
The Effects of Statins on Prostate Cancer Patients Receiving Androgen Deprivation Therapy or Definitive Therapy: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Study Eligibility
2.2. Data Extraction and Quality Assessment
2.3. Statistical Analysis
3. Results and Discussion
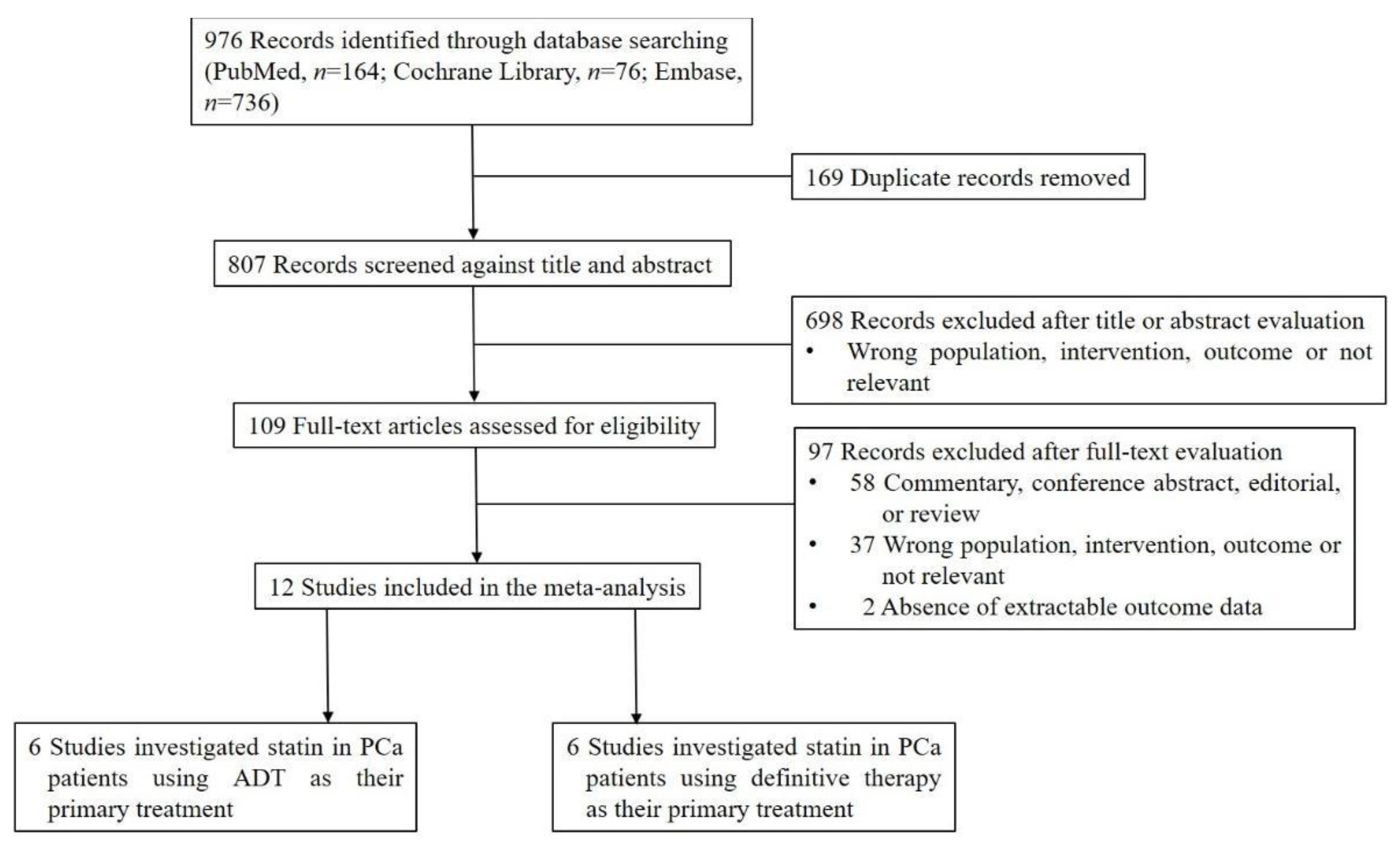
3.1. Literature Search
3.2. Characteristics of the Included Studies

{kind=link}
{kind=link}
{kind=link}
| (a) Author, Year | Study Design, Years, Country | Study Characteristics | Treatment | Time of Statin Use | Follow-Up | Statin Users (n) | Non-Statin Users (n) | Mortality Outcomes | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Jung et al. 2015 [23] | Retrospective cohort, 1997.1–2013.12, Korea | 171 patients with metastatic PCa | ADT | Pre- and post-diagnostic | 52 months (mean) | 46 | 125 | PCa-specific | ||
| Mikkelsen et al. 2017 [24] | Retrospective cohort, 2007.1.1–2013.12.31, Denmark | 537 patients with advanced or metastatic PCa (65.9% metastatic PCa) | ADT, anti-androgens were used as flare protection only | Post-diagnostic and before ADT | 5.7 years (median) | 141 | 396 | All-cause | ||
| Anderson-Carter et al. 2018 [25] | Retrospective cohort, 2000.1.1–2008.12.31, US | 87,346 patients with advanced PCa | ADT for at least 6 months | Post-diagnostic | Until death or the end of the study (2016.5.31) | 53,360 | 33,986 | All-cause; PCa-specific | ||
| Wu et al. 2019 [26] | Retrospective cohort, 2008–2014, Taiwan | 5749 patients with locally advanced and metastatic PCa (55% with metastatic PCa) | ADT | Post-diagnostic | 3.6 years (mean) | 2171 | 3578 | All-cause; PCa-specific | ||
| Hamilton et al. 2021 [27] | Retrospective cohort, 1999.1–2005.11, Canada | 1364 patients with advanced PCa with no distant metastasis | ADT | Post-diagnostic and before ADT | 6.9 years (median) | 585 | 779 | All-cause; PCa-specific | ||
| Peltomaa et al. 2021 [28] | Retrospective cohort, 1996–2015, Finland | 4428 patients with PCa (12.6% with metastatic PCa) | ADT | Post-diagnostic | 6.3 years (median) | 2544 | 1884 | All-cause; PCa-specific | ||
