Author Contributions
Conceptualization, C.M. and M.v.d.A.; methodology, R.B., D.L., J.K.-N., C.M. and M.v.d.A.; formal analysis, D.L.; investigation, R.B., D.L. and M.v.d.A.; data curation, D.L. and J.B.; writing—original draft preparation, R.B. and D.L.; writing—review and editing, R.B., D.L., J.B., P.K.-M., J.K.-N., C.M. and M.v.d.A.; visualization, R.B. and D.L.; supervision, M.v.d.A.; project administration, P.K.-M., J.K.-N., C.M. and M.v.d.A.; funding acquisition, P.K.-M., J.K.-N. and C.M. All authors have read and agreed to the published version of the manuscript.
Acknowledgments
We would like to thank Phillip Elliott for the professional language review, and the whole AdAM study group for their cooperative and productive work in the past years. Members of the Adam study group include: Lara Düvel (BARMER, Wuppertal, Germany), Till Beckmann (BARMER, Wuppertal, Germany), Reinhard Hammerschmidt (KVWL, Dortmund, Germany), Julia Jachmich (KVWL, Dortmund, Germany), Eva Leicher (KVWL, Dortmund, Germany), Benjamin Brandt (KVWL, Dortmund, Germany), Johanna Richard (KVWL, Dortmund, Germany), Frank Meyer (KVWL, Dortmund, Germany), Mathias Flume (KVWL, Dortmund, Germany), Thomas Müller (KVWL, Dortmund, Germany), Ferdinand M. Gerlach (Institute of General Practice, Goethe-University, Frankfurt am Main, Germany), Beate S. Müller (Institute of General Practice, Goethe-University, Frankfurt am Main, Germany), Benno Flaig (Institute of General Practice, Goethe University, Frankfurt am Main, Germany), Ana Isabel González-González (Institute of General Practice, Goethe-University, Frankfurt am Main, Germany), Truc Sophia Dinh (Institute of General Practice, Goethe-University, Frankfurt am Main, Germany), Kiran Chapidi (formerly Institute of General Practice, Goethe-University, Frankfurt am Main, Germany), Peter Ihle (PMV research group, University of Cologne, Cologne, Germany), Ingo Meyer (PMV research group, University of Cologne, Cologne, Germany), Hans Joachim Trampisch (Department of Medical Informatics, Biometry and Epidemiology, Ruhr University, Bochum, Germany), Renate Klaaßen-Mielke (Department of Medical Informatics, Biometry and Epidemiology, Ruhr University, Bochum, Germany), Nina Timmesfeld (Department of Medical Informatics, Biometry and Epidemiology, Ruhr University, Bochum, Germany), Wolfgang Greiner (Department of Health Economics and Health Care Management, Faculty of Health Science, Bielefeld University, Bielefeld, Germany), Bastian Surmann (Department of Health Economics and Health Care Management, Faculty of Health Science, Bielefeld University, Bielefeld, Germany), Holger Pfaff (Institute for Medical Sociology, Health Services Research and Rehabilitation Science, Department of Health Services Research, University of Cologne, Cologne, Germany), Ute Karbach (Technical University Dortmund, Department of Rehabilitation Sociology, Faculty of Rehabilitation Sciences, Dortmund, Germany), Alexandra Piotrowski (Center for Health Economics and Health Services Research, University of Wuppertal, Germany), Karolina Beifuß (Center for Health Economics and Health Services Research, University of Wuppertal, Germany), Sarah Meyer (Center for Health Economics and Health Services Research, University of Wuppertal, Germany), Sara Söling (Center for Health Economics and Health Services Research, University of Wuppertal, Germany), Daniel Grandt (Department of Internal Medicine. Clinic Saarbrücken, Germany), Simone Grandt (RpDoc Solutions GmbH, Saarbrücken, Germany).
Figure 1.
Distribution of patients, GPs, and practices in the defined populations (AP: active population, IP: inactive population, NEP: non-enrolled potentials).
Figure 1.
Distribution of patients, GPs, and practices in the defined populations (AP: active population, IP: inactive population, NEP: non-enrolled potentials).
Figure 2.
