
Anti-Cytomegalovirus Therapy: Whether and When to Initiate, Those Are the Questions


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
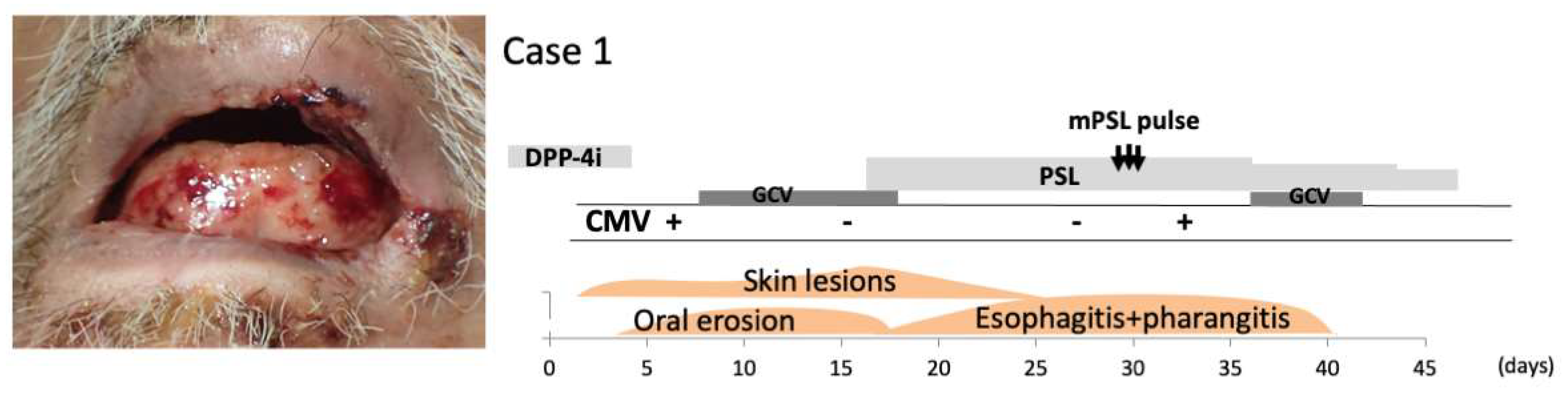
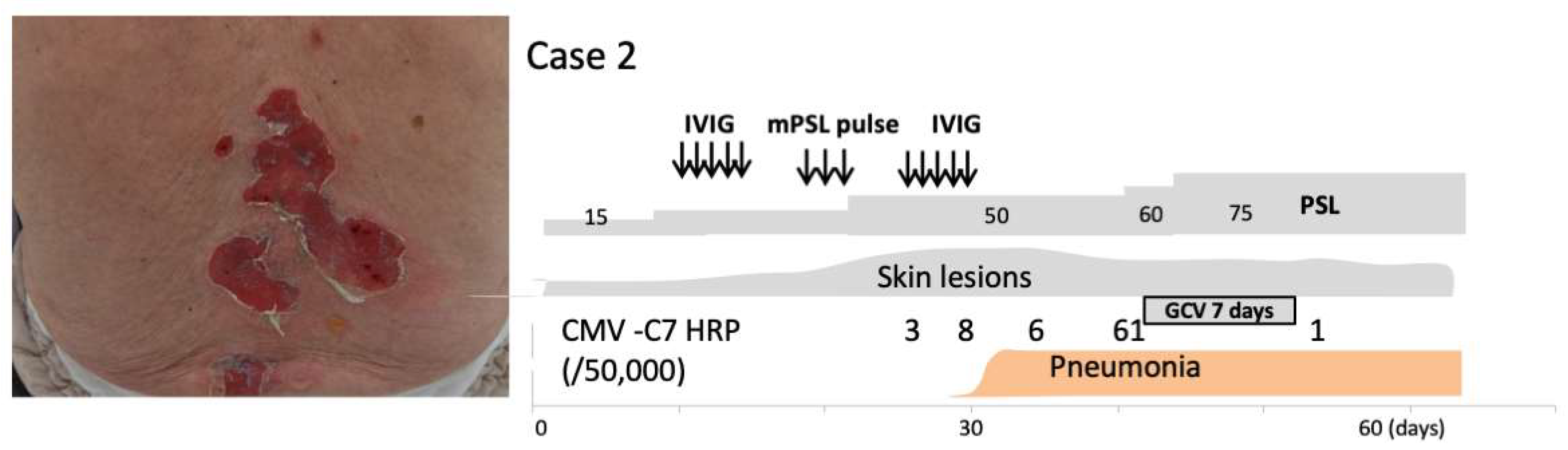
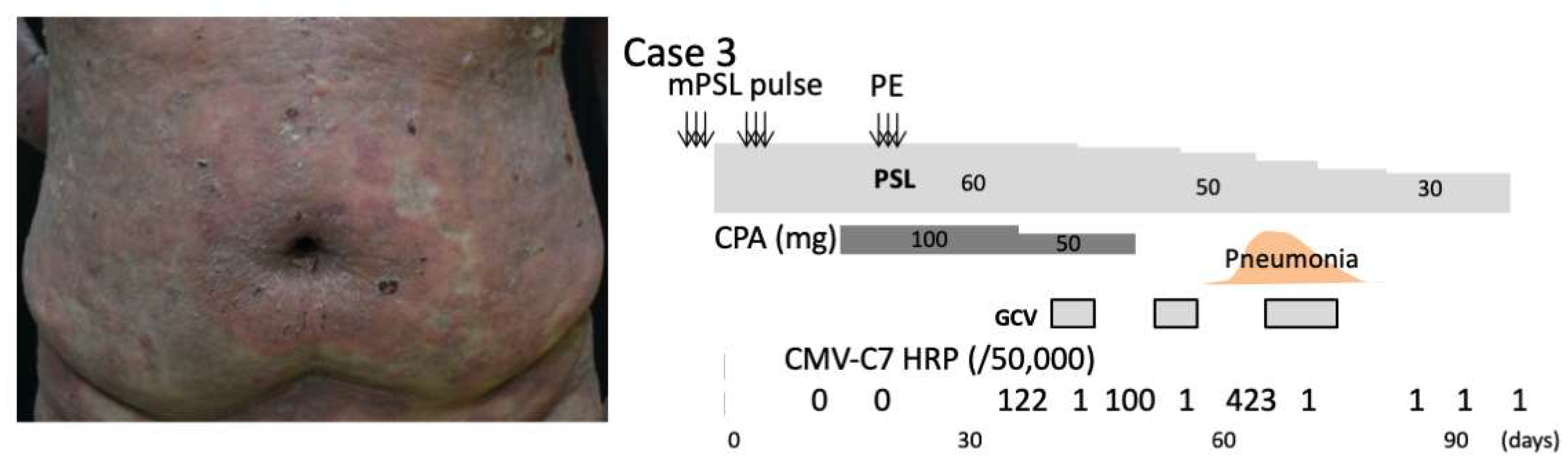
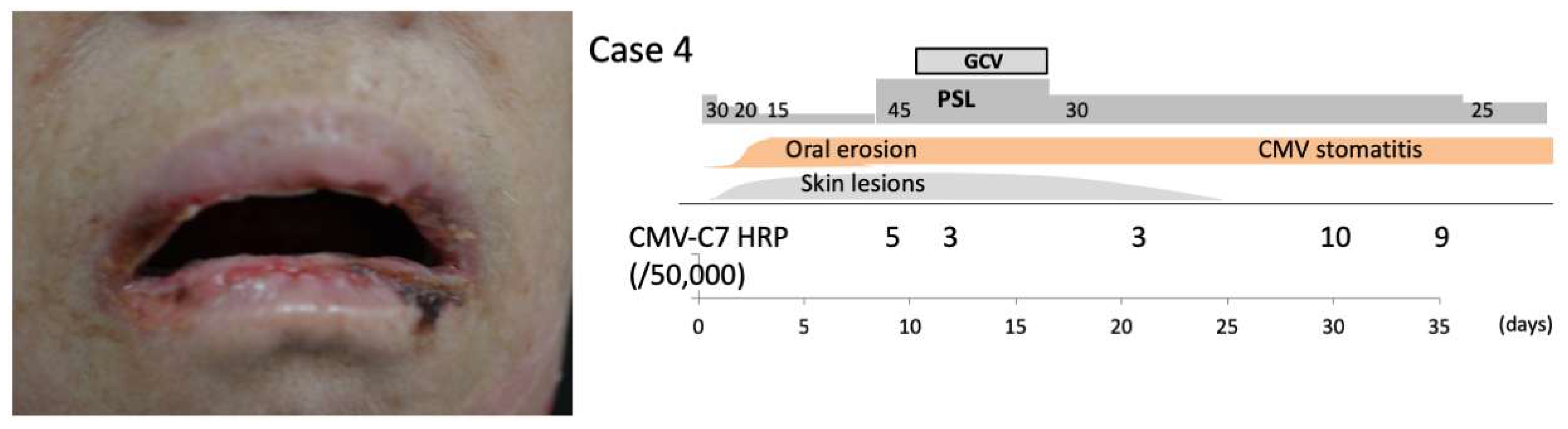
2.1. Case Presentation
2.2. Findings Suggestive of CMV Reactivation in AIBD Patients with Esophagitis and Pneumonia
2.3. Factors Contributing to the Onset of CMV-IRIS
2.4. CMV Reactivation as a Manifestation of IRIS and Anti-CMV Therapy
3. Discussion
3.1. How to Predict CMV-IRIS
3.2. How to Treat CMV-IRIS with Anti-CMV Therapy and Immunosuppressive Therapy
3.3. Recent Topics on the CMV–Host Interactions Relevant to CMV Reactivation
4. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Choi, Y.L.; Kim, J.A.; Jang, K.T.; Kim, D.S.; Kim, W.S.; Lee, J.H.; Yang, J.M.; Lee, E.S.; Lee, D.Y. Characteristics of cutaneous cytomegalovirus infection in non-acquired immune deficiency syndrome, immunocompromised patients. Brit. J. Dermatol. 2006, 155, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Mizukawa, Y.; Hirahara, K.; Kano, Y.; Shiohara, T. Drug-induced hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms severity score: A useful tool for assessing disease severity and predicting fatal cytomegalovirus disease. J. Am. Acad. Dermatol. 2018, 80, 670–678.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoyama, Y.; Sugiyama, S.; Katayama, C.; Kamiya, K. Risk factors for cytomegalovirus reactivation in autoimmune bullous disease patients on immunosuppressive therapy. Australas. J. Dermatol. 2021, 62, e343–e344. [Google Scholar] [CrossRef] [PubMed]
