
Difelikefalin in the Treatment of Chronic Kidney Disease-Associated Pruritus: A Systematic Review


Abstract
:1. Introduction
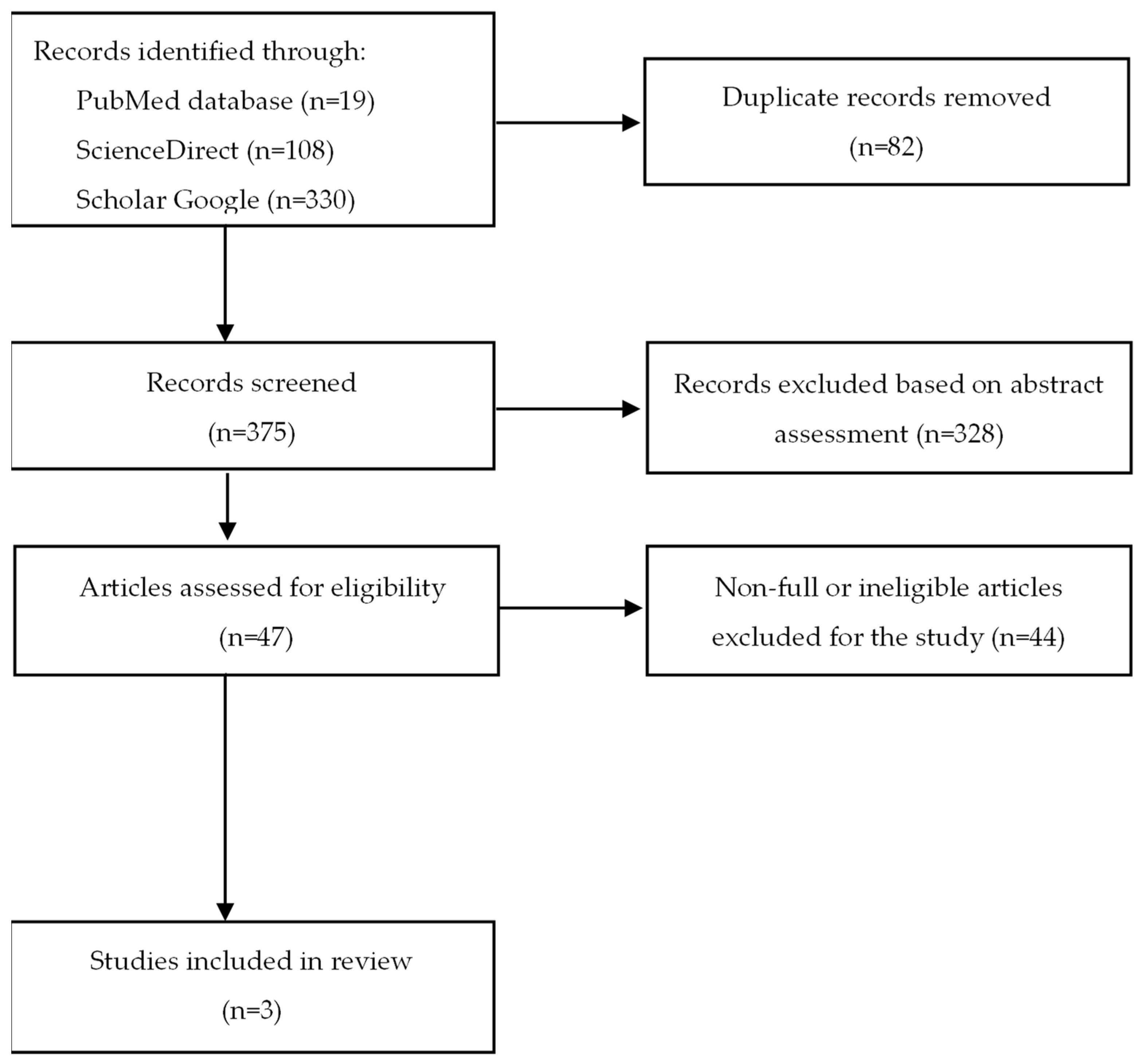
2. Methods
3. Results
3.1. Evaluation of Effectiveness of Difelikefalin
3.1.1. Effect of Difelikefalin on Pruritus Severity
3.1.2. Effect of Difelikefalin on Itch-Related Quality of Life
3.2. Adverse Effects
4. Discussion
Limitation of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Metzger, M.; Abdel-Rahman, E.M.; Boykin, H.; Song, M.-K. A Narrative Review of Management Strategies for Common Symptoms in Advanced CKD. Kidney Int. Rep. 2021, 6, 894–904. [Google Scholar] [CrossRef] [PubMed]
- Nair, D.; Finkelstein, F.O. Pruritus as a Patient-Reported Primary Trial End Point in Hemodialysis: Evaluation and Implications. Am. J. Kidney Dis. 2020, 76, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Makar, M.; Smyth, B.; Brennan, F. Chronic Kidney Disease-Associated Pruritus: A Review. Kidney Blood Press. Res. 2021, 46, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, P.; Garg, V.; Karagaiah, P.; Szepietowski, J.C.; Grabbe, S.; Goldust, M. Chronic Kidney Disease-Associated Pruritus. Toxins 2021, 13, 527. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Pollock, C. Epidemiology and Burden of Chronic Kidney Disease-Associated Pruritus. Clin. Kidney J. 2021, 14, i1–i7. [Google Scholar] [CrossRef] [PubMed]
- Reszke, R.; Szepietowski, J.C. End-Stage Renal Disease Chronic Itch and Its Management. Dermatol. Clin. 2018, 36, 277–292. [Google Scholar] [CrossRef]
- Verduzco, H.A.; Shirazian, S. CKD-Associated Pruritus: New Insights Into Diagnosis, Pathogenesis, and Management. Kidney Int. Rep. 2020, 5, 1387. [Google Scholar] [CrossRef]
- Martin, C.E.; Clotet-Freixas, S.; Farragher, J.F.; Hundemer, G.L. Have We Just Scratched the Surface? A Narrative Review of Uremic Pruritus in 2020. Can. J. Kidney Health Dis. 2020, 7, 2054358120954024. [Google Scholar] [CrossRef]
- Urbonas, A.; Schwartz, R.A.; Szepietowski, J.C. Uremic Pruritus—An Update. Am. J. Nephrol. 2001, 21, 343–350. [Google Scholar] [CrossRef]
- Simonsen, E.; Komenda, P.; Lerner, B.; Askin, N.; Bohm, C.; Shaw, J.; Tangri, N.; Rigatto, C. Treatment of Uremic Pruritus: A Systematic Review. Am. J. Kidney Dis. 2017, 70, 638–655. [Google Scholar] [CrossRef] [Green Version]
- Seckin, D.; Demircay, Z.; Akin, O. Generalized Pruritus Treated with Narrowband UVB. Int. J. Dermatol. 2007, 46, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Gilchrest, B.A. Ultraviolet Phototherapy of Uremic Pruritus. Int. J. Dermatol. 1979, 18, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M.M.L.; Yang, C.C. Uraemic Pruritus Responsive to Broadband Ultraviolet (UV) B Therapy Does Not Readily Respond to Narrowband UVB Therapy. Br. J. Dermatol. 2003, 149, 888–889. [Google Scholar] [CrossRef] [PubMed]