Box plot showing the number of alerts per patient at T0 and T1 (A), stratified according to the subgroups “severe alerts” (B), “completed anamnesis” (C), and a combination of both subgroups (D).
Figure 2.
Box plot showing the number of alerts per patient at T0 and T1 (A), stratified according to the subgroups “severe alerts” (B), “completed anamnesis” (C), and a combination of both subgroups (D).
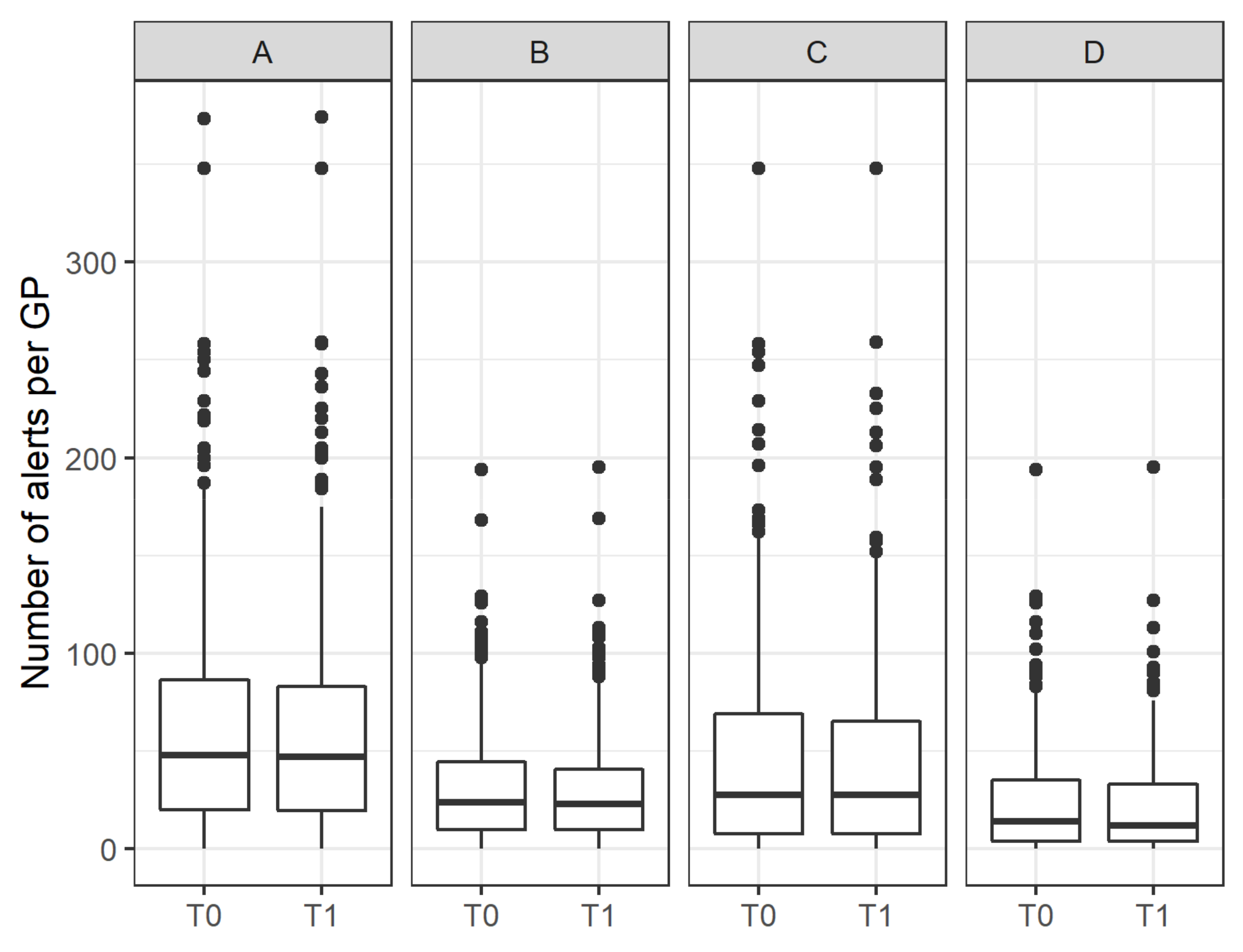
Figure 3.
