peixoto de Miranda, É.J.F.; Takahashi, T.; Iwamoto, F.; Yamashiro, S.; Samano, E.; Macedo, A.V.S.; Ramacciotti, E. Drug-Drug Interactions of 257 Antineoplastic and Supportive Care Agents With 7 Anticoagulants: A Comprehensive Review of Interactions and Mechanisms. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620936325. [Google Scholar] [CrossRef]
- Bauersachs, R.M.; Herold, J. Oral Anticoagulation in the Elderly and Frail. Hamostaseologie 2020, 40, 74–83. [Google Scholar] [CrossRef]
- Proietti, M.; Camera, M.; Gallieni, M.; Gianturco, L.; Gidaro, A.; Piemontese, C.; Pizzetti, G.; Redaelli, F.; Scimeca, B.; Tadeo, C.S.; et al. Use and Prescription of Direct Oral Anticoagulants in Older and Frail Patients with Atrial Fibrillation: A Multidisciplinary Consensus Document. J. Pers. Med. 2022, 12, 469. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Wu, H.; Wang, C.; Lou, B.; She, J. Impact of Age, Sex, and Renal Function on the Efficacy and Safety of Direct Oral Anticoagulants vs. Vitamin K Antagonists for the Treatment of Acute Venous Thromboembolism: A Meta-Analysis of 22,040 Patients. Front. Cardiovasc. Med. 2021, 8, 700740. [Google Scholar] [CrossRef] [PubMed]
- .Deng, K.; Cheng, J.; Rao, S.; Xu, H.; Li, L.; Gao, Y. Efficacy and Safety of Direct Oral Anticoagulants in Elderly Patients With Atrial Fibrillation: A Network Meta-Analysis. Front. Med. 2020, 7, 107. [Google Scholar] [CrossRef] [PubMed]
- Ayalon-Dangur, I.; Vega, Y.; Israel, M.R.; Grossman, A.; Spectre, G.; Shochat, T.; Leibovici, L.; Gafter-Gvili, A. Outcome of Elderly Patients with Venous Thromboembolism Treated with Direct Oral Anticoagulants-A Retrospective Cohort Study. J. Clin. Med. 2021, 10, 5673. [Google Scholar] [CrossRef]
- Geldhof, V.; Vandenbriele, C.; Verhamme, P.; Vanassche, T. Venous thromboembolism in the elderly: Efficacy and safety of non-VKA oral anticoagulants. Thromb. J. 2014, 12, 21. [Google Scholar] [CrossRef]
- Su, X.; Yan, B.; Wang, L.; Cheng, H.; Chen, Y. Comparative efficacy and safety of oral anticoagulants for the treatment of venous thromboembolism in the patients with different renal functions: A systematic review, pairwise and network meta-analysis. BMJ Open 2022, 12, e048619. [Google Scholar] [CrossRef]
- Chan, K.E.; Edelman, E.R.; Wenger, J.B.; Thadhani, R.I.; Maddux, F.W. Dabigatran and rivaroxaban use in atrial fibrillation patients on hemodialysis. Circulation 2015, 131, 972–979. [Google Scholar]
- Martin, K.A.; Beyer-Westendorf, J.; Davidson, B.L.; Huisman, M.V.; Sandset, P.M.; Moll, S. Use of direct oral anticoagulants in patients with obesity for treatment and prevention of venous thromboembolism: Updated communication from the ISTH SSC Subcommittee on Control of Anticoagulation. J. Thromb. Haemost. 2021, 19, 1874–1882. [Google Scholar] [CrossRef]
- Elshafei, M.N.; Mohamed, M.F.H.; El-Bardissy, A.; Ahmed, M.B.; Abdallah, I.; Elewa, H.; Danjuma, M. Comparative effectiveness and safety of direct oral anticoagulants compared to warfarin in morbidly obese patients with acute venous thromboembolism: Systematic review and a meta-analysis. J. Thromb. Thrombolysis 2021, 51, 388–396. [Google Scholar] [CrossRef]
