
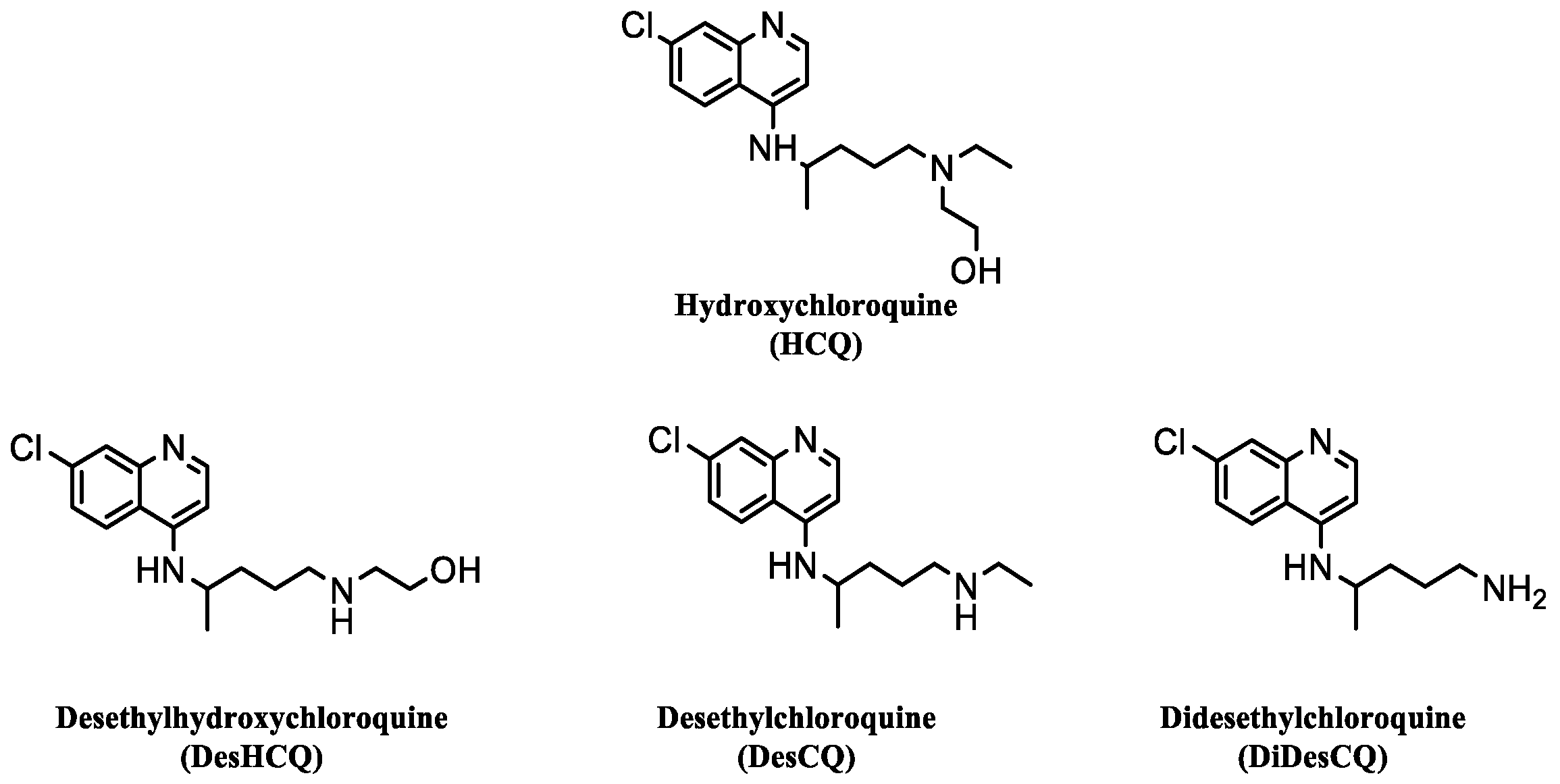
Population Pharmacokinetics of Hydroxychloroquine and 3 Metabolites in COVID-19 Patients and Pharmacokinetic/Pharmacodynamic Application

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Population
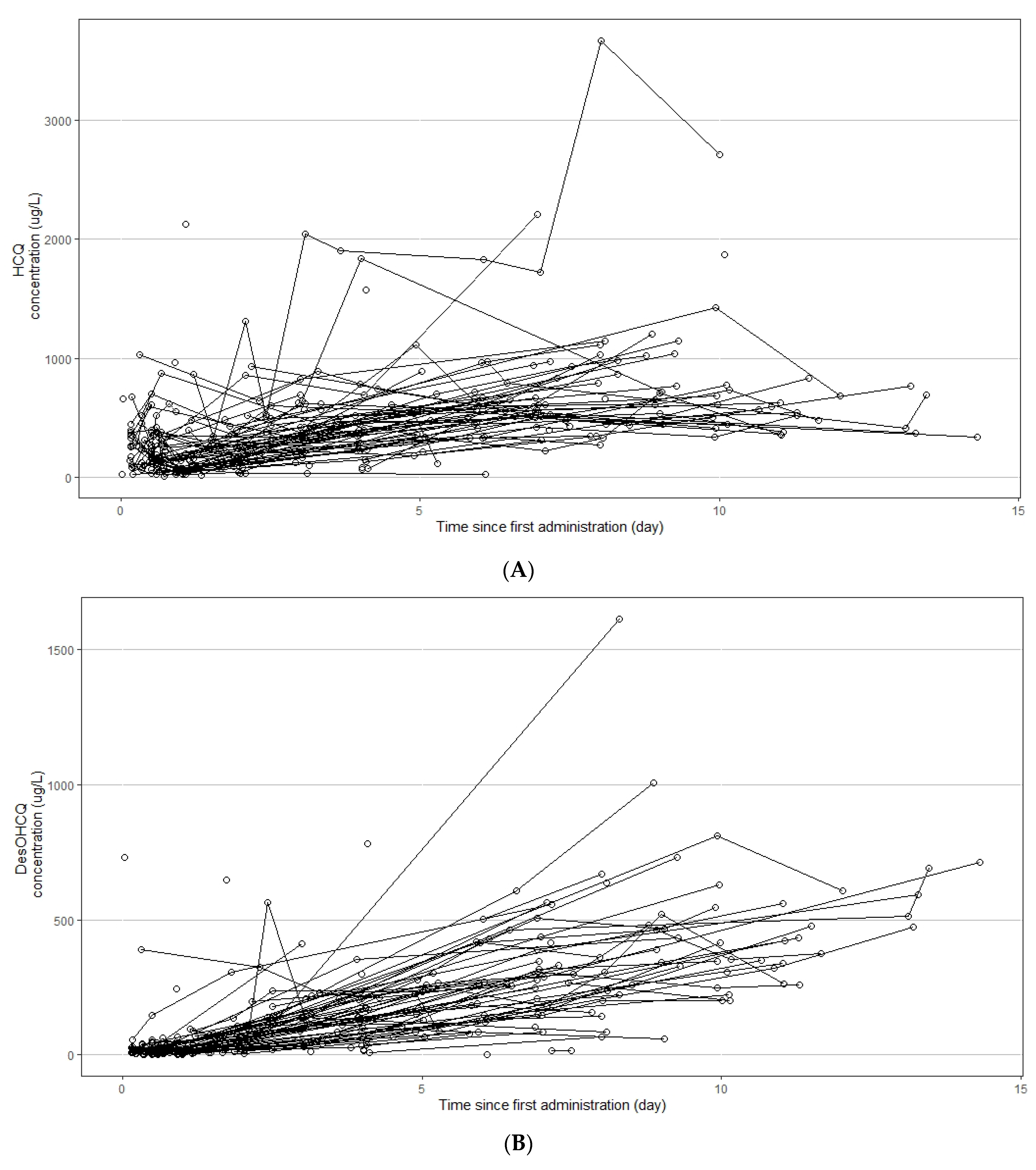
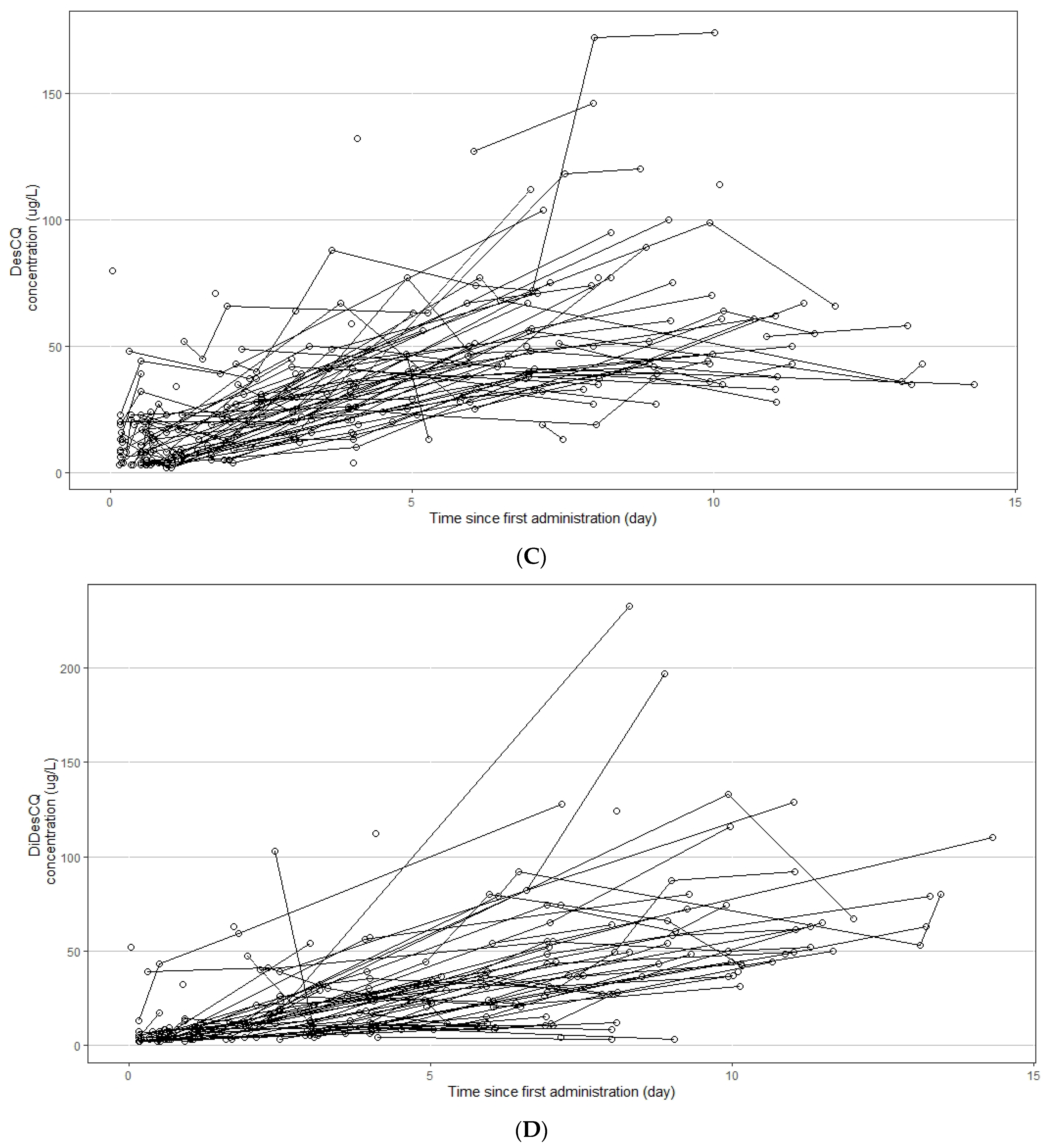
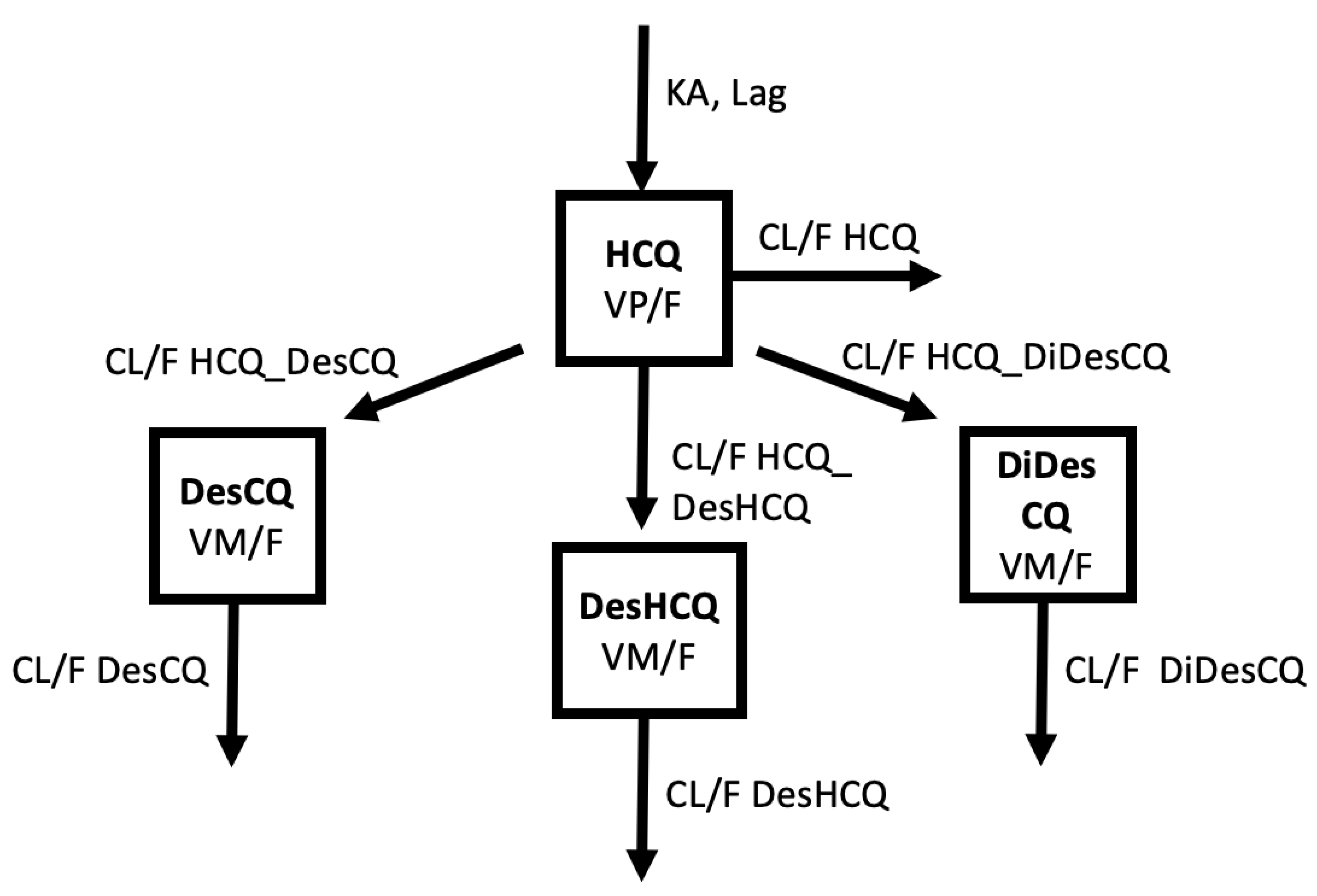
2.1.1. Population Pharmacokinetic Analysis
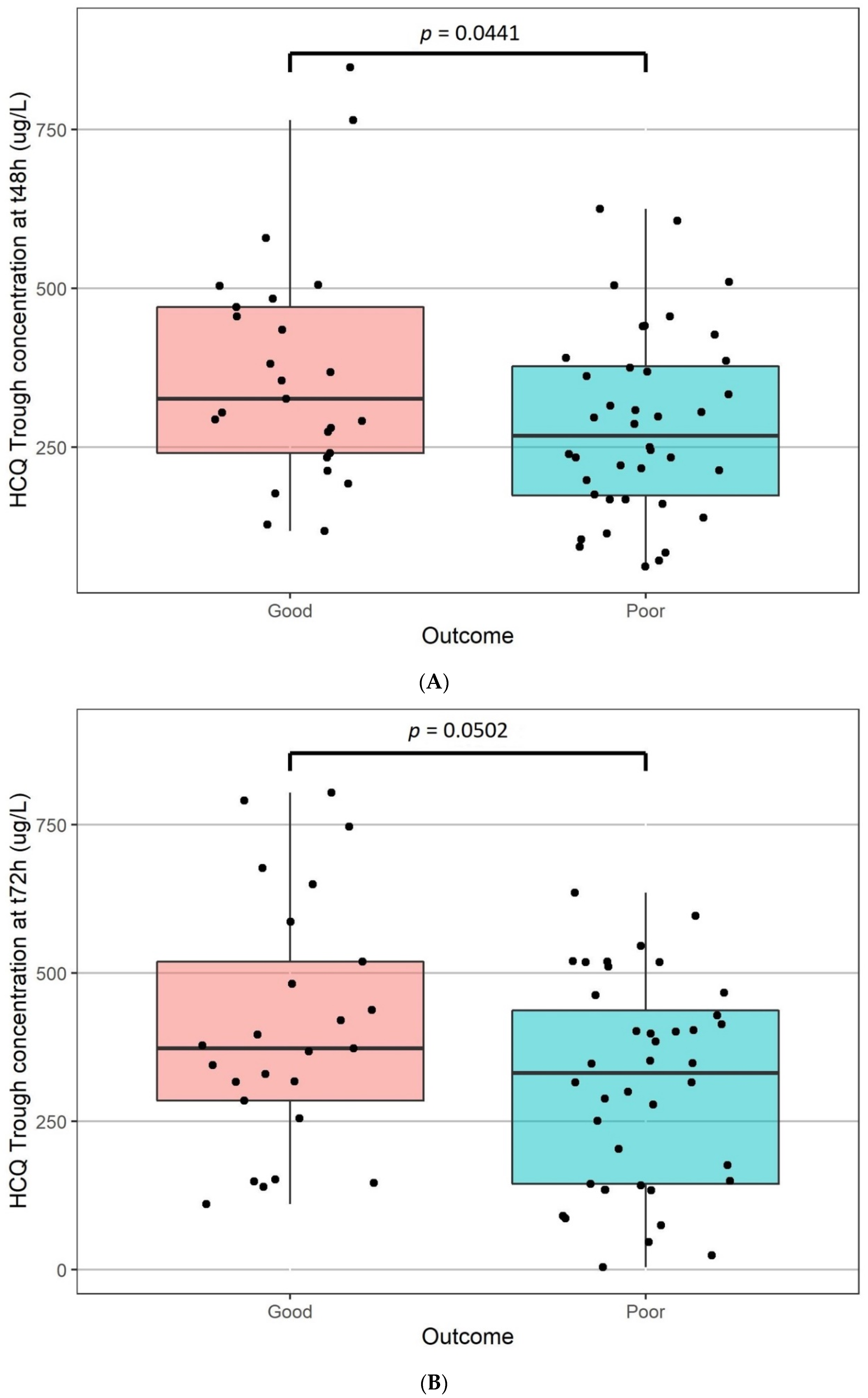
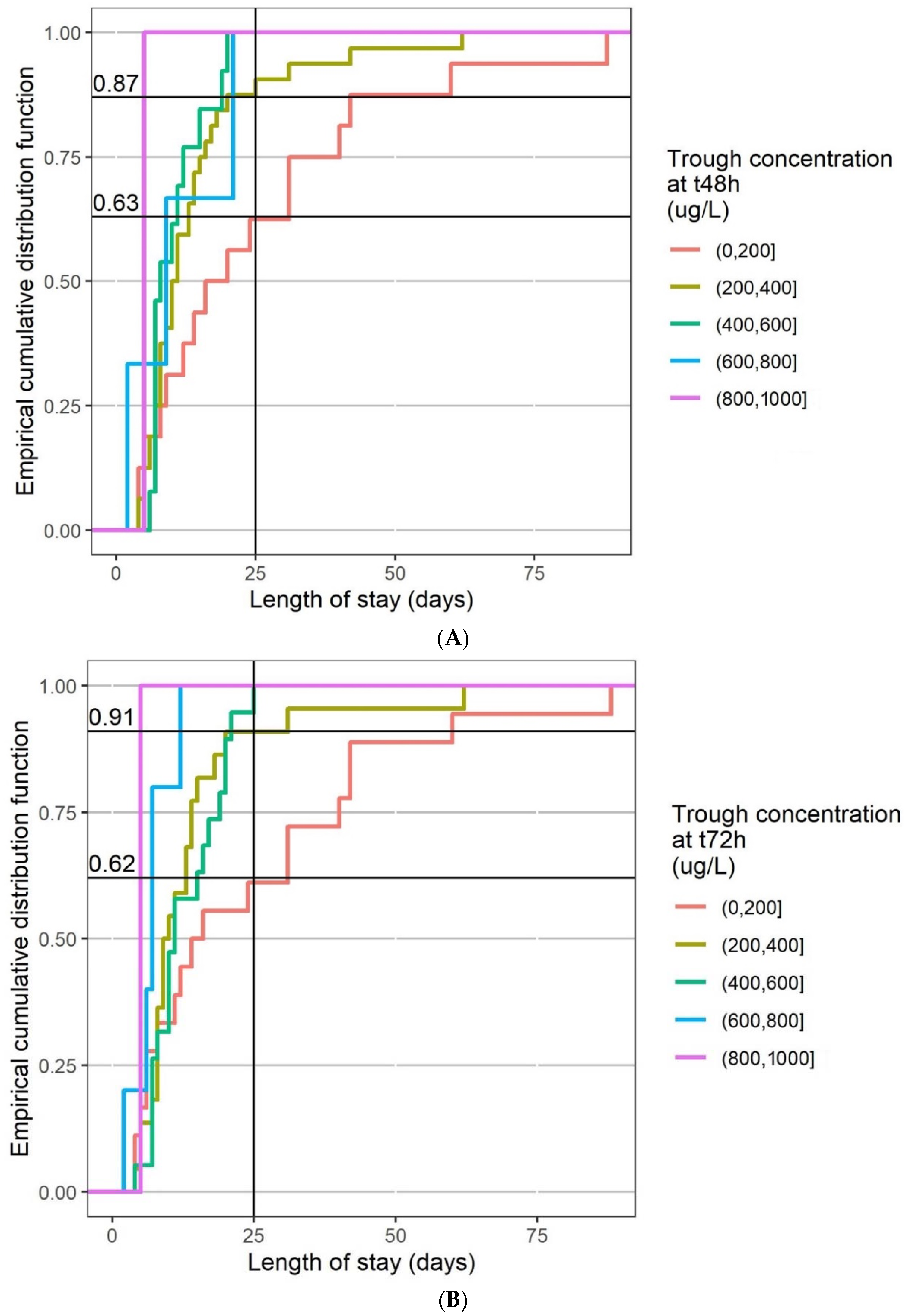
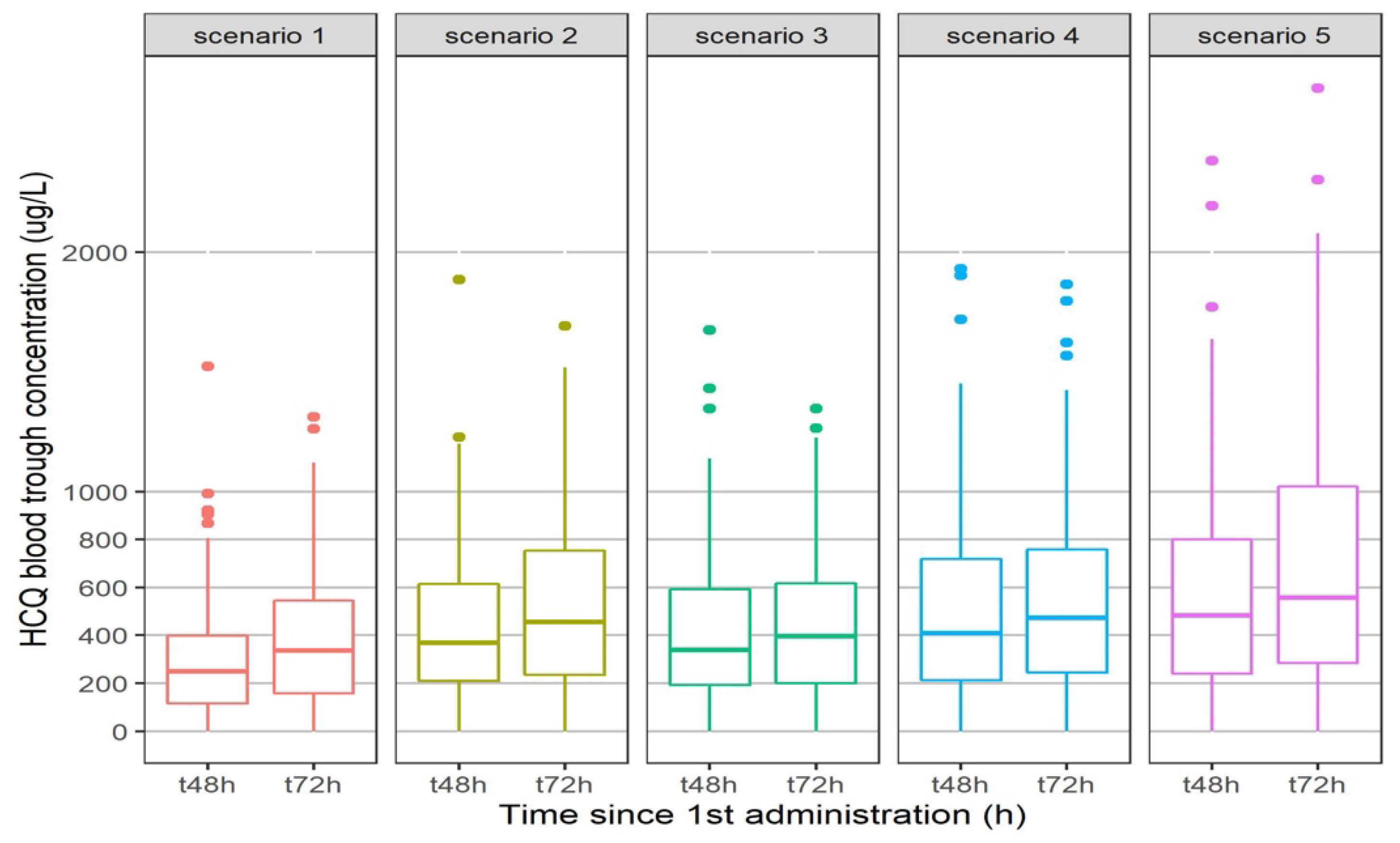
2.1.2. The Pharmacokinetic/Pharmacodynamic Analysis
3. Discussion
4. Materials and Methods
4.1. Population
4.2. HCQ and the 3 Metabolites Measurement
4.3. Pharmacokinetic Analysis
4.4. The Pharmacokinetic/Pharmacodynamic Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martínez, V.G.; Salas, A.A.; Ballestín, S.S. Antiviral Therapeutic Approaches for SARS-CoV-2 Infection: A Systematic Review. Pharmaceuticals 2021, 14, 736. [Google Scholar] [CrossRef] [PubMed]