Box plot showing the number of alerts per GP at T0 and T1 (A), stratified according to the subgroups “severe alerts” (B), “completed anamnesis” (C) and a combination of both subgroups (D).
Figure 3.
Box plot showing the number of alerts per GP at T0 and T1 (A), stratified according to the subgroups “severe alerts” (B), “completed anamnesis” (C) and a combination of both subgroups (D).
Figure 4.
Average change in the number of alerts per GP, stratified according to the number of patients from the active study population treated by the GP (expressed in quartiles).
Figure 4.
Average change in the number of alerts per GP, stratified according to the number of patients from the active study population treated by the GP (expressed in quartiles).
Figure 5.
Steps to be climbed in order to achieve Intervention Fidelity. The left-hand legend shows the dimensions impacted by the steps.
Figure 5.
Steps to be climbed in order to achieve Intervention Fidelity. The left-hand legend shows the dimensions impacted by the steps.
Figure 6.
Number of patients, stratified by the day in the week when T0 was triggered.
Figure 6.
Number of patients, stratified by the day in the week when T0 was triggered.
Figure 7.
Number of patients stratified by month of the year when T0 was triggered.
Figure 7.
Number of patients stratified by month of the year when T0 was triggered.
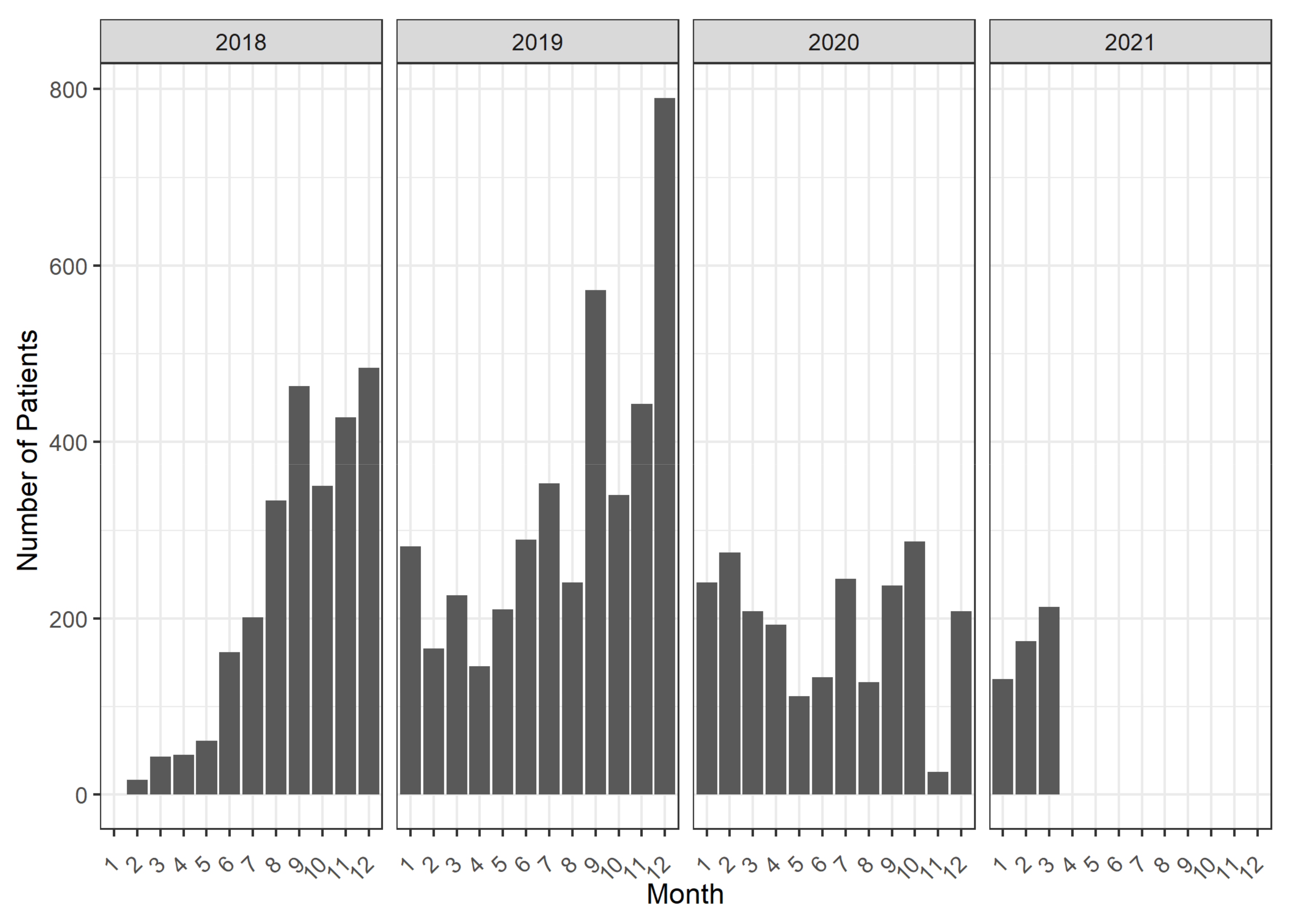
Figure 8.