- Di Nisio, M.; Vedovati, M.C.; Riera-Mestre, A.; Prins, M.H.; Mueller, K.; Cohen, A.T.; Wells, P.S.; Beyer-Westendorf, J.; Prandoni, P.; Bounameaux, H.; et al. Treatment of venous thromboembolism with rivaroxaban in relation to body weight. A sub-analysis of the EINSTEIN DVT/PE studies. Thromb. Haemost. 2016, 116, 739–746. [Google Scholar]
- Sabourin, A.A.; Patel, T.; Saad, S.; Renner, E.; Mouland, E.; Adie, S.; Ha, N.B. Management of anticoagulation in patients with human immunodeficiency virus/acquired immunodeficiency virus. Thromb. Res. 2021, 200, 102–108. [Google Scholar] [CrossRef]
- .Egan, G.; Hughes, C.A.; Ackman, M.L. Drug interactions between antiplatelet or novel oral anticoagulant medications and antiretroviral medications. Ann Pharmacother. 2014, 48, 734–740. [Google Scholar] [CrossRef]
- Mathias, A.A.; German, P.; Murray, B.P.; Wei, L.; Jain, A.; West, S.; Warren, D.; Hui, J.; Kearney, B.P. Pharmacokinetics and Pharmacodynamics of GS-9350: A Novel Pharmacokinetic Enhancer Without Anti-HIV Activity. Clin. Pharmacol. Ther. 2010, 87, 322–329. [Google Scholar] [CrossRef]
- Perram, J.; Joseph, J.; Holloway, C. Novel oral anticoagulants and HIV: Dabigatran use with antiretrovirals. BMJ Case Rep. 2015, 20, bcr2015211651. [Google Scholar] [CrossRef]
- Serrao, A.; Santoro, C.; Foà, R.; Chistolini, A. Use of edoxaban for the treatment of venous thromboembolism in HIV-infected patients. HIV Med. 2020, 21, e7. [Google Scholar] [CrossRef]
- Cattaneo, D.; Formenti, T.; Gidaro, A.; Merlo, A.; Gervasoni, C. Use of Direct Oral Anticoagulants in People Living with HIV: A Single-Center Experience. Semin. Thromb. Hemost. 2020, 46, 999–1001. [Google Scholar] [CrossRef]
- Galgani, A.; Palleria, C.; Iannone, L.F.; De Sarro, G.; Giorgi, F.S.; Maschio, M.; Russo, E. Pharmacokinetic Interactions of Clinical Interest Between Direct Oral Anticoagulants and Antiepileptic Drugs. Front. Neurol. 2018, 9, 1067. [Google Scholar] [CrossRef]
- Giustozzi, M.; Mazzetti, M.; Paciaroni, M.; Agnelli, G.; Becattini, C.; Vedovati, M.C. Concomitant Use of Direct Oral Anticoagulants and Antiepileptic Drugs: A Prospective Cohort Study in Patients with Atrial Fibrillation. Clin. Drug Investig. 2021, 41, 43–51. [Google Scholar] [CrossRef]
- Acton, E.K.; Gelfand, M.A.; Hennessy, S.; Xie, S.X.; Pollard, J.R.; Kasner, S.E.; Willis, A.W. Trends in oral anticoagulant co-prescription with antiepileptic drugs among adults with epilepsy, 2010–2018. Epilepsy Behav. 2020, 113, 107550. [Google Scholar] [CrossRef]
- Pang, W.; Zhang, Z.; Wang, Z.; Zhen, K.; Zhang, M.; Zhang, Y.; Gao, Q.; Zhang, S.; Tao, X.; Wan, J.; et al. Higher Incidence of Chronic Thromboembolic Pulmonary Hypertension After Acute Pulmonary Embolism in Asians Than in Europeans: A Meta-Analysis. Front. Med. 2021, 8, 721294. [Google Scholar] [CrossRef]
- Matthews, D.T.; Hemnes, A.R. Current concepts in the pathogenesis of chronic thromboembolic pulmonary hypertension. Pulm. Circ. 2016, 6, 145–154. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Drug | Dose | Special Consideration | Specific Patient Characteristics | Reversal Agents |
|---|---|---|---|---|
| UFH | 80 unit/kg IV bolus, followed by an 18-unit/kg/h infusion; | Avoid HIT; Osteopenia Pronounced drag-drag interactions | Overt haemodynamic instability; (CrCl) ≤ 30 mL/min; Pragnancy; Severe obesity | Protamine sulfate |