- Razonable, R.R. Cytomegalovirus infection after liver transplantation: Current concepts and challenges. World J. Gastroenterol. 2008, 14, 4849–4860. [Google Scholar] [CrossRef] [Green Version]
- Nebbia, G.; Mattes, F.M.; Sabin, C.A.; Samonakis, D.; Rolando, N.; Burroughs, A.K.; Emery, V.C. Differential Effects of Prednisolone and Azathioprine on the Development of Human Cytomegalovirus Replication Post Liver Transplantation. Transplantation 2007, 84, 605–610. [Google Scholar] [CrossRef]
- Kumar, S.; De, D.; Handa, S.; Ratho, R.; Bhandari, S.; Pal, A.; Kamboj, P.; Sarkar, S. Identification of factors associated with treatment refractoriness of oral lesions in pemphigus vulgaris. Br. J. Dermatol. 2017, 177, 1583–1589. [Google Scholar] [CrossRef]
- Shelburne, S.A.; Hamill, R.J.; Rodriguez-Barradas, M.C.; Greenberg, S.B.; Atmar, R.L.; Musher, D.M.; Gathe, J.C.; Visnegarwala, F.; Trautner, B.W. Immune Reconstitution Inflammatory Syndrome: Emergence of a Unique Syndrome during Highly Active Antiretroviral Therapy. Medicine 2002, 81, 213–227. [Google Scholar] [CrossRef]
- Shiohara, T.; Kurata, M.; Mizukawa, Y.; Kano, Y. Recognition of Immune Reconstitution Syndrome Necessary for Better Management of Patients with Severe Drug Eruptions and Those under Immunosuppressive Therapy. Allergol. Int. 2010, 59, 333–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murdoch, D.M.; Venter, W.D.; Van Rie, A.; Feldman, C. Immune reconstitution inflammatory syndrome (IRIS): Review of common infectious manifestations and treatment options. AIDS Res. Ther. 2007, 4, 9. [Google Scholar] [CrossRef] [Green Version]
- Narita, Y.M.; Horie, C.; Hirahara, K.; Kano, Y.; Shiohara, T.; Mizukawa, Y. Bullous pemphigoid complicated by cytomegalovirus disease as a manifestation of immune reconstitution inflammatory syndrome: Retrospective analyses of our institutional cases and literature review. Int. J. Dermatol. 2018, 57, 202–208. [Google Scholar] [CrossRef]