- Ko, M.J.; Yang, J.Y.; Wu, H.Y.; Hu, F.C.; Chen, S.I.; Tsai, P.J.; Jee, S.H.; Chiu, H.C. Narrowband Ultraviolet B Phototherapy for Patients with Refractory Uraemic Pruritus: A Randomized Controlled Trial. Br. J. Dermatol. 2011, 165, 633–639. [Google Scholar] [CrossRef]
- Mettang, T.; Kremer, A.E. Uremic Pruritus. Kidney Int. 2015, 87, 685–691. [Google Scholar] [CrossRef] [Green Version]
- Reich, A.; Szepietowski, J.C. Opioid-Induced Pruritus: An Update. Clin. Exp. Dermatol. 2010, 35, 2–6. [Google Scholar] [CrossRef]
- Wieczorek, A.; Krajewski, P.; Kozioł-Gałczyńska, M.; Szepietowski, J.C. Opioid Receptors Expression in the Skin of Haemodialysis Patients Suffering from Uraemic Pruritus. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2368–2372. [Google Scholar] [CrossRef] [PubMed]
- Terg, R.; Coronel, E.; Sordá, J.; Muñoz, A.E.; Findor, J. Efficacy and Safety of Oral Naltrexone Treatment for Pruritus of Cholestasis, a Crossover, Double Blind, Placebo-Controlled Study. J. Hepatol. 2002, 37, 717–722. [Google Scholar] [CrossRef]
- Wolfhagen, F.H.J.; Sternieri, E.; Hop, W.C.J.; Vitale, G.; Bertolotti, M.; van Buuren, H.R. Oral Naltrexone Treatment for Cholestatic Pruritus: A Double-Blind, Placebo-Controlled Study. Gastroenterology 1997, 113, 1264–1269. [Google Scholar] [CrossRef] [Green Version]
- Bergasa, N.V.; Ailing, D.W.; Talbot, T.L.; Swain, M.G.; Yurdaydin, C.; Turner, M.L.; Schmitt, J.M.; Walker, E.C.; Jones, E.A. Effects of Naloxone Infusions in Patients with the Pruritus of Cholestasis. A Double-Blind, Randomized, Controlled Trial. Ann. Intern. Med. 1995, 123, 161–167. [Google Scholar] [CrossRef]
- Pauli-Magnus, C.; Mikus, G.; Alscher, D.M.; Kirschner, T.; Nagel, W.; Gugeler, N.; Risler, T.; Berger, E.D.; Kuhlmann, U.; Mettang, T. Naltrexone Does Not Relieve Uremic Pruritus: Results of a Randomized, Double-Blind, Placebo-Controlled Crossover Study. J. Am. Soc. Nephrol. 2000, 11, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Phan, N.Q.; Bernhard, J.D.; Luger, T.A.; Ständer, S. Antipruritic Treatment with Systemic μ-Opioid Receptor Antagonists: A Review. J. Am. Soc. Nephrol. 2010, 63, 680–688. [Google Scholar] [CrossRef]
- Antal, A.S.; Bernhard, J.; Ständer, S. Systemic Kappa Opioid Receptor Agonists in the Treatment of Chronic Pruritus: A Literature Review. Acta Derm. Venereol. 2012, 92, 555–560. [Google Scholar] [CrossRef]
- Lazenka, M.L.; Moerke, M.J.; Townsend, E.A.; Freeman, K.B.; Carroll, F.I.; Negus, S.S. Dissociable Effects of the Kappa Opioid Receptor Agonist Nalfurafine on Pain/Itch-Stimulated and Pain/Itch-Depressed Behaviors in Male Rats. Psychopharmacology 2017, 235, 203–213. [Google Scholar] [CrossRef]