Number of patients, stratified by the month and year when T0 was triggered over the course of the study.
Figure 8.
Number of patients, stratified by the month and year when T0 was triggered over the course of the study.
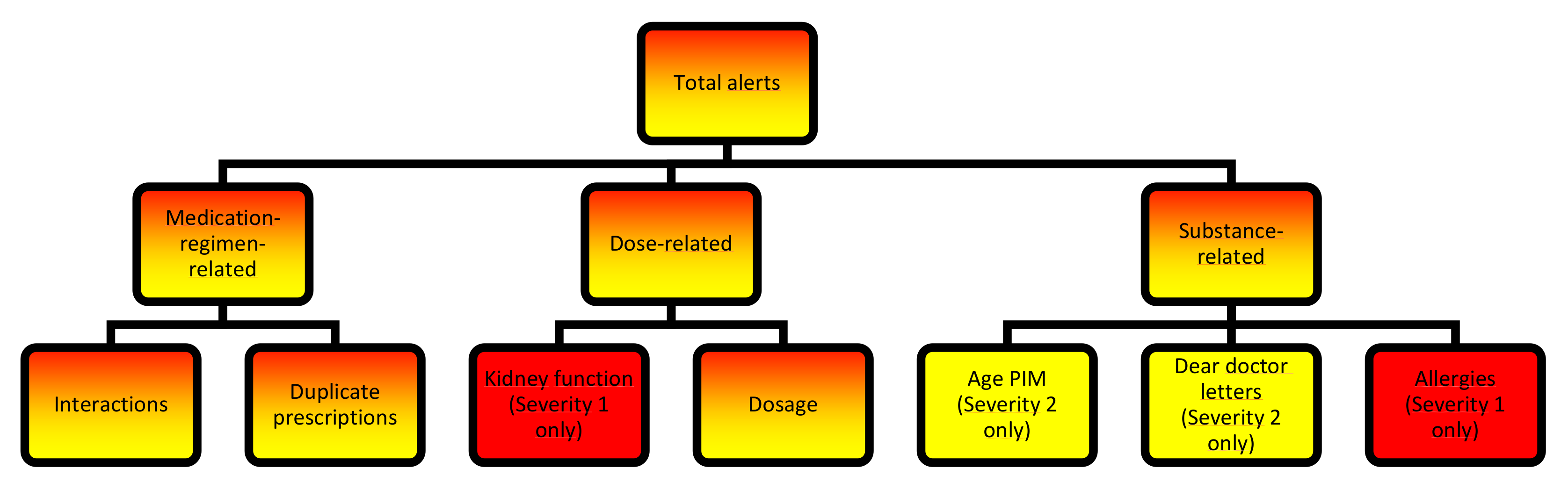
Figure 9.
Alert categories documented by the software. Red font indicates alerts of the highest severity, and yellow font indicates medium severity.
Figure 9.
Alert categories documented by the software. Red font indicates alerts of the highest severity, and yellow font indicates medium severity.
Figure 10.
Schematic working process for GPs that use eMMa. The final step (purple field) defines T1.
Figure 10.
Schematic working process for GPs that use eMMa. The final step (purple field) defines T1.
Figure 11.
Populations that were compared for the Reach dimension.
Figure 11.
Populations that were compared for the Reach dimension.