| (b) Author, Year | All-Cause Mortality | Cancer-Specific Mortality | Adjusted For | |||||||
| HR | 95% CI | p | HR | 95% CI | p | |||||
| Jung et al. 2015 [23] | NR | NR | NR | 0.41 | 0.25–0.66 | <0.001 | Age, hypertension, body-mass index, hypercholesterolemia, PSA level, and metastasis type (bone vs. bone and viscera) | |||
| Mikkelsen et al. 2017 [24] | 1.11 | 0.82–1.50 | 0.49 | NR | NR | NR | Age, CCI score, Gleason score, clinical T-stage, PSA level, and metastatic status (M0 and M1) | |||
| Anderson-Carter et al. 2018 [25] | 0.66 | 0.63–0.68 | <0.001 | 0.56 | 0.53–0.60 | <0.001 | Age, duration of ADT use, race, CCI score, Agent Orange exposure, year of the cancer diagnosis, PSA level, and Gleason score | |||
| Wu et al. 2019 * [26] | 0.75 | 0.68–0.82 | NR | 0.77 | 0.69–0.86 | NR | Cancer stage, cancer grade, and year of the cancer diagnosis, and the use of metformin, NSAIDs, and aspirin | |||
| Hamilton et al. 2021 [27] | 0.64 | 0.53–0.78 | <0.001 | 0.65 | 0.48–0.87 | 0.004 | Age, time from RT to ADT, PSA level, and prior ADT use | |||
| Peltomaa et al. 2021 † [28] | (1) 1.13 (2) 0.84 | (1) 1.02–1.25 (2) 0.76–0.93 | NR | (1) 1.12 (2) 0.82 | (1) 0.96–1.31 (2) 0.69–0.96 | NR | Age, tumor risk group (low, intermediate, high), randomization group (PSA screening or none), use of other medication (antidiabetic and antihypertensive drugs, NSAIDs), and whether participants received radiation therapy in addition to ADT | |||
| (A) Author, Year | Study Design, Years, Country | Study Characteristics | Primary Treatment | Time of Statin Use | Follow-Up | Statin users (n) | Non-statin Users (n) | ADT† | Mortality Outcomes | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Katz et al. 2010 * [8] | Retrospective cohort, 1990–2003, USA | 7042 patients with PCa (clinical stage including T1, T2, ≥T3) | RP or RT | Post-primary treatment | 44 or 42 months (median) | 1824 | 5218 | (1) 14% (2) 15% | All-cause | ||