- Jain, M.R.; Patel, R.B.; Prajapati, K.D.; Vyas, P.; Bandyopadhyay, D.; Prajapati, V.; Bahekar, R.; Patel, P.N.; Kawade, H.M.; Kokare, D.M.; et al. ZYKR1, a Novel, Potent, and Peripherally Selective Kappa Opioid Receptor Agonist Reduces Visceral Pain and Pruritus in Animal Models. Eur. J. Pharmacol. 2022, 924, 174961. [Google Scholar] [CrossRef]
- Inan, S.; Dun, N.J.; Cowan, A. Antipruritic Effect of Nalbuphine, a Kappa Opioid Receptor Agonist, in Mice: A Pan Antipruritic. Molecules 2021, 26, 5517. [Google Scholar] [CrossRef]
- Togashi, Y.; Umeuchi, H.; Okano, K.; Ando, N.; Yoshizawa, Y.; Honda, T.; Kawamura, K.; Endoh, T.; Utsumi, J.; Kamei, J.; et al. Antipruritic Activity of the κ-Opioid Receptor Agonist, TRK-820. Eur. J. Pharmacol. 2002, 435, 259–264. [Google Scholar] [CrossRef]
- Nakao, K.; Hirakata, M.; Miyamoto, Y.; Kainoh, M.; Wakasa, Y.; Yanagita, T. Nalfurafine Hydrochloride, a Selective κ Opioid Receptor Agonist, Has No Reinforcing Effect on Intravenous Self-Administration in Rhesus Monkeys. J. Pharmacol. Sci. 2016, 130, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Ueno, Y.; Mori, A.; Yanagita, T. One Year Long-Term Study on Abuse Liability of Nalfurafine in Hemodialysis Patients. Int. J. Clin. Pharmacol. Ther. 2013, 51, 823–831. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, Y.; Oh, T.; Aihara, E.; Ando, A. Clinical Profiles of Nalfurafine Hydrochloride for the Treatment of Pruritus Patients. Handb. Exp. Pharmacol. 2022, 271, 455–472. [Google Scholar] [CrossRef]
- Weisshaar, E.; Szepietowski, J.C.; Bernhard, J.D.; Hait, H.; Legat, F.J.; Nattkemper, L.; Reich, A.; Sadoghi, B.; Sciascia, T.R.; Zeidler, C.; et al. Efficacy and Safety of Oral Nalbuphine Extended Release in Prurigo Nodularis: Results of a Phase 2 Randomized Controlled Trial with an Open-Label Extension Phase. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 453–461. [Google Scholar] [CrossRef]
- Kumagai, H.; Ebata, T.; Takamori, K.; Muramatsu, T.; Nakamoto, H.; Suzuki, H. Effect of a Novel Kappa-Receptor Agonist, Nalfurafine Hydrochloride, on Severe Itch in 337 Haemodialysis Patients: A Phase III, Randomized, Double-Blind, Placebo-Controlled Study. Nephrol. Dial. Transplant. 2010, 25, 1251–1257. [Google Scholar] [CrossRef] [Green Version]
- Pilla, J.E.; Devulapally, P. Difelikefalin; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Shirazian, S.; Spencer, R.; Kilfeather, S. Reduction of Pruritus by Difelikefalin Correlates With Reductions in Markers for Pruritus and Inflammation in Subjects Undergoing Hemodialysis. Am. J. Kidney Dis. 2022, 79, S42. [Google Scholar]