Table 1.
Group comparison of AP and NEP patients.
Table 1.
Group comparison of AP and NEP patients.
| Predictors | OR | 95% CI | p-Value |
|---|
| (Intercept) | 0.17 | 0.14–0.19 | <0.001 |
| Age | 1.01 | 1.01–1.01 | <0.001 |
| Sex (ref: male) | | | |
| Female | 0.93 | 0.89–0.98 | 0.004 |
| medCDS * | 1.04 | 0.98–1.09 | 0.177 |
| Nursing care level (ref: 0) | | | |
| Nursing care level 1 | 0.76 | 0.65–0.88 | <0.001 |
| Nursing care level 2 | 0.74 | 0.68–0.80 | <0.001 |
| Nursing care level 3 | 0.52 | 0.46–0.57 | <0.001 |
| Nursing care level 4 | 0.34 | 0.29–0.40 | <0.001 |
| Nursing care level 5 | 0.27 | 0.21–0.35 | <0.001 |
| R2 Tjur | 0.011 |
Table 2.
Factors related to the chance of belonging to AP versus IP and AP versus NEP GPs.
Table 2.
Factors related to the chance of belonging to AP versus IP and AP versus NEP GPs.
| | AP vs. IP | AP vs. NEP |
|---|
| Predictors | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
|---|
| (Intercept) | 24.93 | 5.11–129.84 | <0.001 | 5.31 | 1.97–14.51 | 0.001 |
| Specialization (ref: Specialized in general practice) | | | | | | |
| Without specialist qualification | 0.48 | 0.18–1.35 | 0.145 | 1.05 | 0.45–2.42 | 0.909 |
| Internist active in general practice | 0.86 | 0.55–1.36 | 0.519 | 1.27 | 0.93–1.73 | 0.137 |
| Other | 0.34 | 0.03–7.45 | 0.384 | 1.1 | 0.10–23.83 | 0.94 |
| Age GP | 0.97 | 0.94–0.99 | 0.018 | 0.97 | 0.95–0.98 | <0.001 |
| Sex GP (ref: male) | | | | | | |
| Female | 1.03 | 0.65–1.63 | 0.906 | 1.02 | 0.75–1.38 | 0.9 |
| GP network (ref: no) | | | | | | |
| Yes | 0.95 | 0.61–1.51 | 0.825 | 1.21 | 0.89–1.66 | 0.232 |
| Randomization group (ref: control) | | | | | | |
| Intervention | 1.36 | 0.89–2.08 | 0.157 | 1.93 | 1.45–2.57 | <0.001 |
| R2 Tjur | 0.023 | | | 0.051 | | |
Table 3.
Factors related to the chance of belonging to AP versus IP and AP versus NEP practices.
Table 3.
Factors related to the chance of belonging to AP versus IP and AP versus NEP practices.
| | AP vs. IP | AP vs. NEP |
|---|
| Predictors | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
|---|
| (Intercept) | 2.41 | 1.05–5.52 | 0.037 | 1.02 | 0.61–1.72 | 0.933 |
| Number of GPs | 1.22 | 0.88–1.78 | 0.277 | 0.99 | 0.81–1.22 | 0.915 |
| Duration of practice | 1 | 0.98–1.03 | 0.735 | 0.99 | 0.97–1.01 | 0.278 |
| Type of practice (ref: single practice) | | | | | | |
| Group practice | 0.95 | 0.48–1.87 | 0.878 | 1.75 | 1.10–2.79 | 0.018 |
| Medical care center | - | - | 0.987 | 1.12 | 0.15–9.86 | 0.913 |
| Randomization group (ref: control) | | | | | | |
| Intervention | 1.34 | 0.82–2.18 | 0.24 | 2.02 | 1.45–2.82 | <0.001 |
| R2 Tjur | 0.009 | | | 0.046 | | |
Table 4.
Overall number of alerts per category at T0 and change over the course of the study.
Table 4.