- Agostini, M.L.; Andres, E.L.; Sims, A.C.; Graham, R.L.; Sheahan, T.P.; Lu, X.; Smith, E.C.; Case, J.B.; Feng, J.Y.; Jordan, R.; et al. Coronavirus Susceptibility to the Antiviral Remdesivir (GS-5734) Is Mediated by the Viral Polymerase and the Proofreading Exoribonuclease. mBio 2018, 9, e00221-18. [Google Scholar] [CrossRef] [Green Version]
- Choy, K.T.; Wong, A.Y.-L.; Kaewpreedee, P.; Sia, S.F.; Chen, D.; Hui, K.P.Y.; Chu, D.K.W.; Chan, M.C.W.; Cheung, P.P.-H.; Huang, X.; et al. Remdesivir, lopinavir, emetine, and homoharringtonine inhibit SARS-CoV-2 replication in vitro. Antivir. Res. 2020, 178, 104786. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef] [PubMed]
- Mehra, M.R.; Desai, S.S.; Ruschitzka, F.; Patel, A.N. Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: A multinational registry analysis. Lancet 2020. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Mafham, M.; Linsell, L.; Bell, J.L.; Staplin, N.; Emberson, J.R.; Wiselka, M.; Ustianowski, A.; Elmahi, E.; et al. Effect of Hydroxychloroquine in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2020, 383, 2030–2040. [Google Scholar]