- Viscusi, E.R.; Torjman, M.C.; Munera, C.L.; Stauffer, J.W.; Setnik, B.S.; Bagal, S.N. Effect of Difelikefalin, a Selective Kappa Opioid Receptor Agonist, on Respiratory Depression: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Clin. Transl. Sci. 2021, 14, 1886–1893. [Google Scholar] [CrossRef]
- Shram, M.J.; Spencer, R.H.; Qian, J.; Munera, C.L.; Lewis, M.E.; Henningfield, J.E.; Webster, L.; Menzaghi, F. Evaluation of the Abuse Potential of Difelikefalin, a Selective Kappa-Opioid Receptor Agonist, in Recreational Polydrug Users. J. Clin. Transl. Sci. 2022, 15, 535–547. [Google Scholar] [CrossRef]
- Deeks, E.D. Difelikefalin: First Approval. Drugs 2021, 81, 1937–1944. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, 89. [Google Scholar] [CrossRef]
- Fishbane, S.; Mathur, V.; Germain, M.J.; Shirazian, S.; Bhaduri, S.; Munera, C.; Spencer, R.H.; Menzaghi, F.; Aaronson, M.; Alford, K.; et al. Randomized Controlled Trial of Difelikefalin for Chronic Pruritus in Hemodialysis Patients. Kidney Int. Rep. 2020, 5, 600–610. [Google Scholar] [CrossRef] [Green Version]
- Fishbane, S.; Jamal, A.; Munera, C.; Wen, W.; Menzaghi, F. A Phase 3 Trial of Difelikefalin in Hemodialysis Patients with Pruritus. N. Engl. J. Med. 2020, 382, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Narita, I.; Tsubakihara, Y.; Uchiyama, T.; Okamura, S.; Oya, N.; Takahashi, N.; Gejyo, F.; Yamamoto, A.; Ichikawa, A.; Ohishi, A.; et al. Efficacy and Safety of Difelikefalin in Japanese Patients With Moderate to Severe Pruritus Receiving Hemodialysis: A Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e2210339. [Google Scholar] [CrossRef]
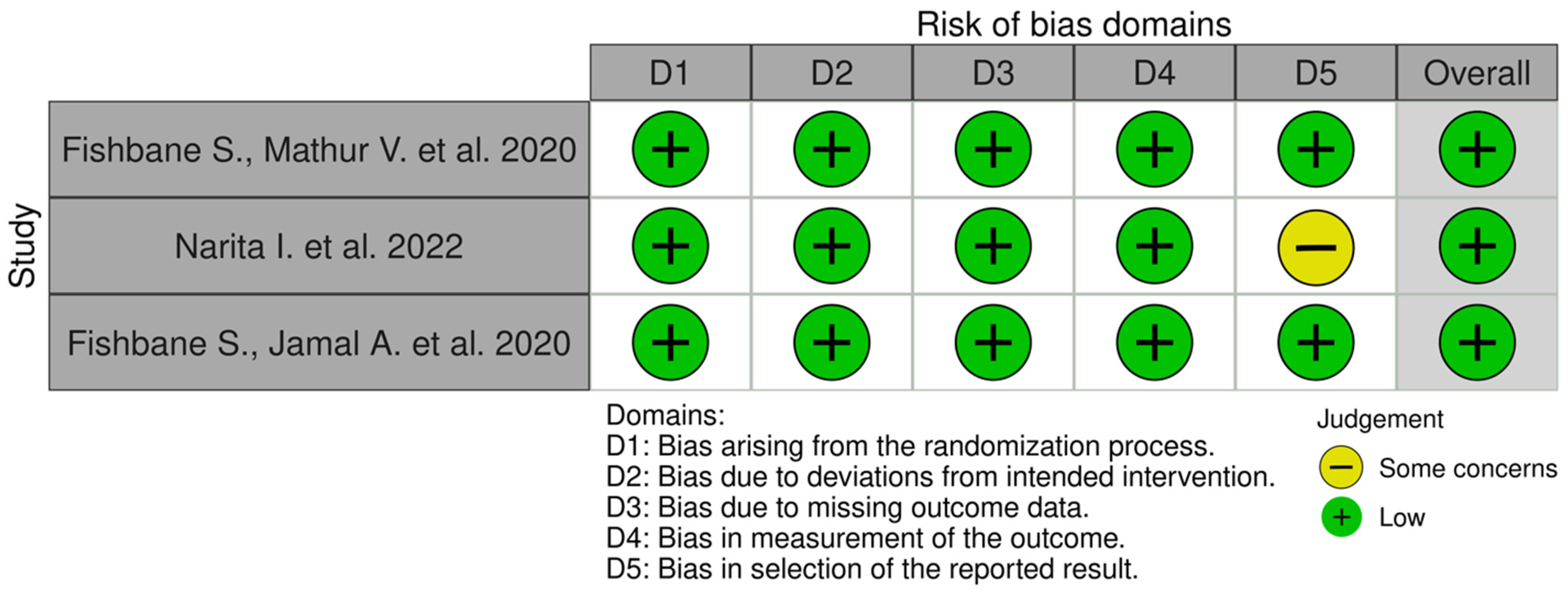
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (Robvis): An R Package and Shiny Web App for Visualizing Risk-of-bias Assessments. Res. Syn. Meth. 2020, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, T.; Yosipovitch, G. Itching as a Systemic Disease. J. Allergy Clin. Immunol. 2019, 144, 375–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimata, N.; Fuller, D.S.; Saito, A.; Akizawa, T.; Fukuhara, S.; Pisoni, R.L.; Robinson, B.M.; Akiba, T. Pruritus in Hemodialysis Patients: Results from the Japanese Dialysis Outcomes and Practice Patterns Study (JDOPPS). Hemodial. Int. 2014, 18, 657–667. [Google Scholar] [CrossRef]
- Rayner, H.C.; Larkina, M.; Wang, M.; Graham-Brown, M.; van der Veer, S.N.; Ecder, T.; Hasegawa, T.; Kleophas, W.; Bieber, B.A.; Tentori, F.; et al. International Comparisons of Prevalence, Awareness, and Treatment of Pruritus in People on Hemodialysis. Clin. J. Am. Soc. Nephrol. CJASN 2017, 12, 2000–2007. [Google Scholar] [CrossRef] [Green Version]