Overall number of alerts per category at T0 and change over the course of the study.
| Analysis | Alert Category | Number of Alerts at T0 (Proportion of
Total Alerts) | Change at T1 (%) | Number of Alerts of Severity 1 at T0 (Proportion of Total Alerts) | Change at T1 (%) (Severity 1 Alerts Only) |
|---|
| Main | Dosage | 15,790 (56%) | −5.0 | 9530 (66%) | −6.2 |
| Kidney | 2625 (9%) | −6.2 | 2625 (18%) | −6.2 |
| Interaction | 5836 (21%) | −0.5 | 449 (3%) | −6.1 |
| Duplicate prescription | 2323 (8%) | 3.2 | 1615 (11%) | 3.8 |
| Age | 1653 (6%) | −0.1 | N/A | N/A |
| Allergy | 143 (1%) | 3.4 | 143 (1%) | 3.4 |
| Sensitivity “completed anamnesis” | Dosage | 8879 (55%) | −9.6 | 5337 (66%) | −11.9 |
| Kidney | 1489 (9%) | −11.5 | 1489 (18%) | −11.5 |
| Interaction | 3400 (21%) | −1.6 | 250 (3%) | −11.6 |
| Duplicate prescription | 1417 (9%) | 3.2 | 990 (12%) | 4.2 |
| Age | 944 (6%) | −1.2 | N/A | N/A |
| Allergy | 83 (1%) | 3.4 | 83 (1%) | 3.4 |
Table 5.
Incidence rate ratio of alerts before and after the intervention, stratified by age, sex, alert category, and severity level.
Table 5.
Incidence rate ratio of alerts before and after the intervention, stratified by age, sex, alert category, and severity level.
| | | Incidence Rate Ratio (T1 vs. T0) |
|---|
| Severity | Category | Female | Male |
|---|
| | | <65 Years | ≥65 <85 | ≥85 | <65 Years | ≥65 <85 | ≥85 |
|---|
| 1 & 2 | Dosage | 0.95 (0.88–1.01) | 0.94 (0.92–0.99) ** | 0.95 (0.90–1.00) | 0.96 (0.89–1.03) | 0.96 (0.91–1.00) | 0.96 (0.88–1.06) |
| Kidney | 0.93 (0.77–1.13) | 0.95 (0.87–1.04) | 0.92 (0.81–1.03) | 0.94 (0.76–1.14) | 0.95 (0.85–1.07) | 0.96 (0.78–1.18) |
| Interaction | 1.01 (0.90–1.13) | 1.00 (0.94–1.06) | 0.98 (0.89–1.09) | 0.99 (0.88–1.12) | 0.99 (0.92–1.07) | 1.01 (0.87–1.18) |
| Duplicate prescription | 1.03 (0.90–1.19) | 1.04 (0.94–1.15) | 1.01 (0.84–1.21) | 1.04 (0.88–1.22) | 1.04 (0.92–1.17) | 1.01 (0.78–1.41) |
| Age | 1.13 (0.67–1.72) | 1.04 (0.99–1.06) | 0.99 (0.84–1.15) | 1.14 (0.56–1.87) | 1.01 (0.88–1.17) | 1.00 (0.74–1.43) |
| Allergy | 1.00 (0.55–1.83) | 1.05 (0.74–1.50) | 1.05 (0.59–1.85) | 1.00 (0.42–2.40) | 1.0 (0.57–1.76) | 1.17 (0.39–3.47) |
| 1 | Dosage | 0.93 (0.85–1.02) | 0.94 (0.90–0.99) * | 0.92 (0.86–0.99) * | 0.95 (0.94–1.02) | 0.95 (0.90–1.01) | 0.94 (0.84–1.07) |
| Kidney | 0.93 (0.77–1.13) | 0.95 (0.87–1.04) | 0.92 (0.81–1.03) | 0.94 (0.76–1.14) | 0.95 (0.85–1.07) | 0.96 (0.78–1.18) |
| Interaction | 0.94 (0.62–1.46) | 0.93 (0.76–1.17) | 0.93 (0.64–1.30) | 0.96 (0.64–1.45) | 0.93 (0.71–1.21) | 1.04 (0.51–1.89) |
| Duplicate prescription | 1.04 (0.88–1.23) | 1.05 (0.94–1.19) | 1.01 (0.81–1.25) | 1.05 (0.87–1.28) | 1.03 (0.90–1.19) | 1.01 (0.74–1.49) |
| Allergy | 1.00 (0.55–1.83) | 1.05 (0.74–1.50) | 1.05 (0.59–1.85) | 1.00 (0.42–2.40) | 1.00 (0.57–1.76) | 1.23 (0.43–3.46) |
Table 6.