- MacGowan, A.; Hamilton, F.; Bayliss, M.; Read, L.; Attwood, M.; Noel, A.; Grier, S.; Morley, A.; Arnold, D.; Maskell, N. Hydroxychloroquine serum concentrations in non-critical care patients infected with SARS-CoV-2. J. Glob. Antimicrob. Resist. 2021, 2, 178–179. [Google Scholar] [CrossRef]
- Perinel, S.; Launay, M.; Botelho-Nevers, E.; Diconne, E.; Louf-Durier, A.; Lachand, R.; Murgier, M.; Page, D.; Vermesch, R.; Thierry, G.; et al. Towards Optimization of Hydroxychloroquine Dosing in Intensive Care Unit COVID-19 Patients. Clin. Infect. Dis. 2020, 71, 2227–2229. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, J.C.; Moine, P.; Davido, B.; Etting, I.; Annane, D.; Larabi, I.A.; Simon, N. Population pharmacokinetics of lopinavir/ritonavir in COVID-19 patient. Eur. J. Clin. Pharmacol. 2021, 77, 389–397. [Google Scholar] [CrossRef]
- Williams, S.B.; Patchen, L.C.; Churchill, F.C. Analysis of blood and urine samples for hydroxychloroquine and three major metabolites by high-performance liquid chromatography with fluorescence detection. J. Chromatogr. 1988, 433, 197–206. [Google Scholar] [CrossRef]
- Davila, L.; Ranganathan, P. Pharmacogenetics: Implications for therapy in rheumatic diseases. Nat. Rev. Rheumatol. 2011, 7, 537–550. [Google Scholar] [CrossRef] [PubMed]
- Brocks, D.R.; Skeith, K.J.; Johnston, C.; Emamibafrani, J.; Davis, P.; Russell, A.S.; Jamali, F. Hematologic disposition of hydroxychloroquine enantiomers. J. Clin. Pharmacol. 1994, 34, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Somer, M.; Kallio, J.; Pesonen, U.; Pyykko, K.; Huupponen, R.; Scheinin, M. Influence of hydroxychloroquine on the bioavailability of oral metoprolol. Br. J. Clin. Pharmacol. 