- Lai, J.W.; Chen, H.C.; Chou, C.Y.; Yen, H.R.; Li, T.C.; Sun, M.F.; Chang, H.H.; Huang, C.C.; Tsai, F.J.; Tschen, J.; et al. Transformation of 5-D Itch Scale and Numerical Rating Scale in Chronic Hemodialysis Patients. BMC Nephrol. 2017, 18, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vernon, M.K.; Swett, L.L.; Speck, R.M.; Munera, C.; Spencer, R.H.; Wen, W.; Menzaghi, F. Psychometric Validation and Meaningful Change Thresholds of the Worst Itching Intensity Numerical Rating Scale for Assessing Itch in Patients with Chronic Kidney Disease-Associated Pruritus. J. Patient-Rep. Outcomes 2021, 5, 1–12. [Google Scholar] [CrossRef]
- Kimel, M.; Zeidler, C.; Kwon, P.; Revicki, D.; Ständer, S. Validation of Psychometric Properties of the Itch Numeric Rating Scale for Pruritus Associated With Prurigo Nodularis: A Secondary Analysis of a Randomized Clinical Trial. JAMA Dermatol. 2020, 156, 1354–1358. [Google Scholar] [CrossRef]
- Naegeli, A.N.; Flood, E.; Tucker, J.; Devlen, J.; Edson-Heredia, E. The Worst Itch Numeric Rating Scale for Patients with Moderate to Severe Plaque Psoriasis or Psoriatic Arthritis. Int. J. Dermatol. 2015, 54, 715–722. [Google Scholar] [CrossRef]
- Elman, S.; Hynan, L.S.; Gabriel, V.; Mayo, M.J. The 5-D Itch Scale: A New Measure of Pruritus. Br. J. Dermatol. 2010, 162, 587–593. [Google Scholar] [CrossRef] [Green Version]
- Mathur, V.S.; Lindberg, J.; Germain, M.; Block, G.; Tumlin, J.; Smith, M.; Grewal, M.; McGuire, D. A Longitudinal Study of Uremic Pruritus in Hemodialysis Patients. Clin. J. Am. Soc. Nephrol. CJASN 2010, 5, 1410. [Google Scholar] [CrossRef] [Green Version]
- Cheung, H.N.; Chan, Y.S.; Hsiung, N.H. Validation of the 5-D Itch Scale in Three Ethnic Groups and Exploring Optimal Cutoff Values Using the Itch Numerical Rating Scale. Biomed. Res. Int. 2021, 2021, 7640314. [Google Scholar] [CrossRef] [PubMed]
- A Phase III Clinical Study of MR13A9 in Hemodialysis Patients with Pruritus. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04711603?term=mr13a9&draw=2&rank=1 (accessed on 22 May 2022).
- A Clinical Study of MR13A9 in Hemodialysis Patients with Pruritus. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03802617?term=mr13a9&draw=2&rank=2 (accessed on 22 May 2022).
- CR845-CLIN3103: A Global Study to Evaluate the Safety and Efficacy of CR845 in Hemodialysis Patients with Moderate-to-Severe Pruritus. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03636269?term=difelikefalin&draw=2&rank=10 (accessed on 22 May 2022).
- Extension Study to Evaluate IV CR845 in Hemodialysis Patients with Moderate-to-Severe Pruritus. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03281538?term=difelikefalin&draw=2&rank=14 (accessed on 22 May 2022).