| Caon et al. 2014 [9] | Retrospective cohort, 2000.1.1–2007.12.31, Canada | 3851 patients with localized PCa (T-stages included T1, T2, T3, and T4) | EBRT ± ADT | Post-primary treatment | 8.4 years (median) | 914 | 2937 | (1) 60% (2) 70% | PCa-specific | ||
| Keskivali et al. 2016 [29] | Retrospective cohort, 1995–2009, Finland | 1314 patients with PCa (pathologic stage including T1–T2 with N0 and T3 with or without N1) | RP | Pre- and post-primary treatment (19.1% pre-primary treatment) | 8.6 years (median) | 528 | 786 | NR | All-cause; PCa-specific | ||
| Joentausta et al. 2019† [30] | Retrospective cohort, 1995–2013, Finland | 14,424 patients with localized PCa (N0 for localized, T3–T4 and all N1 for locally advanced) | RP | Pre- and post-diagnostic | (1) Pre-diagnostic: 6.33 years (median) (2) Post-diagnostic: 9.5 years (median) | (1) Pre-diagnostic: 3435 (2) Post-diagnostic: 6728 | (1) Pre-diagnostic: 10,441 (2) Post-diagnostic: 7651 | (1.1) 14.1% (1.2) 19.7% (2.1) 19.8% (2.2) 19.6% | PCa-specific ₸ | ||
| Li et al. 2019 [31] | Retrospective cohort, 2000–2010, Taiwan | 567 patients with PCa | RT | Pre- and/or Post-diagnostic | NR | 174 | 213 | NR | All-cause | ||
| Prabhu et al. 2021 [32] | Retrospective cohort, 2002–2015, USA | 3088 patients with PCa (pathologic stage including T0, T2b–T2c, T3a–T4) | RP | Pre- and post-primary treatment | 112.8 months (median) | 1222 | 1866 | NR | All-cause | ||
| (B) Author, Year | All-Cause Mortality | Cancer-Specific Mortality | Adjusted For | ||||||||
| HR | 95% CI | p | HR | 95% CI | p | ||||||
| Katz et al. 2010 * [8] | (1) 0.35 (2) 0.59 | (1) 0.21–0.58 (2) 0.37–0.94 | NR | NR | NR | NR |
| ||||
| Caon et al. 2014 [9] | NR | NR | NR | 0.77 | 0.55–1.08 | NR | Aspirin use, age, year of treatment, radiation dose, ADT use or not, PSA level, clinical T stage, CCI score, Gleason score | ||||
| Keskivali et al. 2016 ‡ [29] | (1) 1.08 (2) 1.28 | (1) 0.69–1.69 (2) 0.92–1.78 | NR | (1) 0.99 (2) 0.81 | (1) 0.38–2.57 (2) 0.37–1.78 | NR | Age, cancer stage, Gleason score, PSA level, surgical margin positivity, total cholesterol, and use of antidiabetic and antihypertensive drugs | ||||