2000, 49, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Munster, T.; Gibbs, J.P.; Shen, D.; Baethge, B.A.; Botstein, G.R.; Caldwell, J.; Dietz, F.; Ettlinger, R.; Golden, H.E.; Lindsley, H.; et al. Hydroxychloroquine concentration-response relationships in patients with rheumatoid arthritis. Arthritis Rheum. 2002, 46, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Costedoat-Chalumeau, N.; Amoura, Z.; Hulot, J.S.; Hammoud, H.A.; Aymard, G.; Cacoub, P.; Francès, C.; Wechsler, B.; Le Thi Huong, D.; Ghillani, P.; et al. Low blood concentration of hydroxychloroquine is a marker for and predictor of disease exacerbations in patients with systemic lupus erythematosus. Arthritis Rheum. 2006, 54, 3284–3290. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.S.; Im, J.S.; Cho, J.Y.; Bae, K.S.; Klein, T.A.; Yeom, J.S.; Kim, T.S.; Choi, J.S.; Jang, I.J.; Park, J.W. Pharmacokinetics of hydroxychloroquine and its clinical implications in chemoprophylaxis against malaria caused by Plasmodium vivax. Antimicrob. Agents Chemother. 2009, 53, 1468–1475. [Google Scholar] [CrossRef] [Green Version]
- Miller, D.R.; Khalil, S.K.; Nygard, G.A. Steady-state pharmacokinetics of hydroxychloroquine in rheumatoid arthritis patients. DICP 1991, 25, 1302–1305. [Google Scholar] [CrossRef]
- Tett, S.E.; Cutler, D.J.; Day, R.O.; Brown, K.F. Bioavailability of hydroxychloroquine tablets in healthy volunteers. Br. J. Clin. Pharmacol. 1989, 27, 771–779. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, S.; Concordet, D.; Lanot, T.; Georges, B.; Goudy, P.; Baklouti, S.; Mané, C.; Losha, E.; Vinour, H.; Rousset, D.; et al. Hydroxychloroquine lung pharmacokinetics in critically ill patients with COVID-19. Int. J. Antimicrob. Agents 2021, 57, 106247. [Google Scholar] [CrossRef]
- Recommandations Pour le Suivi Thérapeutique Pharmacologique du lopinavir/r et de l’hydroxychloroquine Chez les Patients Traités Pour une Infection à SARS-CoV-2 (COVID-19). Available online: https://sfpt-fr.org/images/documents/STP/Recommandations_STP_ANRS_AC43_Pharmacologie_v2_26_03_20.pdf (accessed on 14 February 2022).