- Study to Evaluate IV CR845 in Hemodialysis Patients with Moderate-to-Severe Pruritus. Available online: https://www.clinicaltrials.gov/ct2/show/NCT02858726?term=difelikefalin&draw=2&rank=13 (accessed on 22 May 2022).
- A Study to Evaluate the Safety and Efficacy of CR845 in Hemodialysis Patients with Moderate-to-Severe Pruritus (KALM-1). Available online: https://www.clinicaltrials.gov/ct2/show/NCT03422653?term=difelikefalin&draw=2&rank=12 (accessed on 22 May 2022).
- CR845-CLIN3105: A Study to Evaluate the Safety and Effectiveness of CR845 in Hemodialysis Patients with Moderate-to-Severe Pruritus. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03998163?term=difelikefalin&draw=2&rank=11 (accessed on 22 May 2022).
- A Study to Evaluate the Safety and Efficacy of CR845 in Chronic Kidney Disease Patients with Moderate-to-Severe Pruritus. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03617536?term=difelikefalin&draw=2&rank=9 (accessed on 22 May 2022).
- Study to Evaluate the Pharmacokinetics and Metabolism of [14C] CR845 (Difelikefalin) in Patients with End Stage Renal Disease on Hemodialysis and in Healthy Subjects. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03947970?term=difelikefalin&draw=2&rank=8 (accessed on 22 May 2022).
- Intermediate-Size Patient Population Expanded Access Program for Intravenous Difelikefalin. Available online: https://www.clinicaltrials.gov/ct2/show/NCT05031546?term=difelikefalin&draw=2&rank=4 (accessed on 22 May 2022).
- A Study to Evaluate the Safety and Efficacy of Difelikefalin in Advanced Chronic Kidney Disease Patients with Moderate-to-Severe Pruritus and Not on Dialysis. Available online: https://www.clinicaltrials.gov/ct2/show/NCT05342623?term=difelikefalin&draw=2&rank=2 (accessed on 22 May 2022).
- Study to Evaluate the Efficacy and Safety of Oral Difelikefalin (CR845) for Moderate to Severe Pruritus in Subjects with Notalgia Paresthetica (KOMFORT). Available online: https://www.clinicaltrials.gov/ct2/show/NCT04706975?term=difelikefalin&draw=2&rank=1 (accessed on 22 May 2022).
- Study to Evaluate the Safety and Efficacy of Oral CR845 (Difelikefalin) in Patients with Primary Biliary Cholangitis (PBC) and Moderate-to-Severe Pruritus. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03995212?term=difelikefalin&draw=2&rank=7 (accessed on 22 May 2022).
- Study to Evaluate the Efficacy and Safety of Oral Difelikefalin (CR845) for Moderate to Severe Pruritus in Subjects with Atopic Dermatitis. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04018027?term=difelikefalin&draw=2&rank=5 (accessed on 22 May 2022).
- Home-ClinicalTrials.Gov. Available online: https://www.clinicaltrials.gov/ (accessed on 22 May 2022).
- Little, P.J. Peripherally Restricted Opioid Analgesics. ACS Symp. Ser. 2013, 1131, 201–222. [Google Scholar] [CrossRef]
- Fishbane, S.; Wen, W.; Munera, C.; Menzaghi, F. Long-Term Safety and Efficacy of Difelikefalin in Patients With Chronic Kidney Disease–Associated Pruritus: Analysis From KALM-1 and KALM-2. Am. J. Kidney Dis. 2021, 77, 593–594. [Google Scholar] [CrossRef]
- Kapruvia|European Medicines Agency. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/kapruvia (accessed on 22 May 2022).