| LMWH | 1 mg/kg twice daily 1.5 mg/kg once daily | Avoid with severe renal impairment | Pragnancy; Obesity; | Protamine sulfate |
| VKA | Warfarin 5 mg/day once daily 4 mg/day once day-patients > 70 years | Cross the placenta-contraindicated in pregnancy | Antiphospholipid syndrome; Mechanical heart valves; Extremely reduced renal function; Severe mitral stenosis; | 4F-PCC 4 or FFP |
| Apiksaban | 10 mg twice daily for 7 days followed by 5 mg twice daily | Avoid in CrCl < 15 mL/min Severe hepatic impairment | Previous GI bleeding or high risk of bleeding; Patients with CA; Eldery patients; | Andexanet |
| Rivaroxaban | 15 mg- twice daily (3 weeks) then 20 mg once daily (at least 6 months) | Avoid in CrCl < 30 mL/min; (FDA) CrCl < 15 mL/min (EMA). | Low risk of bleeding and without gastrointestinal tumours; Patient preference—a single dose regimen; | Andexanet |
| Dabigatran | 150 mg—twice daily 110 mg—twice daily for patients ≥ 80 years | Avoid in CrCl < 30 mL/min.; Concomitant treatment with P-gp inhibitors in patients with CrCl < 50 mL/min; Reduce dose to 110 mg for patients ≥ 80 years or ≥75 years with at least one bleeding risk factor; | Can be removed by hemodialysis in patients with severe renal impairment; | Idarucizumab |
| Edoxaban | 60 mg—once daily 30 mg—once daily if body weight ≤ 60 kg | Avoid CrCl < 15 mL/min. Severe hepatic dysfunction | Low risk of bleeding and without gastrointestinal tumours | Andexanet |
| Fondaparinux | 5 mg subQ daily <50 kg 7.5 mg subQ daily—50–100 kg 10 mg subQ daily >100 kg | Avoid CrCl < 30 mL/min | HIT (off lable); alergy of LMWH | Factor VIIa |
| Lepirudin | 0.4 mg/kg i.v over 15–20 min, followed by 0.15 mg/kg/h infusion | Avoid Severe renal impairtment | HIT | |
| Argotroban | 2 μg/kg/min Liver dysfunction (bilirubin >1.5 mg/dL) → 0.5–1.2 μg/kg/min | Avoid in severe hepatic dysfunction | HIT | |
| Bivalirudin | 0.15 mg/kg/h | Avoid Severe renal impairtment | HIT (off lable) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lasica, R.; Asanin, M.; Djukanovic, L.; Radovanovic, N.; Savic, L.; Polovina, M.; Stankovic, S.; Ristic, A.; Zdravkovic, M.; Lasica, A.; et al. Dilemmas in the Choice of Adequate Therapeutic Treatment in Patients with Acute Pulmonary Embolism—From Modern Recommendations to Clinical Application. Pharmaceuticals 2022, 15, 1146. https://doi.org/10.3390/ph15091146
Lasica R, Asanin M, Djukanovic L, Radovanovic N, Savic L, Polovina M, Stankovic S, Ristic A, Zdravkovic M, Lasica A, et al. Dilemmas in the Choice of Adequate Therapeutic Treatment in Patients with Acute Pulmonary Embolism—From Modern Recommendations to Clinical Application. Pharmaceuticals. 2022; 15(9):1146. https://doi.org/10.3390/ph15091146
Chicago/Turabian StyleLasica, Ratko, Milika Asanin, Lazar Djukanovic, Nebojsa Radovanovic, Lidija Savic, Marija Polovina, Sanja Stankovic, Arsen Ristic, Marija Zdravkovic, Andjelka Lasica, and et al. 2022. "Dilemmas in the Choice of Adequate Therapeutic Treatment in Patients with Acute Pulmonary Embolism—From Modern Recommendations to Clinical Application" Pharmaceuticals 15, no. 9: 1146. https://doi.org/10.3390/ph15091146