- Bianco, M.; Biolè, C.A.; Cerrato, E. QT Interval in Patients With COVID-19. JAMA Cardiol. 2021, 6, 357. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Sevestre, J.; Mailhe, M.; Doudier, B.; Aubry, C.; Amrane, S.; et al. Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: A pilot observational study. Travel Med. Infect. Dis. 2020, 34, 101663. [Google Scholar] [CrossRef]
- Gautret, P.; Hoang, V.T.; Lagier, J.C.; Raoult, D. Effect of hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial, an update with an intention-to-treat analysis and clinical outcomes. Int. J. Antimicrob. Agents 2021, 57, 106239. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.D.; Diaz, G.; Urba, W.J. Use of hydroxychloroquine in combination with azithromycin for patients with COVID-19 is not supported by recent literature. Int. J. Antimicrob. Agents 2021, 57, 106174. [Google Scholar] [CrossRef]
- Ghazy, R.M.; Almaghraby, A.; Shaaban, R.; Kamal, A.; Beshir, H.; Moursi, A.; Ramadan, A.; Taha, S.H.N. A systematic review and meta-analysis on chloroquine and hydroxychloroquine as monotherapy or combined with azithromycin in COVID-19 treatment. Sci. Rep. 2020, 10, 22139. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.; Freitas-Santos, R.S.; Levi, J.E.; Senerchia, A.A.; Lopes, A.T.A.; Santos, S.R.; Siciliano, R.F.; Pierrotti, L.C. Hydroxychloroquine plus azithromycin early treatment of mild COVID-19 in outpatient setting: A randomized, double-blinded, placebo-controlled clinical trial evaluating viral clearance. Int. J. Antimicrob. Agents 2021, 58, 106428. [Google Scholar] [CrossRef]
- Mitjà, O.; Corbacho-Monné, M.; Ubals, M.; Tebe, C.; Peñafiel, J.; Tobias, A.; Ballana, E.; Alemany, A.; Riera-Martí, N.; Pérez, C.A.; et al. Hydroxychloroquine for Early Treatment of Adults with Mild COVID-19: A Randomized-Controlled Trial. Clin. Infect. Dis. 2021, 73, e4073–e4081. [Google Scholar] [CrossRef]
- Durcan, L.; Clarke, W.A.; Magder, L.S.; Petri, M. Hydroxychloroquine Blood Levels in Systemic Lupus Erythematosus: Clarifying Dosing Controversies and Improving Adherence. J. Rheumatol. 2015, 42, 2092–2097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qu, Y.; Noe, G.; Breaud, A.R.; Vidal, M.; Clarke, W.A.; Zahr, N.; Dervieux, T.; Costedoat-Chalumeau, N.; Blanchet, B. Development and validation of a clinical HPLC method for the quantification of hydroxychloroquine and its metabolites in whole blood. Future Sci. OA 2015, 1, FSO26. [Google Scholar] [CrossRef]
- Yao, X.; Ye, F.; Zhang, M.; Cui, C.; Huang, B.; Niu, P.; Liu, X.; Zhao, L.; Dong, E.; Song, C.; et al. In Vitro Antiviral Activity and Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2020, 71, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Clementi, N.; Criscuolo, E.; Diotti, R.A.; Ferrarese, R.; Castelli, M.; Dagna, L.; Burioni, R.; Clementi, M.; Mancini, N. Combined prophylactic and therapeutic use maximises hydroxychloroquine anti-SARS-CoV-2 effects in vitro. Front. Microbiol. 2020, 11, 1704. [Google Scholar] [CrossRef]
- Liu, J.; Cao, R.; Xu, M.; Wang, X.; Zhang, H.; Hu, H.; Li, Y.; Hu, Z.; Zhong, W.; Wang, M. Hydroxychloroquine, a less toxic derivative of chloroquine, is effective in inhibiting SARS-CoV-2 infection in vitro. Cell Discov. 2020, 6, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tecen-Yucel, K.; Aras-Atik, E.; Bayraktar-Ekincioglu, A. Does therapeutic drug monitoring of hydroxychloroquine improve treatment outcome in intensive care unit patients with COVID-19? Int. J. Clin. Pract. 2021, 75, e13894. [Google Scholar] [CrossRef] [PubMed]
- Beal, S.; Sheiner, L.B.; Boeckmann, A.; Bauer, R.J. NONMEM User’s Guides (1989–2009); Icon Development Solutions: Ellicott City, MD, USA, 2009. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 18 February 2022).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2009. [Google Scholar]
- Holford, N.H. Wings for NONMEM. Last Update 19 August 2017. Available online: http://wfn.sourceforge.net/ (accessed on 18 February 2022).