- Harden, R.; Burns, J.; Connolly, S.; Kirsling, A.; Abousaad, E.; Khoury, A.; Walega, D. (422) CR845, a Peripheral Kappa Opioid, Provides Better Pain Relief with Less Nausea and Vomiting than Placebo in Patients after Bunionectomy. J. Pain 2015, 16, S81. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Title | Fishbane et al. [39] | Narita et al. [41] | Fishbane et al. [40] |
|---|---|---|---|
| Phase | 2 | 2 | 3 |
| Country | US | Japan | US |
| Number of patients | 175 | 247 | 378 |
| Time to end-point | 8 weeks | 8 weeks | 12 weeks |
| Reserach groups | Placebo (n = 45) Difelikefalin 0.5 μg/kg (n = 44) Difelikefalin 1.0 μg/kg (n = 42) Difelikefalin 1.5 μg/kg (n = 44) |
Placebo (n = 63)
Difelikefalin 0.25 μg/kg (n = 61) Difelikefalin 0.5 μg/kg (n = 61) Difelikefalin 1.0 μg/kg (n = 62) | Placebo (n = 165) Difelikefalin 0.5 μg/kg (n = 158) |
| Evaluated parameters | WI-NRS Skindex-10 5-D itch scale Medical Outcomes Study sleep disturbance subscale Patient Global Impression of Worst Itch Severity Patient Global Impression of Change | WI-NRS Skindex-16 5-D itch scale Patient Global Impression of Change | WI-NRS Skindex-10 5-D itch scale |
| Changes from baseline in WI-NRS | |||
| -reduction of weekly mean WI-NRS | Placebo group: −1.9 Difelikefalin 0.5 μg/kg: −3.8 Difelikefalin 1.0 μg/kg: −2.8 Difelikefalin 1.5 μg/kg: −3.2 | Placebo group: −2.86, Difelikefalin 0.25 μg/kg: −2.97 Difelikefalin 0.5 μg/kg: −3.65 Difelikefalin 1.0 μg/kg: −3.64 | N/A |
| -reduction of at least 3 points | Placebo group: 29% Difelikefalin 0.5 μg/kg: 64% Difelikefalin 1.0 μg/kg: N/A Difelikefalin 1.5 μg/kg: 67% | Placebo group: 50% Difelikefalin 0.25 μg/kg: 53% Difelikefalin 0.5 μg/kg: 60% Difelikefalin 1.0 μg/kg: 57% | Placebo group: 27.9% Difelikefalin 0.5 μg/kg: 49.1% |
| -reduction of at least 4 points | Placebo group: 24% Difelikefalin 0.5 μg/kg: 51% Difelikefalin 1.0 μg/kg: N/A Difelikefalin 1.5 μg/kg: N/A | Placebo group: 36%, Difelikefalin 0.25 μg/kg: 34% Difelikefalin 0.5 μg/kg: 51% Difelikefalin 1.0 μg/kg: 43% | Placebo group: 21.2% Difelikefalin 0.5 μg/kg: 40.5% |
| Changes from baseline after treatment in Skindex-10 or Skindex-16 (points) | Placebo group: −8.2 Difelikefalin 0.5 μg/kg: −18.7 Difelikefalin 1.0 μg/kg: −15.5 Difelikefalin 1.5 μg/kg: −15.1 | * Placebo group: −24.04 * Difelikefalin 0.25 μg/kg: −24.25 * Difelikefalin 0.5 μg/kg: −27.79 * Difelikefalin 1.0 μg/kg: −22.69 | Placebo group: –12.0 Difelikefalin 0.5 μg/kg: −17.2 |
| Changes from baseline after treatment in 5-D itch scale (points) | Placebo group: −2.8 Difelikefalin 0.5 μg/kg: −5.7 Difelikefalin 1.0 μg/kg: −5.4 Difelikefalin 1.5 μg/kg: −4.7 | Placebo group: −5.8 Difelikefalin 0.25 μg/kg: −6.6 Difelikefalin 0.5 μg/kg: −6.5 Difelikefalin 1.0 μg/kg: −6.8 | Placebo group: –3.7 Difelikefalin 0.5 μg/kg: –5.0 |
| Adverse effects | |||
| -overall incidence | Placebo group: 4 patients (8.9%) Difelikefalin 0.5 μg/kg: 10 patients (22.7%) Difelikefalin 1.0 μg/kg: 6 patients (14.6%) Difelikefalin 1.5 μg/kg: 11 patients (25.0%) | Placebo group: 42 patients (67%) Difelikefalin 0.25 μg/kg: 44 patients (72%), Difelikefalin 0.5 μg/kg: 47 of 61 patients (77%), Difelikefalin 1.0 μg/kg: 53 of 62 patients (85%) | Placebo group: 117 patients (62.2%) Difelikefalin 0.5 μg/kg: 130 patients (68.8%) |
| -symptoms | Mild: diarrhea, dizziness, nausea, fall, headache More severe: somnolence, abdominal pain, mental status changes | Mild: dizziness, vomiting, nasopharyngitis More severe: somnolence, hypotension | Mild: diarrhea, dizziness, vomiting More severe: hyperkalemia, pneumonia, sepsis, hypotension and chronic obstructive pulmonary disease |
| Title | ClinicalTrials.Gov Identifier | Condition | Phase | Status | Number of Participants | Dose of Difelikefalin | Year |
|---|---|---|---|---|---|---|---|
| Safety and Pharmacokinetics of IV CR845 in Hemodialysis Patients, and Its Efficacy in Patients With Uremic Pruritus | NCT02229929 | CKD-aP | 2 | Completed | 89 | 0.5 μg, 1.0 μg, or 2.5 μg/kg administered after each dialysis session over a 1 week treatment period (3 times/week) | 2014–2016 |