- Mizukawa, Y.; Kimishima, M.; Aoyama, Y.; Shiohara, T. Predictive biomarkers for cytomegalovirus reactivation before and after immunosuppressive therapy: A single-institution retrospective long-term analysis of patients with drug-induced hypersensitivity syndrome (DiHS)/drug reaction with eosinophilia and systemic syndrome (DRESS). Int. J. Infect. Dis. 2020, 100, 239–246. [Google Scholar] [PubMed]
- Sueki, H.; Mizukawa, Y.; Aoyama, Y. Immune reconstitution inflammatory syndrome in non-HIV immunosuppressed patients. J. Dermatol. 2017, 45, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, S.; Yamamoto, T.; Aoyama, Y. Neutrophil to lymphocyte ratio is predictive of severe complications and mortality in patients with dipeptidyl peptidase-4 inhibitor-associated bullous pemphigoid: A retrospective longitudinal observational study. J. Am. Acad. Dermatol. 2022, 86, 1387–1390. [Google Scholar] [CrossRef]
- Aso, Y.; Fukushima, M.; Sagara, M.; Jojima, T.; Iijima, T.; Suzuki, K.; Momobayashi, A.; Kasai, K.; Inukai, T. Sitagliptin, a DPP-4 inhibitor, alters the subsets of circulating CD4+ T cells in patients with type 2 diabetes. Diabetes Res. Clin. Pract. 2015, 110, 250–256. [Google Scholar] [CrossRef]
- Mobacken, H.; Al Karawi, M.; Mohamed, A.; Coode, P. Oesophageal pemphigus vulgaris. Dermatologica 1988, 176, 266–269. [Google Scholar] [CrossRef]
- Çalka, Ö.; Akdeniz, N.; Tuncer, I.; Metin, A.; Cesur, R.S. Oesophageal involvement during attacks in pemphigus vulgaris patients. Clin. Exp. Dermatol. 2006, 31, 515–519. [Google Scholar] [CrossRef]