| Joentausta et al. 2019 ₸ [30] | NR | NR | NR | (1) 0.70 (2) 0.83 | (1) 0.52–0.95 (2) 0.67–1.03 | NR | Age, cancer stage, any use of chemotherapy or radiotherapy for PCa, diabetes, hypertension, coronary artery disease, and obesity | ||||
| Li et al. 2019 § [31] | (1) 0.77 (2) 1.60 (3) 0.24 | (1) 0.50–1.19 (2) 0.91–2.82 (3) 0.09–0.66 | NR | NR | NR | NR | Age, diabetes, hypertension, cardiovascular disease, peripheral artery disease, and atherosclerosis | ||||
| Prabhu et al. 2021 [32] | 1.30 | 0.97–1.74 | 0.077 | NR | NR | NR | NR | ||||
3.3. Quality Assessment of Included Studies
3.4. Statin Use and All-Cause Mortality
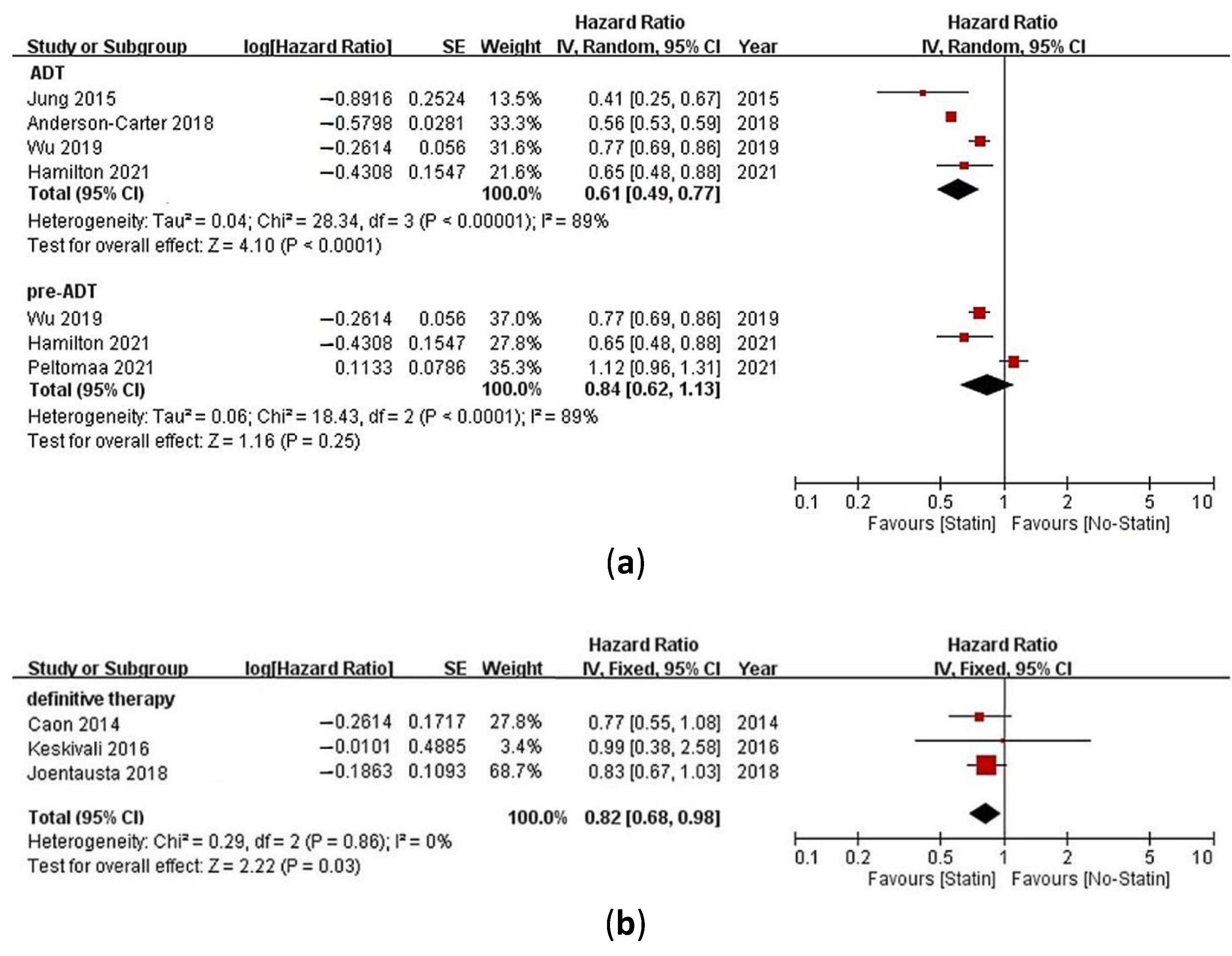
3.5. Statin Use and Cancer-Specific Mortality
3.6. Sensitivity Analysis
3.7. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hu, M.; Cheung, B.M.Y.; Tomlinson, B. Safety of statins: An update. Ther. Adv. Drug Saf. 2012, 3, 133–144. [Google Scholar] [CrossRef] [Green Version]
- Papadopoulos, G.; Delakas, D.; Nakopoulou, L.; Kassimatis, T. Statins and prostate cancer: Molecular and clinical aspects. Eur. J. Cancer (Oxf. Engl. 1990) 2011, 47, 819–830. [Google Scholar] [CrossRef]
- Hamilton, R.J.; Freedland, S.J. Rationale for statins in the chemoprevention of prostate cancer. Curr. Urol. Rep. 2008, 9, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Lifshitz, K.; Ber, Y.; Margel, D. Role of Metabolic Syndrome in Prostate Cancer Development. Eur. Urol. Focus 2021, 7, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Shoag, J.; Barbieri, C.E. Clinical variability and molecular heterogeneity in prostate cancer. Asian J. Androl. 2016, 18, 543–548. [Google Scholar] [CrossRef]
- Marcella, S.W.; David, A.; Ohman-Strickland, P.A.; Carson, J.; Rhoads, G.G. Statin use and fatal prostate cancer: A matched case-control study. Cancer 2012, 118, 4046–4052. [Google Scholar] [CrossRef] [PubMed]