| Study to Evaluate IV CR845 in Hemodialysis Patients With Moderate-to-Severe Pruritus | NCT02858726 | CKD-aP | 2/3 | Completed | 226 | 0.5 μg, 1.0 μg, or 1.5 μg/kg administered after each dialysis session (3 times/week) | 2016–2018 |
| Extension Study to Evaluate IV CR845 in Hemodialysis Patients With Moderate-to-Severe Pruritus | NCT03281538 | CKD-aP | 3 | Completed | 288 | 0.5 μg/kg administered after each dialysis session (3 times/week) | 2017–2021 |
| A Study to Evaluate the Safety and Efficacy of CR845 in Chronic Kidney Disease Patients With Moderate-to-Severe Pruritus | NCT03617536 | CKD-aP | 2 | Completed | 271 | 0.25, 0.5 or 1 mg; oral; once a day | 2018–2020 |
| A Study to Evaluate the Safety and Efficacy of CR845 in Hemodialysis Patients With Moderate-to-Severe Pruritus (KALM-1) | NCT03422653 | CKD-aP | 3 | Completed | 378 | 0.5 μg/kg administered after each dialysis session (3 times/week) | 2018–2020 |
| CR845-CLIN3103: A Global Study to Evaluate the Safety and Efficacy of CR845 in Hemodialysis Patients With Moderate-to-Severe Pruritus | NCT03636269 | CKD-aP | 3 | Completed | 474 | 0.5 μg/kg administered after each dialysis session (3 times/week) | 2018–2021 |
| CR845-CLIN3105: A Study to Evaluate the Safety and Effectiveness of CR845 in Hemodialysis Patients With Moderate-to-Severe Pruritus | NCT03998163 | CKD-aP | 3 | Completed | 222 | 0.5 μg/kg administered after each dialysis session (3 times/week) | 2019–2021 |
| A Clinical Study of MR13A9 in Hemodialysis Patients With Pruritus | NCT03802617 | CKD-aP | 2 | Completed | 247 | 0.25 mg, 0.5 mg, or 1.0 mg/kg administered after each dialysis session (3 times/week) | 2019–2019 |
| Study to Evaluate the Pharmacokinetics and Metabolism of [14C] CR845 (Difelikefalin) in Patients With End Stage Renal Disease on Hemodialysis and in Healthy Subjects | NCT03947970 | Healthy and hemodialysis patients | 1 | Completed | 12 | intravenous bolus-the total dose of CR845 will range from 1.7 to 3.1 μg/kg | 2019–2019 |
| Intermediate-Size Patient Population Expanded Access Program for Intravenous Difelikefalin | NCT05031546 | CKD-aP | N/A | Available | N/A Expanded Access to Treatmend | 0.5 μg kg administered after each dialysis session (3 times/week) | 2021- |
| A Phase III Clinical Study of MR13A9 in Hemodialysis Patients With Pruritus | NCT04711603 | CKD-aP | 3 | Active, not recruiting | 172 | dose undefined, administered after each dialysis session (3 times/week) | 2021- |
| Study to Evaluate the Efficacy and Safety of Oral Difelikefalin (CR845) for Moderate to Severe Pruritus in Subjects With Notalgia Paresthetica (KOMFORT) | NCT04706975 | CKD-aP and notalgia paresthetica | 2 | Recruiting | 120 | 2.0 mg; oral; twice a day | 2021- |
| A Study to Evaluate the Safety and Efficacy of Difelikefalin in Advanced Chronic Kidney Disease Patients With Moderate-to-Severe Pruritus and Not on Dialysis | NCT05342623 | CKD-aP | 3 | Before recruiting | 400 | 1.0 mg; oral; once a day | 2022- |
| Study to Evaluate the Efficacy and Safety of Oral Difelikefalin (CR845) for Moderate to Severe Pruritus in Subjects With Atopic Dermatitis | NCT04018027 | Atopic Dermatitis associated pruritus | 2 | Completed | 401 | 0.25 mg, 0.5 mg, or 1.0 mg, oral; twice a day | 2019–2022 |
| Study to Evaluate the Safety and Efficacy of Oral CR845 (Difelikefalin) in Patients With Primary Biliary Cholangitis (PBC) and Moderate-to-Severe Pruritus | NCT03995212 | Cholestatic Pruritus | 2 | Recruiting | 60 | 1.0 mg; oral; twice a day | 2019–2021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wala, K.; Szepietowski, J.C. Difelikefalin in the Treatment of Chronic Kidney Disease-Associated Pruritus: A Systematic Review. Pharmaceuticals 2022, 15, 934. https://doi.org/10.3390/ph15080934
Wala K, Szepietowski JC. Difelikefalin in the Treatment of Chronic Kidney Disease-Associated Pruritus: A Systematic Review. Pharmaceuticals. 2022; 15(8):934. https://doi.org/10.3390/ph15080934
Chicago/Turabian StyleWala, Kamila, and Jacek C. Szepietowski. 2022. "Difelikefalin in the Treatment of Chronic Kidney Disease-Associated Pruritus: A Systematic Review" Pharmaceuticals 15, no. 8: 934. https://doi.org/10.3390/ph15080934