- Baroco, A.L.; Oldfield, E.C. Gastrointestinal cytomegalovirus disease in the immunocompromised patient. Curr. Gastroenterol. Rep. 2008, 10, 409–416. [Google Scholar] [CrossRef]
- Sun, H.-Y.; Munoz, P.; Torre-Cisneros, J.; Aguado, J.M.; Lattes, R.; Montejo, M.; Garcia-Reyne, A.; Bouza, E.; Valerio, M.; Lara, R.; et al. Mycobacterium Tuberculosis—Associated Immune Reconstitution Syndrome in Solid-Organ Transplant Recipients. Transplantation 2013, 95, 1173–1181. [Google Scholar] [CrossRef]
- Sugiyama, S.; Tanaka, R.; Hayashi, H.; Izumi, K.; Nishie, W.; Aoyama, Y. Acquired Haemophilia A in DPP4 Inhibitor-Induced Bullous Pemphigoid as Immune Reconstitution Syndrome. Acta Derm. Venereol. 2020, 100, adv00178. [Google Scholar] [CrossRef]
- Mizukawa, Y.; Aoyama, Y.; Takahashi, H.; Takahashi, R.; Shiohara, T. Risk of Progression to Autoimmune Disease in Severe Drug Eruption: Risk Factors and the Factor-Guided Stratification. J. Investig. Dermatol. 2021, 142, 960–968.e9. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, R.; Kano, Y.; Yamazaki, Y.; Kimishima, M.; Mizukawa, Y.; Shiohara, T. Defective Regulatory T Cells in Patients with Severe Drug Eruptions: Timing of the Dysfunction Is Associated with the Pathological Phenotype and Outcome. J. Immunol. 2009, 182, 8071–8079. [Google Scholar] [CrossRef] [Green Version]
- Di Bona, D.; Scafidi, V.; Plaia, A.; Colomba, C.; Nuzzo, D.; Occhino, C.; Tuttolomondo, A.; Giammanco, G.; De Grazia, S.; Montalto, G.; et al. HLA and killer cell immunoglobulin-like receptors influence the natural course of CMV infection. J. Infect. Dis. 2014, 210, 1083–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aiello, A.; Accardi, G.; Candore, G.; Caruso, C.; Colomba, C.; Di Bona, D.; Duro, G.; Gambino, C.M.; Ligotti, M.E.; Pandey, J.P. Role