- Niraula, S.; Pond, G.; de Wit, R.; Eisenberger, M.; Tannock, I.F.; Joshua, A.M. Influence of concurrent medications on outcomes of men with prostate cancer included in the TAX 327 study. Can. Urol. Assoc. J. 2013, 7, E74–E81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, M.S.; Carroll, P.R.; Cowan, J.E.; Chan, J.M.; D’Amico, A.V. Association of statin and nonsteroidal anti-inflammatory drug use with prostate cancer outcomes: Results from CaPSURE. BJU Int. 2010, 106, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Caon, J.; Paquette, M.; Hamm, J.; Pickles, T. Does statin or ASA affect survival when prostate cancer is treated with external beam radiation therapy? Prostate Cancer 2014, 2014, 184297. [Google Scholar] [CrossRef]
- Emilsson, L.; García-Albéniz, X.; Logan, R.W.; Caniglia, E.C.; Kalager, M.; Hernán, M.A. Examining bias in studies of statin treatment and survival in patients with cancer. JAMA Oncol. 2018, 4, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Keyes, M.; Crook, J.; Morton, G.; Vigneault, E.; Usmani, N.; Morris, W.J. Treatment options for localized prostate cancer. Can. Fam. Physician 2013, 59, 1269–1274. [Google Scholar]
- Saad, F.; Fizazi, K. Androgen Deprivation Therapy and Secondary Hormone Therapy in the Management of Hormone-sensitive and Castration-resistant Prostate Cancer. Urology 2015, 86, 852–861. [Google Scholar] [CrossRef]
- Meng, Y.; Liao, Y.-B.; Xu, P.; Wei, W.-R.; Wang, J. Statin use and mortality of patients with prostate cancer: A meta-analysis. OncoTargets Ther. 2016, 9, 1689. [Google Scholar]
- Park, H.S.; Schoenfeld, J.D.; Mailhot, R.B.; Shive, M.; Hartman, R.I.; Ogembo, R.; Mucci, L.A. Statins and prostate cancer recurrence following radical prostatectomy or radiotherapy: A systematic review and meta-analysis. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2013, 24, 1427–1434. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Pang, L.; Hu, X.; Wang, W.; Xu, B.; Zhang, X.; Liu, L. The effect of statins on advanced prostate cancer patients with androgen deprivation therapy or abiraterone/enzalutamide: A systematic review and meta-analysis. J. Clin. Pharm. Ther. 2020, 45, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2000. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 18 October 2021).