- Mould, D.R.; Upton, R.N. Basic concepts in population modeling, simulation, and model-based drug development-part 2: Introduction to pharmacokinetic modeling methods. CPT Pharmacomet. Syst. Pharmacol. 2013, 2, e38. [Google Scholar] [CrossRef] [PubMed]
- Lagier, J.C.; Million, M.; Gautret, P.; Colson, P.; Cortaredona, P.; Giraud-Gatineau, A.; Honoré, S.; Gaubert, J.Y.; Fournier, P.E.; Tissot-Dupont, H.; et al. Outcomes of 3737 COVID-19 patients treated with hydroxychloroquine/azithromycin and other regimens in Marseille, France: A retrospective analysis. Travel Med. Infect. Dis. 2020, 36, 101791. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | |||
|---|---|---|---|
| (n = 100) | |||
| Gender | |||
| Male | 66 | −66.00% | |
| Female | 34 | −34.00% | |
| Age (years) | |||
| Mean (SD) | 60.7 | −15.9 | |
| Median [Min, Max] | 62.5 | [20.0, 94.0] | |
| Height (m) | |||
| Mean (SD) | 1.71 | −0.094 | |
| Median [Min, Max] | 1.73 | [1.52, 1.93] | |
| Body weight (kg) | |||
| Mean (SD) | 83.6 | −20.1 | |
| Median [Min, Max] | 82 | [37.5, 190] | |
| Body Mass Index (kg/m2) | |||
| Mean (SD) | 28.9 | −5.41 | |
| Median [Min, Max] | 27.5 | [18.5, 52.4] | |
| Clinical Unit | |||
| Medicine | 75 | −75.00% | |
| ICU | 25 | −25.00% | |
| Loading dose | |||
| Yes | 42 | −42.00% | |
| No | 58 | −58.00% | |
| Azythromycin | |||
| No | 22 | −22.00% | |
| Yes | 78 | −78.00% | |
| Length of stay (days) | |||
| Mean (SD) | 15.8 | −15.3 | |
| Median [Min, Max] | 11 | [2.00, 88.0] | |
| Missing | 35 | −35.00% | |
| Death | |||
| Yes | 8 | −8.00% | |
| No | 92 | −92 | |
| Clinical outcome | |||
| Poor | 40 | −40.00% | |
| Good | 25 | −25.00% | |
| Missing | 35 | −35.00% | |
| PK Parameters | Unit | Value | RSE | Bootstrap | |
|---|---|---|---|---|---|
| (%) | 0.025 | 0.975 | |||
| Lag (fixed) | h | 0.389 | - | - | - |
| KA (fixed) | 1/h | 1.15 | - | - | - |
| CL/F HCQ | L/h | 5.60 | 15.5 | 2.69 | 9.16 |
| VP/F HCQ | L | 1850 | 10.7 | 1560 | 2190 |
| CL HCQ_DesCQ | L/h | 4.99 | 17.5 | 3.73 | 7.57 |
| CL DesCQ | L/h | 49.8 | 23.7 | 30.8 | 85.8 |
| CL HCQ_DesHCQ | L/h | 9.63 | 10.3 | 8.29 | 11.5 |
| CL DesHCQ | L/h | 8.89 | 27.8 | 3.63 | 15.2 |
| CL HCQ_DiDesCQ | L/h | 1.84 | 10.8 | 1.61 | 2.17 |
| CL DiDesCQ | L/h | 11.6 | 27.2 | 6.21 | 20.5 |
| Inter Individual Variability (ω) | |||||
| CL HCQ | 1.327 | 9.2 | 0.899 | 1.790 | |
| VP HCQ | 0.889 | 17.8 | 0.600 | 1.190 | |
| CL DesCQ | 0.362 | 27 | 0.086 | 0.522 | |
| CL DesHCQ | 0.860 | 23.1 | 0.316 | 1.290 | |
| CL DiDesCQ | 0.953 | 18.1 | 0.621 | 1.300 | |
| Residual Unexplained Variability (σ) | |||||
| Proportional HCQ | 0.448 | 9.6 | 0.355 | 0.543 | |
| Additive HCQ | μg/L | 86.9 | 32.9 | 0.87 | 127 |
| Proportional DesCQ | 0.322 | 11.5 | 0.258 | 0.406 | |
| Additive DesCQ | μg/L | 5.78 | 18 | 2.92 | 7.36 |
| Proportional DesHCQ | 0.428 | 12.7 | 0.345 | 0.542 | |
| Additive DesHCQ | μg/L | 6.69 | 19.6 | 3.79 | 8.37 |
| Proportional DiDescCQ | 0.0574 | 13.7 | 0.046 | 0.072 | |
| Additive DiDescCQ | μg/L | 2.49 | 16.7 | 0.62 | 3.21 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alvarez, J.C.; Davido, B.; Moine, P.; Etting, I.; Annane, D.; Larabi, I.A.; Simon, N. Population Pharmacokinetics of Hydroxychloroquine and 3 Metabolites in COVID-19 Patients and Pharmacokinetic/Pharmacodynamic Application. Pharmaceuticals 2022, 15, 256. https://doi.org/10.3390/ph15020256
Alvarez JC, Davido B, Moine P, Etting I, Annane D, Larabi IA, Simon N. Population Pharmacokinetics of Hydroxychloroquine and 3 Metabolites in COVID-19 Patients and Pharmacokinetic/Pharmacodynamic Application. Pharmaceuticals. 2022; 15(2):256. https://doi.org/10.3390/ph15020256
Chicago/Turabian StyleAlvarez, Jean Claude, Benjamin Davido, Pierre Moine, Isabelle Etting, Djillali Annane, Islam Amine Larabi, and Nicolas Simon. 2022. "Population Pharmacokinetics of Hydroxychloroquine and 3 Metabolites in COVID-19 Patients and Pharmacokinetic/Pharmacodynamic Application" Pharmaceuticals 15, no. 2: 256. https://doi.org/10.3390/ph15020256