Incidence rate ratio of unjustified alerts before and after the intervention, stratified by age, sex, alert category, and severity level.
Table 6.
Incidence rate ratio of unjustified alerts before and after the intervention, stratified by age, sex, alert category, and severity level.
| Incidence Rate Ratio (T1 vs. T0) |
|---|
| Severity | Category | Female | Male |
|---|
| | | <65 Years | ≥65 <85 | ≥85 | <65 Years | ≥65 <85 | ≥85 |
|---|
| 1 & 2 | Dosage | 0.85 (0.79–0.91) *** | 0.87 (0.84–0.90) *** | 0.86 (0.82–0.91) *** | 0.86 (0.80–0.93) *** | 0.89 (0.85–0.93) *** | 0.89 (0.81–0.98) * |
| Kidney | 0.78 (0.65–0.95) ** | 0.83 (0.76–0.95) *** | 0.83 (0.73–0.94) ** | 0.83 (0.67–1.03) | 0.86 (0.76–0.97) * | 0.89 (0.72–1.10) |
| Interaction | 0.96 (0.86–1.08) | 0.92 (0.87–0.98) ** | 0.90 (0.81–1.00) | 0.93 (0.83–1.06) | 0.93 (0.86–1.00) | 0.93 (0.80–1.09) |
| Duplicate prescription | 1.00 (0.87–1.14) | 1.01 (0.91–1.11) | 0.94 (0.79–1.14) | 1.02 (0.86–1.20) | 1.01 (0.89–1.15) | 0.97 (0.74–1.27) |
| Age | 1.01 (0.78–1.46) | 0.95 (0.85–1.02) | 0.92 (0.79–1.07) | 1.13 (0.59–1.90) | 0.94 (0.82–1.11) | 0.91 (0.67–1.23) |
| Allergy | 1.00 (0.55–1.83) | 1.02 (0.71–1.46) | 0.96 (0.53–1.82) | 1.00 (0.42–2.40) | 0.92 (0.51–1.63) | 1.17 (0.39–3.47) |
| 1 | Dosage | 0.81 (0.77–0.82) *** | 0.85 (0.81–0.89) *** | 0.83 (0.77–0.89) *** | 0.84 (0.81–0.86) *** | 0.87 (0.82–0.93) *** | 0.87 (0.82–0.93) *** |
| Kidney | 0.783 (0.64–0.95) ** | 0.83 (0.76–0.91) *** | 0.83 (0.73–0.94) ** | 0.83 (0.67–1.03) | 0.86 (0.76–0.97) * | 0.89 (0.72–1.10) |
| Interaction | 0.86 (0.55–1.34) | 0.85 (0.67–1.07) | 0.84 (0.60–1.19) | 0.80 (0.52–1.24) | 0.79 (0.60–1.04) | 0.92 (0.53–1.61) |
| Duplicate prescription | 1.00 (0.85–1.19) | 1.02 (0.91–1.15) | 0.94 (0.76–1.18) | 1.03 (0.85–1.25) | 1.02 (0.88–1.17) | 0.99 (0.73–1.36) |
| Allergy | 0.96 (0.53–1.72) | 1.02 (0.71–1.46) | 0.96 (0.53–1.72) | 1.00 (0.42–2.40) | 0.92 (0.51–1.63) | 1.17 (0.39–3.47) |
Table 7.
Proportion of patients fulfilling the Fidelity criteria.
Table 7.
Proportion of patients fulfilling the Fidelity criteria.
| Alert Category | Number of Patients for Whom the Number of Severe Alerts is >0 at T0 | Number of Patients Fulfilling Fidelity Criteria | Proportion of Patients Fulfilling Fidelity Criteria |
|---|
| Dosage | 3210 | 780 | 24.3% |
| Kidney | 1322 | 383 | 29.0% |
| Interaction | 246 | 71 | 28.9% |
| Duplicate prescription | 787 | 57 | 7.2% |
| Allergy | 64 | 4 | 6.2% |


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}