- Lo, C.K.-L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Houwelingen, H.C.; Arends, L.R.; Stijnen, T. Advanced methods in meta-analysis: Multivariate approach and meta-regression. Stat. Med. 2002, 21, 589–624. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Contour-enhanced meta-analysis funnel plots help distinguish publication bias from other causes of asymmetry. J. Clin. Epidemiol. 2008, 61, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.; Lee, C.; Lee, C.; Kwon, T.; You, D.; Jeong, I.G.; Hong, J.H.; Ahn, H.; Kim, C.-S. Effects of statin use on the response duration to androgen deprivation therapy in metastatic prostate cancer. Korean J. Urol. 2015, 56, 630–636. [Google Scholar] [CrossRef] [Green Version]
- Mikkelsen, M.K.; Thomsen, F.B.; Berg, K.D.; Jarden, M.; Larsen, S.B.; Hansen, R.B.; Brasso, K. Associations between statin use and progression in men with prostate cancer treated with primary androgen deprivation therapy. Scand. J. Urol. 2017, 51, 464–469. [Google Scholar] [CrossRef]
- Anderson-Carter, I.; Posielski, N.; Liou, J.I.; Khemees, T.A.; Downs, T.M.; Abel, E.J.; Jarrard, D.F.; Richards, K.A. The impact of statins in combination with androgen deprivation therapyin patients with advanced prostate cancer: A large observational study. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 130–137. [Google Scholar] [CrossRef]
- Wu, S.-Y.; Fang, S.-C.; Shih, H.-J.; Wen, Y.-C.; Shao, Y.-H.J. Mortality associated with statins in men with advanced prostate cancer treated with androgen deprivation therapy. Eur. J. Cancer 2019, 112, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, R.J.; Ding, K.; Crook, J.M.; O’Callaghan, C.J.; Higano, C.S.; Dearnaley, D.P.; Horwitz, E.M.; Goldenberg, S.L.; Gospodarowicz, M.K.; Klotz, L. The association between statin use and outcomes in patients initiating androgen deprivation therapy. Eur. Urol. 2021, 79, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Peltomaa, A.; Raittinen, P.; Talala, K.; Taari, K.; Tammela, T.; Auvinen, A.; Murtola, T. Prostate cancer prognosis after initiation of androgen deprivation therapy among statin users. A population-based cohort study. Prostate Cancer Prostatic Dis. 2021, 24, 917–924. [Google Scholar] [CrossRef]
- Keskiväli, T.; Kujala, P.; Visakorpi, T.; Tammela, T.L.; Murtola, T.J. Statin use and risk of disease recurrence and death after radical prostatectomy. Prostate 2016, 76, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Joentausta, R.M.; Rannikko, A.; Murtola, T.J. Prostate cancer survival among statin users after prostatectomy in a Finnish nationwide cohort. Prostate 2019, 79, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Si-Tu, J.; Qiu, J.; Lu, L.; Mao, Y.; Zeng, H.; Chen, M.; Lai, C.; Chang, H.-J.; Wang, D. Statin and metformin therapy in prostate cancer patients with hyperlipidemia who underwent radiotherapy: A population-based cohort study. Cancer Manag. Res. 2019, 11, 1189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prabhu, N.; Kapur, N.; Catalona, W.; Leikin, R.; Helenowski, I.; Jovanovich, B.; Gurley, M.; Okwuosa, T.M.; Kuzel, T.M. Statin use and risk of prostate cancer biochemical recurrence after radical prostatectomy. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 130.e9–130.e15. [Google Scholar] [CrossRef] [PubMed]
- Murtola, T.J.; Syvälä, H.; Tolonen, T.; Helminen, M.; Riikonen, J.; Koskimäki, J.; Pakarainen, T.; Kaipia, A.; Isotalo, T.; Kujala, P. Atorvastatin versus placebo for prostate cancer before radical prostatectomy—A randomized, double-blind, placebo-controlled clinical trial. Eur. Urol. 2018, 74, 697–701. [Google Scholar] [CrossRef] [PubMed]