of Immunogenetics in the Outcome of HCMV Infection: Implications for Ageing. Int. J. Mol. Sci. 2019, 20, 685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Bona, D.; Accardi, G.; Aiello, A.; Bilancia, M.; Candore, G.; Colomba, C.; Caruso, C.; Duro, G.; Gambino, C.M.; Macchia, L.; et al. Association between γ marker, human leucocyte antigens and killer immunoglobulin-like receptors and the natural course of human cytomegalovirus infection: A pilot study performed in a Sicilian population. Immunology 2018, 153, 523–531. [Google Scholar] [CrossRef] [Green Version]
- Pandey, J.P.; Kistner-Griffin, E.; Radwan, F.F.; Kaur, N.; Namboodiri, A.M.; Black, L.; Butler, M.A.; Carreón, T.; Ruder, A.M. Immunoglobulin Genes Influence the Magnitude of Humoral Immunity to Cytomegalovirus Glycoprotein, B. J. Infect. Dis. 2014, 210, 1823–1826. [Google Scholar] [CrossRef] [Green Version]
- Shiohara, T.; Mizukawa, Y. Drug-induced hypersensitivity syndrome (DiHS)/drug reaction with eosinophilia and systemic symptoms (DRESS): An update in 2019. Allergol. Int. 2019, 68, 301–308. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aoyama, Y.; Sugiyama, S.; Yamamoto, T. Anti-Cytomegalovirus Therapy: Whether and When to Initiate, Those Are the Questions. Pharmaceuticals 2022, 15, 797. https://doi.org/10.3390/ph15070797
Aoyama Y, Sugiyama S, Yamamoto T. Anti-Cytomegalovirus Therapy: Whether and When to Initiate, Those Are the Questions. Pharmaceuticals. 2022; 15(7):797. https://doi.org/10.3390/ph15070797
Chicago/Turabian StyleAoyama, Yumi, Seiko Sugiyama, and Takenobu Yamamoto. 2022. "Anti-Cytomegalovirus Therapy: Whether and When to Initiate, Those Are the Questions" Pharmaceuticals 15, no. 7: 797. https://doi.org/10.3390/ph15070797