- Hamdy, F.C.; Donovan, J.L.; Lane, J.; Mason, M.; Metcalfe, C.; Holding, P.; Davis, M.; Peters, T.J.; Turner, E.L.; Martin, R.M. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N. Engl. J. Med. 2016, 375, 1415–1424. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.; Porter, D.C.; Chen, X.; Herliczek, T.; Lowe, M.; Keyomarsi, K. Lovastatin-mediated G1 arrest is through inhibition of the proteasome, independent of hydroxymethyl glutaryl-CoA reductase. Proc. Natl. Acad. Sci. USA 1999, 96, 7797–7802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, P.H.; Davidson, M.H.; Stein, E.A.; Bays, H.E.; McKenney, J.M.; Miller, E.; Cain, V.A.; Blasetto, J.W.; Group, S.S. Comparison of the efficacy and safety of rosuvastatin versus atorvastatin, simvastatin, and pravastatin across doses (STELLAR Trial). Am. J. Cardiol. 2003, 92, 152–160. [Google Scholar] [CrossRef]
- Wong, W.W.; Dimitroulakos, J.; Minden, M.; Penn, L. HMG-CoA reductase inhibitors and the malignant cell: The statin family of drugs as triggers of tumor-specific apoptosis. Leukemia 2002, 16, 508–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dulak, J.; Józkowicz, A. Anti-angiogenic and anti-inflammatory effects of statins: Relevance to anti-cancer therapy. Curr Cancer Drug Targets 2005, 5, 579–594. [Google Scholar] [CrossRef] [PubMed]
- Pelton, K.; Freeman, M.R.; Solomon, K.R. Cholesterol and prostate cancer. Curr. Opin. Pharmacol. 2012, 12, 751–759. [Google Scholar] [CrossRef] [Green Version]
- Roy, M.; Kung, H.-J.; Ghosh, P.M. Statins and prostate cancer: Role of cholesterol inhibition vs. prevention of small GTP-binding proteins. Am. J. Cancer Res. 2011, 1, 542–561. [Google Scholar]
- Yokomizo, A.; Shiota, M.; Kashiwagi, E.; Kuroiwa, K.; Tatsugami, K.; Inokuchi, J.; Takeuchi, A.; Naito, S. Statins reduce the androgen sensitivity and cell proliferation by decreasing the androgen receptor protein in prostate cancer cells. Prostate 2011, 71, 298–304. [Google Scholar] [CrossRef]
- Boudreau, D.M.; Yu, O.; Buist, D.S.; Miglioretti, D.L. Statin use and prostate cancer risk in a large population-based setting. Cancer Causes Control 2008, 19, 767–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agalliu, I.; Salinas, C.A.; Hansten, P.D.; Ostrander, E.A.; Stanford, J.L. Statin use and risk of prostate cancer: Results from a population-based epidemiologic study. Am. J. Epidemiol. 2008, 168, 250–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shannon, J.; Tewoderos, S.; Garzotto, M.; Beer, T.M.; Derenick, R.; Palma, A.; Farris, P.E. Statins and prostate cancer risk: A case-control study. Am. J. Epidemiol. 2005, 162, 318–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hou, Y.-C.; Shao, Y.-H. The Effects of Statins on Prostate Cancer Patients Receiving Androgen Deprivation Therapy or Definitive Therapy: A Systematic Review and Meta-Analysis. Pharmaceuticals 2022, 15, 131. https://doi.org/10.3390/ph15020131
Hou Y-C, Shao Y-H. The Effects of Statins on Prostate Cancer Patients Receiving Androgen Deprivation Therapy or Definitive Therapy: A Systematic Review and Meta-Analysis. Pharmaceuticals. 2022; 15(2):131. https://doi.org/10.3390/ph15020131
Chicago/Turabian StyleHou, Yu-Chen, and Yu-Hsuan Shao. 2022. "The Effects of Statins on Prostate Cancer Patients Receiving Androgen Deprivation Therapy or Definitive Therapy: A Systematic Review and Meta-Analysis" Pharmaceuticals 15, no. 2: 131. https://doi.org/10.3390/ph15020131